
Taking Care of an Adolescent and Young Adult Cancer Survivor: A Systematic Review of the Impact of Cancer on Family Caregivers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
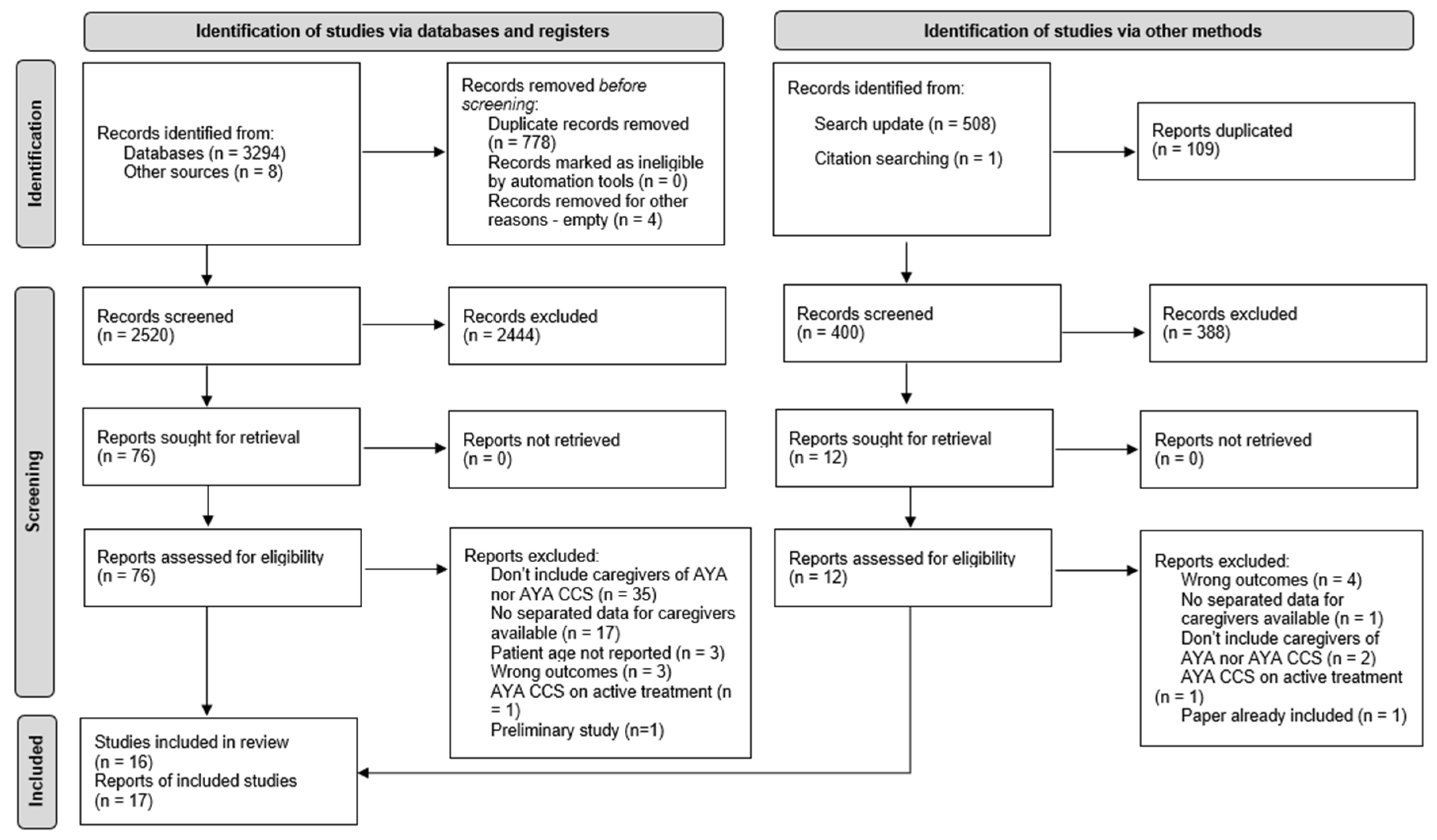
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Study Quality
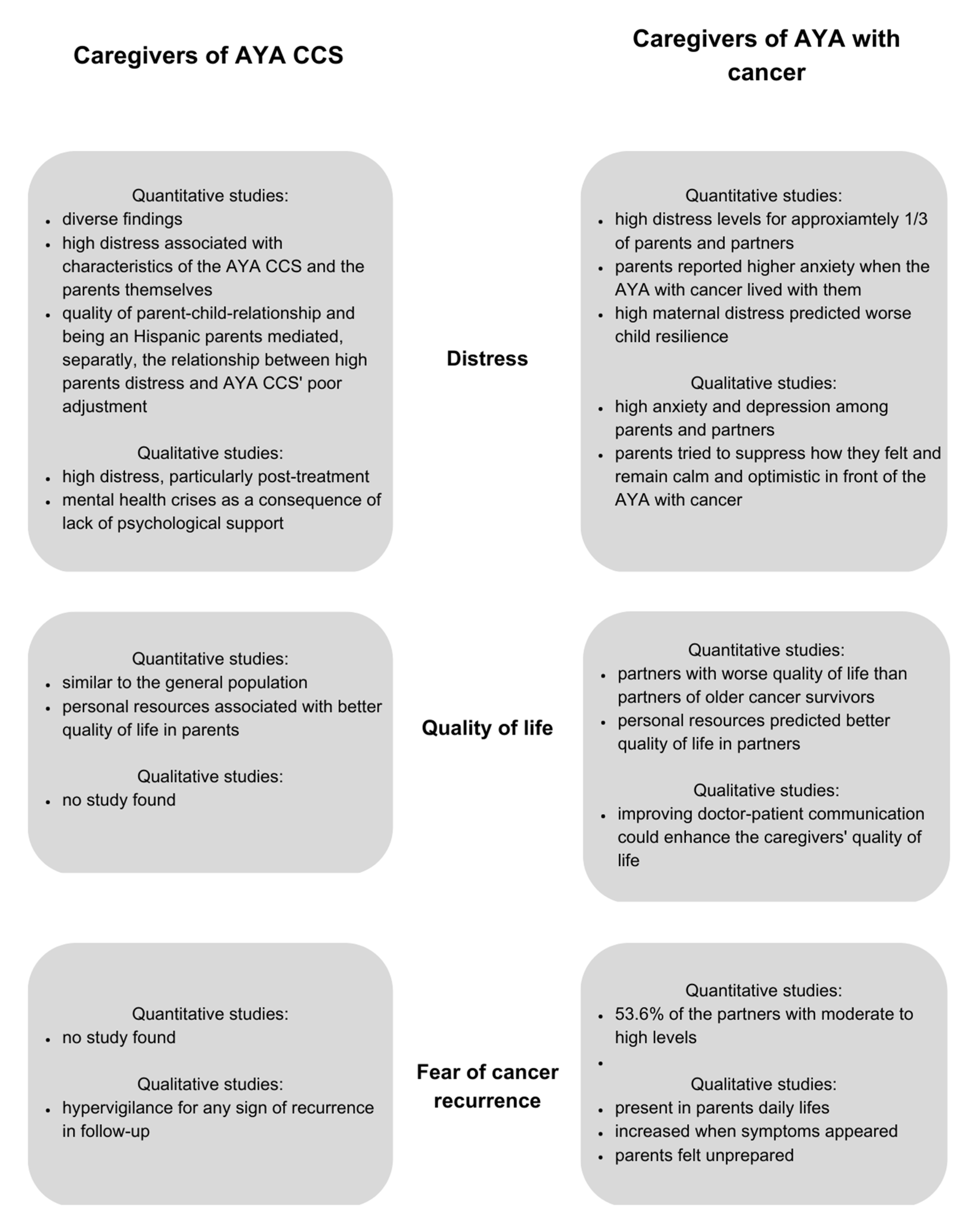
3.4. Distress
3.4.1. Caregivers of AYA CCS
3.4.2. Caregivers of AYA with Cancer
3.5. Quality of Life
3.5.1. Caregivers of AYA CCS
3.5.2. Caregivers of AYA with Cancer
3.6. Fear of Cancer Recurrence
3.6.1. Caregivers of AYA CCS
3.6.2. Caregivers of AYA with Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Northouse, L.L.; Katapodi, M.C.; Schafenacker, A.M.; Weiss, D. The Impact of Caregiving on the Psychological Well-Being of Family Caregivers and Cancer Patients. Semin. Oncol. Nurs. 2012, 28, 236–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langenberg, S.M.C.H.; Poort, H.; Wymenga, A.N.M.; de Groot, J.W.; Muller, E.W.; van der Graaf, W.T.A.; Prins, J.B.; van Herpen, C.M.L. Informal Caregiver Well-Being during and after Patients’ Treatment with Adjuvant Chemotherapy for Colon Cancer: A Prospective, Exploratory Study. Support. Care Cancer 2021, 29, 2481–2491. [Google Scholar] [CrossRef] [PubMed]
- Junkins, C.C.; Kent, E.; Litzelman, K.; Bevans, M.; Cannady, R.S.; Rosenberg, A.R. Cancer across the Ages: A Narrative Review of Caregiver Burden for Patients of All Ages. J. Psychosoc. Oncol. 2020, 38, 782–798. [Google Scholar] [CrossRef] [PubMed]
- Vrijmoet-Wiersma, C.M.; van Klink, J.M.M.; Kolk, A.M.; Koopman, H.M.; Ball, L.M.; Maarten Egeler, R. Assessment of Parental Psychological Stress in Pediatric Cancer: A Review. J. Pediatr. Psychol. 2008, 33, 694–706. [Google Scholar] [CrossRef] [Green Version]
- Borrescio-Higa, F.; Valdés, N. The Psychosocial Burden of Families with Childhood Blood Cancer. Int. J. Env. Res. Public. Health 2022, 19, 599. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, L.; Cernvall, M.; Grönqvist, H.; Ljótsson, B.; Ljungman, G.; von Essen, L. Long-Term Positive and Negative Psychological Late Effects for Parents of Childhood Cancer Survivors: A Systematic Review. PLoS ONE 2014, 9, e103340. [Google Scholar] [CrossRef] [Green Version]
- Bakula, D.M.; Sharkey, C.M.; Perez, M.N.; Espeleta, H.C.; Gamwell, K.L.; Baudino, M.; Delozier, A.M.; Chaney, J.M.; Matt Alderson, R.; Mullins, L.L. Featured Article: The Relationship between Parent and Child Distress in Pediatric Cancer: A Meta-Analysis. J. Pediatr. Psychol. 2019, 44, 1121–1136. [Google Scholar] [CrossRef]
- Bakula, D.M.; Sharkey, C.M.; Perez, M.N.; Espeleta, H.C.; Gamwell, K.L.; Baudino, M.; Delozier, A.M.; Chaney, J.M.; Alderson, R.M.; Mullins, L.L. The Relationship between Parent Distress and Child Quality of Life in Pediatric Cancer: A Meta-Analysis. J. Pediatr. Nurs. 2020, 50, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.W.; Seibel, N.L.; Lewis, D.R.; Albritton, K.H.; Blair, D.F.; Blanke, C.D.; Bleyer, W.A.; Freyer, D.R.; Geiger, A.M.; Hayes-Lattin, B.; et al. Next Steps for Adolescent and Young Adult Oncology Workshop: An Update on Progress and Recommendations for the Future. Cancer 2016, 122, 988–999. [Google Scholar] [CrossRef]
- Adolescent and Young Adult Oncology Progress Review Group. Closing the Gap: Research and Care Implications for Adolescents and Young Adults with Cancer. 2006. Available online: https://www.cancer.gov/types/aya/research/ayao-august-2006.pdf (accessed on 26 January 2023).
- Robison, L.L.; Mertens, A.C.; Boice, J.D.; Breslow, N.E.; Donaldson, S.S.; Green, D.M.; Li, F.P.; Meadows, A.T.; Mulvihill, J.J.; Neglia, J.P.; et al. Study Design and Cohort Characteristics of the Childhood Cancer Survivor Study: A Multi-Institutional Collaborative Project. Med. Pediatr. Oncol. 2002, 38, 229–239. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging Adulthood: A Theory of Development from the Late Teens through the Twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Zebrack, B.J. Psychological, Social, and Behavioral Issues for Young Adults with Cancer. Cancer 2011, 117 (Suppl. S10), 2289–2294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, 160. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Joanna Briggs Institute. Checklist for Analytical Cross Sectional Studies; The Joanna Briggs Institute: Adelaide, SA, Australia, 2020. [Google Scholar]
- The Joanna Briggs Institute. Checklist for Qualitative Research; The Joanna Briggs Institute: Adelaide, SA, Australia, 2017; Volume 6. [Google Scholar]
- Barrett, P.M.; Mullen, L.; McCarthy, T. Enduring Psychological Impact of Childhood Cancer on Survivors and Their Families in Ireland: A National Qualitative Study. Eur. J. Cancer Care 2020, 29, 5. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, D.K.; Fortier, M.A.; Osann, K.; Wilford, J.; Shen, V.; Torno, L.; Sender, L.S.; Parsons, S.K.; Wenzel, L. Quality of Life among Parents of Adolescent and Young Adult Brain Tumor Survivors. J. Pediatr. Hematol. Oncol. 2017, 39, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Meeske, K.A.; Sherman-Bien, S.; Hamilton, A.S.; Olson, A.R.; Slaughter, R.; Kuperberg, A.; Milam, J. Mental Health Disparities between Hispanic and Non-Hispanic Parents of Childhood Cancer Survivors. Pediatr. Blood Cancer 2013, 60, 1470–1477. [Google Scholar] [CrossRef] [Green Version]
- Prikken, S.; Raymaekers, K.; Lemiere, J.; Vercruysse, T.; Uyttebroeck, A.; Luyckx, K. Worries and Benefit Finding in Cancer Survivors and Parents: A Longitudinal Study. J. Pediatr. Psychol. 2022, 47, 641–651. [Google Scholar] [CrossRef]
- Schepers, S.A.; Okado, Y.; Russell, K.; Long, A.M.; Phipps, S. Adjustment in Childhood Cancer Survivors, Healthy Peers, and Their Parents: The Mediating Role of the Parent-Child Relationship. J. Pediatr. Psychol. 2019, 44, 186–196. [Google Scholar] [CrossRef]
- Slaughter, R.I.; Hamilton, A.S.; Cederbaum, J.A.; Unger, J.B.; Baezconde-Garbanati, L.; Milam, J.E. Relationships between Parent and Adolescent/Young Adult Mental Health among Hispanic and Non-Hispanic Childhood Cancer Survivors. J. Psychosoc. Oncol. 2020, 38, 746–760. [Google Scholar] [CrossRef]
- Turner-Sack, A.M.; Menna, R.; Setchell, S.R.; Maan, C.; Cataudella, D. Psychological Functioning, Post-Traumatic Growth, and Coping in Parents and Siblings of Adolescent Cancer Survivors. Oncol. Nurs. Forum 2016, 43, 48–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; He, Q.; Zeng, Y.; Wang, L.; Yu, H.; Yin, W.; Jiang, Y.; Liu, L. Feeling like the Sky Is Falling down: Experiences of Parents of Adolescents Diagnosed with Cancer in One-Child Families in China—A Qualitative Study. J. Clin. Nurs. 2022, 31, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Cohee, A.A.; Adams, R.N.; Johns, S.A.; von Ah, D.; Zoppi, K.; Fife, B.; Monahan, P.O.; Stump, T.; Cella, D.; Champion, V.L. Long-Term Fear of Recurrence in Young Breast Cancer Survivors and Partners. Psychooncology 2017, 26, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohee, A.A.; Bigatti, S.M.; Shields, C.G.; Johns, S.A.; Stump, T.; Monahan, P.O.; Champion, V.L. Quality of Life in Partners of Young and Old Breast Cancer Survivors. Cancer Nurs. 2018, 41, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Congard, A.; Christophe, V.; Duprez, C.; Baudry, A.-S.S.; Antoine, P.; Lesur, A.; Loustalot, C.; Guillemet, C.; Leclercq, M.; Segura, C.; et al. The Self-Reported Perceptions of the Repercussions of the Disease and Its Treatments on Daily Life for Young Women with Breast Cancer and Their Partners. J. Psychosoc. Oncol. 2019, 37, 50–68. [Google Scholar] [CrossRef]
- Lau, N.; Yi-Frazier, J.P.; Bona, K.; Baker, K.S.; McCauley, E.; Rosenberg, A.R. Distress and Resilience among Adolescents and Young Adults with Cancer and Their Mothers: An Exploratory Analysis. J. Psychosoc. Oncol. 2020, 38, 118–124. [Google Scholar] [CrossRef]
- McCarthy, M.C.; McNeil, R.; Drew, S.; Dunt, D.; Kosola, S.; Orme, L.; Sawyer, S.M. Psychological Distress and Posttraumatic Stress Symptoms in Adolescents and Young Adults with Cancer and Their Parents. J. Adolesc. Young Adult Oncol. 2016, 5, 322–329. [Google Scholar] [CrossRef]
- Mikrut, E.E.; Panjwani, A.A.; Cipollina, R.; Revenson, T.A. Emotional Adjustment among Parents of Adolescents and Young Adults with Cancer: The Influence of Social Constraints on Cognitive Processing and Fear of Recurrence. J. Behav. Med. 2020, 43, 237–245. [Google Scholar] [CrossRef]
- Mishra, S.I.; Rishel Brakey, H.; Kano, M.; Nedjat-Haiem, F.R.; Sussman, A.L. Health Related Quality of Life during Cancer Treatment: Perspectives of Young Adult (23–39 Years) Cancer Survivors and Primary Informal Caregivers. Eur. J. Oncol. Nurs. 2018, 32, 48–54. [Google Scholar] [CrossRef]
- Panjwani, A.A.; Millar, B.M.; Revenson, T.A. Tolerating Uncertainty in the Dark: Insomnia Symptoms, Distress, and Well-Being Among Parents of Adolescents and Young Adults with Cancer. Int. J. Behav. Med. 2020, 28, 14–20. [Google Scholar] [CrossRef]
- Walker, A.J.; Lewis, F.M.; Rosenberg, A.R. Walking on Eggshells: Parents’ First Year After Their Adolescent Completes Their Cancer Treatment. J. Pediatr. Oncol. Nurs. 2020, 37, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Decadt, I.; Laenen, A.; Celus, J.; Geyskens, S.; Vansteenlandt, H.; Coolbrandt, A. Caregiver Distress and Quality of Life in Primary Caregivers of Oncology Patients in Active Treatment and Follow-Up. Eur. J. Cancer Care 2021, 30, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Guan, N.; Guariglia, A.; Moore, P.; Xu, F.; Al-Janabi, H. Financial Stress and Depression in Adults: A Systematic Review. PLoS ONE 2022, 17, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Casillas, J.; Kahn, K.L.; Doose, M.; Landier, W.; Bhatia, S.; Hernandez, J.; Zeltzer, L.K. Transitioning Childhood Cancer Survivors to Adult-Centered Healthcare: Insights from Parents, Adolescent, and Young Adult Survivors. Psychooncology 2010, 19, 982–990. [Google Scholar] [CrossRef] [PubMed]
- van Warmerdam, J.; Zabih, V.; Kurdyak, P.; Sutradhar, R.; Nathan, P.C.; Gupta, S. Prevalence of Anxiety, Depression, and posttraumatic stress disorder in Parents of Children with Cancer: A Meta-Analysis. Pediatr. Blood Cancer 2019, 66, 6. [Google Scholar] [CrossRef]
- Peikert, M.L.; Inhestern, L.; Krauth, K.A.; Escherich, G.; Rutkowski, S.; Kandels, D.; Bergelt, C. Returning to Daily Life: A Qualitative Interview Study on Parents of Childhood Cancer Survivors in Germany. BMJ Open. 2020, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Sheng, N.; Ma, J.; Ding, W.; Zhang, Y. Effects of Caregiver-Involved Interventions on the Quality of Life of Children and Adolescents with Chronic Conditions and Their Caregivers: A Systematic Review and Meta-Analysis. Qual. Life Res. 2019, 28, 13–33. [Google Scholar] [CrossRef]
- Smith, A.B.; Wu, V.S.; Lambert, S.; Lamarche, J.; Lebel, S.; Leske, S.; Girgis, A. A Systematic Mixed Studies Review of Fear of Cancer Recurrence in Families and Caregivers of Adults Diagnosed with Cancer. J. Cancer Surviv. 2021, 16, 1184–1219. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Design | Data Collection Method | Type of AYA | Type of Caregiver | Caregiver: Measures |
|---|---|---|---|---|---|---|
| Barrett et al., 2020 [18] | Ireland | Qualitative | Focus group | AYA CCS | Parents | N/A |
| Buchbinder et al., 2017 [19] | USA | Quantitative | In-person | AYA CCS | Parents | QoL: Patient-reported Outcomes Measurement Information System (PROMIS) Global Health |
| Chen et al., 2022 [25] | China | Qualitative | Semi-structured interviews | AYA | Parents | N/A |
| Cohee et al., 2017, 2018 [26,27] | USA | Quantitative | Sent by mail | AYA | Partner | FCR: Concerns About Recurrence Scale (CARS) Depression: Center for Epidemiologic Studies—Depression Scale (CES-D) QoL: Index of Well-Being (IWB) |
| Congard et al., 2019 [28] | USA | Quantitative | In-person recruitment, but participants responded at home | AYA | Partner | Anxiety: State-Trait Anxiety Inventory (STAI) Depression: CES-D |
| Lau et al., 2020 [29] | USA | Quantitative | Online or pen and paper | AYA | Parents | Distress: Kessler Psychological Distress Scale 6 (K6) |
| McCarthy et al., 2016 [30] | Australia | Quantitative | Sent by mail | AYA | Parents | Distress: Kessler Psychological Distress Scale (K10) |
| Meeske et al., 2013 [20] | USA | Quantitative | Sent by mail | AYA CCS | Parents | Depression: CES-D |
| Mikrut et al., 2020 [31] | USA | Quantitative | Web-based survey | AYA | Parents | FCR; CARS Depression: Patient Health Questionnaire (PHQ-9) |
| Mishra et al., 2018 [32] | USA | Qualitative | Semi-structured interview | AYA | Parents and partners | N/A |
| Panjwani et al., 2020 [31] | USA | Quantitative | Web-based survey | AYA | Parents | Depression: PHQ-2 Anxiety: Generalized Anxiety Disorder Scale (GAD-7) |
| Prikken et al., 2022 [21] | Belgium | Quantitative | By mail | AYA CCS | Parents | Depression: CES-D |
| Schepers et al., 2019 [22] | USA | Quantitative | In-person | AYA CCS | Parents | Distress: Brief Symptom Inventory (BSI-18) |
| Slaughter et al., 2020 [23] | USA | Quantitative | Sent by mail | AYA CCS | Parents | Distress: PSS-4 QoL: Pediatric Quality of Life Questionnaire Depression: CES-D |
| Turner-Sack et al., 2016 [24] | Canada | Quantitative | Sent by mail | AYA CCS | Parents | Distress: BSI |
| Walker et al., 2020 [34] | USA | Qualitative | Semi-structured interview | AYA | Parents | N/A |
| Author, Year | Caregiver: Sample Size | Caregiver: Sex | Caregiver: Age (Mean) | Caregiver: Education (Percentage or Years) | Caregiver: Marital Status (Percentage) |
|---|---|---|---|---|---|
| Barrett et al., 2020 [18] | 18 | F = 88.8%, M = 11.2% | Missing | Missing | Missing |
| Buchbinder et al., 2017 [19] | 28 | F = 46.4%, M = 53.6% | 44 (7) | High school/GED or College/Grad School = 25 (89.3%) | Married or living with partner = 19 (67.9%) |
| Chen et al., 2022 [25] | 14 | F = 85.7%, M = 14.3% | 53 | Missing | Married = 12, Divorced = 2 |
| Cohee et al., 2017, 2018 [26,27] | 222/227 | Missing | 47.98 (7.2)/48.04 (7.04) | 14.92 (2.6) years | Living with partner = 100% |
| Congard et al., 2019 [28] | 491 | M = 100% | 43.28 (7.46) | 14.88 (2.552) years | Missing |
| Lau et al., 2020 [29] | 14 | F = 100% | 47 | Missing | Missing |
| McCarthy et al., 2016 [30] | 204 | F = 90%, M = 10% | Missing | Missing | Married/partner = 154 (77%) Separated/Divorced = 23 (11.5%) Single = 23 (11.5%) |
| Meeske et al., 2013 [20] | Hispanic: 79; Non-Hispanic: 69 | Hispanic: F = 90%, M = 10%; Non-Hispanic: F = 85%, M = 15% | Hispanic = 46.77 (6.19), Non-Hispanic = 51.79 (6.61) | Hispanic: Grade school (1–8 years) = 43(54%); Non-hispanic: High school = 20 (34%), Some college = 13 (22%), College/Grad school = 14 (24%) | Hispanic: Married = 59 (75%); Non-hispanic: Married = 38 (63%) |
| Mikrut et al., 2020 [31] | 66 | F = 92%, M = 8% | 55.17 (7.02) | Missing | Married/in a long-term relationship = 80% |
| Mishra et al., 2018 [32] | 8 | F = 50%, M = 50% | 24–65 | College/Bachelor’s degree = 6 | Married/living with partner = 6 |
| Panjwani et al., 2020 [31] | 59 | F = 91%, M = 9% | 55 (7.43) | Missing | Married/in a long term relationship = 80%) |
| Prikken et al., 2022 [21] | 224 | F = 59.4%, M = 40.6% | F = 49.4, M = 51.51 | Higher education: F = 70%, M = 58% | Not married or living with a partner—F = 14%; M = 11% |
| Schepers et al., 2019 [22] | 206 | F = 89.9%, M = 12.1% | 43.67 (7.03) | Missing | Missing |
| Slaughter et al., 2020 [23] | Hispanic: 68; Non-Hispanic: 61 | Hispanic: F = 89.7%, M = 10.3%; Non-hispanic: F = 85.6%, M = 14.8% | Hispanic: 46.32 (6.07); Non-hispanic = 51.98 (6.33) | Missing | Missing |
| Turner-Sack et al., 2016 [24] | 30 | F = 96.6%, M = 3.4% | 45.07 (5.64) | Graduated college/university = 20 | Missing |
| Walker et al., 2020 [34] | 30 | F = 93%, M = 7% | 47 (7) | Missing | Married = 23 (77%) |
| N | |
|---|---|
| Qualitative research | |
| Is there congruity between the stated philosophical perspective and the research methodology? | 2/4 |
| Is there congruity between the research methodology and the research question or objectives? | 4/4 |
| Is there congruity between the research methodology and the methods used to collect data? | 4/4 |
| Is there congruity between the research methodology and the representation and analysis of data? | 4/4 |
| Is there congruity between the research methodology and the interpretation of results? | 4/4 |
| Is there a statement locating the researcher culturally or theoretically? | 1/4 |
| Is the influence of the researcher on the research, and vice-versa, addressed? | 1/4 |
| Are participants, and their voices, adequately represented? | 4/4 |
| Is the research ethical according to current criteria or, for recent studies, and is there evidence of ethical approval by an appropriate body? | 4/4 |
| Do the conclusions drawn in the research report flow from the analysis or interpretation, of the data? | 4/4 |
| Quantitative research | |
| Were the criteria for inclusion in the sample clearly defined? | 13/13 |
| Were the study subjects and the setting described in detail? | 13/13 |
| Was the exposure measured in a valid and reliable way? | Not applicable |
| Were objective, standard criteria used for measurement of the condition? | 13/13 |
| Were confounding factors identified? | 5/13 |
| Were strategies to deal with confounding factors stated? | 5/13 |
| Were the outcomes measured in a valid and reliable way? | 10/13 |
| Was appropriate statistical analysis used? | 13/13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neves, M.C.; Bártolo, A.; Prins, J.B.; Sales, C.M.D.; Monteiro, S. Taking Care of an Adolescent and Young Adult Cancer Survivor: A Systematic Review of the Impact of Cancer on Family Caregivers. Int. J. Environ. Res. Public Health 2023, 20, 5488. https://doi.org/10.3390/ijerph20085488
Neves MC, Bártolo A, Prins JB, Sales CMD, Monteiro S. Taking Care of an Adolescent and Young Adult Cancer Survivor: A Systematic Review of the Impact of Cancer on Family Caregivers. International Journal of Environmental Research and Public Health. 2023; 20(8):5488. https://doi.org/10.3390/ijerph20085488
Chicago/Turabian StyleNeves, Maria Carolina, Ana Bártolo, Judith B. Prins, Célia M. D. Sales, and Sara Monteiro. 2023. "Taking Care of an Adolescent and Young Adult Cancer Survivor: A Systematic Review of the Impact of Cancer on Family Caregivers" International Journal of Environmental Research and Public Health 20, no. 8: 5488. https://doi.org/10.3390/ijerph20085488
APA StyleNeves, M. C., Bártolo, A., Prins, J. B., Sales, C. M. D., & Monteiro, S. (2023). Taking Care of an Adolescent and Young Adult Cancer Survivor: A Systematic Review of the Impact of Cancer on Family Caregivers. International Journal of Environmental Research and Public Health, 20(8), 5488. https://doi.org/10.3390/ijerph20085488