A School-Based Environmental Intervention to Reduce Smoking among High School Students: The Acadiana Coalition of Teens against Tobacco (ACTT)

 ,
,
Abstract
:
1. Introduction
2. Methods
2.1. Design
2.2. Measurement
Health Habits Survey
Data Collection Procedures
2.3. ACTT Intervention Programs
Teacher Workshops
School-Based Media Campaign
Activities
Parent Newsletter
2.4. ACTT Intervention Process Measures
2.5. Statistical Analyses
3. Results
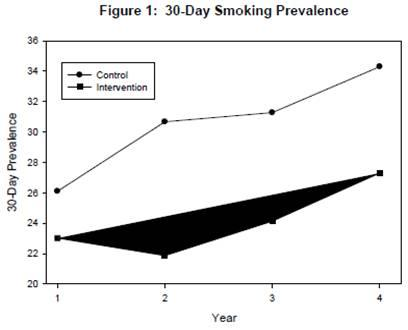
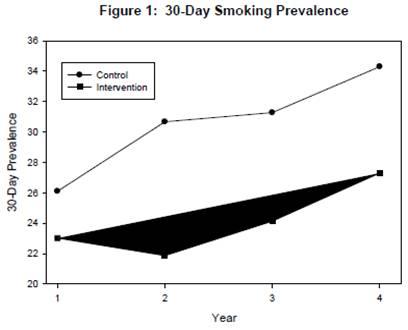
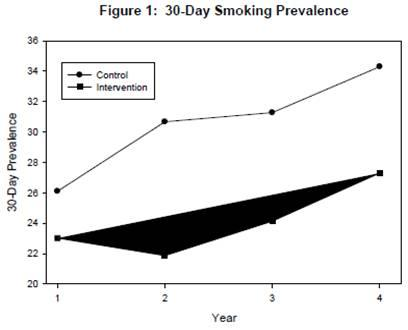
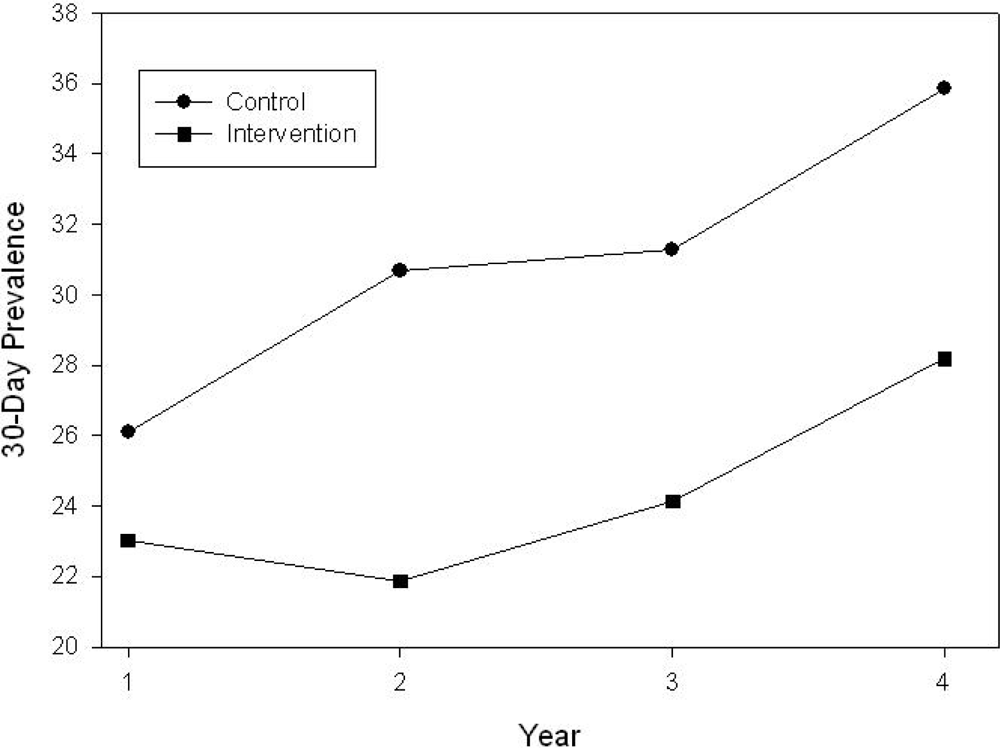
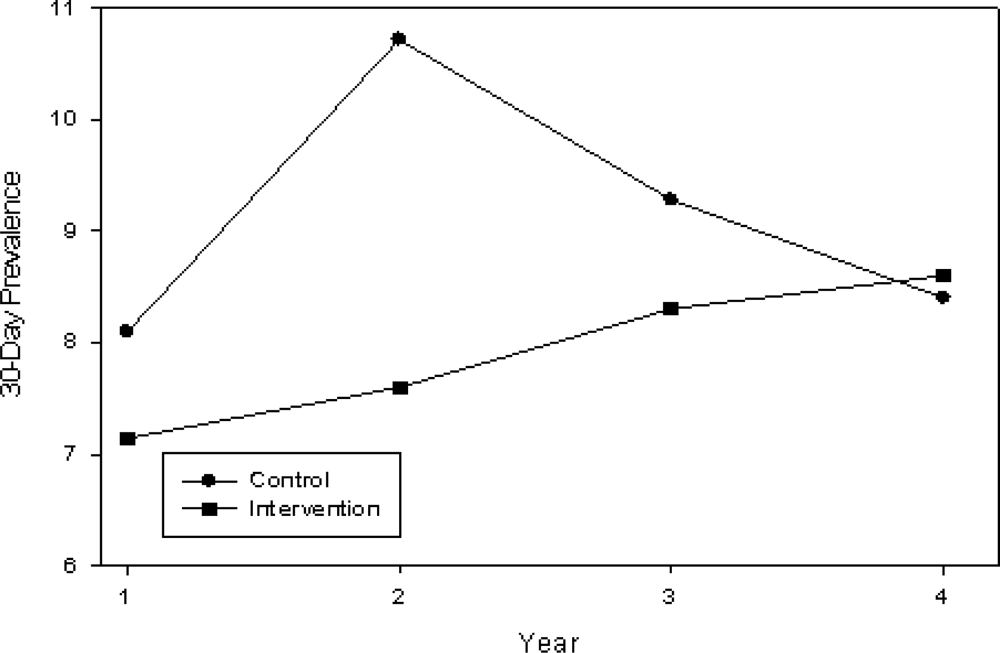
3.1. 30-Day Prevalence of Cigarette Smoking
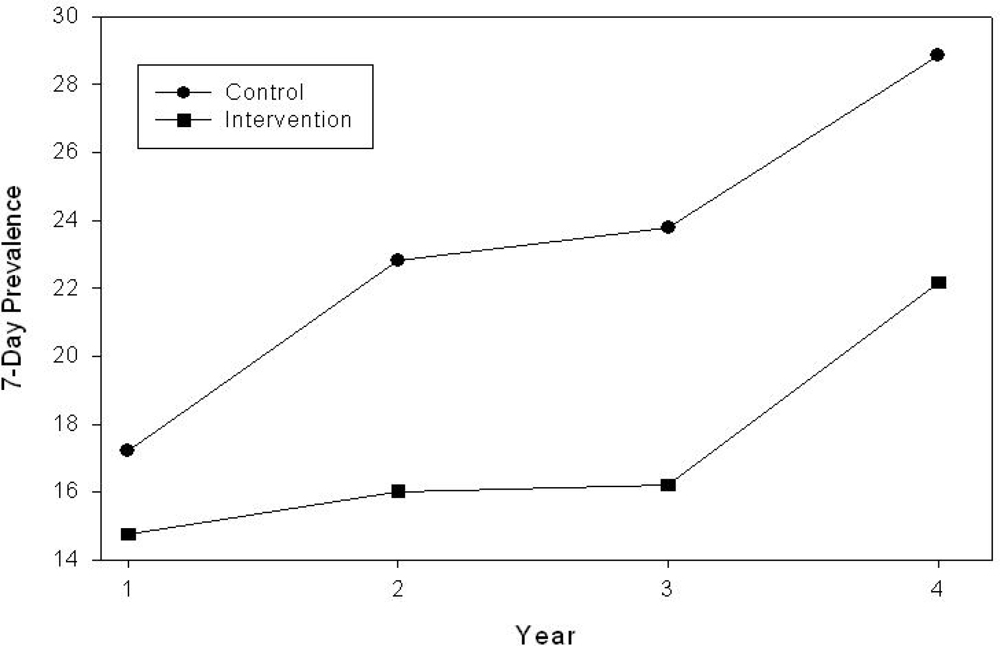
3.2. 7-Day Prevalence of Cigarette Smoking
3.3. 30-Day Prevalence for Smokeless Tobacco
3.4. 30-Day Prevalence by Individual Schools
4. Discussion
4.1. Study Design
4.2. The Intervention
5. Conclusions
Acknowledgments
References and Notes
- Johnston, LD; O’Malley, PM; Bachman, JG. Monitoring the Future national survey results on drug use, 1975–2991, Volume I: Secondary School Students; NIH Publication Nol 02-5106.Bethesda (MD); National Institute on Drug Abuse, 2002; pp. 36–48. [Google Scholar]
- Kann, L; Warren, CW; Harris, WA; Collins, JL; Williams, BI; Ross, JG; Kolbe, LJ. Youth Risk Behavior Surveillance – United States, 1995. MMWR Surveillance Summaries 1996, 45, 1–84. [Google Scholar]
- Kann, L; Warren, W; Collins, JL; Ross, J; Collins, B; Kolbe, LJ. Results from the national school-based 1991 Youth Risk Behavior Survey and progress toward achieving related health objectives for the nation. Public Health Rep 1993, 108, 47–67. [Google Scholar]
- University of Michigan News and Information Services. Cigarette smoking among American teens continues graduate decline; University of Michigan: Ann Arbor, MI, USA, December 17 1999. [Google Scholar]
- U.S. Department of Health and Human Services. Healthy People 2000: National Health Promotion and Disease Prevention Objectives; U.S. Department of Health and Human Services: Washington, D.C., USA, 1990. [Google Scholar]
- US Department of Health and Human Services. Preventing tobacco use among young people: A report of the Surgeon General; Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Promotion, Office on Smoking and Health: Atlanta, GA, USA, 1994. [Google Scholar]
- Spilich, GJ; June, L; Renner, J. Cigarette smoking and cognitive performance. Brit. J. Addict 1992, 87, 1313–1326. [Google Scholar]
- Johnson, EH; Gilbert, D. Familiar and psychological correlates of smoking in black and white adolescents. Ethn. Dis 1991, 1, 320–324. [Google Scholar]
- Johnson, CC; Hunter, SM; Amos, CI; Elder, ST; Berenson, GS. Cigarette smoking, alcohol, and oral contraceptive use by type A adolescent—The Bogalusa Heart Study. J. Behav. Med 1989, 12, 14–24. [Google Scholar]
- American School Health Association. The National Adolescent Student Health Survey; Third Party Publishing: Oakland, CA, USA, 1989. [Google Scholar]
- O’Connell, KA; Cook, MR; Gerkovich, MM; Totocky, M; Swan, GE. Reversal theory and smoking: a state-based approach to ex-smokers’ highly tempting situations. J. Consult. Clin. Psychol 1990, 58, 489–494. [Google Scholar]
- Klesges, RC; Meyers, AW; Klesges, LM; LaVasque, ME. Smoking, body weight, and their effects on smoking behavior: a comprehensive review of the literature. Psychol. Bull 1989, 106, 204–230. [Google Scholar]
- Wilson, JJ. Summary of the attorneys general Master Tobacco Settlement Agreement; 1999; National Conference of State Legislatures: Washington, D.C., USA; Available online: http:academic.udayton.edu/health/syllabi/tobacco/summary.htm (accessed December 2008). [Google Scholar]
- U.S. Department of Health and Human Services. Healthy People 2010 Objectives: draft for public comment; U.S. Department of Health and Human Services: Washington, D.C., USA, 1998. [Google Scholar]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance – United States, 2001. MMWR 2002, 51, 1–64. [Google Scholar]
- Centers for Disease Control and Prevention, Louisiana; Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 1993.
- Campaign for Tobacco-Free Kids. The toll of tobacco in Louisiana.
- Henry, JM; Bankston, CL, III. Ethnic self-identification and symbolic stereotyping: the portrayal of Louisiana Cajuns. Ethn. Racial Stud 2001, 24, 1020–1045. [Google Scholar]
- Johnston, LD; O’Malley, PM; Bachman, JG; Schulenberg, JE. Monitoring the Future national survey results on drug use, 1975–2007: Volume I, secondary school students; (NIH Publication No 08-6418A)National Institute on Drug Abuse: Bethesda, MD, USA, 2008. [Google Scholar]
- U.S. Census Bureau. American FactFinder.
- Glanz, K; Lunde, KB; Leakey, T; Maddock, J; Koga, K; Yamauchi, J; Maskarinec, G; Shigaki, D. Activating multi-ethnic youth for smoking prevention: design, baseline findings and implementation of project SPLASH. J. Cancer Educ 2007, 22, 56–61. [Google Scholar]
- Louisiana Department of Education. Standards, assessments, and accountability: Louisiana’s school, district, and state accountability system.
- Johnson, CC; Myers, L; Webber, LS; Boris, NW. Profiles of the adolescent smoker: models of tobacco use among 9th grade high school students. Acadiana Coalition of Teens against Tobacco (ACTT). Prev. Med 2004, 39, 551–558. [Google Scholar]
- Pechacek, TF; Murray, D; Belcher, JD; Luepker, R. Saliva sample collection manual, molecular epidemiology and biomarkers research laboratory; University of Minnesota: Minneapolis, MN, USA, 1987. [Google Scholar]
- Hong, T; Johnson, CC; Myers, L; Boris, N; Brewer, D; Webber, LS. Process evaluation of an in-school anti-tobacco media campaign in Louisiana. Public Health Rep 2008, 123, 781–789. [Google Scholar]
- Steckler, A; Ethelbah, B; Martin, CJ; Stewart, D; Pardilla, M; Gittelsohn, J; Stone, E; Fenn, D; Smyth, M; Vu, M. Pathways process evaluation results: A school-based prevention trial to promote healthy diet and physical activity in American Indian third, fourth, and fifth grade students. Prev. Med 2003, 37, S80–S90. [Google Scholar]
- Eaton, DK; Kann, L; Kinchen, S; Ross, J; Hawkins, J; Harris, WA; Lowry, R; McManus, T; Chyen, D; Shanklin, S; Lim, C; Grunbaum, JA; Wechsler, H. Youth Risk Behavior Surveillance – United States, 2005. MMWR 2006, 55, 1–108. [Google Scholar]
- Davis, CE; Hunsberger, S; Murray, DM; Fabsitz, RR; Himes, JH; Stephenson, LK; Cabello, B; Skipper, B. Design and statistical analysis for the Pathways Study. Amer. J. Clinical Nutr 1999, 69, 760S–763S. [Google Scholar]
- Zucker, DM; Lakatos, E; Webber, LS; Murray, DM; McKinlay, SM; Feldman, HA; Kelder, SH; Nader, PR. Statistical design of the child and adolescent trial for cardiovascular health (catch): Implications of cluster randomization. Contemp. Clin. Trials 1995, 16, 96–118. [Google Scholar]
- Stevens, J; Murray, DM; Catellier, DJ; Hannan, PJ; Lytle, LA; Elder, JP; Young, DR; Simons-Morton, DG; Webber, LS. Design of the Trial of Activity for Adolescent Girls (TAAG). Contemp. Clin. Trials 2005, 26, 223–233. [Google Scholar]
- Midanik, LT; Polen, MR; Hunkeler, EM; Tekawa, IS; Soghikian, K. Methodologic issues in evaluation stop smoking programs. Amer. J. Public Health 1985, 75, 634–638. [Google Scholar]
- Boris, NW; Johnson, CC; Huang, S; Myers, L; Andrew, K; Webber, LS. Targeting school tobacco policy: Lessons from the Acadiana Coalition of Teens against Tobacco (ACTT). Health Promotion Pract, Prepublished March 26, 2008, doi: 10.1177/1524839907308116.
- Peterson, AV, Jr; Kealey, KA; Mann, SL; Marek, PM; Sarason, IG. Hutchinson Smoking Prevention Project: long-term randomized trial in school-based tobacco use prevention—results on smoking. J. Nat. Cancer Inst 2000, 92, 1979–1991. [Google Scholar]
- Centers for Disease Control and Prevention. Guidelines for school health programs to prevent tobacco use and addiction. MMWR 1994, 43, 1–18. [Google Scholar]
- Pirani, S; Reizes, T. The Turning Point Social Marketing National Excellence Collaborative: integrating social marketing into routine public health practice. J. Public Health Manag. Pract 2005, 11, 131–138. [Google Scholar]
- Summerlin-Long, SK; Goldstein, AO. A statewide movement to promote the adoption of tobacco-free school policies. J. School Health 2008, 78, 625–632. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort Grade Level | Semester | Measurement |
|---|---|---|
| 9th | Fall, 2000 | Formative focus groups |
| 9th | Spring, 2001 | Baseline Health Habits Survey and saliva cotinine sampling |
| 10th | Spring, 2002 | Interim Modified Health Habits Survey* |
| 11th | Spring, 2003 | Modified Health Habits Survey* |
| 12th | Spring, 2004 | Follow-up Health Habits Survey Exit focus groups |
| Cohort Grade Level | Semester | Intervention Activities | |
|---|---|---|---|
| Cohort (Classroom) Only | Schoolwide (Hallway) | ||
| 10th | Fall 2001 | Introduction to program & video
Media contest | “Don’t be a sucker” interactive exhibit
Great American SmokeOut Teacher workshop PSA’s (weekly) Posters (monthly) |
| 10th | Spring 2002 | Kick Butts Day
PSA’s (weekly) Posters (monthly) | |
| 11th | Fall 2002 | Mr. Grossmouth/Jar of Tar
Great American SmokeOut PSA's (weekly) Poster (semester) | |
| 11th | Spring 2003 | Psychodrama | Advocacy
Big Tobacco Valentine's Day cards Kick Butts Day (with pig lungs) PSA's (weekly) Posters (bimonthly) |
| 12th | Fall 2003 | Hats off to seniors | Smoking Roulette
Great American SmokeOut PSA's (weekly) Posters (monthly) |
| 12th | Spring 2004 | Can you handle the TRUTH?
Tobacco Jeopardy Kick Butts Day PSA's (weekly) Posters (monthly) | |
| Activities | Description – Cohort Activities | Semester(s) |
|---|---|---|
| Introduction & video | Introduction to ACTT; interactive quiz about tobacco with questions and prizes. A video “Unfiltered” featured a popular MTV Real World star on a quit smoking weekend with other teens. | Fall, 2001 |
| Media Contest | Cohort volunteered to develop any type of media with an anti-smoking message. Prizes awarded. | Fall, 2001 |
| Valentine Day cards | Four different Valentine Day cards tongue-in-cheek messages from Big Tobacco | Spring, 2003 |
| Psychodrama
| Students competed for trophies by developing, implementing and videotaping a dramatic skit with a smoking prevention theme.
| Spring, 2003
|
| Hats off to seniors
| At an ACTT-sponsored breakfast or lunch, seniors were honored and thanked for participating in the program. Slides of activities at their school were shown on a large screen and table tents contained smoke-free messages.
| Fall, 2003
|
| Description – Schoolwide Activities | ||
| Grossmouth/ Jar of Tar | A chewing tobacco quiz with true/false questions focusing on a display of a model of a diseased mouth and jar with dark liquid representing tar in lungs after smoking one year. | Fall, 2002 |
| Legislative advocacy | Students sent letters to their state senators requesting the repeal of the tobacco preemption law. The law was repealed and the announcement was made in the intervention schools. | Spring, 2003 |
| Smoker’s roulette | Students spun a roulette wheel to identify categories of questions, and, if answered correctly, won prizes. | Fall, 2003 |
| Can you handle the TRUTH? | Can you handle the truth about Big Tobacco messages were placed in strategic places throughout the school. Students wrote anti-smoking messages on banners to be sent to tobacco companies. | Spring, 2004 |
| Jeopardy | Patterned after the TV game, students competed by responding to tobacco facts with a question. | Spring, 2004 |
| Pig lung demonstration | Diseased pig lungs representing a 10-year smoker were touched and examined by students. | Spring 2002, 2003 |
| What’s in a cigarette? | Competitive scavenger hunt for the names of 60 chemicals found in cigarettes which were placed individually around the school. | Spring 2002 |
| Great American SmokeOut | National observance in which pledges not to smoke or to stop smoking were signed by students and teachers and taped to school walls. The grade level with the most pledges won a prize awarded by the school. | Fall, 2001, 2002, 2003 |
| Kick Butts Day | Students asked to join with students nationally to kick butts and participated in various activities. | Spring, 2002, 2003, 2004 |
| Demographic Characteristics | 9th Grade | 12th Grade | ||||
|---|---|---|---|---|---|---|
| Intervention (%) | Control (%) | Total (%) | Intervention (%) | Control (%) | Total (%) | |
| Race/Ethnicity
White African-American | 1,133 (60)
751 (40) | 1,770 (69)
805 (31) | 2,903 (65)
1,556 (35) | 668 (62)
402 (38) | 1,144 (73)
429 (27) | 1,812 (69)
831 (31) |
| Total n | 1,884 | 2,575 | 4,459 | 1,070 | 1,573 | 2,643 |
| Sex
Male Female | 907 (48)
975 (52) | 1,255 (49)
1,317 (51) | 2,162 (49)
2,292 (51) | 456 (43)
613 (57) | 696 (44)
874 (56) | 1,152 (44)
1,487 (56) |
| Total n | 1,882 | 2,572 | 4,454 | 1,069 | 1,570 | 2,639 |
| Age = Mean Years
Range | 15.4
14.0–18.5 | 15.3
11.8–19.0 | 15.4
11.8–19.3 | 18.1
15.6–21.2 | 18.1
14.4–20.4 | 18.1
14.4–21.2 |
| Condition | ||
|---|---|---|
| Control (n = 10) | Intervention (n = 10) | |
| Size of cohort
Mean + SD Small (≤ 175) | 258 + 153
4 | 189 + 136
6 |
| % Male | 48.5 + 5.2 | 49.6 + 5.1 |
| Majority white (> 66.7%) | 7 | 4 |
| Smoking
30 day Prevalence 7 day Prevalence | 26.4 + 4.2
17.2 + 3.0 | 23.0 + 7.0
14.8 + 5.2 |
| Chewing Tobacco
30 day Prevalence | 8.1 + 3.8 | 7.1 + 3.8 |
| Group | |||
|---|---|---|---|
| Control (n = 10) | Intervention (n = 10) | ||
| Year | Mean ± SE | Mean ± SE | F and p values |
| 30-Day Smoking Prevalence | |||
| 1
2 3 4 | 26.1 ± 1.3
30.7 ± 2.5 31.3 ± 3.2 34.3 ± 3.3 | 23.0 ± 2.2
21.9 ± 1.9 24.1 ± 2.5 27.3 ± 3.2 | |
| Year 1 to Year 4 Prevalence Rate | 8.2 ± 2.9 | 4.3 ± 4.2 | F3,54 = 0.99, p = 0.40 |
| 7-Day Smoking Prevalence | |||
| 1
2 3 4 | 17.2 ± 0.9
22.8 ± 2.1 23.8 ± 2.8 27.1 ± 3.2 | 14.8 ± 1.7
16.0 ± 1.5 16.2 ± 2.2 21.5 ± 2.6 | |
| Year 1 to Year 4 Prevalence Rate | 9.9 ± 3.1 | 6.7 ± 3.5 | F3,54 = 1.09, p = 0.36 |
| 30-Day Smokeless Tobacco Prevalence | |||
| 1
2 3 4 | 8.1 ± 1.2
10.7 ± 1.3 9.3 ± 1.1 8.4 ± 1.0 | 7.1 ± 1.2
7.6 ± 0.9 8.3 ± 1.2 8.6 ± 1.3 | |
| Year 1 to Year 4 Prevalence Rate | 0.3 ± 1.3 | 1.5 ± 1.0 | F3,54 = 1.93, p = 0.13 |
| Group Assignment | Grade | |||
|---|---|---|---|---|
| 9th | 12th | |||
| % Prevalence | % White | % Prevalence | % White | |
| 1 | 26.5 | 97.1 | 43.6 | 98.2 |
| 1 | 32.2 | 73.1 | 33.9 | 74.7 |
| 1 | 24.4 | 73.0 | 29.3 | 74.1 |
| 1 | 21.2 | 56.0 | 31.3 | 62.6 |
| 1 | 28.7 | 96.2 | 50.5 | 97.4 |
| 1 | 29.8 | 61.5 | 29.5 | 66.1 |
| 1 | 20.7 | 27.5 | 15.2 | 25.3 |
| 1 | 20.2 | 87.3 | 32.7 | 90.9 |
| 1 | 29.5 | 92.9 | 43.0 | 93.0 |
| 1 | 27.9 | 92.3 | 34.9 | 90.7 |
| 2 | 25.2 | 19.1 | 17.7 | 16.1 |
| 2 | 12.7 | 80.0 | 50.0 | 71.0 |
| 2 | 19.6 | 50.9 | 21.2 | 54.6 |
| 2 | 26.1 | 82.5 | 34.5 | 88.0 |
| 2 | 13.7 | 22.7 | 12.2 | 20.9 |
| 2 | 25.1 | 80.0 | 32.6 | 82.9 |
| 2 | 29.5 | 22.9 | 22.2 | 16.7 |
| 2 | 33.9 | 33.0 | 28.6 | 32.9 |
| 2 | 16.5 | 58.7 | 28.4 | 67.6 |
| 2 | 27.7 | 94.1 | 33.3 | 92.7 |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Johnson, C.C.; Myers, L.; Webber, L.S.; Boris, N.W.; He, H.; Brewer, D. A School-Based Environmental Intervention to Reduce Smoking among High School Students: The Acadiana Coalition of Teens against Tobacco (ACTT). Int. J. Environ. Res. Public Health 2009, 6, 1298-1316. https://doi.org/10.3390/ijerph6041298
Johnson CC, Myers L, Webber LS, Boris NW, He H, Brewer D. A School-Based Environmental Intervention to Reduce Smoking among High School Students: The Acadiana Coalition of Teens against Tobacco (ACTT). International Journal of Environmental Research and Public Health. 2009; 6(4):1298-1316. https://doi.org/10.3390/ijerph6041298
Chicago/Turabian StyleJohnson, Carolyn C., Leann Myers, Larry S. Webber, Neil W. Boris, Hao He, and Dixye Brewer. 2009. "A School-Based Environmental Intervention to Reduce Smoking among High School Students: The Acadiana Coalition of Teens against Tobacco (ACTT)" International Journal of Environmental Research and Public Health 6, no. 4: 1298-1316. https://doi.org/10.3390/ijerph6041298
APA StyleJohnson, C. C., Myers, L., Webber, L. S., Boris, N. W., He, H., & Brewer, D. (2009). A School-Based Environmental Intervention to Reduce Smoking among High School Students: The Acadiana Coalition of Teens against Tobacco (ACTT). International Journal of Environmental Research and Public Health, 6(4), 1298-1316. https://doi.org/10.3390/ijerph6041298