
The SUCCESS Peer Mentoring Program for College Students with Concussion: Preliminary Results of a Mobile Technology Delivered Intervention


Abstract
:1. Introduction
1.1. Peer Mentoring in a Neurobiopsychosocial Model of Concussion
1.2. mHealth Peer Mentoring
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.2.1. Mentor Training
2.2.2. Matching
2.2.3. Educational Resources
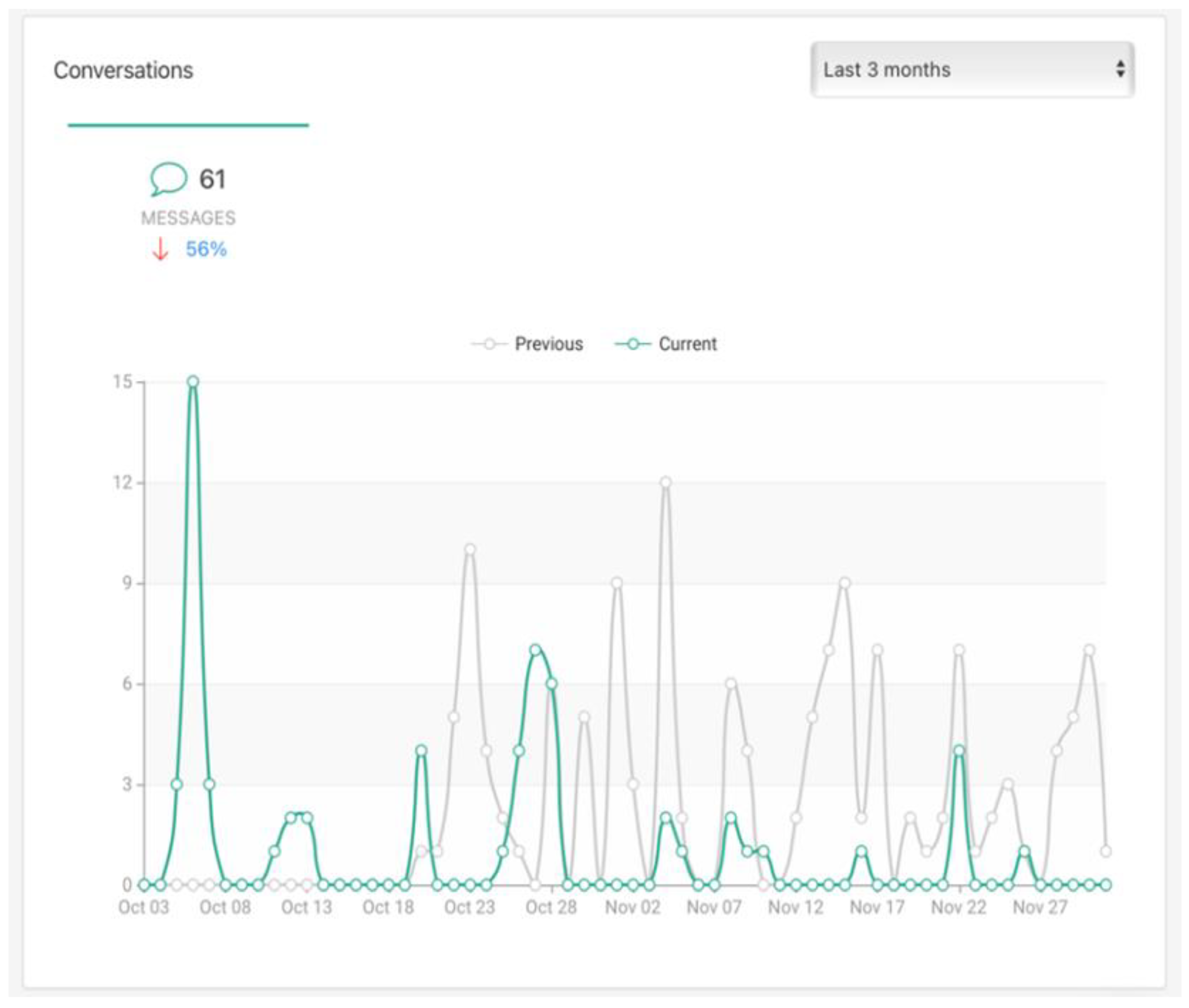
2.2.4. In-App Mentoring
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Mentees
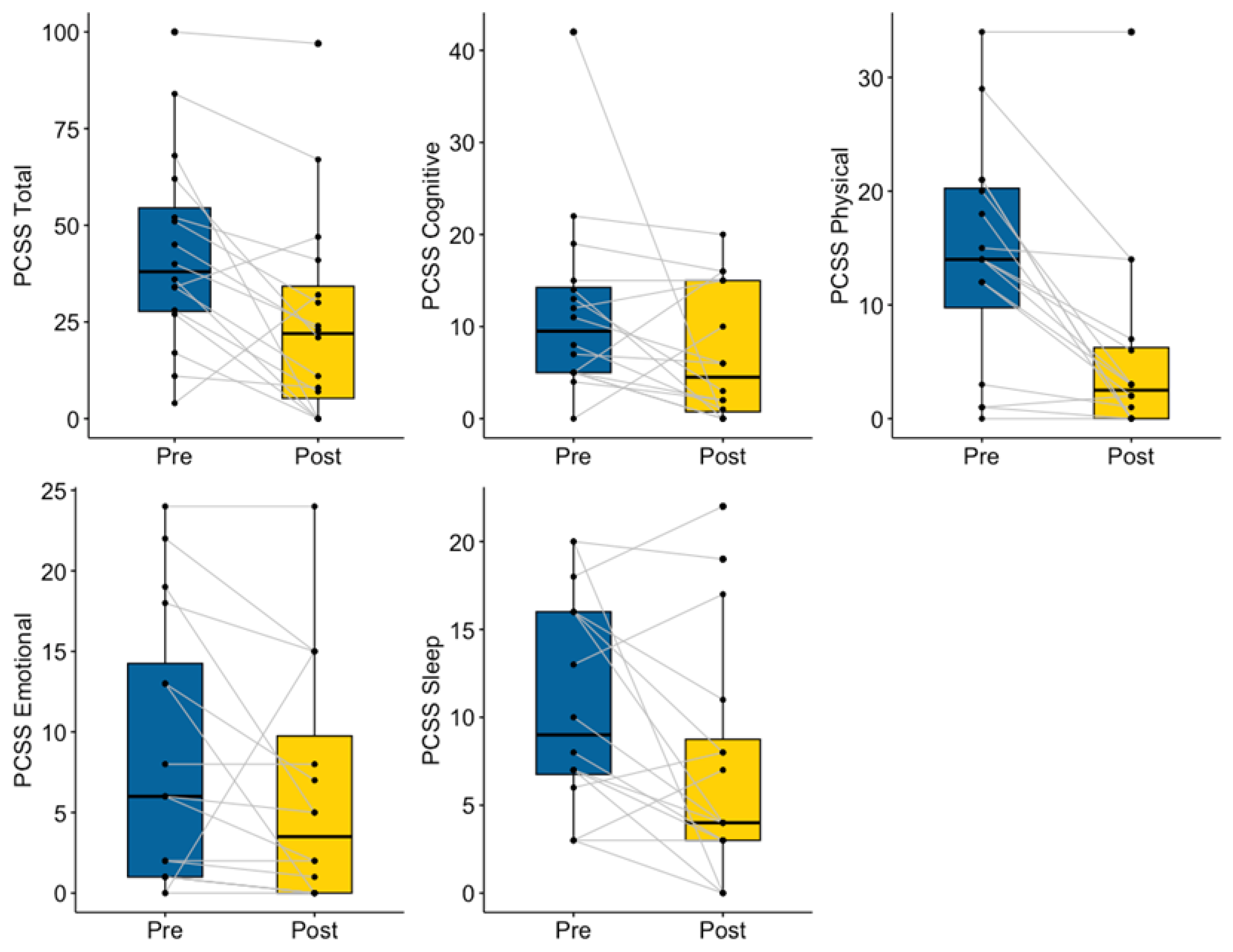
3.1.1. Concussion Symptoms
3.1.2. Academics
3.1.3. Psychosocial Function
3.1.4. Mentee Post-Intervention Feedback Survey
3.2. Mentors
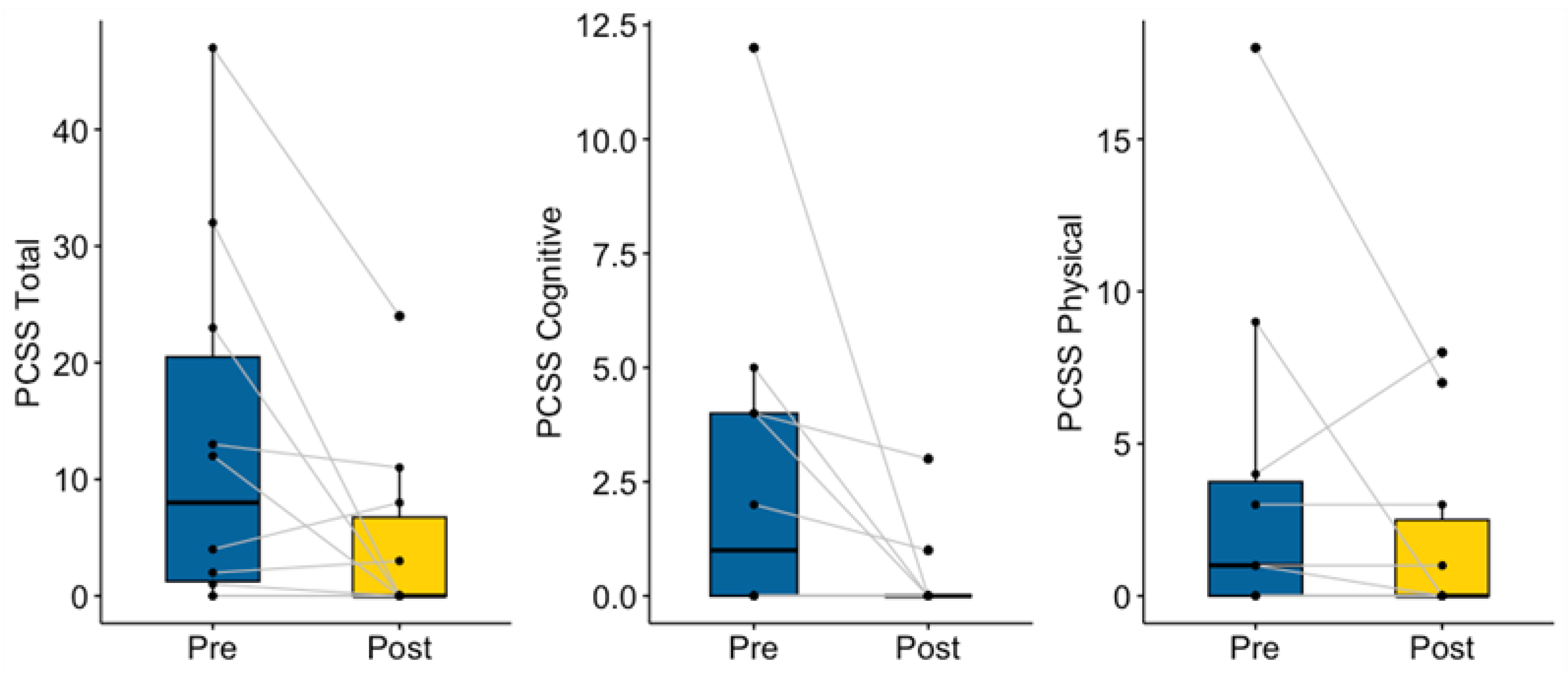
3.2.1. Concussion Symptoms
3.2.2. Psychosocial Function
3.2.3. Mentor Post-Intervention Feedback Survey
4. Discussion
4.1. Concussion, Academic, and Psychosocial Outcomes
4.2. Program Acceptability
4.3. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bryan, M.A.; Rowhani-Rahbar, A.; Comstock, R.D.; Rivara, F. On behalf of the Seattle Sports Concussion Research Collaborative Sports- and Recreation-Related Concussions in US Youth. Pediatrics 2016, 138, e20154635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breck, J.; Bohr, A.; Poddar, S.; McQueen, M.B.; Casault, T. Characteristics and Incidence of Concussion Among a US Collegiate Undergraduate Population. JAMA Netw. Open 2019, 2, e1917626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hux, K.; Brown, J.; Lambert, M. Latent Class Analysis of Brain Injury Symptomatology among College Students. Curr. Res. Concussion 2017, 4, e14–e22. [Google Scholar] [CrossRef] [Green Version]
- Krause, M.; Richards, S. Prevalence of Traumatic Brain Injury and Access to Services in an Undergraduate Population: A Pilot Study. Brain Inj. 2014, 28, 1301–1310. [Google Scholar] [CrossRef] [PubMed]
- Scopaz, K.A.; Hatzenbuehler, J.R. Risk Modifiers for Concussion and Prolonged Recovery. Sport. Health A Multidiscip. Approach 2013, 5, 537–541. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, N.D.; Iaccarino, M.A.; Panenka, W.J.; Iverson, G.L.; McCulloch, K.L.; Dams-O’Connor, K.; Reed, N.; McCrea, M.; Cogan, A.M.; Park Graf, M.J.; et al. Management of Concussion and Mild Traumatic Brain Injury: A Synthesis of Practice Guidelines. Arch. Phys. Med. Rehabil. 2020, 101, 382–393. [Google Scholar] [CrossRef] [Green Version]
- Lumba-Brown, A.; Yeates, K.O.; Sarmiento, K.; Breiding, M.J.; Haegerich, T.M.; Gioia, G.A.; Turner, M.; Benzel, E.C.; Suskauer, S.J.; Giza, C.C.; et al. Diagnosis and Management of Mild Traumatic Brain Injury in Children: A Systematic Review. JAMA Pediatr. 2018, 172, e182847. [Google Scholar] [CrossRef]
- Marshall, S.; Baley, M.; McCullagh, S.; Berrigan, L.; Fischer, L.; Ouchterlony, D.; Rockwell, C.; Velikonja, D. Guideline for Concussion/Mild Traumatic Brain Injury and Persistent Symptoms, 3rd ed.; (for Adults 18+ Years of Age); Ontario Neurotrauma Foundation: Toronto, ON, Canada, 2018. [Google Scholar]
- Babcock, L.; Byczkowski, T.; Wade, S.L.; Ho, M.; Mookerjee, S.; Bazarian, J.J. Predicting Postconcussion Syndrome After Mild Traumatic Brain Injury in Children and Adolescents Who Present to the Emergency Department. JAMA Pediatr. 2013, 167, 156. [Google Scholar] [CrossRef] [Green Version]
- Machamer, J.; Temkin, N.; Dikmen, S.; Nelson, L.D.; Barber, J.; Hwang, P.; Boase, K.; Stein, M.B.; Sun, X.; Giacino, J.; et al. Symptom Frequency and Persistence in the First Year after Traumatic Brain Injury: A TRACK-TBI Study. J. Neurotrauma 2022, 39, 358–370. [Google Scholar] [CrossRef]
- Madhok, D.Y.; Rodriguez, R.M.; Barber, J.; Temkin, N.R.; Markowitz, A.J.; Kreitzer, N.; Manley, G.T.; TRACK-TBI Investigators; Badjatia, N.; Duhaime, A.-C.; et al. Outcomes in Patients With Mild Traumatic Brain Injury Without Acute Intracranial Traumatic Injury. JAMA Netw. Open 2022, 5, e2223245. [Google Scholar] [CrossRef]
- Bevilacqua, Z.W.; Kerby, M.E.; Fletcher, D.; Chen, Z.; Merritt, B.; Huibregtse, M.E.; Kawata, K. Preliminary Evidence-Based Recommendations for Return to Learn: A Novel Pilot Study Tracking Concussed College Students. Concussion 2019, 4, CNC63. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, E.B.; Bazarian, J.J.; Mapstone, M.; Block, R.; van Wijngaarden, E. Academic Dysfunction After a Concussion Among US High School and College Students. Am. J. Public Health 2016, 106, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.N.; Lempke, L.B.; Johnson, R.S.; Lynall, R.C.; Schmidt, J.D. Concussion Characteristics and Early Postinjury Outcomes Between College Students and Intercollegiate Athletes. Arch. Phys. Med. Rehabil. 2022, 103, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Childers, C.; Hux, K. Invisible Injuries: The Experiences of College Students with Histories of Mild Traumatic Brain Injury. J. Postsecond. Educ. Disabil. 2016, 29, 389–405. [Google Scholar]
- Moreau, M.S.; Langdon, J.L.; Buckley, T.A. The Lived Experience of an In-Season Concussion Amongst NCAA Division I Student-Athletes. Int. J. Exerc. Sci. 2014, 7, 62–74. [Google Scholar]
- Pei, Y.; O’Brien, K.H. Reading Abilities Post Traumatic Brain Injury in Adolescents and Adults: A Systematic Review and Meta-Analysis. Am. J. Speech Lang. Pathol. 2021, 30, 789–816. [Google Scholar] [CrossRef]
- Kontos, A.P.; Deitrick, J.M.; Collins, M.W.; Mucha, A. Review of Vestibular and Oculomotor Screening and Concussion Rehabilitation. J. Athl. Train. 2017, 52, 256–261. [Google Scholar] [CrossRef] [Green Version]
- Torres, D.M.; Galetta, K.M.; Phillips, H.W.; Dziemianowicz, E.M.S.; Wilson, J.A.; Dorman, E.S.; Laudano, E.; Galetta, S.L.; Balcer, L.J. Sports-Related Concussion: Anonymous Survey of a Collegiate Cohort. Neurol. Clin. Pract. 2013, 3, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Magasi, S.; Papadimitriou, C. Peer Support Interventions in Physical Medicine and Rehabilitation: A Framework to Advance the Field. Arch. Phys. Med. Rehabil. 2022, 103, S222–S229. [Google Scholar] [CrossRef]
- Griffin, M.M.; Wendel, K.F.; Day, T.L.; McMillan, E.D. Developing Peer Supports for College Students with Intellectual and Developmental Disabilities. J. Postsecond. Educ. Disabil. 2016, 29, 263–269. [Google Scholar]
- Morris, R.P.; Fletcher-Smith, J.C.; Radford, K.A. A Systematic Review of Peer Mentoring Interventions for People with Traumatic Brain Injury. Clin. Rehabil. 2017, 31, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Stanish, H.I.; Temple, V.A. Efficacy of a Peer-guided Exercise Programme for Adolescents with Intellectual Disability. J. Appl. Res. Intellect. Disabil. 2012, 25, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Wobma, R.; Nijland, R.H.M.; Ket, J.C.F.; Kwakkel, G. Evidence for Peer Support in Rehabilitation for Individuals with Acquired Brain Injury: A Systematic Review. J. Rehabil. Med. 2016, 48, 837–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durish, C.L.; Yeates, K.O.; Brooks, B.L. Psychological Resilience as a Predictor of Symptom Severity in Adolescents With Poor Recovery Following Concussion. J. Int. Neuropsychol. Soc. 2019, 25, 346–354. [Google Scholar] [CrossRef]
- Kreutzer, J.S.; Marwitz, J.H.; Sima, A.P.; Bergquist, T.F.; Johnson-Greene, D.; Felix, E.R.; Whiteneck, G.G.; Dreer, L.E. Resilience Following Traumatic Brain Injury: A Traumatic Brain Injury Model Systems Study. Arch. Phys. Med. Rehabil. 2016, 97, 708–713. [Google Scholar] [CrossRef]
- Hibbard, M.R.; Cantor, J.; Charatz, H.; Rosenthal, R.; Ashman, T.; Gundersen, N.; Ireland-Knight, L.; Gordon, W.; Avner, J.; Gartner, A. Peer Support in the Community: Initial Findings of a Mentoring Program for Individuals with Traumatic Brain Injury and Their Families. J. Head Trauma Rehabil. 2002, 17, 112–131. [Google Scholar] [CrossRef]
- Northcott, S.; Behn, N.; Monnelly, K.; Moss, B.; Marshall, J.; Thomas, S.; Simpson, A.; McVicker, S.; Flood, C.; Goldsmith, K.; et al. “For Them and for Me”: A Qualitative Exploration of Peer Befrienders’ Experiences Supporting People with Aphasia in the SUPERB Feasibility Trial. Disabil. Rehabil. 2022, 44, 5025–5037. [Google Scholar] [CrossRef]
- Gassaway, J.; Jones, M.L.; Sweatman, W.M.; Young, T. Peer-Led, Transformative Learning Approaches Increase Classroom Engagement in Care Self-Management Classes during Inpatient Rehabilitation of Individuals with Spinal Cord Injury. J. Spinal Cord Med. 2019, 42, 338–346. [Google Scholar] [CrossRef]
- Lorig, K.; Ritter, P.L.; Villa, F.J.; Armas, J. Community-Based Peer-Led Diabetes Self-Management: A Randomized Trial. Diabetes Educ. 2009, 35, 641–651. [Google Scholar] [CrossRef]
- Willis, E. Patients’ Self-Efficacy within Online Health Communities: Facilitating Chronic Disease Self-Management Behaviors through Peer Education. Health Commun. 2016, 31, 299–307. [Google Scholar] [CrossRef]
- Gassaway, J.; Jones, M.L.; Sweatman, W.M.; Hong, M.; Anziano, P.; DeVault, K. Effects of Peer Mentoring on Self-Efficacy and Hospital Readmission After Inpatient Rehabilitation of Individuals With Spinal Cord Injury: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 98, 1526–1534.e2. [Google Scholar] [CrossRef] [PubMed]
- Ernst, W.; Kneavel, M.E. Development of a Peer Education Program to Improve Concussion Knowledge and Reporting in Collegiate Athletes. J. Athl. Train. 2020, 55, 448–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kneavel, M.E.; Ernst, W.; McCarthy, K.S. Randomized Controlled Trial of a Novel Peer Concussion-Education Program for Collegiate Athletes. J. Athl. Train. 2020, 55, 456–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youth Concussion Awareness Network (You-CAN) Team; Hickling, A.; Mallory, K.D.; Wilson, K.E.; Del Fernandes, R.; Fuselli, P.; Reed, N. The Youth Concussion Awareness Network (You-CAN)—A School-Based Peer-Led Intervention to Improve Concussion Reporting and Social Support: The Protocol for a Cluster Randomized Trial. BMC Public Health 2020, 20, 186. [Google Scholar] [CrossRef] [Green Version]
- Yeates, K.O. Mild Traumatic Brain Injury and Postconcussive Symptoms in Children and Adolescents. J. Int. Neuropsychol. Soc. 2010, 16, 953–960. [Google Scholar] [CrossRef] [Green Version]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; von Steinbuechel, N. A Multidimensional Approach to Post-Concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pei, Y.; Kemp, A.M.; O’Brien, K.H. Investigating the Student in Returning to Learn after Concussion: A Systematic Review and Meta-Analysis. J. Sch. Health 2023, in press. [Google Scholar] [CrossRef]
- Kita, H.; Mallory, K.D.; Hickling, A.; Wilson, K.E.; Kroshus, E.; Reed, N. Social Support during Youth Concussion Recovery. Brain Inj. 2020, 34, 784–792. [Google Scholar] [CrossRef] [Green Version]
- Northcott, S.; Simpson, A.; Thomas, S.; Barnard, R.; Burns, K.; Hirani, S.P.; Hilari, K. “Now I Am Myself”: Exploring How People With Poststroke Aphasia Experienced Solution-Focused Brief Therapy Within the SOFIA Trial. Qual. Health Res. 2021, 31, 2041–2055. [Google Scholar] [CrossRef]
- Belch, H.A. Retention and Students with Disabilities. J. Coll. Stud. Retent. Res. Theory Pract. 2004, 6, 3–22. [Google Scholar] [CrossRef]
- Macnow, T.; Curran, T.; Tolliday, C.; Martin, K.; McCarthy, M.; Ayturk, D.; Babu, K.M.; Mannix, R. Effect of Screen Time on Recovery From Concussion: A Randomized Clinical Trial. JAMA Pediatr. 2021, 175, 1124. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.J.; Boles, S.; Derksen, V.; Dawyduk, B.; Amadu, A.; Stelmack, K.; Kowalchuk, M.; Russell, K. Evaluation of a Pilot Paediatric Concussion Telemedicine Programme for Northern Communities in Manitoba. Int. J. Circumpolar Health 2019, 78, 1573163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas, B.B.; Shepard, M.; Hentz, J.G.; Kutyreff, C.; Hershey, L.G.; Starling, A.J. Feasibility and Accuracy of Teleconcussion for Acute Evaluation of Suspected Concussion. Neurology 2017, 88, 1580–1583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belanger, H.G.; Toyinbo, P.; Barrett, B.; King, E.; Sayer, N.A. Concussion Coach for Postconcussive Symptoms: A Randomized, Controlled Trial of a Smartphone Application with Afghanistan and Iraq War Veterans. Clin. Neuropsychol. 2022, 36, 2093–2119. [Google Scholar] [CrossRef] [PubMed]
- Chrisman, S.P.D.; Mendoza, J.A.; Zhou, C.; Palermo, T.M.; Gogue-Garcia, T.; Janz, K.F.; Rivara, F.P. Pilot Study of Telehealth Delivered Rehabilitative Exercise for Youth With Concussion: The Mobile Subthreshold Exercise Program (MSTEP). Front. Pediatr. 2021, 9, 645814. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.; Plourde, V.; Hartling, L.; Scott, S.D. “You Can’t Fix Your Brain”: Exploring Concussion Experiences of Children and Parents. J. Spec. Pediatr. Nurs. 2022, 27, e12357. [Google Scholar] [CrossRef]
- O’Brien, K.H.; Wallace, T.; Kemp, A. Student Perspectives on the Role of Peer Support Following Concussion: Development of the SUCCESS Peer Mentoring Program. Am. J. Speech Lang. Pathol. 2021, 30, 933–948. [Google Scholar] [CrossRef]
- Kemp, A.; Pei, Y.; O’Brien, K.; Wallace, T. Success in College after Concussion with Effective Student Supports (SUCCESS): Persona Testing of a Peer Mentoring Program. Arch. Phys. Med. Rehabil. 2021, 102, e55. [Google Scholar] [CrossRef]
- Kemp, A.; Gartell, R.; O’Brien, K.; Wallace, T.; Pei, Y. Infographic Development for the Success in College after Concussion with Effective Student Supports (SUCCESS) Peer Mentoring Program. Arch. Phys. Med. Rehabil. 2021, 102, e55. [Google Scholar] [CrossRef]
- Lovell, M.R.; Collins, M.W. Neuropsychological Assessment of the College Football Player. J. Head Trauma Rehabil. 1998, 13, 9–26. [Google Scholar] [CrossRef]
- Owen, S.V.; Froman, R.D. Development of a College Academic Self-Efficacy Scale. In Proceedings of the Annual Meeting of the National Council on Measurement in Education, New Orleans, LA, USA, 6–8 April 1988. [Google Scholar]
- Ader, D.N. Developing the Patient-Reported Outcomes Measurement Information System (PROMIS). Med. Care 2007, 45, S1–S2. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Tulsky, D.S.; Kisala, P.A.; Victorson, D.; Carlozzi, N.; Bushnik, T.; Sherer, M.; Choi, S.W.; Heinemann, A.W.; Chiaravalloti, N.; Sander, A.M.; et al. TBI-QOL: Development and Calibration of Item Banks to Measure Patient Reported Outcomes Following Traumatic Brain Injury. J. Head Trauma Rehabil. 2016, 31, 40–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fordal, L.; Stenberg, J.; Iverson, G.L.; Saksvik, S.B.; Karaliute, M.; Vik, A.; Olsen, A.; Skandsen, T. Trajectories of Persistent Postconcussion Symptoms and Factors Associated With Symptom Reporting After Mild Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2022, 103, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Desai, N.; Wiebe, D.J.; Corwin, D.J.; Lockyer, J.E.; Grady, M.F.; Master, C.L. Factors Affecting Recovery Trajectories in Pediatric Female Concussion. Clin. J. Sport Med. 2019, 29, 361–367. [Google Scholar] [CrossRef]
- Valera, E.M.; Joseph, A.-L.C.; Snedaker, K.; Breiding, M.J.; Robertson, C.L.; Colantonio, A.; Levin, H.; Pugh, M.J.; Yurgelun-Todd, D.; Mannix, R.; et al. Understanding Traumatic Brain Injury in Females: A State-of-the-Art Summary and Future Directions. J. Head Trauma Rehabil. 2021, 36, E1–E17. [Google Scholar] [CrossRef]
- Krisi, M.; Nagar, R. The Effect of Peer Mentoring on Mentors Themselves: A Case Study of College Students. Int. J. Disabil. Dev. Educ. 2021, 1–13. [Google Scholar] [CrossRef]
- Brown, S.E.; Takahashi, K.; Roberts, K.D. Mentoring Individuals with Disabilities in Postsecondary Education: A Review of the Literature. J. Postsecond. Educ. Disabil. 2010, 23, 98–111. [Google Scholar]
- pcori. PCORI’s Process for Peer Review of Primary Research and Public Release of Research Findings. 2015. Available online: https://www.pcori.org/resources/pcoris-process-peer-review-primary-research-and-public-release-research-findings (accessed on 1 February 2023).
- Sheridan, M.A.; Peverill, M.; Finn, A.S.; McLaughlin, K.A. Dimensions of Childhood Adversity Have Distinct Associations with Neural Systems Underlying Executive Functioning. Dev. Psychopathol. 2017, 29, 1777–1794. [Google Scholar] [CrossRef] [Green Version]
- Mittenberg, W.; Tremont, G.; Zielinski, R.E.; Fichera, S.; Rayls, K.R. Cognitive-Behavioral Prevention of Postconcussion Syndrome. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 1996, 11, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Arnett, J.J. Emerging Adulthood: What Is It, and What Is It Good For? Child Dev. Perspect. 2007, 1, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Tucker, K.; Sharp, G.; Qingmin, S.; Scinta, T.; Thanki, S. Fostering Historically Underserved Students’ Success: An Embedded Peer Support Model That Merges Non-Cognitive Principles with Proven Academic Support Practices. Rev. High. Educ. 2020, 43, 861–885. [Google Scholar] [CrossRef]
- Gregg, N.; Galyardt, A.; Wolfe, G.; Moon, N.; Todd, R. Virtual Mentoring and Persistence in STEM for Students With Disabilities. Career Dev. Transit. Except. Individ. 2017, 40, 205–214. [Google Scholar] [CrossRef]
- Dennis, J.M.; Phinney, J.S.; Chuateco, L.I. The Role of Motivation, Parental Support, and Peer Support in the Academic Success of Ethnic Minority First-Generation College Students. J. Coll. Stud. Dev. 2005, 46, 223–236. [Google Scholar] [CrossRef]
- Whiteman, S.D.; Barry, A.E.; Mroczek, D.K.; MacDermid Wadsworth, S. The Development and Implications of Peer Emotional Support for Student Service Members/Veterans and Civilian College Students. J. Couns. Psychol. 2013, 60, 265–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaughan, C.G.; Ledoux, A.-A.; Sady, M.D.; Tang, K.; Yeates, K.O.; Sangha, G.; Osmond, M.H.; Freedman, S.B.; Gravel, J.; Gagnon, I.; et al. Association Between Early Return to School Following Acute Concussion and Symptom Burden at 2 Weeks Postinjury. JAMA Netw. Open 2023, 6, e2251839. [Google Scholar] [CrossRef]
- Kemp, A.M.; O’Brien, K.H.; Wallace, T. Reconceptualizing Recovery After Concussion: A Phenomenological Exploration of College Student Experiences. Am. J. Speech Lang. Pathol. 2023, 32, 867–882. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Gender | Race | Class Standing | Total Number of Concussions | Time Post Injury (Months) | Injury Mechanism | Program Chat Usage * | |
|---|---|---|---|---|---|---|---|---|
| Mentee | ||||||||
| PR1 | 25 | M | White | Graduate | 1 | 5 | Sports/Rec | 28 |
| PR2 | 22 | F | White | Senior | 1 | 4 | MVC | 77 |
| PR3 | 21 | F | Asian | Graduate | 0 | 5 | MVC | 31 |
| PR4 | 21 | M | White | Senior | 4 | 2.5 | Struck By | 43 |
| PR5 | 26 | F | White | Graduate | 3 | 3 | Struck By | 29 |
| PR6 | 20 | F | White | Junior | 1 | 1 | Sports/Rec | 49 |
| PR7 | 25 | F | White | Graduate | 3 | 0.5 | MVC | 21 |
| PR8 | 21 | M | White | Junior | 4+ | 2 | Struck By | 8 |
| PR9 | 18 | F | White | Freshman | 2 | 3 | Sports/Rec | 25 |
| PR10 | 21 | F | White | Junior | 1 | 12 | Sports/Rec | 27 |
| PR11 | 19 | F | White | Sophomore | 3+ | 1 | Sports/Rec | 54 |
| PR12 | 20 | F | Black | Junior | 1 | 7 | Sports/Rec | 10 |
| PR13 | 21 | F | Black | Junior | 1 | 3 | Struck By | 12 |
| PR14 | 20 | F | Asian | Junior | 1 | 7 | Sports/Rec | 18 |
| PR15 | 19 | F | Black | Sophomore | 1 | 1 | Struck By | 31 |
| PR16 | 20 | M | White | Senior | 2 | 2 | Sports/Rec | 23 |
| Mentor | ||||||||
| MR1 | 23 | F | White | Senior | 1 | 21 | Struck By | |
| MR2 | 20 | F | Black | Junior | 1 | 14 | Struck By | |
| MR3 | 22 | F | White | Senior | 2 | 21 | Sports/Rec | |
| MR4 | 22 | M | Asian | New graduate (under-graduate) | 3 | 7 | MVC, Sports/Rec, Struck By | |
| MR5 | 20 | F | White | Junior | 2+ | 23 | Sports/Rec | |
| MR6 | 21 | NB | White | Senior | 2+ | 31 | Sports/Rec | |
| MR7 | 25 | F | White | New graduate (under-graduate) | 2+ | 24 | Sports/Rec | |
| MR8 | 23 | F | White | New graduate (under-graduate) | 3 | 8 | Sports/Rec | |
| MR9 | 23 | F | White | Junior | 0 | 24 | MVC | |
| MR10 | 24 | M | White | Senior | 5 | 42 | Sports/Rec | |
| MR11 | 21 | F | White | Junior | 0 | 12 | MVC | |
| Measurement Tools | Domain | Description |
|---|---|---|
| Post-Concussion Symptom Scale (PCSS) [51] | Concussion Symptoms | 22 item self-report of presence and severity of concussion symptoms. |
| Academic Dysfunction Survey (ADS) [13] | Academics | 29 item survey of self-reported academic problems post-concussion. |
| College and Academic Self-Efficacy Scale (CASES) [52] | Psychosocial Function: Academic Self-Efficacy | 19 item self-report of confidence about completing academic tasks, and in likelihood of success as a student. |
| Patient Reported Outcome Measurement Information System (PROMIS) Self-Efficacy Instruments [53] | Psychosocial Function: General Self-Efficacy | 10 item survey used to assess patient-reported health status for physical, mental, and social well–being. |
| Depression, Anxiety, Stress Scale (DASS) [54] | Psychosocial Function: Mental Health | 42 item scale assessing mental health domains. |
| Traumatic Brain Injury Quality of Life Scale (TBI-QoL) [55] | Psychosocial Function: Quality of Life | 10 item survey of participation in academic, vocational, and social activities (adapted to add academics). |
| Post-Mentoring Feedback Survey | Program and App Usage | Survey of program and app feedback with 8 open ended questions and 7 sliding scale (6 for mentors) questions asking participants to rank either the likelihood of recommending the program to a mentee or a mentor (2 questions) and helpfulness (5 questions for mentees, 4 for mentors) of the app or program features. |
| App Usage Data | Use of communication features (chat, videoconferencing) by frequency and type. |
| Item | Mean | Median | Range |
|---|---|---|---|
| How likely would you be to recommend this program to a friend to become a Mentee if they sustained a concussion? (n = 14) (0 = not at all likely; 100 = definitely recommend) | 86.86 | 94 | 50–100 |
| How likely would you be to recommend this program to a friend to become a Mentor if they had already recovered from a concussion? (n = 13) (0 = not at all likely; 100 = definitely recommend) | 89.38 | 92 | 50–100 |
| How helpful were each of the following? (0 = not at all; 100 = very helpful) | |||
| Support provided by your Peer Mentor (n = 14) | 96.07 | 100 | 77–100 |
| SUCCESS Program Handouts (n = 11) | 70 | 72 | 19–100 |
| The App (n = 9) | 62.89 | 60 | 17–100 |
| The SUCCESS Team (n = 12) | 81.08 | 80.5 | 52–100 |
| Participating in the SUCCESS Program (n = 13) | 90 | 96 | 56–100 |
| Item | Mean | Median | Range |
|---|---|---|---|
| How likely would you be to recommend this program to a friend to become a Mentee if they sustained a concussion? (0 = not at all likely; 100 = definitely) | 96.6 | 100 | 75–100 |
| How likely would you be to recommend this program to a friend to become a Mentor if they had already recovered from a concussion? (0 = not at all likely; 100 = definitely) | 93.7 | 100 | 75–100 |
| How helpful were each of the following? (0 = not at all; 100 = very helpful) | |||
| SUCCESS training | 87.5 | 93 | 50–100 |
| SUCCESS Program Handouts | 78.7 | 78.5 | 50–100 |
| The App | 76.3 | 90 | 26–100 |
| The SUCCESS Team | 99.2 | 100 | 97–100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Brien, K.H.; Pei, Y.; Kemp, A.M.; Gartell, R.; Gore, R.K.; Wallace, T. The SUCCESS Peer Mentoring Program for College Students with Concussion: Preliminary Results of a Mobile Technology Delivered Intervention. Int. J. Environ. Res. Public Health 2023, 20, 5438. https://doi.org/10.3390/ijerph20085438
O’Brien KH, Pei Y, Kemp AM, Gartell R, Gore RK, Wallace T. The SUCCESS Peer Mentoring Program for College Students with Concussion: Preliminary Results of a Mobile Technology Delivered Intervention. International Journal of Environmental Research and Public Health. 2023; 20(8):5438. https://doi.org/10.3390/ijerph20085438
Chicago/Turabian StyleO’Brien, Katy H., Yalian Pei, Amy M. Kemp, Rebecca Gartell, Russell K. Gore, and Tracey Wallace. 2023. "The SUCCESS Peer Mentoring Program for College Students with Concussion: Preliminary Results of a Mobile Technology Delivered Intervention" International Journal of Environmental Research and Public Health 20, no. 8: 5438. https://doi.org/10.3390/ijerph20085438
APA StyleO’Brien, K. H., Pei, Y., Kemp, A. M., Gartell, R., Gore, R. K., & Wallace, T. (2023). The SUCCESS Peer Mentoring Program for College Students with Concussion: Preliminary Results of a Mobile Technology Delivered Intervention. International Journal of Environmental Research and Public Health, 20(8), 5438. https://doi.org/10.3390/ijerph20085438