
Attachment, Feeding Practices, Family Routines and Childhood Obesity: A Systematic Review of the Literature


Abstract
:1. Introduction
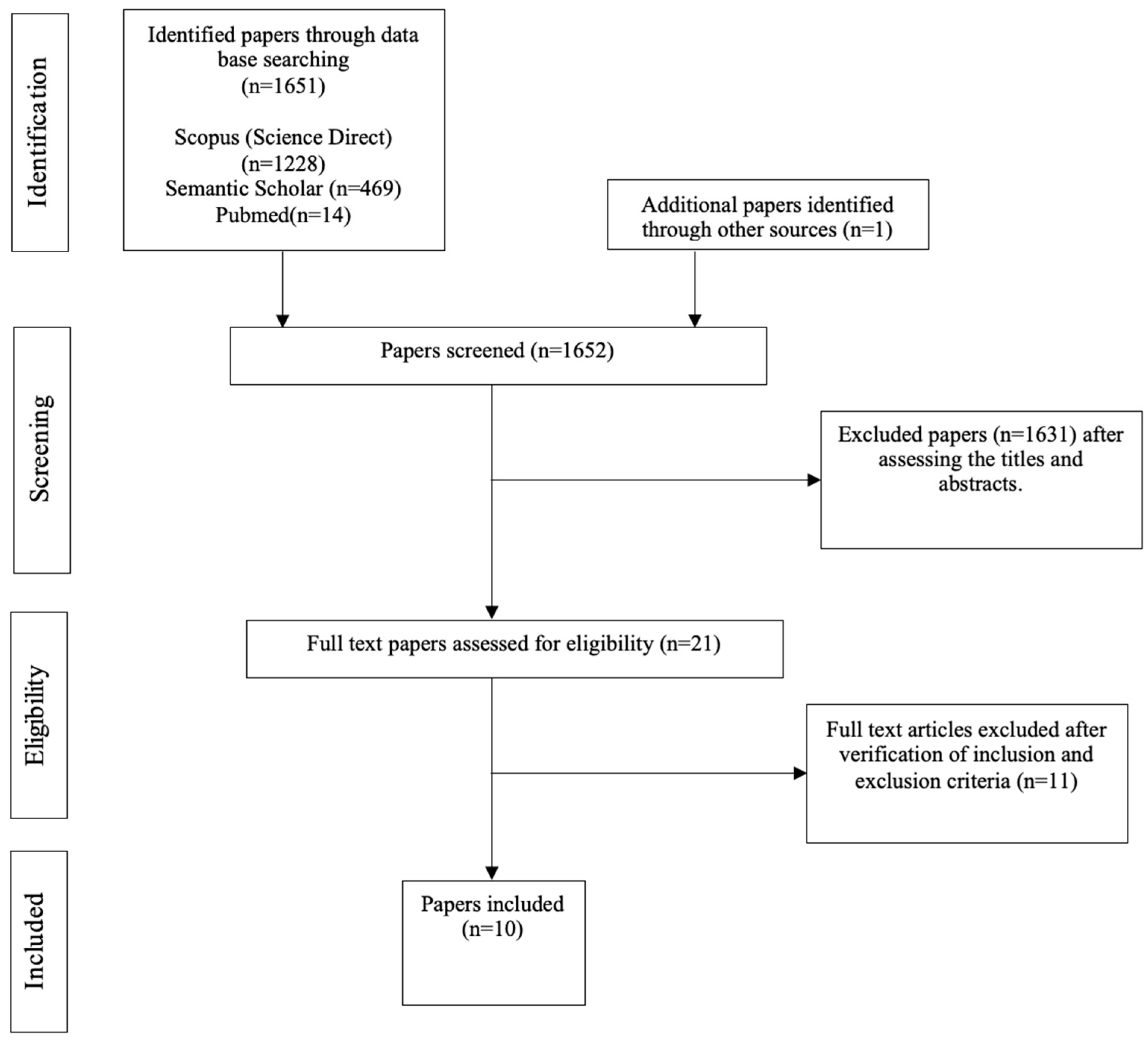
2. Materials and Methods
3. Results
3.1. Characteristics of the Analyzed Papers
3.2. Study Quality and Risk of Bias Assessment
3.3. Analysis of Papers
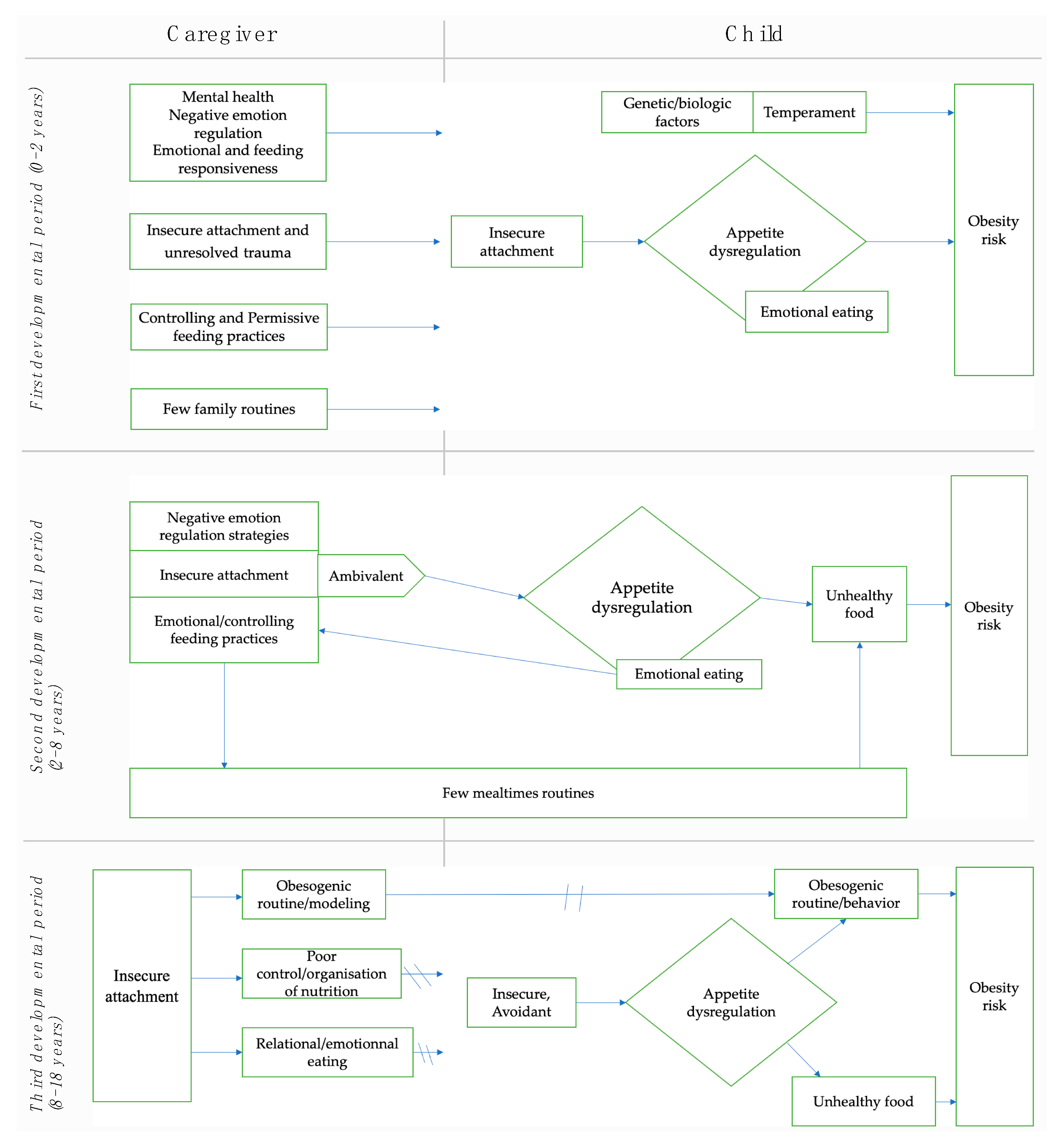
First Developmental Period (0–2 Years)
3.4. Second Developmental Period (2–8 Years)
3.5. Third Developmental Period (8–18 Years)
4. Discussion
4.1. First Developmental Period (0–2 Years)
4.2. Second Developmental Period (2–8 Years)
4.3. Third Developmental Period (8–18 Years)
4.4. Practical Applications
4.5. Study Limitations and Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Reisz et al. (2019) [21] | Saltzman et al. (2018b) [45] | |
|---|---|---|
| Was the research question or objective in this paper clearly stated? (0–1) | 1 | 1 |
| Was the study population clearly specified and defined? (0–1) | 1 | 1 |
| Was the participation rate of eligible persons at least 50%? (0–1) | 1 | 1 |
| Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? (0–1) | 0 | 1 |
| Was a sample size justification, power description, or variance and effect estimates provided? (0–1) | 1 | 1 |
| For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? (0–0.5–1) | 1 | 0.5 |
| Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? (0–1) | 1 | 0 |
| For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)? (0–0.5–1) | 1 | 0.5 |
| Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? (0–0.5–1) | 1 | 1 |
| Was the exposure(s) assessed more than once over time? (0–0.5–1) | 1 | 0.5 |
| Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? (0–1) | 1 | 1 |
| Was loss to follow-up after baseline 20% or less? (0–1) | 1 | 1 |
| Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? (0–0.5–1) | 0 | 1 |
| Overall quality rating ** | 11a Fair | 10.5b Good |
| Powell et al. (2017) [63] | Hardman et al. (2016) [60] | Bost et al. (2014) [64] | Pasztak-Opiłka et al. (2020) [61] | Lamson et al. (2020) [62] | |
|---|---|---|---|---|---|
| Was the research question or objective in this paper clearly stated? (0–1) | 1 | 1 | 1 | 1 | 1 |
| Was the study population clearly specified and defined? (0–1) | 1 | 1 | 1 | 0 | 1 |
| Was the participation rate of eligible persons at least 50%? (0–1) | 1 | 1 | 1 | 1 | 1 |
| Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? (0–1) | 0 | 0 | 1 | 0 | 1 |
| Was a sample size justification, power description, or variance and effect estimates provided? (0–1) | 1 | 1 | 1 | 1 | 0 |
| For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)? (0–0.5–1) | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
| Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? (0–0.5–1) | 1 | 1 | 1 | 1 | 0.5 |
| Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? (0–1) | 1 | 1 | 1 | 1 | 1 |
| Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? (0–0.5–1) | 1 | 0 | 1 | 0 | 0 |
| Overall quality rating ** | 7.5a Good | 6.5b Fair | 8c Good | 5.5d Fair | 6e Fair |
| Reisz et al. (2019) [21] | Saltzman et al. (2018b) [45] | Powell et al. (2017) [63] | Hardman et al. (2016) [60] | Bost et al. (2014) [64] | Pasztak-Opiłka et al. (2020) [61] | Lamson et al. (2020) [62] | |
|---|---|---|---|---|---|---|---|
| Did the study address a clearly focused issue? | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the cohort recruited in an acceptable way? | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the exposure accurately measured to minimize bias? | Yes | Yes | Yes | Yes | Yes | All measuring tools were validated except the KZZ | Yes |
| Was the outcome accurately measured to minimize bias? | Yes | Yes | Yes | Yes | Yes | Yes, but not for mother’s eating behaviors (KZZ) | Yes |
| A. Have the authors identified all important confounding factors? B. Have they taken account of the confounding factors in the design and/or analysis? | a. Yes b. No | a. Yes b. Yes | a. Yes b. Yes | a. Yes b. No | a. Yes b. Yes | a. Yes b. No | a. Yes b. No |
| A. Was the follow up of subject complete enough? B. Was the follow up of subjects long enough? | a. Yes b. Yes | a. Yes b. Cannot tell | |||||
| What are the results of this study? | See Table 2 | See Table 2 | See Table 3 | See Table 3 | See Table 3 | See Table 4 | See Table 4 |
| How precise are the results? | Statistical results clear but confidence intervals not given | Statistical results clear and confidence intervals given | Statistical results clear and confidence intervals given | Statistical results clear and confidence intervals given | Statistical results clear but confidence intervals not given | Statistical results not very clear, confidence intervals not given | Statistical results clear but confidence intervals not given |
| Are the results believable? | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Can the results be applied to local population? | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Do the results of this study fit with other available evidence? | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| What are the implications of this study for practice? | Observational data supported by other evidence | Mixed methodology (observational data, self-reports, interview) provides robust evidence for recommendations of change into clinical practice. | Use of only self-reports. Evidence is less robust for recommendations of change into clinical practice. | Use of only self-reports. Evidence is less robust for recommendations of change into clinical practice. | Use of only self-reports. Evidence is less robust for recommendations of change into clinical practice. | Use of only self-reports. Evidence is less robust for recommendations. | Use of only self-reports. Evidence is less robust for recommendations. |
| Bergmeier, et al. 2020 [59] | Saltzman et al. (2018a) [58] | Fiese and Bost (2016) [32] | |
|---|---|---|---|
| Did the review address a clearly focused question? | Yes | Yes | Yes |
| Did the authors look for the right type of papers? | Cannot tell. No standardized methodology structured this review | Cannot tell. No standardized methodology structured this review | Cannot tell. No standardized methodology structured this review |
| Do you think all the important, relevant studies were included? | Cannot tell | Cannot tell | Cannot tell |
| Did the review’s authors do enough to assess quality of the included studies? | Review quality was not stated | Review quality was not stated | Review quality was not stated |
| If the results of the review have been combined, was it reasonable to do so? | Cannot tell | Cannot tell | Cannot tell |
| What are the overall results of the review? | See Table 2 | See Table 2. | See Table 2. |
| How precise are the results? | Results precisely discussed and synthesized | Results precisely discussed and synthesized | Results precisely discussed and synthesized |
| Can the results be applied to the local population? | Cannot tell | Cannot tell | Cannot tell |
| Were all important outcomes considered? | Yes | Yes. | Yes |
| Are the benefits worth the harms and costs? | Cannot tell | Cannot tell | Cannot tell |
References
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of Childhood and Adult Obesity in the United States, 2011–2012. JAMA 2014, 311, 806. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.L.; Medlow, S.; Steinbeck, K. The Health Consequences of Obesity in Young Adulthood. Curr. Obes. Rep. 2016, 5, 30–37. [Google Scholar] [CrossRef]
- Czernichow, S.; Ciangura, C.; Oppert, J.-M. Obesity in the adult. Rev. Prat. 2006, 56, 2275–2281. [Google Scholar] [PubMed]
- Lucchini, C.; Da Fonseca, D. Connaissances et pratiques médicales autour du harcèlement entre adolescents. Perfect. Pédiatrie 2020, 3, 139–146. [Google Scholar] [CrossRef]
- Harrison, K.; Bost, K.K.; McBride, B.A.; Donovan, S.M.; Grigsby-Toussaint, D.S.; Kim, J.; Liechty, J.M.; Wiley, A.; Teran-Garcia, M.; Jacobsohn, G.C. Toward a Developmental Conceptualization of Contributors to Overweight and Obesity in Childhood: The Six-Cs Model: Developmental Ecological Model of Child Obesity. Child Dev. Perspect. 2011, 5, 50–58. [Google Scholar] [CrossRef]
- Santos, A.F.; Martins, M.C.; Fernandes, C.; Bost, K.K.; Veríssimo, M. Relation between Attachment and Obesity in Preschool Years: A Systematic Review of the Literature. Nutrients 2021, 13, 3572. [Google Scholar] [CrossRef]
- Anderson, S.E.; Whitaker, R.C. Attachment Security and Obesity in US Preschool-Aged Children. Arch. Pediatr. Adolesc. Med. 2011, 165, 235–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratt, K.J.; Skelton, J.A. Family Functioning and Childhood Obesity Treatment: A Family Systems Theory-Informed Approach. Acad. Pediatr. 2018, 18, 620–627. [Google Scholar] [CrossRef]
- Berge, J.M.; Rowley, S.; Trofholz, A.; Hanson, C.; Rueter, M.; MacLehose, R.F.; Neumark-Sztainer, D. Childhood Obesity and Interpersonal Dynamics During Family Meals. Pediatrics 2014, 134, 923–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihrshahi, S.; Baur, L.A. What Exposures in Early Life Are Risk Factors for Childhood Obesity? J. Paediatr. Child Health 2018, 54, 1294–1298. [Google Scholar] [CrossRef]
- Bates, C.R.; Buscemi, J.; Nicholson, L.M.; Cory, M.; Jagpal, A.; Bohnert, A.M. Links between the Organization of the Family Home Environment and Child Obesity: A Systematic Review: Home Organization and Child Obesity. Obes. Rev. 2018, 19, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Messina, S. Not Just about Food: An Attachment Perspective on Feeding. Ph.D. Thesis, University of Texas at Austin, Austin, TX, USA, 2016. [Google Scholar]
- Bergmeier, H.; Skouteris, H.; Hetherington, M. Systematic Research Review of Observational Approaches Used to Evaluate Mother-Child Mealtime Interactions during Preschool Years. Am. J. Clin. Nutr. 2015, 101, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Bergmeier, H.; Skouteris, H.; Horwood, S.; Hooley, M.; Richardson, B. Associations between Child Temperament, Maternal Feeding Practices and Child Body Mass Index during the Preschool Years: A Systematic Review of the Literature: Temperament and Weight of Preschoolers. Obes. Rev. 2014, 15, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.E.; Keim, S.A. Parent–Child Interaction, Self-Regulation, and Obesity Prevention in Early Childhood. Curr. Obes. Rep. 2016, 5, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Vohs, K.D.; Baumeister, R.F. (Eds.) Handbook of Self-Regulation: Research, Theory, and Applications; Guilford Publications: New York, NY, USA, 2016. [Google Scholar]
- Smith, K.E.; Luo, S.; Mason, T.B. A Systematic Review of Neural Correlates of Dysregulated Eating Associated with Obesity Risk in Youth. Neurosci. Biobehav. Rev. 2021, 124, 245–266. [Google Scholar] [CrossRef] [PubMed]
- Alexander, K.E.; Siegel, H.I. Perceived Hunger Mediates the Relationship between Attachment Anxiety and Emotional Eating. Eat. Behav. 2013, 14, 374–377. [Google Scholar] [CrossRef]
- Rommel, D.; Nandrino, J.-L.; Ducro, C.; Andrieux, S.; Delecourt, F.; Antoine, P. Impact of Emotional Awareness and Parental Bonding on Emotional Eating in Obese Women. Appetite 2012, 59, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, J.; Shaver, P.R. (Eds.) Handbook of Attachment: Theory, Research, and Clinical Applications; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Reisz, S.; Aviles, A.I.; Messina, S.; Duschinsky, R.; Jacobvitz, D.; Hazen, N. Fathers’ Attachment Representations and Infant Feeding Practices. Appetite 2019, 142, 104374. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R.; Pereg, D. Attachment Theory and Affect Regulation: The Dynamics, Development, and Cognitive Consequences of Attachment-Related Strategies. Motiv. Emot. 2003, 27, 77–102. [Google Scholar] [CrossRef]
- Cooke, J.E.; Kochendorfer, L.B.; Stuart-Parrigon, K.L.; Koehn, A.J.; Kerns, K.A. Parent–Child Attachment and Children’s Experience and Regulation of Emotion: A Meta-Analytic Review. Emotion 2019, 19, 1103–1126. [Google Scholar] [CrossRef]
- Groh, A.M.; Narayan, A.J. Infant Attachment Insecurity and Baseline Physiological Activity and Physiological Reactivity to Interpersonal Stress: A Meta-Analytic Review. Child Dev. 2019, 90, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, F.; Molteni, R.; Racagni, G.; Riva, M.A. Neuronal Plasticity: A Link between Stress and Mood Disorders. Psychoneuroendocrinology 2009, 34, S208–S216. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Bixler, E.O. Short Sleep and Obesity: Are Poor Sleep, Chronic Stress, and Unhealthy Behaviors the Link? Sleep 2008, 31, 1203. [Google Scholar]
- Ainsworth, M. Attachment, 1st ed.; Wiley: New York, NY, USA, 1984; pp. 559–602. [Google Scholar]
- Gicevic, S.; Aftosmes-Tobio, A.; Manganello, J.A.; Ganter, C.; Simon, C.L.; Newlan, S.; Davison, K.K. Parenting and Childhood Obesity Research: A Quantitative Content Analysis of Published Research 2009–2015. Obes. Rev. 2016, 17, 724–734. [Google Scholar] [CrossRef]
- Hughes, S.O.; Power, T.G.; Papaioannou, M.A.; Cross, M.B.; Nicklas, T.A.; Hall, S.K.; Shewchuk, R.M. Emotional Climate, Feeding Practices, and Feeding Styles: An Observational Analysis of the Dinner Meal in Head Start Families. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiese, B.H. Routines and Rituals: Opportunities for Participation in Family Health. OTJR Occup. Particip. Health 2007, 27 (Suppl. 1), 41S–49S. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.J.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental Constructs in Food Parenting Practices: A Content Map to Guide Future Research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef] [Green Version]
- Fiese, B.H.; Bost, K.K. Family Ecologies and Child Risk for Obesity: Focus on Regulatory Processes: Family Ecologies and Child Risk for Obesity. Fam. Relat. 2016, 65, 94–107. [Google Scholar] [CrossRef]
- Marsh, S.; Gerritsen, S.; Taylor, R.; Galland, B.; Parag, V.; Maddison, R. Promotion of Family Routines and Positive Parent-Child Interactions for Obesity Prevention: Protocol for the 3 Pillars Study Randomized Controlled Trial. JMIR Res. Protoc. 2019, 8, e12792. [Google Scholar] [CrossRef]
- Burgess-Champoux, T.L.; Larson, N.; Neumark-Sztainer, D.; Hannan, P.J.; Story, M. Are Family Meal Patterns Associated with Overall Diet Quality during the Transition from Early to Middle Adolescence? J. Nutr. Educ. Behav. 2009, 41, 79–86. [Google Scholar] [CrossRef]
- Yuasa, K.; Sei, M.; Takeda, E.; Ewis, A.A.; Munakata, H.; Onishi, C.; Nakahori, Y. Effects of Lifestyle Habits and Eating Meals Together with the Family on the Prevalence of Obesity among School Children in Tokushima, Japan: A Cross-Sectional Ques-Tionnaire-Based Survey. J. Med. Invest. 2008, 55, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kininmonth, A.R.; Smith, A.D.; Llewellyn, C.H.; Dye, L.; Lawton, C.L.; Fildes, A. The Relationship between the Home Environment and Child Adiposity: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 4. [Google Scholar] [CrossRef]
- Heilmann, A.; Rouxel, P.; Fitzsimons, E.; Kelly, Y.; Watt, R.G. Longitudinal Associations between Television in the Bedroom and Body Fatness in a UK Cohort Study. Int. J. Obes. 2017, 41, 1503–1509. [Google Scholar] [CrossRef] [Green Version]
- de Moraes Ferrari, G.L.; Araújo, T.L.; Oliveira, L.C.; Matsudo, V.; Fisberg, M. Association between Electronic Equipment in the Bedroom and Sedentary Lifestyle, Physical Activity, and Body Mass Index of Children. J. Pediatr. (Rio J.) 2015, 91, 574–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkin, A.J.; Corder, K.; van Sluijs, E.M.F. Bedroom Media, Sedentary Time and Screen-Time in Children: A Longitudinal Analysis. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 137. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.-L.; Esquivel, J.H.; Guo, J.; Chesla, C.A.; Tang, S. Risk Factors for Obesity in Preschool-Aged Children in China. Int. Nurs. Rev. 2018, 65, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.M.; Arnold, A.; Marshall, D.; McCargar, L.J.; Raine, K.D.; Willows, N.D. Associations among the Food Environment, Diet Quality and Weight Status in Cree Children in Québec. Public Health Nutr. 2009, 12, 1504–1511. [Google Scholar] [CrossRef] [Green Version]
- Spagnola, M.; Fiese, B.H. Family Routines and Rituals: A Context for Development in the Lives of Young Children. Infants Young Child. 2007, 20, 284–299. [Google Scholar] [CrossRef] [Green Version]
- Wendland, B.E.; Atkinson, L.; Steiner, M.; Fleming, A.S.; Pencharz, P.; Moss, E.; Gaudreau, H.; Silveira, P.P.; Arenovich, T.; Matthews, S.G.; et al. Low Maternal Sensitivity at 6 Months of Age Predicts Higher BMI in 48 Month Old Girls but Not Boys. Appetite 2014, 82, 97–102. [Google Scholar] [CrossRef]
- Poulin, M.H. Relations Entre La Pratique Des Routines Familiales, Le Style d’attachement Maternel, l’adaptation Du Parent et l’adaptation Des Enfants d’âge Scolaire; Université du Québec: Québec City, Canada, 2012. [Google Scholar]
- Saltzman, J.A. Family Chaos, Attachment Security, and Responsiveness: Associations with Appetite Self-Regulation in Early Childhood. Ph.D. Thesis, University of Illinois at Urbana-Champaign, Champaign, IL, USA, 2018. [Google Scholar]
- Thamotharan, S.; Lange, K.; Zale, E.L.; Huffhines, L.; Fields, S. The Role of Impulsivity in Pediatric Obesity and Weight Status: A Meta-Analytic Review. Clin. Psychol. Rev. 2013, 33, 253–262. [Google Scholar] [CrossRef]
- Groesz, L.M.; McCoy, S.; Carl, J.; Saslow, L.; Stewart, J.; Adler, N.; Laraia, B.; Epel, E. What Is Eating You? Stress and the Drive to Eat. Appetite 2012, 58, 717–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evers, C.; Marijn Stok, F.; de Ridder, D.T.D. Feeding Your Feelings: Emotion Regulation Strategies and Emotional Eating. Pers. Soc. Psychol. Bull. 2010, 36, 792–804. [Google Scholar] [CrossRef] [Green Version]
- Russell, A.; Russell, C.G. Appetite Self-Regulation Declines across Childhood While General Self-Regulation Improves: A Narrative Review of the Origins and Development of Appetite Self-Regulation. Appetite 2021, 162, 105178. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The Integrative Review: Updated Methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Sabatier, C.; Restrepo Cervantes, D.; Moreno Torres, M.; Hoyos De los Rios, O.; Palacio Sañudo, J. Regulación Emocional En Niños y Adolescentes: Conceptos, Procesos e Influencias. Psicol. Desde El Caribe 2017, 34, 75–90. [Google Scholar] [CrossRef]
- Brumariu, L.E. Parent-Child Attachment and Emotion Regulation: Parent-Child Attachment and Emotion Regulation. New Dir. Child Adolesc. Dev. 2015, 2015, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Guedeney, A.; Guedeney, N.; Tereno, S. L’attachement: Approche Théorique et Évaluation; Elsevier Health Sciences: Issy-les-Moulineaux, France, 2021. [Google Scholar]
- National Heart Lung and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 27 February 2023).
- Burnett, A.J.; Lamb, K.E.; McCann, J.; Worsley, A.; Lacy, K.E. Parenting Styles and the Dietary Intake of Pre-School Children: A Systematic Review. Psychol. Health 2020, 35, 1326–1345. [Google Scholar] [CrossRef]
- Beckers, D.; Karssen, L.T.; Vink, J.M.; Burk, W.J.; Larsen, J.K. Food Parenting Practices and Children’s Weight Outcomes: A Systematic Review of Prospective Studies. Appetite 2021, 158, 105010. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Check Lists. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 22 March 2023).
- Saltzman, J.A.; Fiese, B.H.; Bost, K.K.; McBride, B.A. Development of Appetite Self-Regulation: Integrating Perspectives from Attachment and Family Systems Theory: Corrigendum. Child Dev. Perspect. 2018, 12, 269. [Google Scholar] [CrossRef]
- Bergmeier, H.; Paxton, S.J.; Milgrom, J.; Anderson, S.E.; Baur, L.; Hill, B.; Lim, S.; Green, R.; Skouteris, H. Early Mother-Child Dyadic Pathways to Childhood Obesity Risk: A Conceptual Model. Appetite 2020, 144, 104459. [Google Scholar] [CrossRef]
- Hardman, C.A.; Christiansen, P.; Wilkinson, L.L. Using Food to Soothe: Maternal Attachment Anxiety Is Associated with Child Emotional Eating. Appetite 2016, 99, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasztak-Opiłka, A.; de Jonge, R.; Zachurzok, A.; Górnik-Durose, M.E. Adult Attachment Styles and Mothers’ Life Satisfaction in Relation to Eating Behaviors in the Families with Overweight and Obese Children. PLoS ONE 2020, 15, e0243448. [Google Scholar] [CrossRef] [PubMed]
- Lamson, A.L.; Didericksen, K.W.; Winter, A.; Brimhall, A.S.; Lazorick, S. Attachment, Parenting, and Obesogenic Behavior: A Dyadic Perspective. J. Marital Fam. Ther. 2020, 46, 455–470. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.M.; Frankel, L.A.; Umemura, T.; Hazen, N. The Relationship between Adult Attachment Orientation and Child Self-Regulation in Eating: The Mediating Role of Persuasive-Controlling Feeding Practices. Eat. Behav. 2017, 26, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Bost, K.K.; Wiley, A.R.; Fiese, B.; Hammons, A.; McBride, B. Associations Between Adult Attachment Style, Emotion Regulation, and Preschool Children’s Food Consumption. J. Dev. Behav. Pediatr. 2014, 35, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Pickler, R.H. Understanding, Promoting, and Measuring the Effects of Mother-Infant Attachment During Infant Feeding. J. Obstet. Gynecol. Neonatal Nurs. 2009, 38, 468–469. [Google Scholar] [CrossRef]
- Messina, S.; Reisz, S.; Hazen, N.; Jacobvitz, D. Not Just about Food: Attachments Representations and Maternal Feeding Practices in Infancy. Attach. Hum. Dev. 2020, 22, 514–533. [Google Scholar] [CrossRef]
- Golan, M.; Bachner-Melman, R. Self-Regulation and the Management of Childhood Obesity. J. Community Med. Health Educ. 2011, 1, 2. [Google Scholar] [CrossRef]
- Frankel, L.A.; Hughes, S.O.; O’Connor, T.M.; Power, T.G.; Fisher, J.O.; Hazen, N.L. Parental Influences on Children’s Self-Regulation of Energy Intake: Insights from Developmental Literature on Emotion Regulation. J. Obes. 2012, 2012, 327259. [Google Scholar] [CrossRef] [Green Version]
- Evans, G.W.; Gonnella, C.; Marcynyszyn, L.A.; Gentile, L.; Salpekar, N. The Role of Chaos in Poverty and Children’s Socioemotional Adjustment. Psychol. Sci. 2005, 16, 560–565. [Google Scholar] [CrossRef]
- Rodgers, R.F.; Paxton, S.J.; McLean, S.A.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Maternal Negative Affect Is Associated with Emotional Feeding Practices and Emotional Eating in Young Children. Appetite 2014, 80, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Paxton, S.J.; Massey, R.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Maternal Feeding Practices Predict Weight Gain and Obesogenic Eating Behaviors in Young Children: A Prospective Study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maunder, R.G.; Hunter, J.J. Attachment and Psychosomatic Medicine: Developmental Contributions to Stress and Disease. Psychosom. Med. 2001, 63, 556–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afonso, L.; Lopes, C.; Severo, M.; Santos, S.; Real, H.; Durão, C.; Moreira, P.; Oliveira, A. Bidirectional Association between Parental Child-Feeding Practices and Body Mass Index at 4 and 7 y of Age. Am. J. Clin. Nutr. 2016, 103, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Rhee, K.E.; Coleman, S.M.; Appugliese, D.P.; Kaciroti, N.A.; Corwyn, R.F.; Davidson, N.S.; Bradley, R.H.; Lumeng, J.C. Maternal Feeding Practices Become More Controlling After and Not Before Excessive Rates of Weight Gain. Obesity 2009, 17, 1724–1729. [Google Scholar] [CrossRef]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting Styles, Feeding Styles, Feeding Practices, and Weight Status in 4–12 Year-Old Children: A Systematic Review of the Literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef] [Green Version]
- Spoor, S.T.P.; Bekker, M.H.J.; Van Strien, T.; van Heck, G.L. Relations between Negative Affect, Coping, and Emotional Eating. Appetite 2007, 48, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Waller, E.; Scheidt, C.E. Somatoform Disorders as Disorders of Affect Regulation: A Development Perspective. Int. Rev. Psychiatry 2006, 18, 13–24. [Google Scholar] [CrossRef]
- Oskis, A.; Clow, A.; Hucklebridge, F.; Bifulco, A.; Jacobs, C.; Loveday, C. Understanding Alexithymia in Female Adolescents: The Role of Attachment Style. Personal. Individ. Differ. 2013, 54, 97–102. [Google Scholar] [CrossRef]
- Casagrande, M.; Boncompagni, I.; Forte, G.; Guarino, A.; Favieri, F. Emotion and Overeating Behavior: Effects of Alexithymia and Emotional Regulation on Overweight and Obesity. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2020, 25, 1333–1345. [Google Scholar] [CrossRef]
- Hagger, M.S.; Rebar, A.L. Habits. In The Wiley Encyclopedia of Health Psychology; Paul, R.H., Salminen, L.E., Heaps, J., Cohen, L.M., Eds.; Wiley: Hoboken, NJ, USA, 2020; pp. 177–182. [Google Scholar] [CrossRef]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Preparing People for Change, 2nd ed.; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Cárcamo, R.A.; van Jzendoorn, M.H.I.; Vermeer, H.J.; van der Veer, R. The Validity of the Massie-Campbell Attachment During Stress Scale (ADS). J. Child Fam. Stud. 2013, 23, 767–775. [Google Scholar] [CrossRef]
- Viaux-Savelon, S.; Leclere, C.; Aidane, E.; Bodeau, N.; Camon-Senechal, L.; Vatageot, S.; Feldman, R.; Cohen, D. Validation de la version française du Coding Interactive Behavior sur une population d’enfants à la naissance et à 2 mois. Neuropsychiatr. Enfance Adolesc. 2014, 62, 53–60. [Google Scholar] [CrossRef]
- Roosen, M.A.; Safer, D.; Adler, S.; Cebolla, A.; van Strien, T. Terapia dialéctico-comportamental grupal adaptada para el tratamiento “comedores emocionales” obesos; un estudio piloto. Nutr. Hosp. 2012, 27, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, Processes and Outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Strien, T. Causes of Emotional Eating and Matched Treatment of Obesity. Curr. Diab. Rep. 2018, 18, 35. [Google Scholar] [CrossRef] [Green Version]
- van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for Assessment of Restrained, Emotional, and External Eating Behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Bateman, A.; Fonagy, P. Mentalization Based Treatment for Borderline Personality Disorder. World Psychiatry 2010, 9, 11–15. [Google Scholar] [CrossRef]
- Pugliese1, J.; Lecours, S.; Boucher, M.-È. Régulation émotionnelle et alexithymie: Des précurseurs des conduites alimentaires à risque. Rev. Québécoise Psychol. 2019, 40, 235–261. [Google Scholar] [CrossRef]
- Vazquez, C.E.; Cubbin, C. Socioeconomic Status and Childhood Obesity: A Review of Literature from the Past Decade to Inform Intervention Research. Curr. Obes. Rep. 2020, 9, 562–570. [Google Scholar] [CrossRef]
- Goisis, A.; Martinson, M.; Sigle, W. When Richer Doesn’t Mean Thinner: Ethnicity, Socioeconomic Position, and the Risk of Child Obesity in the United Kingdom. Demogr. Res. 2019, 41, 649–678. [Google Scholar] [CrossRef] [Green Version]


| Developmental Period | Characteristics |
|---|---|
| Early developmental period (heteroregulation); 0–2 years. | The child’s self-regulatory processes are primarily conditioned by his/her environment, particularly by the GC. The latter are directly involved in modulating the child’s expressions at a feeding, emotional, and behavioral level [51]. |
| Second developmental period (transition from heteroregulation to more autonomous regulation); 2–8 years. | The child becomes more autonomous, acquires and applies self-regulation strategies but is still be dependent on interpersonal regulation, especially CG responses. As he/she grows and becomes less dependent on the parent–child dyadic relationship, the child turns to extended social support from friends, and other adults in his/her environment [51,52]. |
| Third developmental period (autonomy); 8–18 years. | The child/adolescent is considered autonomous in his or her self-regulation capacities. He/she is an active partner in the relationship with an individualized opinion [53], no longer needing the proximity with his CG to help him/her self-regulate, but their availability and accessibility [53]. The child has a repertoire of numerous self-regulation strategies provided by the different interpersonal past and present experiences. |
| a. Attachment, Feeding Practices, Childhood Obesity | |||
|---|---|---|---|
| Reference | Sample | Method | Key Findings |
| Reisz et al. (2019) [21] Fathers’ attachment representations and infant feeding practices. UK and USA Quality: Fair | n = 118 Fathers Mean Age: 30 year-old (y-o) fathers Child: Age: From birth to 8-month-old (m-o) infants 41% female Ethnicity: 82% white Education: Well educated Socio-economic Status (SES): Middle-class | Design: Empirical, longitudinal (L) (11 months) Measures: T1 (Third trimester of pregnancy) Semi-structured interview Adult Attachment Interview (AAI): Autonomous, dismissing, preoccupied, unresolved state of mind T2 (8-m-o infants): Observational assessment tool (Feeding Scale: videotape and coding scale): attunement, conflict, control Child’s weight: not reported (NR) | Fathers were more controlling with their sons than with their daughters, regardless of their attachment representation (p = 0.02). Secure fathers:
|
| Reference | Method | Key findings | |
| Bergmeier, et al., 2020 [59] Early mother–child dyadic pathways to childhood obesity risk: A conceptual model. Australia Quality: Not measured (NM) | Literature review: Focus on parent–child relationships to help understand pathways that lead from parent–child feeding interactions to child body mass index Developmental stages included:
| Attachment:
| |
| b. Attachment, family routines, and childhood obesity | |||
| Reference | Sample | Method | Key Findings |
| Saltzman et al. (2018b) [45] Family chaos, attachment security, and responsiveness: Associations with appetite self-regulation in early childhood USA Quality: Good | n = 110 families Parent Mean Age: 30.90 years Maternal ethnicity: 80.90% white Education: Well educated SES: Average, high income Child: Mean Age: 20.97 months (17.80–34.90) 51.40% female | Design: Empirical, L However, (CD) time points not determined Measures: Family: Mealtime routines and Household Chaos (HC): Mother self-report: CHAOS: Confusion, Hubbub and Order Scale (CHAOS); Family Ritual Questionnaire (FRQ); Relationship Scales Questionnaire (RSQ); Caregiver Feeding Styles Questionnaire (CFSQ); Coping with Children’s Negative Emotions Scale (CCNES); Children’s Eating Behavior Questionnaire (CEBQ); Infant Behaviors Questionnaire -Revised (IBQR). Maternal attachment: Scriptedness and insecurity (dismissing) and fearful: Semi-structured interview: The Attachment Script Assessment (ASA) Responsiveness: (feeding and emotional responsiveness during mealtimes and in general) and Child’s appetite dysregulation (Responsiveness to food and emotional overeating) Observational data: The observational Feeding Behavior Coding System (FBCS method; mealtime videos) Child’s weight: NR | HC, feeding routines, and maternal responsiveness are directly associated with the child’s appetite dysregulation (p < 0.05). More dinner routines were associated with less appetite dysregulation in children with highly insecure mothers (p < 0.05). Dinner routines were not associated with appetite dysregulation in children of more insecure mothers; they are considered protective factors for these children (p < 0.05). HC was associated with higher levels of appetite dysregulation in children whose mothers had low levels of emotional responsiveness (p < 0.05). HC was not associated with different levels of appetite dysregulation in children whose mothers reported high levels of emotional responsiveness (p < 0.05). |
| Reference | Method | Key Findings | |
| Saltzman et al. (2018a) [58] Development of appetite self-regulation: Integrating perspectives from attachment and family systems theory USA Quality: NR | Literature review: Includes research from attachment and family system theories regarding the influence of individual, dyadic, and family factors on the development of children’s appetite self-regulation abilities Developmental stages included: Infancy–Early childhood | Risk pathway:
| |
| c. Attachment, feeding practices, family routines, childhood obesity | |||
| Reference | Method | Key Findings | |
| Fiese and Bost (2016) [32] Family ecologies and child risk for obesity: Focus on regulatory processes USA Quality: NR | Literature review: Focus on specific proximal regulatory processes that connect different ecologies (biological regulation, child regulation, family regulation, food environment regulation) implicated in the increase or decrease in child’s obesity risk Developmental stages included: CD | Individual biology
Family routines represent a context where the child’s negative emotions can be answered to and socialized, especially during mealtimes. If negative affect is associated with a struggle around eating, there is less opportunity for a positive learning of self-regulation. When the family environment is unpredictable, then the fluidity of essential interactions for a healthy development is disrupted. | |
| a. Attachment, Feeding Practices, Childhood Obesity | |||
|---|---|---|---|
| Reference | Sample | Method | Key Findings |
| Powell et al., (2017) [63] The relationship between adult attachment orientation and child self-regulation in eating: The mediating role of persuasive-controlling feeding practices. USA Quality: Good | n = 265 68.3% mothers Mean Age = 31.37 Child: Mean Age = 4.17 (range 2.12–7.03) Ethnicity: 72.9% White SES: Average, high income | Design: Empirical, cross-sectional (CS) Measures: Self-reports: Adult attachment: Relationship structures questionnaire of the Experiences in Close Relationships—Revised (ECR-RS): anxiety and avoidance Parental feeding practice: The Feeding Practices and Structure Questionnaire (FPSQ): persuasive feeding (reward for behavior and for eating) Child eating self-regulation: Child Eating and Behavior Questionnaire (CEBQ): self-regulated eating (emotional overeating, food responsiveness) Child’s weight: NR | The relationship between anxious parental attachment style and the child’s self-regulatory abilities is significant when mediated by persuasive feeding. High levels of anxious parental attachment:
When controlling for gender, the significant associations were stronger for fathers than for mothers (p < 0.001). |
| Hardman et al. (2016) [60] Using food to soothe: Maternal attachment anxiety is associated with child emotional eating. UK Quality: Fair | n = 77 Mother Mean Age: 39.23 BMI: 25.93 Child Mean Age: 8.3 (range 3–12) 51% female BMI z-scores: 0.17 Education: Majority educated | Design: Empirical, CS Measures, Self-reports: Maternal: Attachment: Experiences in close Relationships (ERC): anxiety Disinhibited eating: Three Factor Eating Questionnaire (TFEQ) Emotional feeding strategies: Parental Feeding Strategies Questionnaire (PFSQ). Child emotional eating (CEBQ) Weight: Self-report (mother), BMI Z-scores (child) | Mothers with Anxious attachment:
|
| b. Attachment, feeding practices, family routines, childhood obesity | |||
| Reference | Sample | Method | Key findings |
| Bost et al. (2014) [64] Associations between adult attachment style, emotion regulation, and preschool children’s food consumption. USA Quality: Fair | n = 497 families Caregiver’s Mean Age: 32.45 90% female Education Well educated SES Average Child Mean Age (month): 39.04 (range: 2.5–3.5 years) Ethnicity 70%: White | Design: Empirical, CS Measures: Self-report: Adult attachment: (RSQ): anxious/fearful, dismissing/avoidant, secure CG responses to their children’s negative emotion: The Coping with Children’s Negative Emotion Scale (CCNES): distress, punitive, minimization emotion or problem focused reaction Expressive encouragement CG feeding styles: Comprehensive Feeding Practices Questionnaire (CFPQ): emotion-related pressuring feeding and healthy eating styles Family Mealtime Routine: Family Ritual Questionnaire (FRQ): frequency, planning, communication Child television viewing and food consumption: Early Childhood Longitudinal Study-B (ECLS-B): index of total minutes child television viewing CG depression/anxiety: Depression Anxiety Stress Scales (DASS) Weight: CG BMI communicated in descriptive data, no mention of child BMI, nor the assessment weight method | Links between:
|
| a. Attachment, Family Routines, Childhood Obesity | |||
|---|---|---|---|
| Reference | Sample | Method | Key Findings |
| Pasztak-Opiłka et al. (2020) [61] Adult attachment styles and mothers’ life satisfaction in relation to eating behaviors in the families with overweight and obese children Poland Quality: Fair | n = 52 dyads Mothers Mean Age = 41.81 Child: Mean Age: 14 (range: 11–18 years) BMI: 19% overweight 81% obesity Education: Secondary school (42%) SES: Average and high income | Design: Empirical, CS Measures: Self-reports: Mother’s attachment: Questionnaire of Attachment styles (KSP): secure, anxious, avoidant Mother’s life satisfaction: Satisfaction with life scale (SWLS) Mother’s Eating Behavior (EB): Eating behaviors questionnaire (KZZ): Positive EB: knowledge and control of nutrition. Negative EB: negative beliefs and cultural customs; regulation of family relationships and emotions; incorrect organization of nutrition One-item scale for financial situation. Weight and height: mother’s self-report Objective measures: Medical diagnosis based on centile grids | Insecure attachment:
|
| Lamson et al. (2020) [62] Attachment, Parenting, and Obesogenic Behavior: A Dyadic Perspective USA Quality: Fair | n = 77 dyads. 86.6% female Parents Mean Age: 37.29 years Education: Elementary and Middle school (48%). Child: 48.7% female Mean Age: 11.93 (range 7–16 years) BMI: 55.3% overweight 30.3% obesity Ethnicity: 77.6% Hispanic | Design: Empirical, CS Measures: Self-reports CG Attachment: Experiences in Close Relationship Structure (ECR-RS): anxiety and avoidance Caregiving behavioral style: Three Factor Eating Questionnaire (TFEQ-R18V2): hyper-activated and deactivated Modeling of obesogenic behaviors: The Family Health Behavior Scale (FHBS) CG and child obesogenic behaviors: The Caregiving System Scale (CSS): individual dietary intake; physical expenditure; health behaviors; self-regulation of eating; uncontrolled and emotional eating. Child Attachment: Parent Modeling of Eating Behaviors Scale (PARM): anxiety and avoidance Objective measure of the child’s BMI: Measured by trained research team | Insecure attached children:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clément, S.; Tereno, S. Attachment, Feeding Practices, Family Routines and Childhood Obesity: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2023, 20, 5496. https://doi.org/10.3390/ijerph20085496
Clément S, Tereno S. Attachment, Feeding Practices, Family Routines and Childhood Obesity: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2023; 20(8):5496. https://doi.org/10.3390/ijerph20085496
Chicago/Turabian StyleClément, Sarah, and Susana Tereno. 2023. "Attachment, Feeding Practices, Family Routines and Childhood Obesity: A Systematic Review of the Literature" International Journal of Environmental Research and Public Health 20, no. 8: 5496. https://doi.org/10.3390/ijerph20085496
APA StyleClément, S., & Tereno, S. (2023). Attachment, Feeding Practices, Family Routines and Childhood Obesity: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health, 20(8), 5496. https://doi.org/10.3390/ijerph20085496