
Examining the Role of Interpersonal Violence in Racial Disparities in Breastfeeding in North Dakota (ND PRAMS 2017–2019)
 , , ,
, , ,
Abstract
:1. Introduction
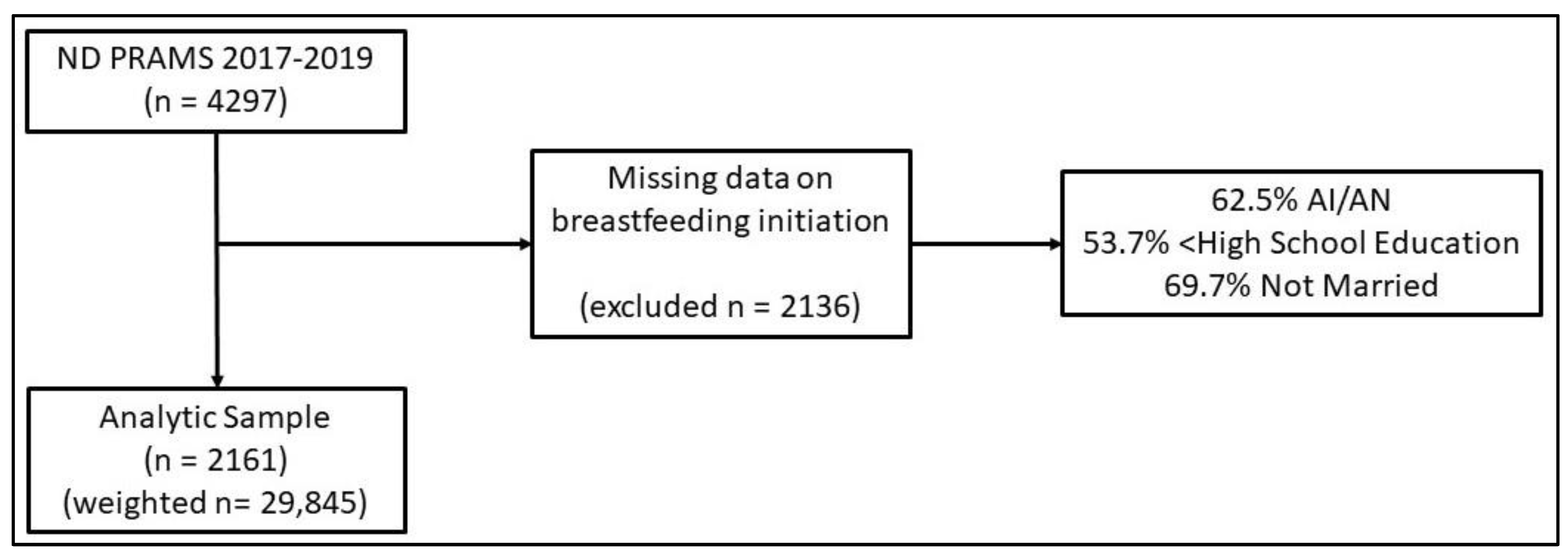
2. Materials and Methods
2.1. Race/Ethnicity
2.2. Breastfeeding
2.3. Interpersonal Violence
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eidelman, A.I.; Schanler, R.J.; Johnston, M.; Landers, S.; Noble, L.; Szucs, K.; Viehmann, L. Breastfeeding and the Use of Human Milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; DeVine, D.; Trikalinos, T.; Lau, J. Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries. Evid. Rep. Technol. Assess. (Full Rep.) 2007, 153, 1–186. [Google Scholar] [CrossRef]
- Weaver, J.M.; Schofield, T.J.; Papp, L.M. Breastfeeding duration predicts greater maternal sensitivity over the next decade. Dev. Psychol. 2018, 54, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Kuperberg, K.; Evers, S. Feeding Patterns and Weight Among First Nations Children. Can. J. Diet. Pract. Res. 2007, 67, 79–84. [Google Scholar] [CrossRef]
- Fagot-Campagna, A.; Pettitt, D.J.; Engelgau, M.M.; Burrows, N.R.; Geiss, L.S.; Valdez, R.; Beckles, G.L.; Saaddine, J.; Gregg, E.W.; Williamson, D.F.; et al. Type 2 diabetes among North adolescents: An epidemiologic health perspective. J. Pediatr. 2000, 136, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Warne, D.; Wescott, S. Social Determinants of American Indian Nutritional Health. Curr. Dev. Nutr. 2019, 3, 12–18. [Google Scholar] [CrossRef]
- Houghton, M.D.; Graybeal, T.E. Breast-feeding Practices of Native American Mothers Participating in WIC. J. Am. Diet. Assoc. 2001, 101, 245–247. [Google Scholar] [CrossRef]
- Houghtaling, B.; Shanks, C.B.; Ahmed, S.; Rink, E. Grandmother and health care professional breastfeeding perspectives provide opportunities for health promotion in an American Indian community. Soc. Sci. Med. 2018, 208, 80–88. [Google Scholar] [CrossRef]
- Rhodes, K.L.; Hellerstedt, W.L.; Davey, C.S.; Pirie, P.L.; Daly, K.A. American Indian breastfeeding attitudes and practices in Minnesota. Matern. Child. Health J. 2008, 12, 46–54. [Google Scholar] [CrossRef]
- Chiang, K.V.; Li, R.; Anstey, E.H.; Perrine, C.G. Racial and Ethnic Disparities in Breastfeeding Initiation–United States, 2019. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 769–774. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau QuickFacts: North Dakota. Available online: https://www.census.gov/quickfacts/ND?#qf-headnote-a (accessed on 22 September 2022).
- Mercy, J.A.; Hillis, S.D.; Butchart, A.; Bellis, M.A.; Ward, C.L.; Fang, X.; Rosenberg, M.L. Interpersonal violence: Global impact and paths to prevention. In Injury Prevention and Environmental Health, 3rd ed.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017; pp. 71–96. [Google Scholar] [CrossRef]
- Caleyachetty, R.; Uthman, O.A.; Bekele, H.N.; Martín-Cañavate, R.; Marais, D.; Coles, J.; Steele, B.; Uauy, R.; Koniz-Booher, P. Maternal exposure to intimate partner violence and breastfeeding practices in 51 low-income and middle-income countries: A population-based cross-sectional study. PLoS Med. 2019, 16, e1002921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doig, A.C.; Jasczynski, M.; Fleishman, J.L.; Aparicio, E.M. Breastfeeding among mothers who have experienced childhood maltreatment: A review. J. Hum. Lact. 2020, 36, 710–722. [Google Scholar] [CrossRef] [PubMed]
- Normann, A.K.; Bakiewicz, A.; Madsen, F.K.; Khan, K.S.; Rasch, V.; Linde, D.S. Intimate partner violence and breastfeeding: A systematic review. BMJ Open 2020, 10, e034153. [Google Scholar] [CrossRef]
- Kendall-Tackett, K.A. Violence against women and the perinatal period: The impact of lifetime violence and abuse on pregnancy, postpartum, and breastfeeding. Trauma Violence Abus. 2007, 8, 344–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coles, J. Qualitative study of breastfeeding after childhood sexual assault. J. Hum. Lact. 2009, 25, 317–324. [Google Scholar] [CrossRef]
- Rosay, A.B. Violence Against American Indian and Alaska Native Women and Men: 2010 Findings from the National Intimate Partner and Sexual Violence Survey Item Type Report. Available online: http://hdl.handle.net/11122/7025 (accessed on 22 August 2022).
- Bachman, R.; Zaykowski, H.; Kallmyer, R.; Poteyeva, M.; Lanier, C. Violence Against American Indian and Alaska Native Women and the Criminal Justice Response: What Is Known; National Institute of Justice/NCJRS: Rockville, MD, USA, 2008. [Google Scholar]
- Wallace, M.; Gillispie-Bell, V.; Cruz, K.; Davis, K.; Vilda, D. Homicide during pregnancy and the postpartum period in the United States, 2018–2019. Obstet. Gynecol. 2021, 138, 762–769. [Google Scholar] [CrossRef]
- Scribano, P.V.; Stevens, J.; Kaizar, E. The effects of intimate partner violence before, during, and after pregnancy in nurse visited first time mothers. Matern. Child. Health J. 2012, 17, 307–318. [Google Scholar] [CrossRef]
- National Coalition Against Domestic Violence. Domestic Violence in North Dakota; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2021; Available online: https://assets.speakcdn.com/assets/2497/north_dakota-2021101912193459.pdf (accessed on 20 August 2022).
- North Dakota Council on Abused Women’s Services. North Dakota Domestic Violence Facts-2019. Available online: https://www.cawsnorthdakota.org/wp-content/uploads/2020/06/2019-ND-DV-Fact-Sheet_8.5x11.pdf (accessed on 24 August 2022).
- Dokkedahl, S.B.; Kirubakaran, R.; Bech-Hansen, D.; Kristensen, T.R.; Elklit, A. The psychological subtype of intimate partner violence and its effect on mental health: A systematic review with meta-analyses. Syst. Rev. 2022, 11, 163. [Google Scholar] [CrossRef] [PubMed]
- Wallenborn, J.T.; Cha, S.; Masho, S.W. Association Between Intimate Partner Violence and Breastfeeding Duration: Results From the 2004–2014 Pregnancy Risk Assessment Monitoring System. J. Hum. Lact. 2018, 34, 233–241. [Google Scholar] [CrossRef]
- Siwik, E.; Larose, S.; Peres, D.; Jackson, K.T.; Burke, S.M.; Mantler, T. Experiences of At-Risk Women in Accessing Breastfeeding Social Support During the Covid-19 Pandemic. J. Hum. Lact. 2022, 38, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Mezzavilla, R.D.S.; Vianna, G.V.D.B.; Lindsay, A.C.; Hasselmann, M.H. Intimate partner violence, breastfeeding, breastmilk substitutes and baby bottle use in the first year of life. Cien. Saude. Colet. 2021, 26, 1955–1964. [Google Scholar] [CrossRef] [PubMed]
- Chaves, K.; Eastwood, J.; Ogbo, F.; Hendry, A.; Jalaludin, B.; Khanlari, S.; Page, A. Intimate partner violence identified through routine antenatal screening and maternal and perinatal health outcomes. BMC Pregnancy Childbirth 2019, 19, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller-Graff, L.E.; Ahmed, A.H.; Paulson, J.L. Intimate Partner Violence and Breastfeeding Outcomes in a Sample of Low-Income Women. J. Hum. Lact. 2018, 34, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Silverman, J.G.; Decker, M.R.; Reed, E.; Raj, A. Intimate Partner Violence around the Time of Pregnancy: Association with Breastfeeding Behavior. Available online: www.liebertpub.com (accessed on 15 September 2022).
- Shulman, H.B.; V D, D.; Harrison, L.; Smith, R.A.; Warner, L. The Pregnancy Risk Assessment Monitoring System (PRAMS): Overview of Design and Methodology. Am. J. Public Health 2018, 108, 1305–1313. [Google Scholar] [CrossRef]
- Kotelchuck, M. The Adequacy of Prenatal Care Utilization Index: Its US Distribution and Association with Low Birthweight. Am. J. Public Health 1994, 84, 1486–1489. [Google Scholar] [CrossRef] [Green Version]
- Mezzavilla, R.D.S.; Ferreira, M.D.F.; Curioni, C.C.; Lindsay, A.C.; Hasselmann, M.H. Intimate partner violence and breastfeeding practices: A systematic review of observational studies. J. Pediatr. 2018, 94, 226–237. [Google Scholar] [CrossRef]
- Brown, L.L.; Talker, R.; Stoddard, G.J.; Clayton, J.; Millar, M.M.; Jo, Y.; Bardsley, T.; Stipelman, C.H. Breastfeeding Attitudes and Practices in a Rural Utah Navajo Community. Matern. Child. Health J. 2022, 26, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Danielson, R.A.; Wallenborn, J.T.; Warne, D.K.; Masho, S.W. Disparities in Risk Factors and Birth Outcomes Among American Indians in North Dakota. Matern. Child. Health J. 2018, 22, 1519–1525. [Google Scholar] [CrossRef]
- Miller-Graff, L.; Scheid, C.R. Breastfeeding continuation at 6 weeks postpartum remediates the negative effects of prenatal intimate partner violence on infant temperament. Dev. Psychopathol. 2019, 32, 503–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theobald, B. Reproduction on the Reservation: Pregnancy, Childbirth, and Colonialism in the Long Twentieth Century; The University of North Carolina Press: Chapel Hill, NC, USA, 2019. [Google Scholar]
- Shaw, E.; Mason, C.N.; Lacarte, V.; Jauregui, E. Holding Up Half the Sky: Mothers as Workers, Primary Caregivers & Breadwinners during COIVID-19. 2020. Available online: https://iwpr.org/wp-content/uploads/2020/07/Holding-Up-Half-the-Sky-Mothers-as-Breadwinners.pdf (accessed on 20 July 2022).
- Mathews, B.; Pacella, R.; Dunne, M.P.; Simunovic, M.; Marston, C. Improving measurement of child abuse and neglect: A systematic review and analysis of national prevalence studies. PLoS ONE 2020, 15, e0227884. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Overall (n = 29,845) | American Indian (n = 2499) | White (n = 23,585) | Other Racial Identities (n = 3760) | |
|---|---|---|---|---|
| Initiation of breastfeeding a | ||||
| Yes | 88.24 (26,336) | 68.87 (1721) | 90.19 (21,271) | 88.94 (3344) |
| No | 11.76 (3509) | 31.13 (778) | 9.81 (2314) | 11.06 (416) |
| Breastfed at least 2 mo. a | ||||
| Yes | 67.28 (20,079) | 40.90 (1022) | 69.45 (16,379) | 71.22 (2678) |
| No | 32.72 (9765) | 59.10 (1477) | 30.55 (7206) | 28.78 (1082) |
| Breastfed at least 6 mo. a | ||||
| Yes | 59.08 (17,633) | 28.81 (720) | 62.27 (14,687) | 59.18 (2225) |
| No | 40.92 (12,212) | 71.19 (1779) | 37.73 (8898) | 40.82 (1535) |
| Maternal Age in years a | ||||
| <=20 | 3.40 (1016) | 12.41 (310) | 2.68 (632) | 1.97 (74) |
| 21-35 | 83.55 (24,934) | 77.75 (1943) | 85.43 (20,148) | 75.64 (2844) |
| >35 | 13.05 (3894) | 9.84 (246) | 11.89 (2805) | 22.39 (842) |
| Income a | ||||
| $48,001 or above | 60.29 (17,995) | 14.97 (374) | 70.21 (16,560) | 28.19 (1060) |
| $48,000 or below | 39.71 (11,850) | 85.03 (2125) | 29.79 (7025) | 71.81 (2700) |
| Insurance Before Pregnancy a | ||||
| Yes | 92.46 (27,593) | 92.00 (2299) | 94.00 (22,168) | 83.14 (3126) |
| No | 7.54 (2251) | 8.00 (200) | 6.00 (1417) | 16.86 (634) |
| Education Level a | ||||
| More than HS | 70.26 (20,968) | 44.46 (1111) | 75.91 (17,903) | 51.97 (1954) |
| Less than or Equal to HS | 29.74 (8876) | 55.54 (1388) | 24.09 (5682) | 48.03 (1806) |
| Received WIC a | ||||
| Yes | 23.5 (7030) | 55.8 (1396) | 15.6 (3679) | 51.9 (1955) |
| No | 76.5 (22815) | 44.2 (1103) | 84.4 (19,906) | 48.1 (1805) |
| Substance Use During Pregnancy a | ||||
| Yes | 3.76 (1121) | 9.64 (241) | 3.16 (746) | 3.54 (133) |
| No | 96.24(28,723) | 90.36 (2258) | 96.84 (22,839) | 96.46 (3627) |
| Pregnancy Intention | ||||
| Did not want | 5.31 (1584) | 7.56 (189) | 4.84 (1141) | 6.76 (254) |
| Wanted | 94.69 (28,261) | 92.44 (2310) | 95.16 (22,444) | 93.24 (3506) |
| Kotelchuck index a | ||||
| Inadequate | 12.3 (3669) | 43.5 (1089) | 8.3 (1967) | 16.3 (613) |
| Intermediate | 10.6 (3180) | 15.4 (384) | 8.9 (2099) | 18.5 (697) |
| Adequate | 54.3 (16,193) | 26.9 (671) | 58.3 (13,740) | 47.4 (1782) |
| Adequate Plus | 22.8 (6802) | 14.2 (355) | 24.5 (5779) | 17.8 (668) |
| Chronic Disease a | ||||
| Yes | 20.08 (5925) | 27.17 (673) | 20.78 (4867) | 10.70 (386) |
| No | 79.92 (23586) | 72.83 (1804) | 79.22 (18558) | 89.30 (3223) |
| Overweight a | ||||
| Yes | 53.06 (15,835) | 62.30 (1557) | 53.21 (12,548) | 46.00 (1730) |
| No | 46.94 (14,010) | 37.70 (942) | 46.79 (11,036) | 54.00 (2031) |
| Marital Status a | ||||
| Yes | 66.81 (19,940) | 18.53 (463) | 71.82 (16,939) | 67.46 (2537) |
| No | 33.19 (9905) | 81.47 (2036) | 28.18 (6646) | 32.54 (1224) |
| High ACEs a | ||||
| Yes | 18.65 (5565) | 29.73 (743) | 19.11 (4506) | 8.35 (314) |
| No | 81.35 (24,280) | 70.27 (1756) | 80.89 (19,078) | 91.65 (3446) |
| Overall (n = 29,845) | American Indian (n = 2499) | White (n = 23,585) | Other Racial Identities (n = 3760) | |
|---|---|---|---|---|
| Any Violence Exposure Before Pregnancy a | ||||
| Yes | 3.35 (1000) | 11.68 (292) | 2.75 (649) | 1.54 (58) |
| No | 96.65 (28,845) | 88.32 (2207) | 97.24 (22,936) | 98.46 (3702) |
| Husband/Partner a | ||||
| Yes | 2.07 (618) | 7.64 (191) | 1.48 (349) | 2.05 (77) |
| No | 97.93 (29,227) | 92.36 (2308) | 98.52 (23,236) | 97.95 (3683) |
| Ex-Husband/Partner a | ||||
| Yes | 2.12 (632) | 5.60 (140) | 1.69 (399) | 2.45 (92) |
| No | 97.88 (29,213) | 94.40 (2359) | 98.31 (23,186) | 97.55 (3668) |
| Family a | ||||
| Yes | 1.50 (447) | 5.76 (144) | 0.94 (221) | 2.15 (81) |
| No | 98.50 (29,398) | 94.24 (2355) | 99.06 (23,364) | 97.85 (3679) |
| Other | ||||
| Yes | 1.93 (575) | 4.04 (101) | 1.77 (418) | 1.46 (55) |
| No | 98.07 (29270) | 95.96 (2398) | 98.23 (23167) | 98.54 (3705) |
| Any Violence Exposure During Pregnancy | ||||
| Yes | 2.17 (647) | 7.16 (179) | 1.70 (403) | 1.72 (65) |
| No | 97.83 (29,198) | 92.84 (2320) | 98.30 (23,182) | 98.28 (3695) |
| Husband/Partner a | ||||
| Yes | 2.01 (601) | 6.20 (155) | 1.42 (336) | 2.90 (109) |
| No | 97.99 (29,244) | 93.80 (2344) | 98.58 (23,249) | 97.10 (3651) |
| Ex-Husband/Partner a | ||||
| Yes | 1.45 (433) | 4.32 (108) | 1.12 (264) | 1.59 (60) |
| No | 98.55 (29,412) | 95.68 (2391) | 98.88 (23,321) | 98.40 (3700) |
| Family a | ||||
| Yes | 1.47 (438) | 5.80 (145) | 0.94 (222) | 1.84 (69) |
| No | 98.53 (29,407) | 94.20 (2354) | 99.06 (23,363) | 98.16 (3691) |
| Other | ||||
| Yes | 1.57 (468) | 3.40 (85) | 1.44 (340) | 1.14 (43) |
| No | 98.43 (29,377) | 96.60 (2414) | 98.56 (23,245) | 98.86 (3717) |
| Breastfeeding Initiation OR (95% CI) | |||||
|---|---|---|---|---|---|
| American Indian | Other Racial Identities | White | Violence Variable Estimate | ||
| Crude Model | 0.24 (0.18, 0.31) a | 0.87 (0.49, 1.52) | Ref. | - | |
| Sociodemographic Model | 0.55 (0.37, 0.83) a | 1.14 (0.60, 2.18) | Ref. | - | |
| Violence Before Pregnancy | Any Interpersonal Violence | 0.55 (0.36, 0.82) a | 1.16 (0.61, 2.22) | Ref. | 0.39 (0.11, 1.42) |
| Husband/Partner | 0.55 (0.37, 0.83) a | 1.14 (0.60, 2.18) | Ref. | 0.94 (0.37, 2.36) | |
| Ex- Husband/Partner | 0.55 (0.37, 0.83) a | 1.14 (0.60, 2.18) | Ref. | 0.95 (0.36, 2.18) | |
| Other Family | 0.56 (0.37, 0.84) a | 1.15 (0.60, 2.19) | Ref. | 0.68 (0.24, 1.95) | |
| Other | 0.55 (0.37, 0.83) a | 1.15 (0.60, 2.19) | Ref. | 0.49 (0.18, 1.31) | |
| Violence During Pregnancy | Any Interpersonal Violence | 0.55 (0.37, 0.83) a | 1.14 (0.60, 2.18) | Ref. | 0.77 (0.20, 2.89) |
| Husband/Partner | 0.54 (0.36, 0.82) a | 1.14 (0.59, 2.17) | Ref. | 1.33 (0.52, 3.42) | |
| Ex- Husband/Partner | 0.55 (0.37, 0.83) a | 1.14 (0.60, 2.18) | Ref. | 1.31 (0.46, 3.73) | |
| Other Family | 0.55 (0.37, 0.83) a | 1.14 (0.60, 2.18) | Ref. | 0.87 (0.34, 2.23) | |
| Other | 0.55 (0.37, 0.83) a | 1.14 (0.60, 2.18) | Ref. | 1.25 (0.42, 3.67) | |
| Breastfeeding Duration—2 Months OR (95% CI) | |||||
|---|---|---|---|---|---|
| American Indian | Other Racial Identities | White | Violence Variable Estimate | ||
| Crude Model | 0.30 (0.25, 0.36) a | 1.08 (0.75, 1.57) | Ref. | - | |
| Sociodemographic Model | 0.70 (0.53, 0.94) a | 1.25 (0.77, 2.03) | Ref. | - | |
| Violence Before Pregnancy | Any Interpersonal Violence | 0.70 (0.53, 0.94) a | 1.27 (0.78, 2.05) | Ref. | 0.36 (0.08, 1.60) |
| Husband/Partner | 0.72 (0.54, 0.97) a | 1.27 (0.78, 2.05) | Ref. | 0.59 (0.23, 1.49) | |
| Ex- Husband/Partner | 0.71 (0.53, 0.94) a | 1.26 (0.77, 2.04) | Ref. | 0.69 (0.29, 1.62) | |
| Other Family | 0.72 (0.54, 0.96) a | 1.26 (0.78, 2.05) | Ref. | 0.44 (0.13, 1.44) | |
| Other | 0.70 (0.53, 0.94) a | 1.25 (0.77, 2.03) | Ref. | 0.48 (0.18, 1.21) | |
| Violence During Pregnancy | Any Interpersonal Violence | 0.71 (0.53, 0.95) a | 1.27 (0.78, 2.06) | Ref. | 0.23 (0.05, 1.09) |
| Husband/Partner | 0.72 (0.54, 0.97) a | 1.28 (0.79, 2.07) | Ref. | 0.49 (0.19, 1.21) | |
| Ex- Husband/Partner | 0.71 (0.53, 0.95) a | 1.26 (0.78, 2.04) | Ref. | 0.45(0.17, 1.17) | |
| Other Family | 0.72 (0.54, 0.96) a | 1.26 (0.78, 2.04) | Ref. | 0.50 (0.16, 1.53) | |
| Other | 0.71 (0.53, 0.95) a | 1.25 (0.78, 2.04) | Ref. | 0.48 (0.18, 1.21) | |
| Breastfeeding Duration—6 Months OR (95% CI) | |||||
|---|---|---|---|---|---|
| American Indian | Other Racial Identities | White | Violence Variable Estimate | ||
| Crude Model | 0.24 (0.20, 0.29) | 0.87 (0.62, 1.23) | Ref. | - | |
| Sociodemographic Model | 0.62 (0.47, 0.83) | 0.89 (0.57, 1.38) | Ref. | - | |
| Violence Before Pregnancy | Any Interpersonal Violence | 0.62 (0.47, 0.83) | 0.89 (0.57, 1.39) | Ref. | 0.61 (0.11, 3.13) |
| Husband/Partner | 0.63 (0.47, 0.85) | 0.89 (0.57, 1.39) | Ref. | 0.67 (0.24, 1.90) | |
| Ex- Husband/Partner | 0.62 (0.47, 0.83) | 0.89 (0.57, 1.39) | Ref. | 0.46 (0.18, 1.16) | |
| Other Family | 0.63 (0.48, 0.85) | 0.89 (0.57, 1.39) | Ref. | 0.47 (0.12, 1.78) | |
| Other | 0.62 (0.47, 0.83) | 0.89 (0.57, 1.39) | Ref. | 0.70 (0.24, 2.00) | |
| Violence During Pregnancy | Any Interpersonal Violence | 0.62 (0.47, 0.84) | 0.90 (0.58, 1.40) | Ref. | 0.34 (0.06, 1.88) |
| Husband/Partner | 0.64 (0.48, 0.85) | 0.90 (0.58, 1.41) | Ref. | 0.51 (0.19, 1.36) | |
| Ex- Husband/Partner | 0.62 (0.47, 0.83) | 0.89 (0.57, 1.39) | Ref. | 0.70 (0.24, 1.98) | |
| Other Family | 0.63 (0.47, 0.84) | 0.89 (0.57, 1.39) | Ref. | 0.70 (0.20, 2.46) | |
| Other | 0.62 (0.47, 0.83) | 0.89 (0.57, 1.39) | Ref. | 0.63 (0.22, 1.77) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanichy, M.; Schmidt, L.; Anderson, R.; Njau, G.; Stiffarm, A.; Schmidt, M.; Stepanov, A.; Williams, A. Examining the Role of Interpersonal Violence in Racial Disparities in Breastfeeding in North Dakota (ND PRAMS 2017–2019). Int. J. Environ. Res. Public Health 2023, 20, 5445. https://doi.org/10.3390/ijerph20085445
Kanichy M, Schmidt L, Anderson R, Njau G, Stiffarm A, Schmidt M, Stepanov A, Williams A. Examining the Role of Interpersonal Violence in Racial Disparities in Breastfeeding in North Dakota (ND PRAMS 2017–2019). International Journal of Environmental Research and Public Health. 2023; 20(8):5445. https://doi.org/10.3390/ijerph20085445
Chicago/Turabian StyleKanichy (Makah), MichaeLynn, Lexie Schmidt, RaeAnn Anderson, Grace Njau, Amy Stiffarm (Aaniiih), Matthew Schmidt, Anastasia Stepanov, and Andrew Williams. 2023. "Examining the Role of Interpersonal Violence in Racial Disparities in Breastfeeding in North Dakota (ND PRAMS 2017–2019)" International Journal of Environmental Research and Public Health 20, no. 8: 5445. https://doi.org/10.3390/ijerph20085445
APA StyleKanichy, M., Schmidt, L., Anderson, R., Njau, G., Stiffarm, A., Schmidt, M., Stepanov, A., & Williams, A. (2023). Examining the Role of Interpersonal Violence in Racial Disparities in Breastfeeding in North Dakota (ND PRAMS 2017–2019). International Journal of Environmental Research and Public Health, 20(8), 5445. https://doi.org/10.3390/ijerph20085445