
How do Informal Caregivers of Seniors’ Tasks Lead to Presenteeism and Absenteeism Behaviors? A Canadian Quantitative Study


Abstract
:1. Introduction
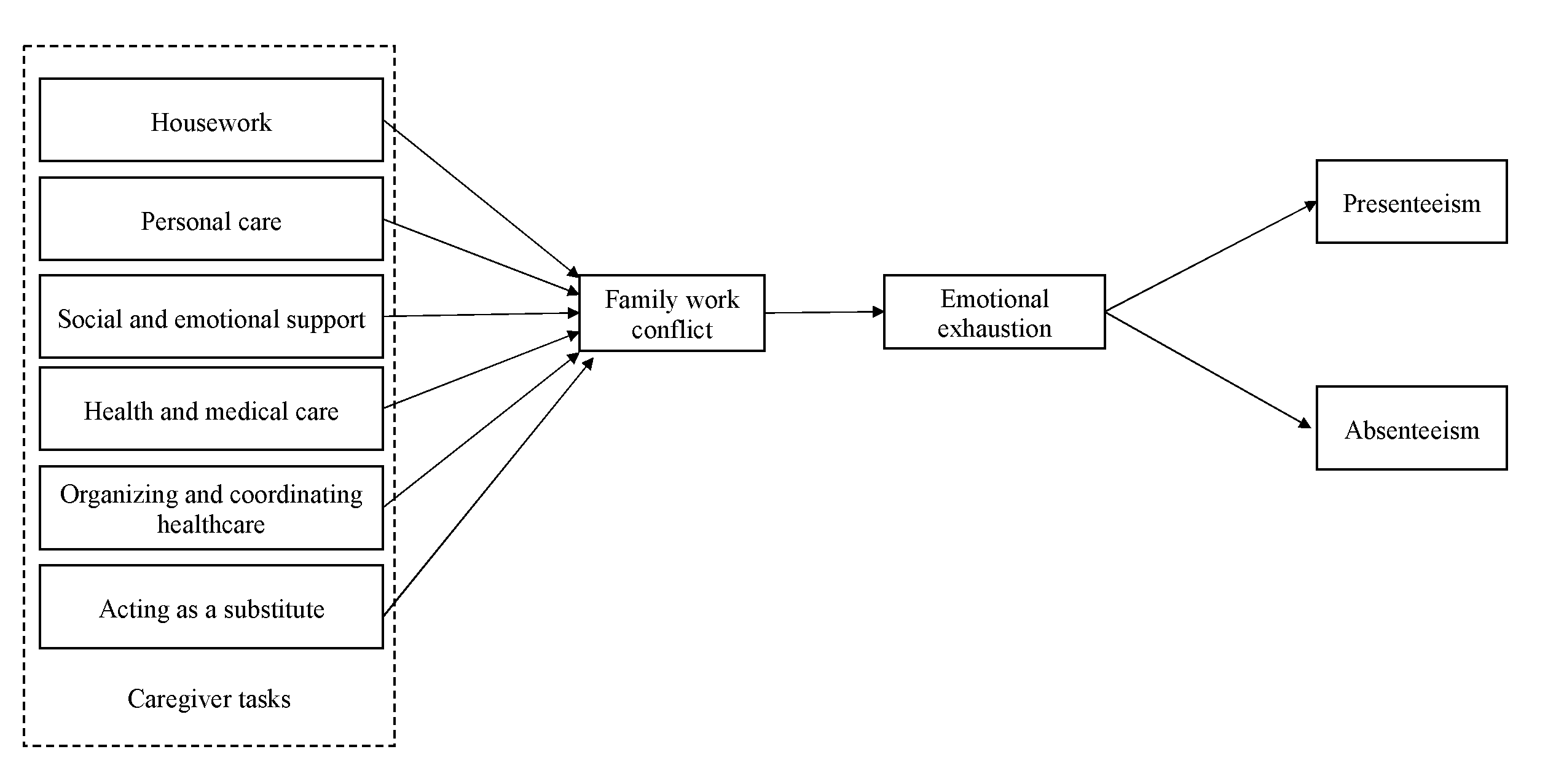
2. Theoretical Framework and Hypotheses
2.1. The Burden of Informal Caregiving
2.2. The Relationship between Informal Caregiving Role and Family–Work Conflict
2.3. The Relationship between Family–Work Conflict and Emotional Exhaustion
2.4. The Relationship between Emotional Exhaustion, Presenteeism, and Absenteeism
3. Materials and Methods
3.1. Data Collection and Sample
3.2. Descriptive Statistics and Correlations
3.3. Measures
- Independent variable
- Roles of informal senior caregivers
- Dependent variables
- Presenteeism
- Absenteeism
- Mediating variables
- Family–work conflict
- Emotional exhaustion
- Control variables:
4. Analysis
4.1. Preliminary Analyses
4.2. Data-Analysis Strategy
4.3. Measurement Model
4.3.1. CFA
4.3.2. Common Method Bias
4.3.3. Control Variables
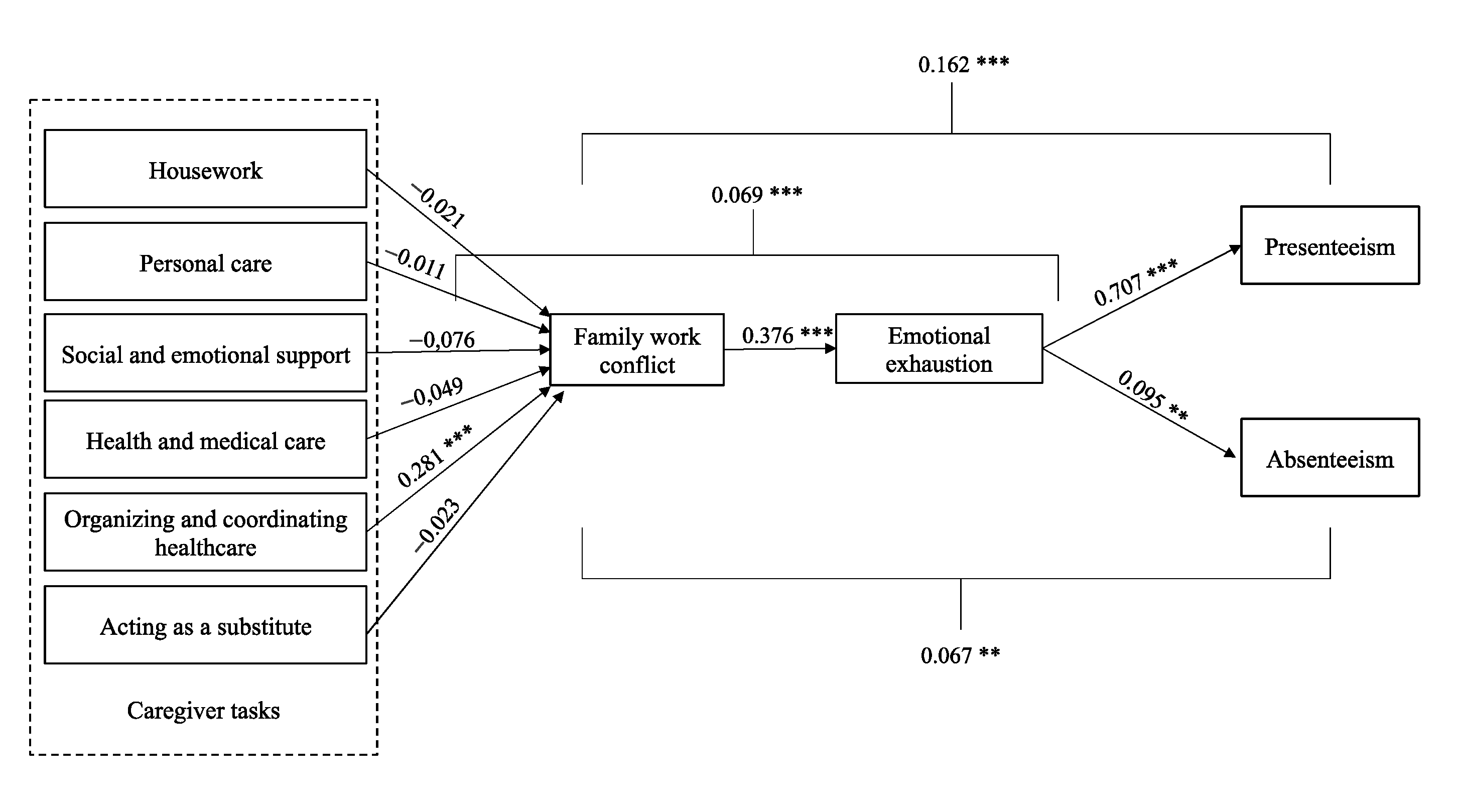
5. Results
Supplementary Analysis
6. Discussion
7. Theoretical and Practical Implications
8. Limitations
9. Future Research Directions
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Ageing and Health. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 9 January 2023).
- United Nations. World Population Prospects 2019; United Nation—Department of Economic and Social Affairs: New York, NY, USA, 2019. [Google Scholar]
- Retraite Québec. Constats sur la Retraite au Québec; Gouvernement du Québec: Québec, QC, Canada, 2016; p. 37. [Google Scholar]
- Latulipe, D.; St-Onge, S.; Gagné, C.; Ballesteros-Leiva, F.; Legault, M.-È.B. Le proongement de la vie professionnelle des Québécois: Une nécessité pour la société, les travailleurs et les employeurs? Retraite Et Société 2017, 78, 45–67. [Google Scholar]
- Hopps, M.; Iadeluca, L.; McDonald, M.; Makinson, G.T. The burden of family caregiving in the United States: Work productivity, health care resource utilization, and mental health among employed adults. J. Multidiscip. Healthc. 2017, 10, 437–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Institute for Health Information. Unpaid Caregiver Challenges and Supports. 2022. Available online: https://www.cihi.ca/en/dementia-in-canada/unpaid-caregiver-challenges-and-supports (accessed on 10 March 2020).
- Family Caregiver Alliance. Caregiver Statistics: Demographics. 2019. Available online: https://www.caregivercalifornia.org/2021/05/06/caregiver-caregiving-statistics/ (accessed on 10 March 2020).
- Statistics Canada. Informal Caregiving for Seniors. 2015. Available online: https://www150.statcan.gc.ca/n1/pub/82-003-x/2012003/article/11694-eng.htm (accessed on 10 March 2020).
- L’appui. L’appui Pour les Proches Aidants D’aînés. 2016. Available online: https://www.lappui.org/ (accessed on 15 December 2019).
- CDC. Caregiving for Family and Friends—A Public Health Issue. 2019. Available online: https://www.cdc.gov/aging/caregiving/caregiver-brief.html (accessed on 10 March 2020).
- Dumais, L. In-Home and Caregiver Support—A Necessary Philanthropic Intervention? Montréal, QC, Canada, 2018. [Google Scholar]
- Goverrnment of Canada. EI Caregiving Benefits: Do You Qualify. Available online: https://www.canada.ca/en/services/benefits/ei/caregiving/eligibility.html (accessed on 10 March 2020).
- Evans, C.J. Health and work productivity assessment: State of the art or state of flux? J. Occup. Environ. Med. 2004, 46 (Suppl. 6), S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Johansson, G.; Lundberg, I. Adjustment Latitude and Attendance Requirements as Determinants of Sickness Absence or Attendance. Empirical Tests of the Illness Flexibility Model. Soc. Sci. Med. 2004, 58, 1857–1868. [Google Scholar] [CrossRef] [PubMed]
- Vézina, M.; Cloutier, E.; Stock, S.; Lippel, K.; Fortin, E.; Delisle, A.; St-Vincent, M.; Funes, A.; Duguay, P.; Vézina, S.; et al. Enquête Québécoise sur les Conditions de Travail, D’emploi et de Santé et de Sécurité du Travail (EQCOTESST); Institut de Recherche Robert-Sauvé en Santé et Sécurité du Travail—Institut National de Santé Publique du Québec et Institut de la Statistique du du Québec: Québec, QC, Canada, 2011. [Google Scholar]
- Folger, J. The Causes and Costs of Absenteeism. 2021. Available online: https://www.investopedia.com/articles/personal-finance/070513/causes-and-costs-absenteeism.asp (accessed on 3 September 2022).
- Zuba, M.; Schneider, U. What helps working informal caregivers? The role of workplace characteristics in balancing work and adult-care responsibilities. J. Fam. Econ. Issues 2013, 34, 460–469. [Google Scholar] [CrossRef]
- Zacher, H.; Schulz, H. Employees’ eldercare demands, strain, and perceived support. J. Manag. Psychol. 2015, 30, 183–198. [Google Scholar] [CrossRef]
- Greenhaus, J.H.; Beutell, N.J. Sources of Conflict between Work and Family Roles. Acad. Manag. Rev. 1985, 10, 76–88. [Google Scholar] [CrossRef]
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Feinberg, L.; Reinhard, S.C.; Houser, A.; Choula, R. Valuing the Invaluable: 2011 Update, the Growing Contributions and Costs of Family Caregiving; AARP Public Policy Institute: Washington, DC, USA, 2011; Volume 32, p. 2011. [Google Scholar]
- The National Alliance for Caregiving (NARC). Caregiving in the U.S. 2015; AART Public Policy Institute: Philadelphia, PA, USA, 2015. [Google Scholar]
- Lecours, C. Portrait des Proches Aidants et les Conséquences de Leurs Responsabilités D’aidant; Institut de la Statistique du Québec: Québec, QC, Canada, 2015. [Google Scholar]
- Schulz, R.; Tompkins, C.A. Informal Care. In The Role of Human Factors in Home Health Care: Workshop Summary; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Ferrara, M.; Langiano, E.; Di Brango, T.; Di Cioccio, L.; Bauco, C.; De Vito, E. Prevalence of stress, anxiety and depression in with Alzheimer caregivers. Health Qual. Life Outcomes 2008, 6, 93. [Google Scholar] [CrossRef] [Green Version]
- Bevans, M.; Sternberg, E.M. Caregiving burden, stress, and health effects among family caregivers of adult cancer patients. JAMA 2012, 307, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Grandey, A.A.; Cropanzano, R. The Conservation of Resources Model Applied to Work–Family Conflict and Strain. J. Vocat. Behav. 1999, 54, 350–370. [Google Scholar] [CrossRef] [Green Version]
- Truzzi, A.; Valente, L.; Ulstein, I.; Engelhardt, E.; Laks, J.; Engedal, K. Burnout in Familial Caregivers of Patients with Dementia; Elsevier Science: Amsterdam, The Netherlands, 2012; Volume 34. [Google Scholar]
- St-Armour, N.; Leverdure, J.; Devault, A.; Manseau, S. La Difficulté de Concilier Travail-Famille: Ses Impacts sur la Santé Physique et Mentale des Familles Québécoises; Institut National de Santé Publique du Québec: Québec, QC, Canada, 2005. [Google Scholar]
- Davis, K.D.; Gere, J.; Sliwinski, M.J. Investigating the work–family conflict and health link: Repetitive thought as a mechanism. Stress Health 2017, 33, 330–338. [Google Scholar] [CrossRef] [PubMed]
- McDaniel, K.R.; Allen, D.G. Working and Care-giving: The Impact on Caregiver Stress, Family-Work Conflict, and Burnout. J. Life Care Plan. 2012, 10, 21–32. [Google Scholar] [CrossRef]
- Alarcon, G.M. A meta-analysis of burnout with job demands, resources, and attitudes. J. Vocat. Behav. 2011, 79, 549–562. [Google Scholar] [CrossRef]
- Bowling, N.A.; Alarcon, G.M.; Bragg, C.B.; Hartman, M.J. A meta-analytic examination of the potential correlates and consequences of workload. Work Stress 2015, 29, 95–113. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Halbesleben, J.; Neveu, J.-P.; Westman, M. Conservation of resources in the organizational context: The reality of resources and their consequences. Annu. Rev. Organ. Psychol. Organ. Behav. 2018, 5, 103–128. [Google Scholar] [CrossRef] [Green Version]
- Mazanec, S.R.; Daly, B.J.; Douglas, S.L.; Lipson, A.R. Work productivity and health of informal caregivers of persons with advanced cancer. Res. Nurs. Health 2011, 34, 483–495. [Google Scholar] [CrossRef]
- Demerouti, E.; Blanc, P.M.; Schaufeli, W.; Hox, J. Present but sick: A three-wave study on job demands, presenteeism and burnout. Career Dev. Int. 2009, 14, 50–68. [Google Scholar] [CrossRef] [Green Version]
- Clancy, R.L.; Fisher, G.G.; Daigle, K.L.; Henle, C.A.; McCarthy, J.; Fruhauf, C.A. Eldercare and Work Among Informal Caregivers: A Multidisciplinary Review and Recommendations for Future Research. J. Bus. Psychol. 2020, 35, 9–27. [Google Scholar] [CrossRef]
- Vignoli, M.; Guglielmi, D.; Bonfiglioli, R.; Violante, F.S. How job demands affect absenteeism? The mediating role of work–family conflict and exhaustion. Int. Arch. Occup. Environ. Health 2016, 89, 23–31. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Van Rhenen, W. How changes in job demands and resources predict burnout, work engagement, and sickness absenteeism. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2009, 30, 893–917. [Google Scholar] [CrossRef] [Green Version]
- Roelen, C.; Van Hoffen, M.; Groothoff, J.; De Bruin, J.; Schaufeli, W.; Van Rhenen, W. Can the Maslach Burnout Inventory and Utrecht Work Engagement Scale be used to screen for risk of long-term sickness absence? Int. Arch. Occup. Environ. Health 2015, 88, 467–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brislin, R.W. Translation and content analysis of oral and written material. In Handbook of Cross-Cultural Psychology; Triandis, H.C., Brislin, R.W., Eds.; Library of Congress Cataloging-in-Publication Data: Boston, UK, 1980. [Google Scholar]
- Turpin, R.S.; Ozminkowski, R.J.; Sharda, C.E.; Collins, J.J.; Berger, M.L.; Billotti, G.M.; Baase, C.M.; Olson, M.J.; Nicholson, S. Reliability and validity of the Stanford Presenteeism Scale. J. Occup. Environ. Med. 2004, 46, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Gutek, B.A.; Searle, S.; Klepa, L. Rational versus gender role explanations for work-family conflict. J. Appl. Psychol. 1991, 76, 560–568. [Google Scholar] [CrossRef]
- Halinski, M.; Duxbury, L.; Stevenson, M. Employed Caregivers’ Response to Family-Role Overload: The Role of Control-at-Home and Caregiver Type. J. Bus. Psychol. 2020, 35, 99–115. [Google Scholar] [CrossRef]
- Gareth, J.; Daniela, W.; Trevor, H.; Robert, T. An Introduction to Statistical Learning: With Applications in R.; Spinger: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Hu, L.-t.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Podsakoff, N.P. Sources of Method Bias in Social Science Research and Recommendations on How to Control It. Annu. Rev. Psychol. 2012, 63, 539–569. [Google Scholar] [CrossRef] [Green Version]
- Golden, S.; Nageswaran, S. Caregiver Voices: Coordinating Care for Children with Complex Chronic Conditions. Clin. Pediatr. 2012, 51, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Boles, M.; Pelletier, B.; Lynch, W. The Relationship Between Health Risks and Work Productivity. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2004, 46, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Hemp, P. Presenteeism: At work-but out of it. Harv. Bus. Rev. 2004, 82, 49–58. [Google Scholar]
- Karanika-Murray, M.; Biron, C. The health-performance framework of presenteeism: Towards understanding an adaptive behaviour. Hum. Relat. 2019, 73, 242–261. [Google Scholar] [CrossRef] [Green Version]
- Van den Broeck, A.; Ferris, D.L.; Chang, C.-H.; Rosen, C.C. A Review of Self-Determination Theory’s Basic Psychological Needs at Work. J. Manag. 2016, 42, 1195–1229. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Demerouti, E.; De Boer, E.; Schaufeli, W.B. Job demands and job resources as predictors of absence duration and frequency. J. Vocat. Behav. 2003, 62, 341–356. [Google Scholar] [CrossRef]
- Maxwell, S.E.; Cole, D.A. Bias in cross-sectional analyses of longitudinal mediation. Psychol. Methods 2007, 12, 23–44. [Google Scholar] [CrossRef] [Green Version]
- Stratton, S.J. Population Research: Convenience Sampling Strategies. Prehospital Disaster Med. 2021, 36, 373–374. [Google Scholar] [CrossRef]
- Evans, J.R.; Mathur, A. The value of online surveys. Internet Res. 2005, 15, 195–219. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Task | Definition |
|---|---|
| Housework | Doing laundry, meals, house maintenance, etc. |
| Personal care | Bathing, toileting, dressing, feeding, supervising the elderly, and helping the person move around. |
| Social and Emotional Support | Providing presence, talking with the person, organizing and participating in leisure activities, managing family conflicts, problem-solving, and managing emotions. |
| Health and Medical Care | Encouraging healthy lifestyles, promoting adherence to treatment, managing and administering medications, using medical equipment, preparing meals according to a specific diet, responding to emergencies, and providing care. |
| Organizing and coordinating healthcare | Seeking information, promoting understanding, communicating with healthcare professionals, coordinating the various stakeholders, making appointments, renewing prescriptions, negotiating with insurance companies, etc. |
| Acting as a substitute | Dealing with legal and financial issues, managing personal assets, and participating in treatment planning and decisions. |
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Gender | - | - | - | ||||||||||||
| 2. Age | 43.80 | 11.09 | 0.141 ** | 1 | |||||||||||
| 3. Number of dependents | 1.67 | 1.41 | −0.058 * | −0.025 | 1 | ||||||||||
| 4. Housework tasks | 2.98 | 3.39 | −0.039 | 0.144 ** | −0.007 | 1 | |||||||||
| 5. Personal care tasks | 1.69 | 2.59 | −0.013 | 0.123 ** | 0.019 | 0.614 ** | 1 | ||||||||
| 6. Social and emotional support tasks | 3.75 | 3.60 | 0.089 ** | 0.096 ** | −0.009 | 0.531 ** | 0.475 ** | 1 | |||||||
| 7. Health and medical care tasks | 1.76 | 2.43 | 0.068 * | 0.148 ** | 0.024 | 0.515 ** | 0.652 ** | 0.550 ** | 1 | ||||||
| 8. Organization and coordination of health care tasks | 1.54 | 2.21 | 0.076 * | 0.162 ** | 0.020 | 0.485 ** | 0.651 ** | 0.513 ** | 0.784 ** | 1 | |||||
| 9. Acting as a substitute tasks | 1.54 | 2.35 | 0.068 * | 0.144 ** | 0.028 | 0.467 ** | 0.579 ** | 0.461 ** | 0.654 ** | 0.765 ** | 1 | ||||
| 10. Family-work conflict | 1.30 | 0.68 | −0.033 | −0.048 | 0.184 ** | 0.103 ** | 0.146 ** | 0.155 ** | 0.173 ** | 0.239 ** | 0.173 ** | 1 | (0.77) | ||
| 11. Emotional exhaustion | 2.45 | 1.43 | 0.020 | 0.004 | −0.014 | 0.065 * | 0.060 * | 0.119 ** | 0.100 ** | 0.104 ** | 0.084 ** | 0.359 ** | 1 | (0.91) | |
| 12. Presenteeism | 1.11 | 0.40 | 0.072 * | −0.028 | 0.030 | 0.011 | 0.040 | 0.109 ** | 0.082 ** | 0.110 ** | 0.087 ** | 0.348 ** | 0.733 ** | 1 | (0.84) |
| 13. Absenteeism | 1.34 | 1.28 | 0.211 ** | 0.049 | 0.119 ** | 0.077 * | 0.165 ** | 0.125 ** | 0.272 ** | 0.298 ** | 0.294 ** | 0.230 ** | 0.112 ** | 0.214 ** | 1 |
| Tasks | Mean (Hours/Month) | SD |
|---|---|---|
| Housework | 2.98 | 3.39 |
| Personal care | 1.69 | 2.59 |
| Social and emotional support | 3.75 | 3.60 |
| Health and medical care | 1.76 | 2.43 |
| Organizing and coordinating healthcare | 1.54 | 2.21 |
| Acting as a substitute | 1.54 | 2.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beauchamp Legault, M.-È.; Chênevert, D.; Maisonneuve, F.; Mansour, S. How do Informal Caregivers of Seniors’ Tasks Lead to Presenteeism and Absenteeism Behaviors? A Canadian Quantitative Study. Int. J. Environ. Res. Public Health 2023, 20, 5392. https://doi.org/10.3390/ijerph20075392
Beauchamp Legault M-È, Chênevert D, Maisonneuve F, Mansour S. How do Informal Caregivers of Seniors’ Tasks Lead to Presenteeism and Absenteeism Behaviors? A Canadian Quantitative Study. International Journal of Environmental Research and Public Health. 2023; 20(7):5392. https://doi.org/10.3390/ijerph20075392
Chicago/Turabian StyleBeauchamp Legault, Marie-Ève, Denis Chênevert, Francis Maisonneuve, and Sari Mansour. 2023. "How do Informal Caregivers of Seniors’ Tasks Lead to Presenteeism and Absenteeism Behaviors? A Canadian Quantitative Study" International Journal of Environmental Research and Public Health 20, no. 7: 5392. https://doi.org/10.3390/ijerph20075392
APA StyleBeauchamp Legault, M. -È., Chênevert, D., Maisonneuve, F., & Mansour, S. (2023). How do Informal Caregivers of Seniors’ Tasks Lead to Presenteeism and Absenteeism Behaviors? A Canadian Quantitative Study. International Journal of Environmental Research and Public Health, 20(7), 5392. https://doi.org/10.3390/ijerph20075392