
Potential Relationship between Poor Oral Hygiene and MRONJ: An Observational Retrospective Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
Assumptions
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Advisory Task Force on Bisphosphonate-Related Ostenonecrosis of the Jaws, American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2007, 65, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Carlson, E.R.; Assael, L.A. Comprehensive review of bisphosphonate therapy: Implications for the oral and maxillofacial surgery patient. J. Oral Maxillofac. Surg. 2009, 67 (Suppl. 5), 1. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related oste-onecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956, Erratum in J. Oral Maxillofac. Surg. 2015, 73, 1440; Erratum in J. Oral Maxillofac. Surg. 2015, 73, 1879. [Google Scholar] [CrossRef]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Schiødt, M.; Mendes, R.A.; Ripamonti, C.; Hope, S.; Drudge-Coates, L.; Niepel, D.; Van den Wyngaert, T. Medication-related osteonecrosis of the jaw: Definition and best practice for prevention, diagnosis, and treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 117–135. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, S.; Gralow, J.; Marx, R.E.; Hoff, A.O.; Schubert, M.M.; Huryn, J.M.; Toth, B.; Damato, K.; Valero, V. Practical guidelines for the prevention, diagnosis, and treatment of osteonecrosis of the jaw in patients with cancer. J. Oncol. Pract. 2006, 2, 7–14. [Google Scholar] [CrossRef]
- Tempesta, A.; Capodiferro, S.; Di Nanna, S.; D’Agostino, S.; Dolci, M.; Scarano, A.; Gambarini, G.; Maiorano, E.; Favia, G.; Limongelli, L. Medication-related osteonecrosis of the jaw triggered by endodontic failure in oncologic patients. Oral Dis. 2022, 20. Online ahead of print. [Google Scholar] [CrossRef]
- Lorenzo-Pouso, A.I.; Pérez-Sayáns, M.; Chamorro-Petronacci, C.; Gándara-Vila, P.; López-Jornet, P.; Carballo, J.; Gar-cía-García, A. Association between periodontitis and medication-related osteonecrosis of the jaw: A systematic review and meta-analysis. J. Oral Pathol. Med. 2020, 49, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.P.; Katsarelis, H.; Pazianas, M.; Dhariwal, D.K. Periodontal Disease, Dental Implants, Extractions and Medications Related to Osteonecrosis of the Jaws. Dent. Update 2015, 42, 878–880, 883–884, 887–889. [Google Scholar] [CrossRef]
- Avishai, G.; Muchnik, D.; Masri, D.; Zlotogorski-Hurvitz, A.; Chaushu, L. Minimizing MRONJ after Tooth Extraction in Cancer Patients Receiving Bone-Modifying Agents. J. Clin. Med. 2022, 11, 1807. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, recognition, prevention, and treatment. J. Oral Maxillofac. Surg. 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- Kos, M. Association of dental and periodontal status with bisphosphonate-related osteonecrosis of the jaws. A retrospective case controlled study. Arch. Med. Sci. 2014, 10, 117–123. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxil-lofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws-2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef]
- Mawardi, H.; Giro, G.; Kajiya, M.; Ohta, K.; Almazrooa, S.; Alshwaimi, E.; Woo, S.B.; Nishimura, I.; Kawai, T. A role of oral bacteria in bisphosphonate-induced osteonecrosis of the jaw. J. Dent. Res. 2011, 90, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Mücke, T.; Krestan, C.R.; Mitchell, D.A.; Kirschke, J.S.; Wutzl, A. Bisphosphonate and Medication-Related Osteonecrosis of the Jaw: A Review. Semin. Musculoskelet. Radiol. 2016, 20, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Poxleitner, P.; Engelhardt, M.; Schmelzeisen, R.; Voss, P. The Prevention of Medication-related Osteonecrosis of the Jaw. Dtsch Arztebl. Int. 2017, 114, 63–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pittman, K.; Antill, Y.C.; Goldrick, A.; Goh, J.; de Boer, R.H. Denosumab: Prevention and management of hypocalcemia, os-teonecrosis of the jaw and atypical fractures. Asia Pac. J. Clin. Oncol. 2017, 13, 266–276. [Google Scholar] [CrossRef] [Green Version]
- Vandone, A.M.; Donadio, M.; Mozzati, M.; Ardine, M.; Polimeni, M.A.; Beatrice, S.; Ciuffreda, L.; Scoletta, M. Impact of dental care in the prevention of bisphosphonate-associated osteonecrosis of the jaw: A single-center clinical experience. Ann. Oncol. 2012, 23, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Krimmel, M.; Ripperger, J.; Hairass, M.; Hoefert, S.; Kluba, S.; Reinert, S. Does dental and oral health influence the development and course of bisphosphonate-related osteonecrosis of the jaws (BRONJ)? Oral Maxillofac. Surg. 2014, 18, 213–218. [Google Scholar] [CrossRef]
- Bonacina, R.; Mariani, U.; Villa, F.; Villa, A. Preventive strategies and clinical implications for bisphosphonate-related osteonecrosis of the jaw: A review of 282 patients. J. Can. Dent. Assoc. 2011, 77, b147. [Google Scholar]
- Yamamoto, N.; Sukegawa, S.; Sukegawa-Takahashi, Y.; Honda, T.; Furuki, Y.; Kawasaki, K.; Ozaki, T. Relationship between oral condition and risk factors for jaw osteonecrosis in patients with hip fractures. J. Med. Investig. 2020, 67, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Al Abdullateef, A.; Alhareky, M.S. Awareness among patient at risk of developing Medication Related Osteonecrosis of the Jaw (MRONJ)—A primary prevention strategy. Saudi Pharm. J. 2020, 28, 771–778. [Google Scholar] [CrossRef]
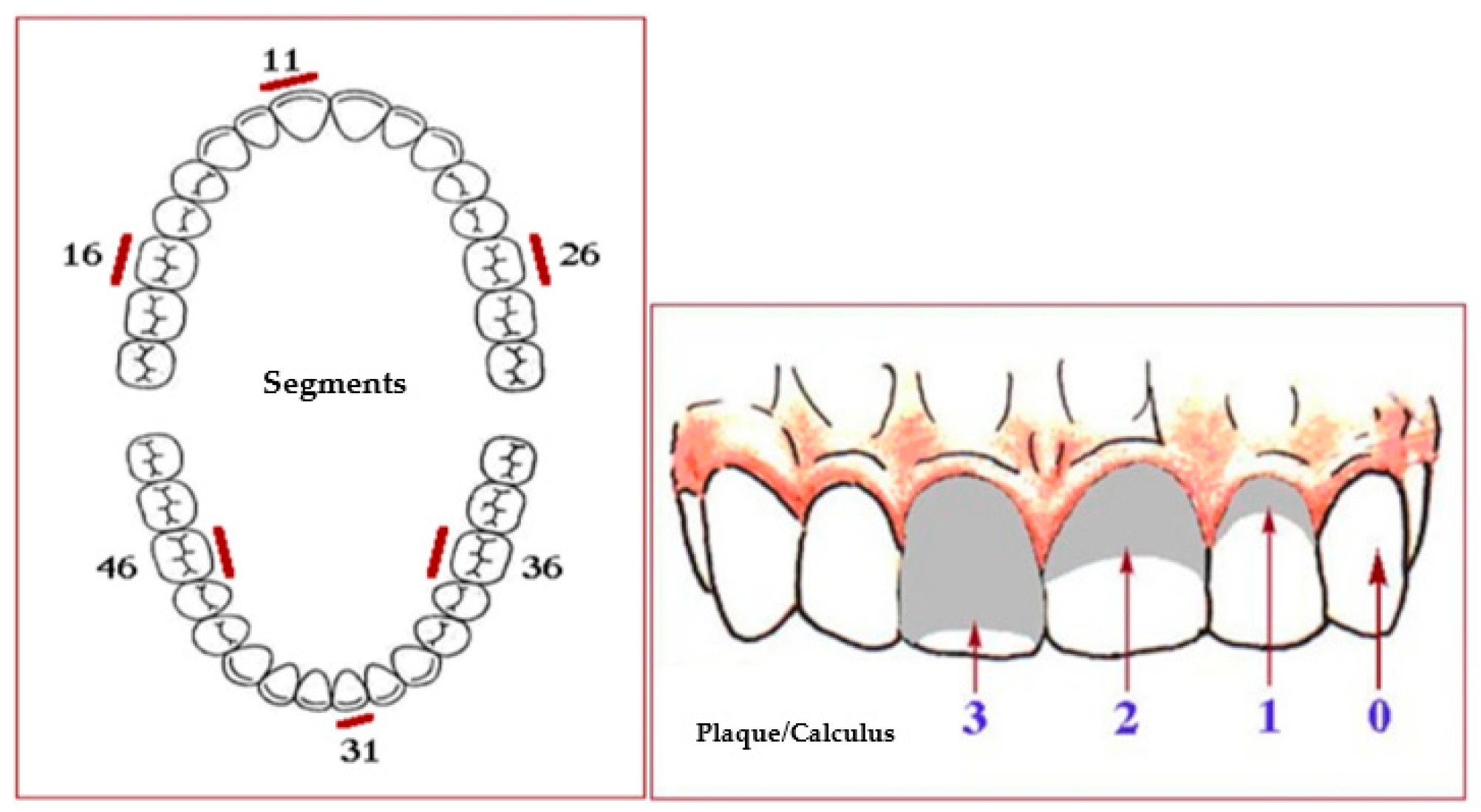
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- Fregatto, L.F.; Costa, I.B.; De Bortoli Teixeira, D.; Duarte, J.C.M.; Mascarin, A.M.N.; da Silveira Junior, S.B.; Serva, B.E.B.M.; da Silva, R.G.; Junior, F.A.; Cola, P.C. Oral hygiene and oral microbiota in children and young people with neurological im-pairment and oropharyngeal dysphagia. Sci. Rep. 2021, 11, 18090. [Google Scholar] [CrossRef]
- Preshaw, P.M. Detection and diagnosis of periodontal conditions amenable to prevention. BMC Oral Health 2015, 15 (Suppl. 1), S5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Al-Nawas, B.; Grötz, K.A.; Thomas, C.; Thüroff, J.W.; Zinser, V.; Gamm, H.; Beck, J.; Wagner, W. Prevalence and risk factors of bisphosphonate-associated osteonecrosis of the jaw in prostate cancer patients with advanced disease treated with zoledronate. Eur. Urol. 2008, 54, 1066–1072. [Google Scholar] [CrossRef]
- Carmagnola, D.; Celestino, S.; Abati, S. Dental and periodontal history of oncologic patients on parenteral bisphosphonates with or without osteonecrosis of the jaws: A pilot study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, e10–e15. [Google Scholar] [CrossRef]
- Kunchur, R.; Goss, A.N. The oral health status of patients on oral bisphosphonates for osteoporosis. Aust. Dent. J. 2008, 53, 354–357; quiz 366. [Google Scholar] [CrossRef]
- Diniz-Freitas, M.; Fernández-Feijoo, J.; Diz Dios, P.; Pousa, X.; Limeres, J. Denosumab-related osteonecrosis of the jaw following non-surgical periodontal therapy: A case report. J. Clin. Periodontol. 2018, 45, 570–577. [Google Scholar] [CrossRef]
- Zheng, Y.; Dong, X.; Chen, S.; He, Y.; An, J.; Liu, M.; He, L.; Zhang, Y. Low-level laser therapy prevents medication-related osteonecrosis of the jaw-like lesions via IL-1RA-mediated primary gingival wound healing. BMC Oral Health 2023, 23, 14. [Google Scholar] [CrossRef]
- Torres, A.A.; de Freitas, B.L.; Carneiro, P.P.; de Sousa, A.L.A.; Arêa Leão Ferraz, M.Â.; de Pinho Mendes, J.; Costa, A.L.F.; Pinto, A.S.B. Medication-Related Osteonecrosis of the Jaw and Low-Level Laser Therapy as Adjuvant Treatment: A Case Report. J. Lasers Med. Sci. 2020, 11, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Momesso, G.A.C.; Lemos, C.A.A.; Santiago-Júnior, J.F.; Faverani, L.P.; Pellizzer, E.P. Laser surgery in management of medi-cation-related osteonecrosis of the jaws: A meta-analysis. Oral Maxillofac. Surg. 2020, 24, 133–144. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S1–S8. [Google Scholar] [CrossRef]
- Bodem, J.P.; Kargus, S.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Value of nonsurgical therapeutic management of stage I bisphosphonate-related osteonecrosis of the jaw. J. Craniomaxillofac. Surg. 2015, 43, 1139–1143. [Google Scholar] [CrossRef]
- Momesso, G.A.C.; de Souza Batista, F.R.; de Sousa, C.A.; de Lima, V.N.; Polo, T.O.B.; Hassumi, J.S.; Garcia Júnior, I.R.; Fa-verani, L.P. Successful Use of Lower-Level Laser Therapy in the Treatment of Medication-Related Osteonecrosis of the Jaw. J. Lasers Med. Sci. 2017, 8, 201–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, S.; Miccoli, S.; Limongelli, L.; Tempesta, A.; Favia, G.; Maiorano, E.; Favia, G. New dimensional staging of bisphos-phonate-related osteonecrosis of the jaw allowing a guided surgical treatment protocol: Long-term follow-up of 266 lesions in neoplastic and osteoporotic patients from the university of bari. Int. J. Dent. 2014, 2014, 935657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, L.; Sun, X.; Liu, Z.; Qiu, Y.; Niu, Y. Pathogenesis and multidisciplinary management of medication-related osteonecrosis of the jaw. Int. J. Oral Sci. 2020, 12, 30. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Localization | ||
| Upper jaw + lower jaw | 10 | 22.22 |
| Upper jaw | 21 | 46.67 |
| Lower jaw | 14 | 31.11 |
| AAOMS_Stage_1 | ||
| (−Inf, 1] | 3 | 6.67 |
| (1, 2] | 31 | 68.89 |
| (2, 3] | 11 | 24.44 |
| (3, Inf] | 0 | 0.00 |
| Drug | ||
| Zoledronic acid | 32 | 71.11 |
| +Alendronic acid | 1 | 2.22 |
| Alendronic acid | 6 | 13.33 |
| Monoclonal antibodies | 6 | 12.11 |
| Variable | M | SD | SEM | Min | Max | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|
| OHI-S | 3.39 | 1.83 | 0.27 | 1.10 | 6.00 | 0.27 | −1.48 |
| AAOMS_Stage | 2.13 | 0.55 | 0.11 | 1.00 | 3.00 | 0.10 | 0.23 |
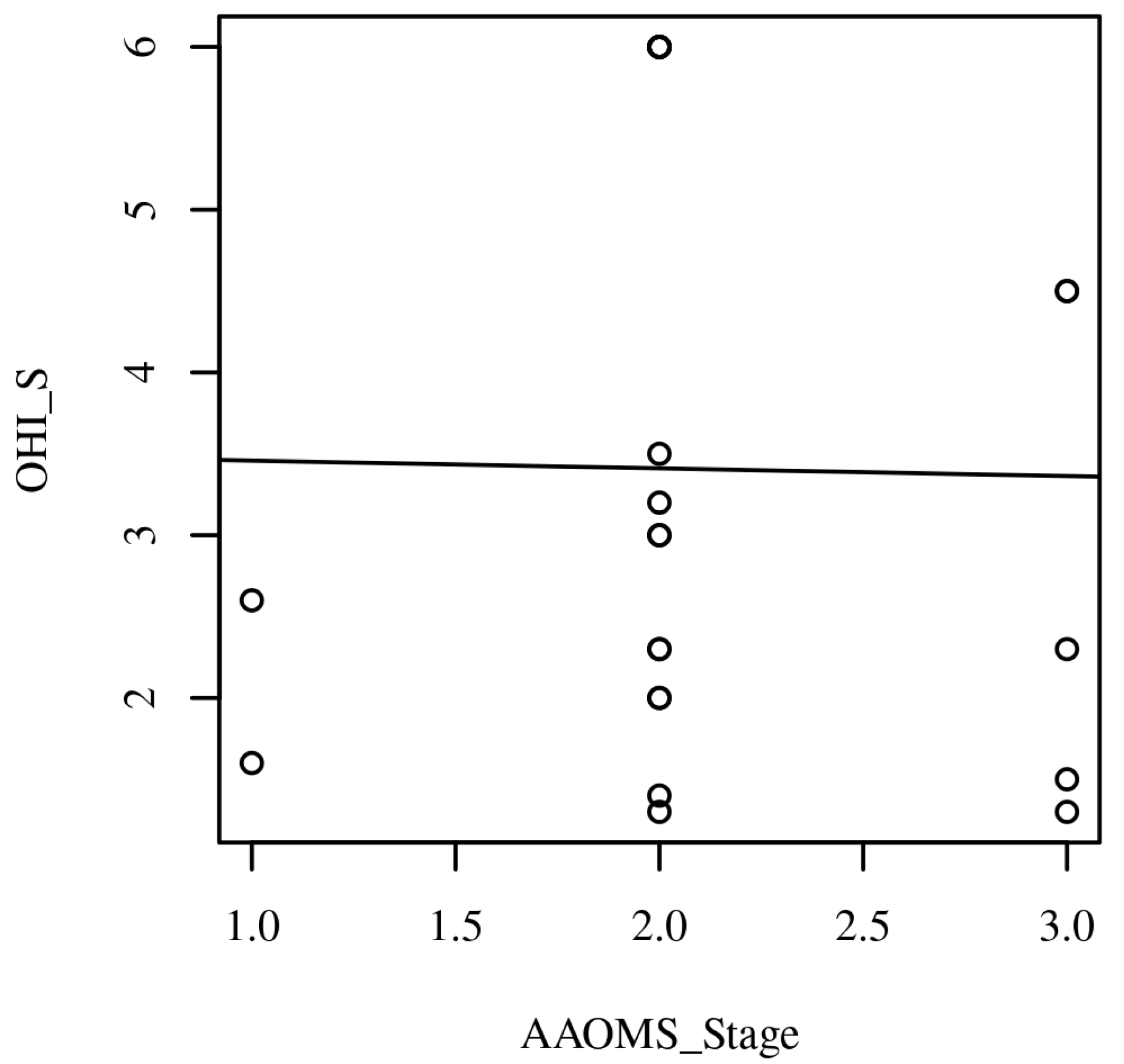
| Combination | r | 95.00% CI | p |
|---|---|---|---|
| AAOMS_Stage-OHI-S | −0.01 | [−0.42, 0.40] | 0.948 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Agostino, S.; Valentini, G.; Dolci, M.; Ferrara, E. Potential Relationship between Poor Oral Hygiene and MRONJ: An Observational Retrospective Study. Int. J. Environ. Res. Public Health 2023, 20, 5402. https://doi.org/10.3390/ijerph20075402
D’Agostino S, Valentini G, Dolci M, Ferrara E. Potential Relationship between Poor Oral Hygiene and MRONJ: An Observational Retrospective Study. International Journal of Environmental Research and Public Health. 2023; 20(7):5402. https://doi.org/10.3390/ijerph20075402
Chicago/Turabian StyleD’Agostino, Silvia, Giulia Valentini, Marco Dolci, and Elisabetta Ferrara. 2023. "Potential Relationship between Poor Oral Hygiene and MRONJ: An Observational Retrospective Study" International Journal of Environmental Research and Public Health 20, no. 7: 5402. https://doi.org/10.3390/ijerph20075402
APA StyleD’Agostino, S., Valentini, G., Dolci, M., & Ferrara, E. (2023). Potential Relationship between Poor Oral Hygiene and MRONJ: An Observational Retrospective Study. International Journal of Environmental Research and Public Health, 20(7), 5402. https://doi.org/10.3390/ijerph20075402