Factors Associated with Higher Body Mass Index, Weight Concern, and Weight Gain in a Multinational Cohort Study of Smokers Intending to Quit

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Entry Criteria
2.3. Recruitment
2.4. Data Collection
2.5. Ethics
2.6. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Demographics
3.3. Smoking History and Outcome
3.4. Weight
3.5. Factors Associated with High BMI at Baseline
3.6. Factors Associated with Baseline Weight Concerns
3.7. Factors Associated with Baseline Confidence to Prevent Weight Gain
3.8. Factors Associated with Weight Gain during the Follow-Up Period
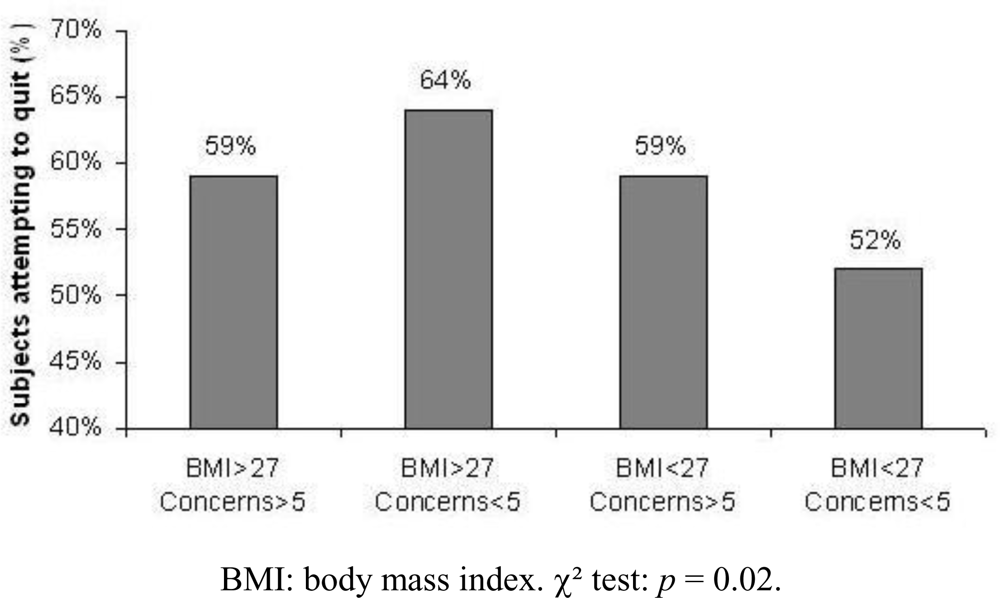
3.9. Impact of Body Mass Index and Weight Concerns on Smoking Cessation Attempts
4. Discussion
Acknowledgments
References
- The 2004 United States Surgeon General's Report: The Health Consequences of Smoking. NSW Public Health Bull 2004, 15, 107.
- Samet, JM. The 1990 Report of the Surgeon General: The Health Benefits of Smoking Cessation. Am. Rev. Respir. Dis 1990, 142, 993–994. [Google Scholar]
- Jeffery, RW; Hennrikus, DJ; Lando, HA; Murray, DM; Liu, JW. Reconciling conflicting findings regarding postcessation weight concerns and success in smoking cessation. Health Psychol 2000, 19, 242–246. [Google Scholar]
- Perkins, KA. Weight gain following smoking cessation. J. Consult. Clin. Psychol 1993, 61, 768–777. [Google Scholar]
- Aronne, LJ. Epidemiology, morbidity, and treatment of overweight and obesity. J. Clin. Psychiatry 2001, 62, 13–22. [Google Scholar]
- Caterson, ID; Gill, TP. Obesity: epidemiology and possible prevention. Best Pract. Res. Clin. Endocrinol. Metab 2002, 16, 595–610. [Google Scholar]
- Albanes, D; Jones, DY; Micozzi, MS; Mattson, ME. Associations between smoking and body weight in the US population: analysis of NHANES II. Am. J. Public Health 1987, 77, 439–444. [Google Scholar]
- Klesges, RC; Klesges, LM; Meyers, AW. Relationship of smoking status, energy balance, and body weight: analysis of the Second National Health and Nutrition Examination Survey. J. Consult. Clin. Psychol 1991, 59, 899–905. [Google Scholar]
- Goldbourt, U; Medalie, JH. Characteristics of smokers, non-smokers and ex-smokers among 10,000 adult males inIsrael. II. Physiologic, biochemical and genetic characteristics. Am. J. Epidemiol 1977, 105, 75–86. [Google Scholar]
- Hjermann, I; Helgeland, A; Holme, I; Lung-Larsen, G; Leren, P. The intercorrelation of serum cholesterol, cigarette smoking and body weight. The Oslo Study. Acta Med. Scand 1976, 200, 479–485. [Google Scholar]
- Wannamethee, G; Shaper, AG. Body weight and mortality in middle aged British men: impact of smoking. BMJ 1989, 299, 1497–1502. [Google Scholar]
- Gordon, T; Kannel, WB; Dawber, TR; McGee, D. Changes associated with quitting cigarette smoking: the Framingham Study. Am. Heart J 1975, 90, 322–328. [Google Scholar]
- Hall, SM; Ginsberg, D; Jones, RT. Smoking cessation and weight gain. J. Consult. Clin. Psychol 1986, 54, 342–346. [Google Scholar]
- Klesges, RC; Winders, SE; Meyers, AW; Eck, LH; Ward, KD; Hultquist, CM; Ray, JW; Shadish, WR. How much weight gain occurs following smoking cessation? A comparison of weight gain using both continuous and point prevalence abstinence. J. Consult. Clin. Psychol 1997, 65, 286–291. [Google Scholar]
- Pisinger, C; Jorgensen, T. Waist circumference and weight following smoking cessation in a general population: the Inter99 study. Prev. Med 2007, 44, 290–295. [Google Scholar]
- Nides, M; Rand, C; Dolce, J; Murray, R; O'Hara, P; Voelker, H; Connett, J. Weight gain as a function of smoking cessation and 2-mg nicotine gum use among middle-aged smokers with mild lung impairment in the first 2 years of the Lung Health Study. Health Psychol 1994, 13, 354–361. [Google Scholar]
- Pirie, PL; Murray, DM; Luepker, RV. Gender differences in cigarette smoking and quitting in a cohort of young adults. Am. J. Public Health 1991, 81, 324–327. [Google Scholar]
- Williamson, DF; Madans, J; Anda, RF; Kleinman, JC; Giovino, GA; Byers, T. Smoking cessation and severity of weight gain in a national cohort. N. Engl. J. Med 1991, 324, 739–745. [Google Scholar]
- Koster, A; Leitzmann, MF; Schatzkin, A; Adams, KF; van Eijk, JT; Hollenbeck, AR; Harris, TB. The combined relations of adiposity and smoking on mortality. Am. J. Clin. Nutr 2008, 88, 1206–1212. [Google Scholar]
- Pednekar, MS; Gupta, PC; Hebert, JR; Hakama, M. Joint effects of tobacco use and body mass on all-cause mortality in Mumbai, India: results from a population-based cohort study. Am. J. Epidemiol 2008, 167, 330–340. [Google Scholar]
- Klesges, RC; Ward, KD; Ray, JW; Cutter, G; Jacobs, DR, Jr; Wagenknecht, LE. The prospective relationships between smoking and weight in a young, biracial cohort: the Coronary Artery Risk Development in Young Adults Study. J. Consult. Clin. Psychol 1998, 66, 987–993. [Google Scholar]
- Gerace, TA; Hollis, J; Ockene, JK; Svendsen, K. Smoking cessation and change in diastolic blood pressure, body weight, and plasma lipids. MRFIT Research Group. Prev. Med 1991, 20, 602–620. [Google Scholar]
- Killen, JD; Fortmann, SP; Newman, B. Weight change among participants in a large sample minimal contact smoking relapse prevention trial. Addict. Behav 1990, 15, 323–332. [Google Scholar]
- Borrelli, B; Mermelstein, R. The role of weight concern and self-efficacy in smoking cessation and weight gain among smokers in a clinic-based cessation program. Addict. Behav 1998, 23, 609–622. [Google Scholar]
- Jarry, JL; Coambs, RB; Polivy, J; Herman, CP. Weight gain after smoking cessation in women: the impact of dieting status. Int. J. Eat. Disord 1998, 24, 53–64. [Google Scholar]
- Klesges, RC; Brown, K; Pascale, RW; Murphy, M; Williams, E; Cigrang, JA. Factors associated with participation, attrition, and outcome in a smoking cessation program at the workplace. Health Psychol 1988, 7, 575–589. [Google Scholar]
- Klesges, RC; Shumaker, SA. Understanding the relations between smoking and body weight and their importance to smoking cessation and relapse. Health Psychol 1992, 11, 1–3. [Google Scholar]
- Meyers, AW; Klesges, RC; Winders, SE; Ward, KD; Peterson, BA; Eck, LH. Are weight concerns predictive of smoking cessation? A prospective analysis. J. Consult. Clin. Psychol 1997, 65, 448–452. [Google Scholar]
- Pomerleau, CS; Zucker, AN; Stewart, AJ. Characterizing concerns about post-cessation weight gain: results from a national survey of women smokers. Nicotine Tob. Res 2001, 3, 51–60. [Google Scholar]
- Weekley, CK, III; Klesges, RC; Reylea, G. Smoking as a weight-control strategy and its relationship to smoking status. Addict. Behav 1992, 17, 259–271. [Google Scholar]
- French, SA; Jeffery, RW; Klesges, LM; Forster, JL. Weight concerns and change in smoking behavior over two years in a working population. Am. J. Public Health 1995, 85, 720–722. [Google Scholar]
- French, SA; Jeffery, RW; Pirie, PL; McBride, CM. Do weight concerns hinder smoking cessation efforts? Addic.t Behav 1992, 17, 219–226. [Google Scholar]
- Pisinger, C; Jorgensen, T. Weight concerns and smoking in a general population: the Inter99 study. Prev. Med 2007, 44, 283–289. [Google Scholar]
- Pinto, BM; Borrelli, B; King, TK; Bock, BC; Clark, MM; Roberts, M; Marcus, BH. Weight control smoking among sedentary women. Addict. Behav 1999, 24, 75–86. [Google Scholar]
- Clark, MM; Hurt, RD; Croghan, IT; Patten, CA; Novotny, P; Sloan, JA; Dakhil, SR; Croghan, GA; Wos, EJ; Rowland, KM; Bernath, A; Morton, RF; Thomas, SP; Tschetter, LK; Garneau, S; Stella, PJ; Ebbert, LP; Wender, DB; Loprinzi, CL. The prevalence of weight concerns in a smoking abstinence clinical trial. Addict. Behav 2006, 31, 1144–1152. [Google Scholar]
- Sorensen, G; Pechacek, TF. Attitudes toward smoking cessation among men and women. J. Behav. Med 1987, 10, 129–137. [Google Scholar]
- Gross, J; Stitzer, ML; Maldonado, J. Nicotine replacement: effects of postcessation weight gain. J. Consult. Clin. Psychol 1989, 57, 87–92. [Google Scholar]
- Killen, JD; Fortmann, SP; Kraemer, HC; Varady, AN; Davis, L; Newman, B. Interactive effects of depression symptoms, nicotine dependence, and weight change on late smoking relapse. J. Consult. Clin. Psychol 1996, 64, 1060–1067. [Google Scholar]
- McBride, CM; French, SA; Pirie, PL; Jeffery, RW. Changes over time in weight concerns among women smokers engaged in the cessation process. Ann. Behav. Med 1996, 18, 273–279. [Google Scholar]
- Norregaard, J; Tonnesen, P; Petersen, L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev. Med 1993, 22, 261–271. [Google Scholar]
- West, R; Gilsenan, A; Coste, F; Zhou, X; Brouard, R; Nonnemaker, J; Curry, SJ; Sullivan, SD. The ATTEMPT cohort: a multi-national longitudinal study of predictors, patterns and consequences of smoking cessation; introduction and evaluation of internet recruitment and data collection methods. Addiction 2006, 101, 1352–1361. [Google Scholar]
- Heatherton, TF; Kozlowski, LT; Frecker, RC; Fagerstrom, KO. The Fagerstrom Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict 1991, 86, 1119–1127. [Google Scholar]
- EuroQol--a new facility for the measurement of health-related quality of life. The EuroQol Group. Health Policy 1990, 16, 199–208.
- Flegal, KM; Carroll, MD; Kuczmarski, RJ; Johnson, CL. Overweight and obesity in the United States: prevalence and trends, 1960–1994. Int. J. Obes. Relat.Metab. Disord 1998, 22, 39–47. [Google Scholar]
- Pirie, PL; McBride, CM; Hellerstedt, W; Jeffery, RW; Hatsukami, D; Allen, S; Lando, H. Smoking cessation in women concerned about weight. Am. J. Public Health 1992, 82, 1238–1243. [Google Scholar]
- Hall, SM; Tunstall, CD; Vila, KL; Duffy, J. Weight gain prevention and smoking cessation: cautionary findings. Am. J. Public Health 1992, 82, 799–803. [Google Scholar]
- Cheskin, LJ; Hess, JM; Henningfield, J; Gorelick, DA. Calorie restriction increases cigarette use in adult smokers. Psychopharmacology (Berl) 2005, 179, 430–436. [Google Scholar]
- Perkins, KA; Marcus, MD; Levine, MD; D'Amico, D; Miller, A; Broge, M; Ashcom, J; Shiffman, S. Cognitive-behavioral therapy to reduce weight concerns improves smoking cessation outcome in weight-concerned women. J. Consult. Clin. Psychol 2001, 69, 604–613. [Google Scholar]


{kind=link}
| Characteristic | Total (n=2,009) | Canada (n=208) | France (n=201) | U.K. (n=200) | U.S. (n=1,400) |
|---|---|---|---|---|---|
| Mean age (years) | 47.9 (SD=8.3) | 46.9 (SD=7.3) | 45.5 (SD=7.4) | 46.2 (SD=7.8) | 48.6 (SD=8.5) |
| Ethnicity (% white) | 90 | 94 | 97 | 97 | 89 |
| Marital status (% married) | 53 | 51 | 48 | 54 | 54 |
| Education (% 14 or more years of formal education*) | 90%* | 55% | 52% | 99%* | |
| Employment status (% full-time, part-time or self-employed) | 67 | 68 | 66 | 68 | 66 |
| Characteristic | Total (n=2,009) | Canada (n=208) | France (n=201) | UK (n=200) | US (n=1,400) |
|---|---|---|---|---|---|
| Mean age when started smoking (years) | 16.7 (SD=5.2) | 16.3 (SD=5.4) | 18.1 (SD=6.3) | 16.3 (SD=4.8) | 16.6 (SD=5.0) |
| Percent having made a quit attempt before | 95 | 96 | 93 | 97 | 95 |
| Median number previous quit attempts | 4 | 4 | 3 | 3 | 4 |
| Mean FTND score | 5.2 (2.3) | 4.8 (2.4) | 4.7 (2.3) | 4.9 (2.4) | 5.4 (2.2) |
| Mean weight (kg)* | 82.6 (19.0) | 80.7 (19.2) | 73.8 (15.7) | 81.3 (17.1) | 84.4 (19.2) |
| Mean BMI (kg/m2) | 28.0 (5.7) | 27.5 (5.8) | 25.3 (4.7) | 27.7 (5.8) | 28.5 (5.8) |
| Mean weight concern scale | 5.5 (2.3) | 5.2 (2.5) | 6.4 (2.4) | 5.4 (2.3) | 5.4 (2.3) |
| Mean confidence to prevent weight gain scale | 5.6 (2.2) | 5.7 (2.3) | 5.2 (2.4) | 4.9 (2.2) | 5.7 (2.1) |
| Dependent variables | Baseline BMI ≥ 27 | Baseline Weight concerns ≥5 | Baseline Weight confidence ≥5 |
|---|---|---|---|
| N | 1986 | 1986 | 1986 |
| Country | <0.0001 | 0.0002 | 0.0001 |
| Education (low/middle/high) | 0.51 | 0.43 | <0.0001 |
| Income (low/middle/high) | 0.20 | 0.71 | 0.0006 |
| Gender | 0.41 | <0.0001 | <0.0001 |
| Marital status (married/single) | 0.41 | 0.076 | 0.56 |
| Cigarettes per day (≥ 20) | 0.0013 | 0.82 | 0.011 |
| Quit attempts in the 3 months previous to baseline | 0.049 | 0.015 | 0.96 |
| Race (white/black/other) | 0.0016 | 0.49 | 0.097 |
| Age (continuous) | 0.59 | <0.0001 | 0.007 |
| Weight concerns (continuous) | <0.0001 | N/A | <0.0001 |
| Weight confidence (continuous) | <0.0001 | <0.0001 | N/A |
| FTND (continuous) | 0.11 | <0.0001 | <0.0001 |
| Quality of Life (continuous) | 0.0002 | 0.010 | <0.0001 |
| BMI (continuous) | N/A | <0.0001 | <0.0001 |
| Effect | Odds ratio | 95% CI |
|---|---|---|
| Body Mass Index ≥ 27 kg/m2 | ||
| Country (versus U.S.A.) | ||
| Canada | 0.828 | 0.604 – 1.136 |
| France | 0.193 | 0.133 – 0.280 |
| United Kingdom | 0.775 | 0.562 – 1.069 |
| Cigarettes/day (≥ 20 versus <20) | 1.308 | 1.073 – 1.593 |
| Quit attempts in the 3 months previous to baseline (Yes versus No) | 1.247 | 1.017–1.529 |
| Race (Black versus White) | 1.683 | 1.072–2.641 |
| Weight concerns (Borrelli scale) | 1.273 | 1.218 – 1.329 |
| Quality of life (EQ-5D score) | 0.611 | 0.425 – 0.879 |
| Weight concerns (≥5) | ||
| Country (versus U.S.A.) | ||
| Canada | 0.686 | 0.482 – 0.976 |
| France | 2.664 | 1.787 – 3.973 |
| United Kingdom | 0.736 | 0.506 – 1.069 |
| Gender (Female versus Male) | 2.147 | 1.724 – 2.673 |
| Age | 0.982 | 0.969 – 0.995 |
| BMI | 1.097 | 1.073 – 1.121 |
| Weight confidence (Borrelli scale) | 0.625 | 0.590 – 0.663 |
| Weight confidence (≥5) | ||
| Country (versus U.S.A.) | ||
| Canada | 0.824 | 0.564 – 1.203 |
| France | 0.978 | 0.660 – 1.449 |
| United Kingdom | 0.410 | 0.283 – 0.594 |
| Educational level (high vs low) | 2.054 | 1.174 – 3.595 |
| Income (medium vs low) | 1.447 | 1.085 – 1.930 |
| Gender (Female versus Male) | 0.768 | 0.612 – 0.965 |
| Nicotine dependence (FTND score) | 0.915 | 0.870 – 0.961 |
| Body Mass Index ≥ 27 kg/m2 | ||
| Quality of life (EQ-5D score) | 1.565 | 1.038 – 2.359 |
| Weight concerns (Borrelli score) | 0.686 | 0.649 – 0.724 |
| Dependent variable | Weight increase ≥5% in 6 months |
|---|---|
| N | 1,284 |
| Country | 0.033 |
| Income (low/middle/high) | 0.013 |
| Gender | 0.041 |
| Marital status (married/single) | 0.0008 |
| Quality of Life (continuous) | 0.074 |
| Cigarette-free days in 6 months (continuous) | <0.0001 |
| Effect | Odds ratio | 95% CI |
|---|---|---|
| Weight increase (≥5%) | ||
| being single | 1.46 | 1.01 – 2.10 |
| 30 days without smoking | 1.35 | 1.31 – 1.52 |
| Low income (low vs medium or high) | 1.48 | 1.03 – 2.14 |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Aubin, H.-J.; Berlin, I.; Smadja, E.; West, R. Factors Associated with Higher Body Mass Index, Weight Concern, and Weight Gain in a Multinational Cohort Study of Smokers Intending to Quit. Int. J. Environ. Res. Public Health 2009, 6, 943-957. https://doi.org/10.3390/ijerph6030943
Aubin H-J, Berlin I, Smadja E, West R. Factors Associated with Higher Body Mass Index, Weight Concern, and Weight Gain in a Multinational Cohort Study of Smokers Intending to Quit. International Journal of Environmental Research and Public Health. 2009; 6(3):943-957. https://doi.org/10.3390/ijerph6030943
Chicago/Turabian StyleAubin, Henri-Jean, Ivan Berlin, Elisheva Smadja, and Robert West. 2009. "Factors Associated with Higher Body Mass Index, Weight Concern, and Weight Gain in a Multinational Cohort Study of Smokers Intending to Quit" International Journal of Environmental Research and Public Health 6, no. 3: 943-957. https://doi.org/10.3390/ijerph6030943
APA StyleAubin, H. -J., Berlin, I., Smadja, E., & West, R. (2009). Factors Associated with Higher Body Mass Index, Weight Concern, and Weight Gain in a Multinational Cohort Study of Smokers Intending to Quit. International Journal of Environmental Research and Public Health, 6(3), 943-957. https://doi.org/10.3390/ijerph6030943