


Effects of Two Physical Activity Interventions on Sleep and Sedentary Time in Pregnant Women
 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Ethics and Public Involvement
2.2. Setting
2.3. Participants and Study Design
2.4. Interventions
2.5. Outcomes
2.5.1. Sleep Quantity and Quality by Pittsburgh Sleep Quality Index
2.5.2. Sedentary Time by the Pregnancy Physical Activity Questionnaire
2.5.3. Sleep and Sedentary Time by the Activity Tracker
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
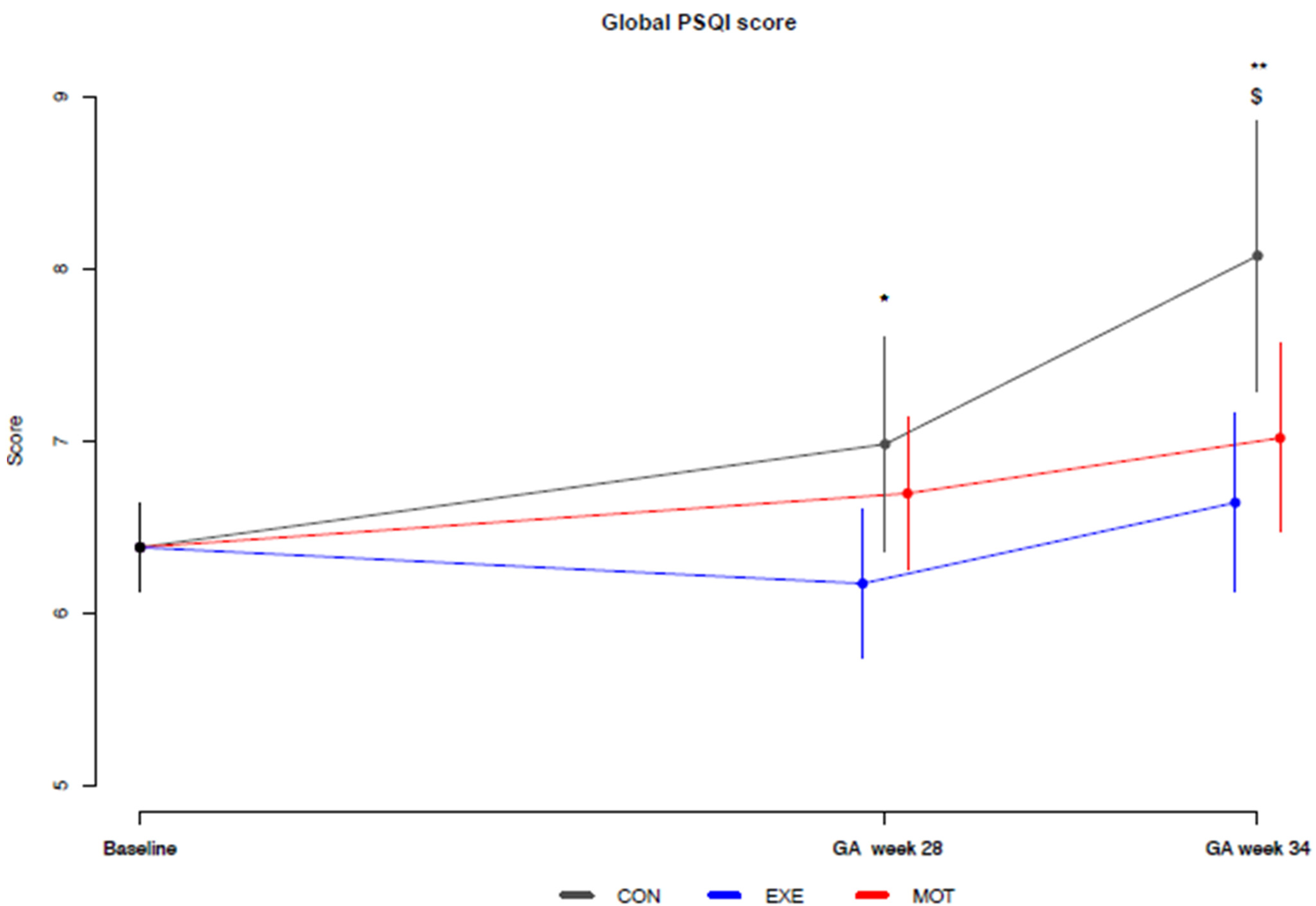
3.2. Sleep Quantity and Quality by the Pittsburgh Sleep Quality Index
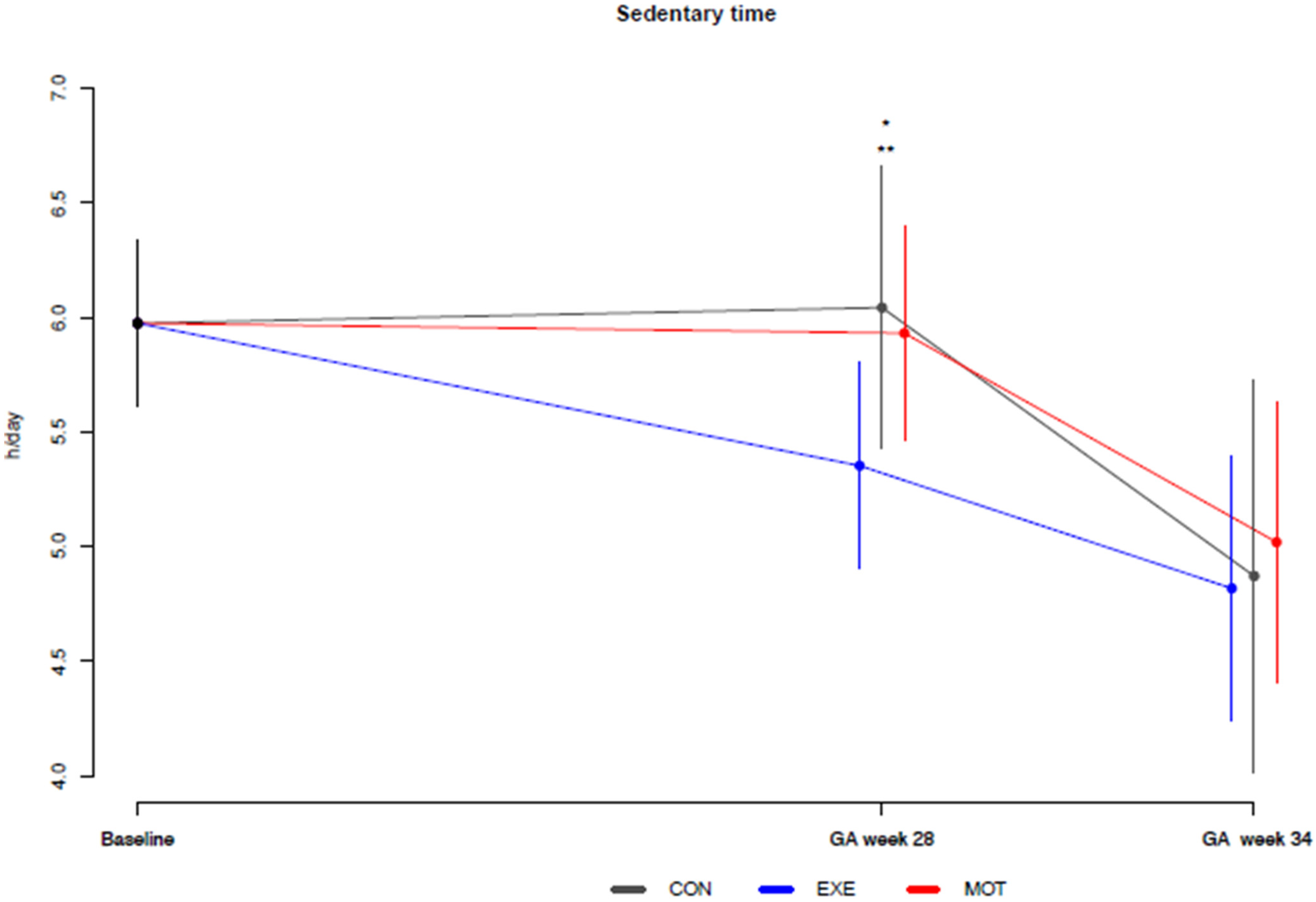
3.3. Sedentary Time by the Pregnancy Physical Activity Questionnaire
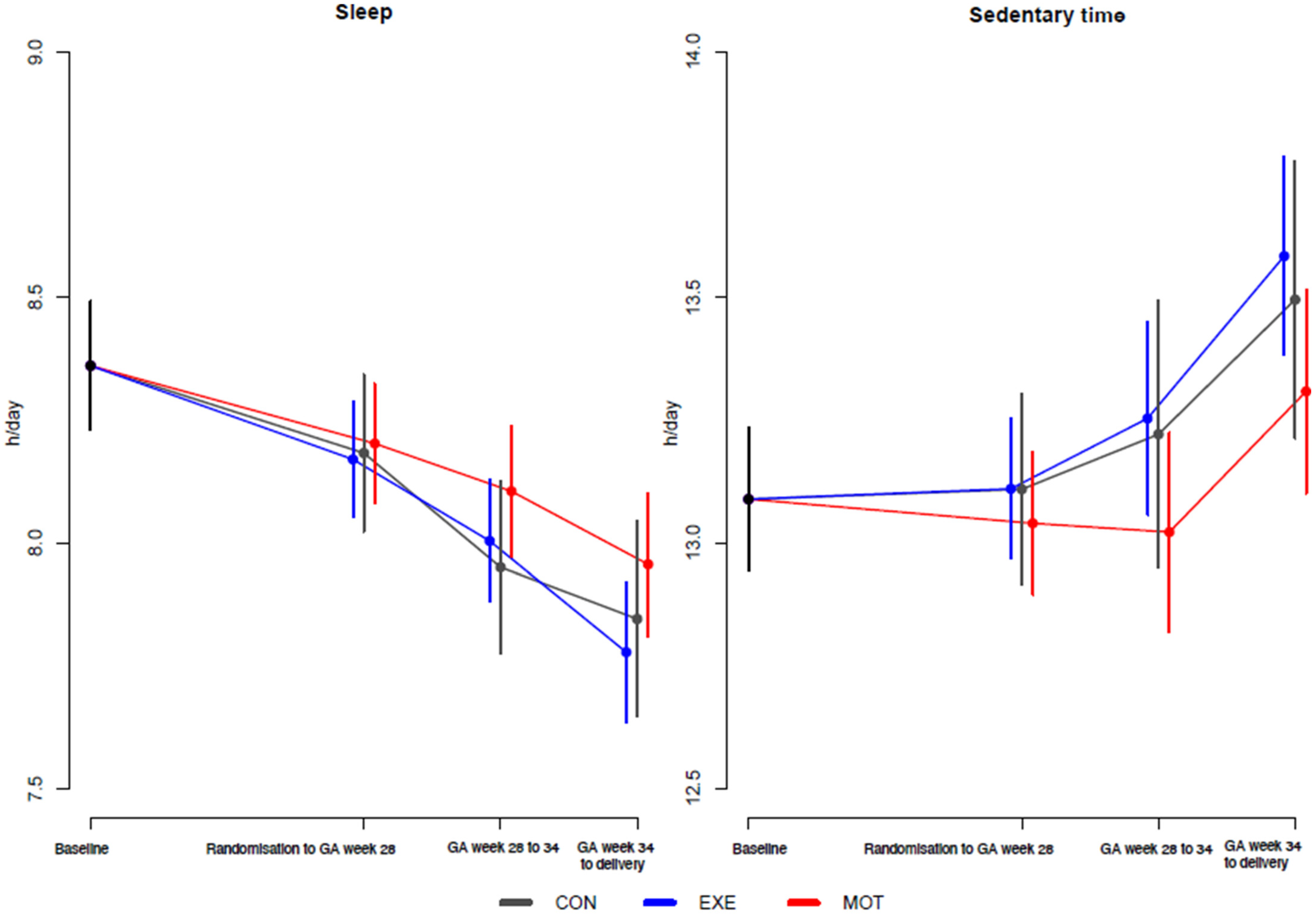
3.4. Sleep and Sedentary Time by the Activity Tracker
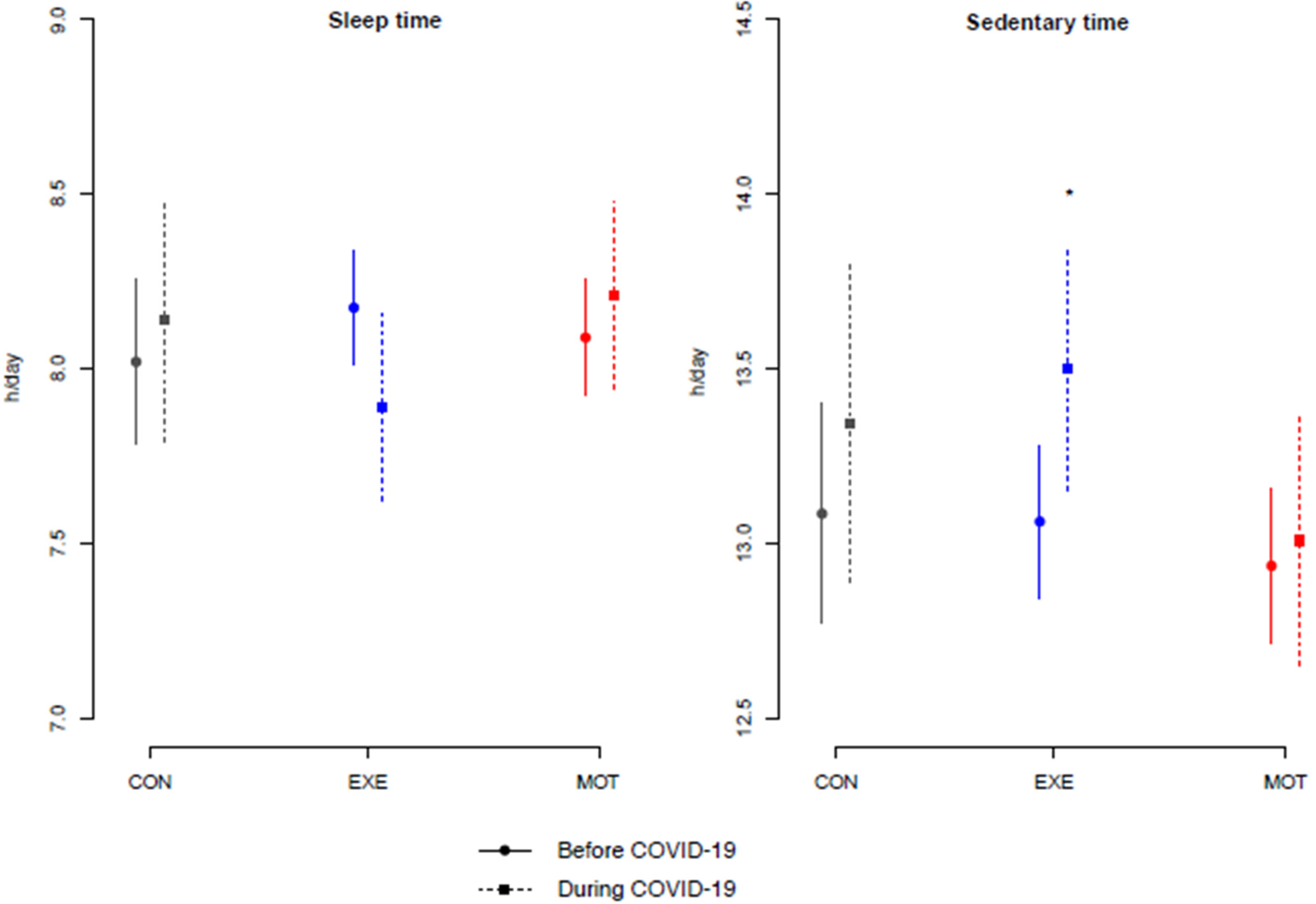
3.5. COVID-19 Impact on Sleep and Sedentary Time as Measured by the Activity Tracker
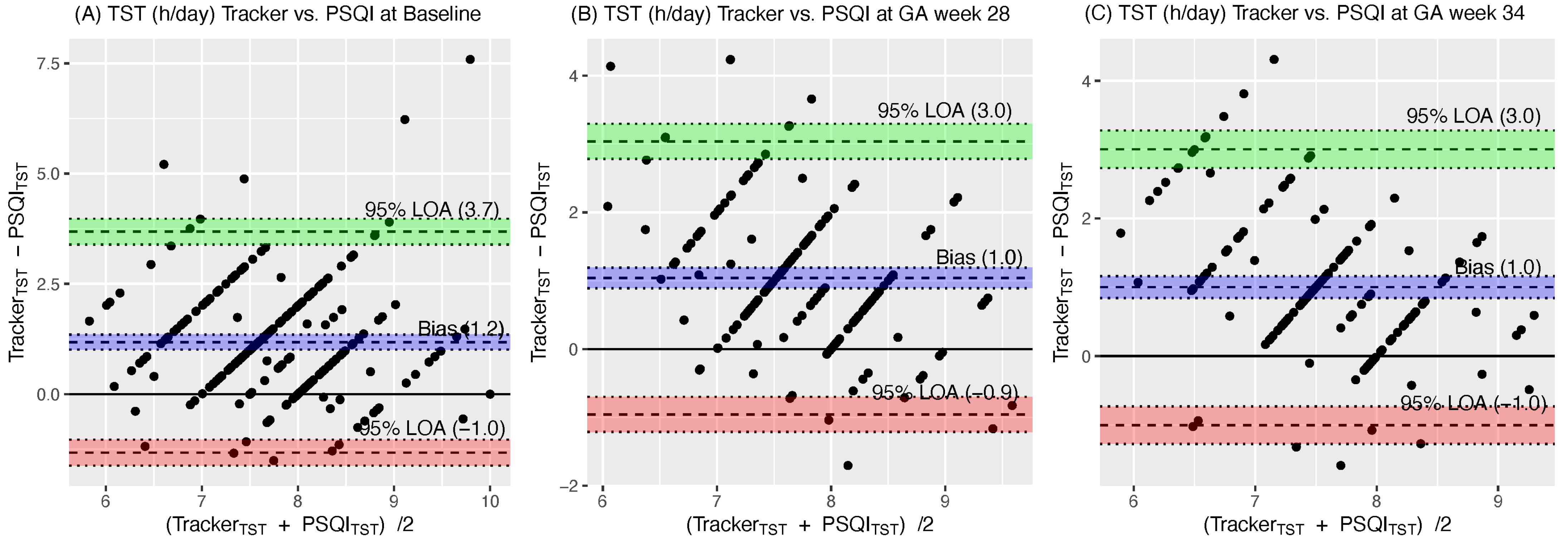
3.6. Comparison of Sleep Time from the Activity Tracker and the Pittsburgh Sleep Quality Index
4. Discussion
4.1. Effectiveness of Physical Activity Interventions on Sleep Quality as Determined by the Pittsburgh Sleep Quality Index
4.2. Effectiveness of Physical Activity Interventions on Sedentary Time as Determined by the Pregnancy Physical Activity Questionnaire
4.3. Sleep and Sedentary Time as Determined by the Activity Tracker
4.4. Sedentary Time Measured by the Pregnancy Physical Activity Questionnaire and the Activity Tracker
4.5. Validity of Activity Trackers for Measuring Total Sleep Time
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Registration
Abbreviations
References
- The American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period. ACOG Committee Opinion No. 804. Obstet. Gynecol. 2020, 135, e178–e188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cilar Budler, L.; Budler, M. Physical Activity during Pregnancy: A Systematic Review for the Assessment of Current Evidence with Future Recommendations. BMC Sports Sci. Med. Rehabil. 2022, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Zhang, X.; Wang, Y.; Li, J.; Xu, Y.; Song, X.; Su, S.; Zhu, X.; Vitiello, M.V.; Shi, J.; et al. Sleep Disturbances during Pregnancy and Adverse Maternal and Fetal Outcomes: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2021, 58, 101436. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.J.; Pien, G.W.; Duntley, S.P.; Macones, G.A. Sleep Deprivation during Pregnancy and Maternal and Fetal Outcomes: Is There a Relationship? Sleep Med. Rev. 2010, 14, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvestri, R.; Aricò, I. Sleep Disorders in Pregnancy. Sleep Sci. 2019, 12, 232–239. [Google Scholar] [CrossRef] [Green Version]
- Sedov, I.D.; Cameron, E.E.; Madigan, S.; Tomfohr-Madsen, L.M. Sleep Quality during Pregnancy: A Meta-Analysis. Sleep Med. Rev. 2018, 38, 168–176. [Google Scholar] [CrossRef]
- Wang, F.; Boros, S. The Effect of Physical Activity on Sleep Quality: A Systematic Review. Eur. J. Physiother. 2021, 23, 11–18. [Google Scholar] [CrossRef]
- Cannon, S.S.; Lastella, M.; Evenson, K.R.; Hayman, M.J. The Association between Physical Activity and Sleep during Pregnancy: A Systematic Review. Behav. Sleep Med. 2022, 16, 1–16. [Google Scholar] [CrossRef]
- Paulino, D.S.M.; Borrelli, C.B.; Faria-Schützer, D.B.; Brito, L.G.O.; Surita, F.G. Non-Pharmacological Interventions for Improving Sleep Quality During Pregnancy: A Systematic Review and Meta-Analysis. Rev. Bras. De Ginecol. E Obs. RBGO Gynecol. Obstet. 2022, 44, 776–784. [Google Scholar] [CrossRef]
- Brislane, Á.; Hayman, M.J.; Davenport, M.H. A Delphi Study to Identify Research Priorities Regarding Physical Activity, Sedentary Behavior and Sleep in Pregnancy. Int. J. Environ. Res. Public Health 2022, 19, 2909. [Google Scholar] [CrossRef]
- Pate, R.R.; O’neill, J.R.; Lobelo, F.; Pate, R.R.; O’neill, J.R. The Evolving Definition of “sedentary”. Exerc. Sport Sci. Rev. 2008, 36, 173–178. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J.H. Sedentary Time in Adults and the Association with Diabetes, Cardiovascular Disease and Death: Systematic Review and Meta-Analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary Behaviors and Subsequent Health Outcomes in Adults: A Systematic Review of Longitudinal Studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Fazzi, C.; Saunders, D.H.; Linton, K.; Norman, J.E.; Reynolds, R.M. Sedentary Behaviours during Pregnancy: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 32. [Google Scholar] [CrossRef] [Green Version]
- di Fabio, D.R.; Blomme, C.K.; Smith, K.M.; Welk, G.J.; Campbell, C.G. Adherence to Physical Activity Guidelines in Mid-Pregnancy Does Not Reduce Sedentary Time: An Observational Study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Roland, C.B.; Knudsen, S.D.P.; Alomairah, S.A.; Andersen, A.D.; Bendix, J.; Clausen, T.D.; Molsted, S.; Jensen, A.K.; Teilmann, G.; Jespersen, A.P.; et al. Structured Supervised Exercise Training or Motivational Counselling during Pregnancy on Physical Activity Level and Health of Mother and Offspring: FitMum Study Protocol. BMJ Open 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Knudsen, S.D.P.; Alomairah, S.A.; Roland, C.B.; Jessen, A.D.; Hergel, I.-M.; Clausen, T.D.; Larsen, J.E.; van Hall, G.; Jensen, A.K.; Molsted, S.; et al. Effects of Structured Supervised Exercise Training or Motivational Counseling on Pregnant Women’s Physical Activity Level: FitMum Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, 1–13. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- University of Pittsburgh. Pittsburgh Sleep Quality Index (PSQI); University of Pittsburgh: Pittsburgh, PA, USA, 1988. [Google Scholar]
- Qiu, C.; Gelaye, B.; Zhong, Q.-Y.; Enquobahrie, D.A.; Frederick, I.O.; Williams, M.A. Construct Validity and Factor Structure of the Pittsburgh Sleep Quality Index among Pregnant Women in a Pacific-Northwest Cohort. Sleep Breath. 2016, 20, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Mindell, J.A.; Cook, R.A.; Nikolovski, J. Sleep Patterns and Sleep Disturbances across Pregnancy. Sleep Med. 2015, 16, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Chasan-Taber, L.; Schmidt, M.D.; Roberts, D.E.; Hosmer, D.; Markenson, G.; Freedson, P.S. Development and Validation of a Pregnancy Physical Activity Questionnaire. Med. Sci. Sports Exerc. 2004, 36, 1750–1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krøner, F.H.; Knudsen, S.D.P.; Roland, C.B.; Alomairah, S.A.; Molsted, S. Validity and Reliability of the Danish Version of the Pregnancy Physical Activity Questionnaire to Assess Levels of Physical Activity during Pregnancy. J. Matern. Fetal Neonatal Med. 2020, 35, 4566–4572. [Google Scholar] [CrossRef]
- Barone Gibbs, B.; Paley, J.L.; Jones, M.A.; Whitaker, K.M.; Connolly, C.P.; Catov, J.M. Validity of Self-Reported and Objectively Measured Sedentary Behavior in Pregnancy. BMC Pregnancy Childbirth 2020, 20, 99. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Aminian, S.; et al. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A Second Update of Codes and MET Values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Statistical Analysis Plan (SAP) for the FitMum Randomized Controlled Trial. Available online: https://clinicaltrials.gov/ProvidedDocs/30/NCT03679130/SAP_000.pdf (accessed on 13 November 2022).
- Garmin International. Available online: https://www.garmin.com (accessed on 13 November 2022).
- Sleep Tracking|Garmin Technology. Available online: https://www.garmin.com/en-US/garmin-technology/health-science/sleep-tracking/ (accessed on 27 January 2023).
- Liang, K.; Zeger, S.L. Longitudinal Data Analysis of Continuous and Discrete Responses for Pre-Post Designs. Sankhyā Indian J. Stat. 2000, 62, 134–148. [Google Scholar]
- van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Yang, Y.; Li, W.; Ma, T.-J.; Zhang, L.; Hall, B.J.; Ungvari, G.S.; Xiang, Y.-T. Prevalence of Poor Sleep Quality in Perinatal and Postnatal Women: A Comprehensive Meta-Analysis of Observational Studies. Front. Psychiatry 2020, 11, 161. [Google Scholar] [CrossRef] [Green Version]
- Broberg, L.; Tabor, A.; Rosthøj, S.; Backhausen, M.; Frokjaer, V.G.; Damm, P.; Hegaard, H.K. Effect of Supervised Group Exercise on Psychological Well-Being among Pregnant Women with or at High Risk of Depression (the EWE Study): A Randomized Controlled Trial. Acta Obstet. Gynecol. Scand. 2020, 100, 129–138. [Google Scholar] [CrossRef]
- Yang, S.Y.; Lan, S.J.; Yen, Y.Y.; Hsieh, Y.P.; Kung, P.T.; Lan, S.H. Effects of Exercise on Sleep Quality in Pregnant Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Asian Nurs. Res. 2020, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hyun, A.H.; Cho, J.Y.; Koo, J.H. Effect of Home-Based Tele-Pilates Intervention on Pregnant Women: A Pilot Study. Healthcare 2022, 10, 125. [Google Scholar] [CrossRef]
- Hawkins, M.; Chasan-Taber, L.; Marcus, B.; Stanek, E.; Braun, B.; Ciccolo, J.; Markenson, G. Impact of an Exercise Intervention on Physical Activity during Pregnancy: The Behaviors Affecting Baby and You Study. Am. J. Public Health 2014, 104, e74–e81. [Google Scholar] [CrossRef] [PubMed]
- Bisson, M.; Alméras, N.; Dufresne, S.S.; Robitaille, J.; Rhéaume, C.; Bujold, E.; Frenette, J.; Tremblay, A.; Marc, I. A 12-Week Exercise Program for Pregnant Women with Obesity to Improve Physical Activity Levels: An Open Randomised Preliminary Study. PLoS ONE 2015, 10, 1–17. [Google Scholar] [CrossRef]
- Talebi, E.; Mohaddesi, H.; Vahabzadeh, D.; Rasuli, J. Examination of Influence of Social Media Education through Mobile Phones on the Change in Physical Activity and Sedentary Behavior in Pregnant Women: A Randomized Controlled Trial. BMC Womens Health 2022, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, M.; Kim, Y.; Gabriel, K.P.; Rockette-Wagner, B.J.; Chasan-Taber, L. Sedentary Behavior Patterns in Non-Pregnant and Pregnant Women. Prev. Med. Rep. 2017, 6, 97. [Google Scholar] [CrossRef] [PubMed]
- Kominiarek, M.A.; Yeh, C.; Balmert, L.C.; Facco, F.; Grobman, W.; Simon, M. Sleep Duration during Pregnancy Using an Activity Tracking Device Case Report E309. Am. J. Perinatol. Rep. 2020, 10, 309–314. [Google Scholar] [CrossRef]
- Alomairah, S.A.; Knudsen, S.D.P.; Roland, C.B.; Hergel, I.-M.; Molsted, S.; Clausen, T.D.; Løkkegaard, E.; Bendix, J.M.; Maddison, R.; Löf, M.; et al. Methods to Estimate Energy Expenditure, Physical Activity, and Sedentary Time in Pregnant Women: A Validation Study Using Doubly Labeled Water. J. Meas. Phys. Behav. 2023, 1, 1–11. [Google Scholar] [CrossRef]
- Knudsen, S.D.P.; Roland, C.B.; Alomairah, S.A.; Jessen, A.D.; Molsted, S.; Clausen, T.D.; Løkkegaard, E.; Stallknecht, B.; Bønnelycke, J.; Bendix, J.M.; et al. Physical Activity in Pregnancy: A Mixed Methods Process Evaluation of the FitMum Randomised Controlled Trial Interventions. BMC Public Health 2022, 22, 1–13. [Google Scholar] [CrossRef]
- Evenson, K.R.; Spade, C.L. Review of Validity and Reliability of Garmin Activity Trackers. J. Meas. Phys. Behav. 2020, 3, 170–185. [Google Scholar] [CrossRef]
- Evenson, K.R.; Goto, M.M.; Furberg, R.D. Systematic Review of the Validity and Reliability of Consumer-Wearable Activity Trackers. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kastelic, K.; Dobnik, M.; Löfler, S.; Hofer, C.; Šarabon, N. Validity, Reliability and Sensitivity to Change of Three Consumer-Grade Activity Trackers in Controlled and Free-Living Conditions among Older Adults. Sensors 2021, 21, 6245. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, C.; de Zambotti, M. Into the Wild…the Need for Standardization and Consensus Recommendations to Leverage Consumer-Facing Sleep Technologies. Sleep 2022, 45, zsac233. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CON vs. EXE | CON vs. MOT | MOT vs. EXE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GA Week 28 | GA Week 34 | GA Week 28 | GA Week 34 | GA Week 28 | GA Week 34 | |||||||
| Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | |
| PSQI | ||||||||||||
| Global PSQI score | −0.8 [−2; −0.1] | 0.031 | −1 [−2; −0.5] | 0.002 | −0.3 [−1.0; 0.5] | 0.451 | −1.0 [−2; −0.1] | 0.026 | −0.5 [−0.1.1; 0.1] | 0.848 | −0.4 [−1.1; 0.3] | 0.309 |
| Total sleep time (h/day) | 0.06 [−0.3; 0.41] | 0.727 | 0.1 [−0.3; 0.5] | 0.702 | 0.11 [−0.24; 0.5] | 0.554 | 0.27 [−0.14; 0.7] | 0.191 | −0.04 [−0.3; 0.2] | 0.757 | −0.2 [−0.5; 0.1] | 0.234 |
| Total time in bed (h/day) | −0.20 [−0.6; 0.17] | 0.282 | −0.1 [−0.5; 0.3] | 0.637 | −0.14 [−0.5; 0.2] | 0.474 | 0.02 [−0.4; 0.4] | 0.921 | −0.1 [−0.4; 0.2] | 0.686 | −0.1 [−0.4; 0.2] | 0.469 |
| Subjective sleep quality | 0.11 [ 0.1; 0.3] | 0.340 | 0.03 [−0.24; 0.32] | 0.795 | 0.11 [−0.12; 0.35] | 0.341 | 0.1 [−0.2; 0.4] | 0.494 | −0.005 [−0.2; 0.2] | 0.961 | −0.05 [−0.30; 0.2] | 0.661 |
| Sleep efficiency (%) | 3 [−0.9; 7] | 0.133 | 3 [−2; 8] | 0.240 | 2.7 [−1.4; 6.9] | 0.199 | 3.7 [−1.3; 8.86] | 0.146 | 0.4 [−2.9; 3.8] | 0.804 | −0.8 [−4.7; 3.1] | 0.696 |
| Sleep Disturbance | −0.14 [−0.3; 0.1] | 0.164 | −0.3 [−0.5; −0.05] | 0.019 | −0.07 [−0.3; 0.1] | 0.485 | −0.14 [−0.4; 0.11] | 0.279 | −0.1 [−0.24; 0.1] | 0.388 | −0.2 [−0.3; 0.03] | 0.098 |
| Sleep Medications | −0.1 [−0.3; 0.07] | 0.246 | −0.1 [−0.3; 0.1] | 0.324 | 0.0003 [−0.2; 0.2] | 0.997 | −0.02 [−0.2; 0.15] | 0.801 | −0.1 [−0.2; 0.04] | 0.153 | −0.1 [−0.2; 0.1] | 0.344 |
| Sleep latency | −0.33 [−0.7; 0.04] | 0.077 | −0.5 [−0.8; 0.05] | 0.027 | −0.2 [−0.6; 0.1] | 0.221 | −0.21 [−0.6; 0.2] | 0.325 | −0.09 [0.4; −0.2] | 0.541 | −0.25 [−0.5; 0.04] | 0.098 |
| Daytime Dysfunction | −0.03 [−0.3; 0.2] | 0.758 | −0.3 [−0.5; 0.00] | 0.052 | 0.20 [−0.03; 0.4] | 0.095 | −0.146 [−0.43; 0.14] | 0.313 | −0.2 [−0.4; −0.04] | 0.017 | −0.13 [−0.32; 0.1] | 0.186 |
| PPAQ | ||||||||||||
| Sedentary time h/day | −0.69 [−1; −0.0] | 0.0498 | −0.05 [−1; –0.9] | 0.916 | −0.11 [−0.8; −0.6] | 0.754 | 0.1 [−0.8; −1.2] | 0.776 | −0.6 [−1.0; −0.02] | 0.042 | −0.1 [−1.0; 0.6] | 0.776 |
| CON vs. EXE | CON vs. MOT | MOT vs. EXE | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GA Week 28 | GA Week 34 | Delivery | GA Week 28 | GA Week 34 | Delivery | GA Week 28 | GA Week 34 | Delivery | ||||||||||
| Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | Differences [95% CI] | p-Value | |
| Tracker outcomes | ||||||||||||||||||
| Total sleep time (h/day) | −0.01 [−0.2; 0.2] | 0.890 | 0.05 [−0.1; 0.3] | 0.603 | −0.07 [−0.3; 0.2] | 0.573 | 0.02 [−0.2; 0.2] | 0.833 | 0.15 [−0.1; 0.4] | 0.151 | 0.1 [−0.1 to 0.4] | 0.366 | −0.03 [−0.2; 0.1] | 0.669 | −0.1 [−0.3; 0.1] | 0.247 | −0.08 [−0.4; 0.02 | 0.072 |
| Sedentary time (h/day) | 0.001 [−0.2; 0.2] | 0.993 | 0.03 [−0.3; 0.4] | 0.845 | 0.1 [−0.3; 0.4] | 0.609 | −0.1 [−0.3; 0.1] | 0.534 | −0.2 [−0.5; 0.1] | 0.234 | −0.1 [−0.5; 0.2] | 0.285 | 0.1 [−0.1; 0.2] | 0.437 | 0.2 [−0.04; 0.5] | 0.095 | 0.3 [−0.03; 0.5] | 0.053 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alomairah, S.A.; Knudsen, S.d.P.; Roland, C.B.; Molsted, S.; Clausen, T.D.; Bendix, J.M.; Løkkegaard, E.; Jensen, A.K.; Larsen, J.E.; Jennum, P.; et al. Effects of Two Physical Activity Interventions on Sleep and Sedentary Time in Pregnant Women. Int. J. Environ. Res. Public Health 2023, 20, 5359. https://doi.org/10.3390/ijerph20075359
Alomairah SA, Knudsen SdP, Roland CB, Molsted S, Clausen TD, Bendix JM, Løkkegaard E, Jensen AK, Larsen JE, Jennum P, et al. Effects of Two Physical Activity Interventions on Sleep and Sedentary Time in Pregnant Women. International Journal of Environmental Research and Public Health. 2023; 20(7):5359. https://doi.org/10.3390/ijerph20075359
Chicago/Turabian StyleAlomairah, Saud Abdulaziz, Signe de Place Knudsen, Caroline Borup Roland, Stig Molsted, Tine D. Clausen, Jane M. Bendix, Ellen Løkkegaard, Andreas Kryger Jensen, Jakob Eg Larsen, Poul Jennum, and et al. 2023. "Effects of Two Physical Activity Interventions on Sleep and Sedentary Time in Pregnant Women" International Journal of Environmental Research and Public Health 20, no. 7: 5359. https://doi.org/10.3390/ijerph20075359
APA StyleAlomairah, S. A., Knudsen, S. d. P., Roland, C. B., Molsted, S., Clausen, T. D., Bendix, J. M., Løkkegaard, E., Jensen, A. K., Larsen, J. E., Jennum, P., & Stallknecht, B. (2023). Effects of Two Physical Activity Interventions on Sleep and Sedentary Time in Pregnant Women. International Journal of Environmental Research and Public Health, 20(7), 5359. https://doi.org/10.3390/ijerph20075359