A Review of the Urban Development and Transport Impacts on Public Health with Particular Reference to Australia: Trans-Disciplinary Research Teams and Some Research Gaps

Abstract
:1. Introduction
2. Trans-disciplinary Research Teams
2.1. Trans-Disciplinary – Definition and Methodology
“Transdisciplinary thinking is primarily a process of assembling and mapping the possible interconnections of disciplinary knowledge about any given…problem until the fullest possible understanding of the problem emerges” [10].“Transdisciplinarity is an integrative process in which researchers work jointly to develop and use a shared conceptual framework that synthesizes and extends discipline-specific theories, concepts, methods, or all three to create new models and language to address a common research problem” [8].
- problem definition;
- assembling a team of researchers;
- reviewing existing knowledge on the research problem, especially disciplinary and interdisciplinary conceptualizations and explanations;
- designing the research enquiry from research gaps; implementing the research enquiry;
- refining conceptual understandings and synthesizing data sets; and
- recommending the types of interventions (usually with stakeholders) to resolve the problem.
2.2. Example of Aircraft Noise and Community Health (Stress)
2.3. Trans-Disciplinary Research into Transport and Health
3. Conceptual Representation
4. Literature Review
4.1. Literature on Human Settlements, Density and Heath
4.2. Literature on Transport Impacts on Health
- “Exposure to fine and coarse PM in ambient air has been associated with a short-term increase in mortality and morbidity from cardiovascular and respiratory diseases.
- Studies have found long-term average mortality rates 17% – 26% higher than expected in communities with high levels of fine particulate matter.
- Diesel exhaust and nitrogen dioxide have been tied to increased asthma symptoms and response to allergens.
- Exposure to diesel exhaust has also been associated with increased rates of lung cancer and mortality and morbidity.
- Air toxics can cause negative health effects including cancer and respiratory, neurological, reproductive, and developmental effects.”
- significant increase in the risk of death from cardiopulmonary causes
- significant increase in asthma prevalence in children
- impacts on lung development in children
- increased cardiac arrhythmias
4.3. Literature on Visualization and GIS
4.4. Future Issues – Climate Change
- Association between heavy rainfall and Ross River virus disease.
- Both insects and insect-borne diseases (including malaria and dengue fever) have been experienced at increasingly higher altitudes in Africa, Asia and Latin America.
- Heavy rainfall may cause outbreaks of cryptosporidiosis which causes severe diarrheic diseases in children and can cause death in immuno-compromised individuals.
- An increase of the temperature can activate the blooms and vibrios (cholera) in fishes.
- The emergence of Hantavirus pulmonary syndrome may be linked to heavy rainfall resulting in growth in rodent populations and subsequent disease transmission.
- Extreme flooding or hurricanes can lead to outbreaks of leptospirosis and by their violent nature, natural disasters like storms, floods, cyclones, have the potential to cause morbidity, mortality, and property loss [152].
4.5. Classification of the Knowledge Base and Research Gaps [166]
“The spatial and temporal dynamics of social and environmental determinants of human health in urban systems. Who gets sick and where do they live? What are the relative contributions of social versus environmental factors? What types of interventions are available and appropriate?
Measures of health in different urban forms. What contribution does urban pattern and social–ecological processes in urban environments make to the functionality of urban habitats? Can we identify the characteristics of dysfunctional and functional urban landscapes and incorporate this knowledge into better urban planning, design, construction and management?”
4. Conclusions
Acknowledgments
References
- McMichael, A. Population Health as a Primary Criterion of Sustainability. EcoHealth 2006, 3, 182–186. [Google Scholar]
- de Loof, F; Black, DA; Black, JA. Rural Transport Isolation and Health Outcomes, Results from the Swiss Red Cross Survey in Lao PDR. J. East Asia Soc. Trans. Stud., Environ. Saf 2001, 4, 183–198. [Google Scholar]
- Ramadier, T. Transdisciplinarity and its Challenges, The Case of Urban Studies. Futures 2004, 36, 423–439. [Google Scholar]
- World Conference on Transport Research Society; World Conference on Transport Research Society: Lyon, France, 2009.
- Rosenfield, PL. The Potential of Transdisciplinary Research for Sustaining and Extending Linkages between the Health and Social Sciences. Soc. Sci. Med 1992, 35, 1343–1357. [Google Scholar]
- Wuchty, S; Jones, BF; Uzzi, B. The Increasing Dominance of Teams in Production of Knowledge. Science 2007, 316, 1036–1039. [Google Scholar]
- Stokols, D; Misra, S; Moser, RP; Hall, KL; Taylor, BK. The Ecology of Team Science, Understanding Contextual Influences on Transdisciplinary Collaboration. Am. J. Prev. Med 2008, 35, S96–115. [Google Scholar]
- Stokols, D; Hall, KL; Taylor, BK; Moser, RP. The Science of Team Science, Overview of the Field and Introduction to the Supplement. Am. J. Prev. Med 2008, 35, S77–89. [Google Scholar]
- Rose, RM; Prager, D. Views from the Field: The Value of Interdisciplinary Networks. Available online: http://www.gih.org/usr_doc/Research_Networks_February_2009.pdf (accessed 15 March, 2009).
- Higginbotham, N; Albrecht, G; Connor, L. Health Social Science, A Transdisciplinary and Complexity Perspective; Oxford University Press: Melbourne, Australia, 2001. [Google Scholar]
- Parkes, MW; Bienen, L; Breilh, J; Hsu, L-N; McDonald, M; Patz, JA; Rosenthal, JP; Sahani, M; Sleigh, A; Waltner-Toews, D. All Hands on Deck, Transdisciplinary Approaches to Emerging Infectious Disease. EcoHealth 2005, 2, 258–272. [Google Scholar]
- Sallis, JF; Cervero, RB; Ascher, W; Henderson, KA; Kraft, MK; Kerr, J. An Ecological Approach to Creating Active Living Communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar]
- Botany Bay Studies Unit. UNSW: Sydney, Australia; Available online: http// www.bbsu.unsw.edu.au/(accessed March 15, 2009).
- Black, J.
- Horonjeff, R; McKelvey, F. Planning and Design of Airports, 4th Ed ed; McGraw Hill: New York, USA, 1999. [Google Scholar]
- Australia, Senate Select Committee. Falling on Deaf Ears, Report of the Senate Select Committee on Aircraft Noise in Sydney; Senate Select Committee: Canberra, Australia, 1995. [Google Scholar]
- Department of Transport and Regional Services. Discussion Paper, Expanding Ways to Describe and Assess Aircraft Noise; National Capital Printing: Canberra, Australia, 2002. [Google Scholar]
- Issarayangyun, T; Samuels, S; Black, J. The Noise Gap Index, A New Way to Describe and Assess Aircraft Noise Impacts on the Community. Proceedings of the 2004 Conference of the Australian Acoustical Society, Gold Coast, Queensland, Australia, November 3–5, 2004.
- Issarayangyun, T; Samuels, S; Black, J; Black, D. Aircraft Noise and Environmental Health, A Trans-disciplinary Approach. Proceedings of 28th Australasian Transport Research Forum Sydney, Sydney, Australia, September 28–30, 2005, (CD_ROM).
- Black, DA; Black, JA; Issarayangyun, T; Samuels, SE. Aircraft Noise Exposure and Resident’s Stress and Hypertension, A Public Health Perspective for Airport Environmental Management. J. Air Transp. Manag 2007, 13, 264–276. [Google Scholar]
- Black, DA; Black, JA; Issarayangyun, T; Samuels, SE. Public Health Responses to Aircraft Noise and its Mitigation. J. Air Transp. Manag 2007, 13, 264–276. [Google Scholar]
- Manocha, R; Marks, GB; Kenchington, P; Peters, D; Salome, CM. Sahaja Yoga in the Management of Moderate to Severe Asthma, A Randomised Controlled Trial. Thorax 2002, 57, 110–115. [Google Scholar]
- Black, DA; Black, JA. Public Health and the Sustainability of Cities, Sydney Airport’s Noise Pollution and Community Wellbeing. In Dialogues in Urban Planning, Towards Sustainable Regions; Gilmore, T, Blakely, E, Pizzaro, R, Eds.; Sydney University Press: Sydney, Australia, 2008; pp. 153–174. [Google Scholar]
- Black, J; Hayashi, Y. A Trans-disciplinary Framework, Challenges in Modelling the Sustainable City. Proceedings of the 9th International Conference on Computers in Urban Planning and Urban Management, June 29, to July 1, 2005; University College London: London, UK.
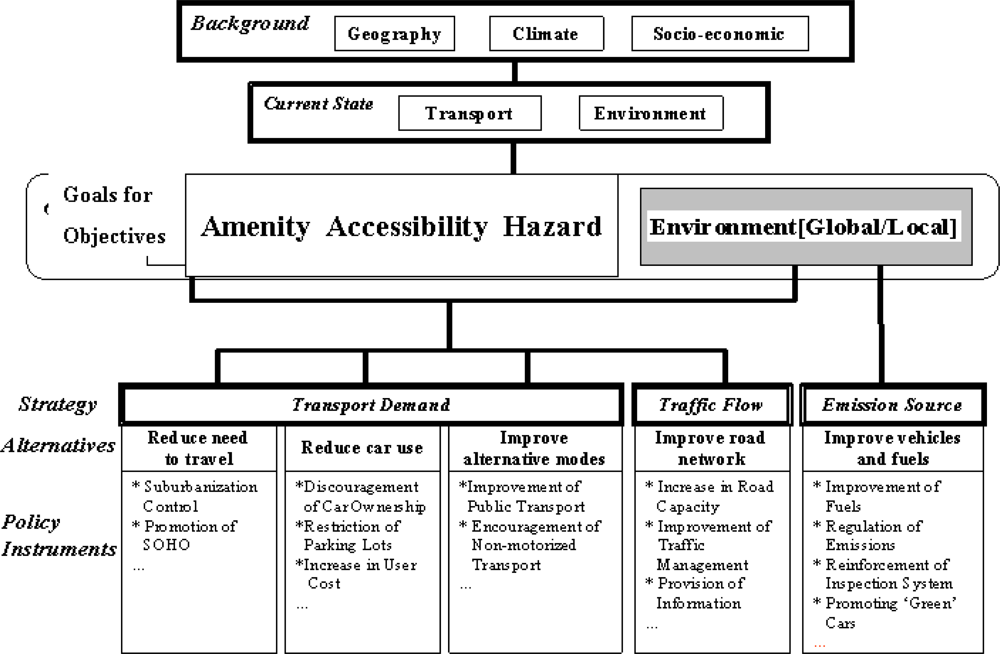
- Kachi, N; Kato, H; Hayashi, Y; Black, J. Making Cities More Compact by Improving Transport and Amenity and Reducing Hazard. J. East Asia Soc. Trans. Stud 2005, 6, 3819–3834. [Google Scholar]
- World Resources Institute. Climate Analysis Indicator Tools. Available online: http//cait.wri.org/figures.php (accessed March 18, 2009).
- Wilcox, B; Aguirre, AA; Daszak, P; Horwitz, P; Martens, P; Parkes, M; Patz, J; Waltner-Toews, D. A Transdisciplinary Imperative for a Sustainable Future. EcoHealth 2004, 1, 3–5. [Google Scholar]
- World Conference on Transport Research Society. World Conference on Transport Research Society.
- EcoHealth Journal. EcoHealth Journal. Available online: http// www.springerlink.com/content/1612-9202 (accessed March 15, 2009).
- Higginbotham, N; Connor, L; Albrecht, G; Freeman, S; Agho, K. Validation of an Environmental Distress Scale. EcoHealth 2006, 3, 245–254. [Google Scholar]
- Albrecht, G. ‘Solastalgia’ a New Concept in Health and Identity. PAN 2005, 3, 41–55. [Google Scholar]
- Greenaway, S; McCreanor, T; Witten, K. Reducing CO(2) Emissions from Domestic Travel, Exploring the Social and Health Impacts. EcoHealth 2009. [Google Scholar]
- Ali, R; Zhao, H. Wuhan, China and Pittsburgh, USA, Urban Environmental Health Past, Present, and Future. EcoHealth 2008, 5, 159–166. [Google Scholar]
- World Conference on Transport Research. 11th World Conference on Transport Research; University of California: Berkeley, California, USA; Available online: http,//www.uctc.net/wctrs/program/WCTR2007Catalogue.pdf (accessed 15 March, 2009).
- Hironori, K; Shiroyama, H; Nakagawa, Y; Fukayama, T. Trans-disciplinary Problem Structuring in Transport Planning. Proceedings of 11th World Conference on Transport Research Society Conference, University of California: Berkeley, CA, USA; June 24–28, 2007.
- Black, DA; Black, JA. Aircraft Noise and Public Health: A Research Design for Innovative Airport Environmental Management. Proceedings of 11th World Conference on Transport Research Society Conference, University of California: Berkeley, CA, USA; June 24–28, 2007.
- Dora, C. A different route to health, implications of transport policies. BMJ 1999, 318, 1686–1689. [Google Scholar]
- World Conference on Transport Research Society and Institute for Transport Policy Studies. Urban Transport and the Environment - An International Perspective; World Conference on Transport Research Society and Institute for Transport Policy Studies and Elsevier, Amsterdam, The Netherlands, 2004. [Google Scholar]
- O’Brien, KL; Leichenko, RM. Double Exposure, Assessing the Impacts of Climate Change within the Context of Economic Globalization. Global Environ Change 2000, 10, 221–232. [Google Scholar]
- Leichenko, RM; Karen, LOB. Double Exposure, Global Environmental Change in an Era of Globalization; Oxford Univ. Press: New York, USA, 2008. [Google Scholar]
- Patz, J. Launch of the International Association for Ecology and Health at Its First Biennial Conference, Message from the President Elect. EcoHealth 2007, 4, 6–9. [Google Scholar]
- McMichael, AJ. Population Health as the ‘Bottom Line’ of Sustainability, A Contemporary Challenge for Public Health Researchers. Eur. J. Public Health 2006, 16, 579–581. [Google Scholar]
- State of Environment Gateway; United Nations Environmental Program: Washington DC, USA; Available online: www.grida.no/soe/ (accessed March 8, 2009).
- Hood, E. Toward a New Understanding of Aging. Environ. Health Perspect 2003, 111, A756–759. [Google Scholar]
- Nicholls, RJ; Hanson, S; Herweijer, C; Patmore, N; Hallegatte, S; Corfee-Morlot, J; Chateau, J; Muir-Wood, R. Ranking of the World’s Cities most Exposed to Coastal Flooding Today and in the Future; Organisation for Economic Co-operation and Development (OECD): Paris, France, 2007. [Google Scholar]
- Nakanishi, H; Black, J; Doust, K. Sustainable Urban Planning and Urban Responses to Climate Change - A Review of Practices in the ACT, New South Wales and Victoria, Australia. Proceedings of “Social Challenges of Global Change” - IHDP 7th Open Meeting 2009, the 7th International Science Conference on the Human Dimensions of Global Environmental Change, Bonn, Germany, 26–30, April, 2009.
- Black, J; Doust, K; Nakanishi, H. Metrics of Environmental Sustainability, Social Equity and Economic Efficiency. Proceedings of “Social Challenges of Global Change” - IHDP 7th Open Meeting 2009, the 7th International Science Conference on the Human Dimensions of Global Environmental Change, Bonn, Germany, April 26–30, 2009.
- Blakely, E; Black, J. Transit-oriented Developments and Busways in Australia. Proceedings of 11th World Conference on Transport Research Society Conference, University of California: Berkeley, CA, USA; June 24–28, 2007, (CD-ROM).
- Patrick, DL; Erickson, P. Health Status and Health Policy, Quality of Life in Health Care Evaluation and Resource Allocation; Oxford University Press: New York, USA, 1993. [Google Scholar]
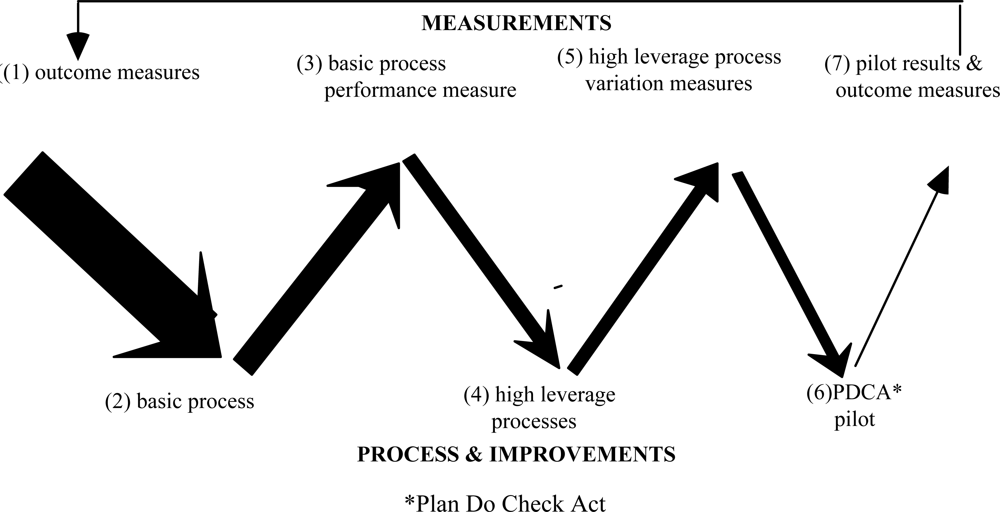
- Batalden, PB; Nelson, EC; Roberts, JS. Linking Outcomes Measurement to Continual Improvement, The Serial” V” Way of Thinking about Improving Clinical Care. Joint Comm. J. Qual. Improvement 1994, 20, 167. [Google Scholar]
- Corbett, J; Hagerstrand, T. Time Geography; Centre for Spatially Informed Social Science, University of California: Santa Barabara, CA, USA; Available online: http,//www.csiss.org/classics/content/29 (accessed March 10, 2009).
- Schærström, A. Epidemiological Landscapes–Health and Ill Health in Time and Space. Available online: http://www.keg.lu.se/ngm/html/papers/paper_schaerstrom3.pdf (accessed 20 January 2009).
- Black, J; Doust, K; Nakanishi, H. Metrics of Environmental Sustainability, Social Equity and Economic Efficiency. Proceedings of “Social Challenges of Global Change” - IHDP 7th Open Meeting 2009, In Proceedings of the 7th International Science Conference on the Human Dimensions of Global Environmental Change, Bonn, Germany, April 26–30, 2009.
- Jones, PM; Dix, MC. Understanding Travel Behaviour; Gower Publishing Company: Aldershot, Hants, UK, 1983. [Google Scholar]
- Hägerstrand, T. Survival and Arena, on the Life-history of Individuals in Relation to Their Geographical Environment. The Monadnock 1975, 49, 9–29. [Google Scholar]
- Schærström, A. Pathogenic Paths? A Time Geographical Approach in Medical Geography; Lund University Press: Lund, Sweden, 1996. [Google Scholar]
- Edwards, JD. Transportation Planning Handbook; Prentice Hall: Englewood Cliffs, NJ, USA, 1992. [Google Scholar]
- Ton, TT; Black, JA; Vandebona, U. An Object-Oriented Software Design for Transport Modeling: Software Development to Calculate Road Traffic Noise. Transportation 1998, 25, 307–328. [Google Scholar]
- Ton, TT; Black, JA. Geographical Information Systems and Land-use Transport Models: Towards Integration. Masters, EG, Pollard, JR, Eds.; University of New South Wales: Kensington, Australia, 1993; pp. 263–276. [Google Scholar]
- Black, J; Trinder, J; Ton, T; Masters, U; Tudge, R. A Spatial Decision Support System for Road-based Transport Planning. In World Transport Research - Proceedings of the 7th World Conference on Transport Research, Vol 3, Transport Policy, 1996; Hensher, D, King, J, Oum, T, Eds.; Elsevier: Amsterdam, The Netherlands, 1996; pp. 71–83. [Google Scholar]
- Alexander, C; Ishikawa, S; Silverstein, M; Jacobson, M; Fiksdahl-King, I; Angel, S. Center for Environmental Studies: A Pattern Language, Towns, Buildings, Construction; Oxford University Press: New York USA, 1977. [Google Scholar]
- Buchanan, CD. Ministry of Transport, Britain. In Traffic in Towns, The Specially Shortened Edition of the Buchanan Report; Penguin Books: Harmondsworth, Middlesex, UK, 1963. [Google Scholar]
- Rauh, V. A. Health and Community Design, the Impact of the Built Environment on Physical Activity. Environ. Health Perspect 2003, 111, 1348–1351. [Google Scholar]
- Meade, MS; Earickson, RJ. Medical Geography; The Guilford Press: New York, USA, 2005. [Google Scholar]
- Frumkin, H; Frank, L; Jackson, R. Urban Sprawl and Public Health: Designing, Planning and Building for Healthy Communities; Island Press: Washington, DC, USA, 2004. [Google Scholar]
- Jackson, L. E. The Relationship of Urban Design to Human Health and Condition. Landscape Urban Plan 2003, 64, 191–200. [Google Scholar]
- Galea, S; Vlahov, D. MyiLibrary Handbook of Urban Health Populations, Methods, and Practice; Springer-Verlag: Berlin, Germany, 2005. [Google Scholar]
- Galea, S; Vlahov, D. Urbanization. In Environmental Health, from Global to Local; Frumkin, H, Ed.; Jossey-Bass: San Francisco, CA, USA, 2005; pp. 387–413. [Google Scholar]
- Giles-Corti, B. The Impact of Urban Form on Public Health, Current or Emerging Issues Paper; Department of Resources, the Environment and Water; Australian Government: Canberra, Australia, 2006. [Google Scholar]
- Sugiyama, T. Environments for Active Lifestyles, Sustainable Environments May Enhance Human Health. Environ. Health Insights 2008, 2, 93–96. [Google Scholar]
- Cochrane, T; Davey, RC; Gidlow, C; Smith, GR; Fairburn, J; Armitage, CJ; Stephansen, H; Speight, S. Small Area and Individual Level Predictors of Physical Activity in Urban Communities, A Multi-Level Study in Stoke on Trent, England. Int. J. Environ. Res. Public Health 2009, 6, 654–677. [Google Scholar]
- US Department of Health and Human Services. Physical Activity and Health, A report of the Surgeon General; US Department of Health and Human Services: Washington DC, USA, 1999. [Google Scholar]
- Active Living by Design; Active Living Research: San Diego, CA, USA.
- Lovasi, GS; Moudon, AV; Pearson, AL; Hurvitz, PM; Larson, EB; Siscovick, DS; Berke, EM; Lumley, T; Psaty, BM. Using Neighborhood Built Environment Characteristics to Predict Walking for Exercise. Int. J. Health Geogr 2008, 7, 10. [Google Scholar]
- Brown, LD; Kraft, MK. Active Living as an Institutional Challenge, Lessons from the Robert Wood Johnson Foundation’s “Celebrate Fitness” Program. J. Health Politics, Pol. Law 2008, 33, 497–523. [Google Scholar]
- Active Living, the Built Environment, and the Policy Agenda. J Health Politics, Pol Law. 2008.
- Manifesto on Transport and Green Cities. Doctors for the Environment Australia: South Australia, 2007. Available online: http://www.dea.org.au/UserFiles/File/pdf_documents/GREEN_CITY_MANIFESTO_2.pdf (accessed 20 February, 2009).
- Benjamin, CG. Transportation Policy & Health, Building for a Healthy America Hidden Health Costs of Transportation Policy, Saving Lives and Dollars; American Public Health Association: Washington, DC, USA, 2009. [Google Scholar]
- Mitchell, RB; Rapkin, C. Urban Traffic, A Function of Land Use; Columbia University Press: New York, USA, 1954. [Google Scholar]
- Blunden, WR; Black, JA. The Land-use/Transport System, 2nd Ed ed; Pergamon Press: Sydney, Australia, 1984. [Google Scholar]
- Blunden, WR. Introduction to Traffic Science; Printerhall: London, England, 1967. [Google Scholar]
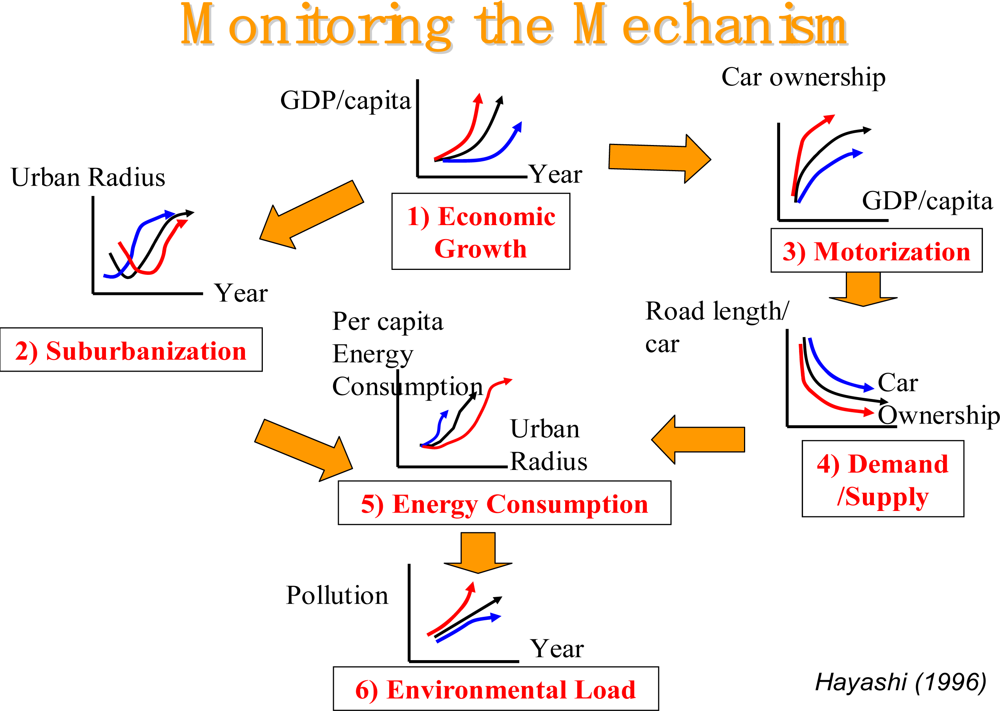
- Transport, Land-use and the Environment; Hayashi, Y; Roy, J (Eds.) Kluwer Academic Publishers: Dordrecht, The Netherlands, 1996.
- Ortúzar, J-dD; Willumsen, LG. Modeling Transport, 3rd Ed ed; John Wiley & Sons: Chichester, England, 2001. [Google Scholar]
- Newman, P; Kenworthy, J. Sustainability and Cities, Overcoming Automobile Dependence; Island Press: Washington, DC, USA, 1993. [Google Scholar]
- Journal of Accident Analysis & Prevention. Available online: http://www.elsevier.com/wps/find/journaldescription.cws_home/336/description#description (accessed March 9, 2009).
- Babisch, W; Beule, B; Schust, M; Kersten, N; Ising, H. Traffic Noise and Risk of Myocardial Infarction. Epidemiology 2005, 16, 33–40. [Google Scholar]
- Babisch, W. Traffic Noise and Cardiovascular Disease, Epidemiological Review and Synthesis. Noise Health 2000, 8, 9–32. [Google Scholar]
- Finegold, LS; Job, S; De Jong, R; Griefahn, B. The Effect of Noise on Public Health. The ASHA Leader 2004, 13, 6–7. [Google Scholar]
- Ising, H; Kruppa, B. Health Effects Caused by Noise, Evidence in the Literature from the Past 25 Years. Noise Health 2004, 6, 5–13. [Google Scholar]
- Netterstrom, B; Juel, K. Impact of Work-Related and Psychosocial Factors on the Development of Ischemic Heart Disease Among Urban Bus Drivers in Denmark. Scand. J. Work Environ. Health 1988, 14, 231–238. [Google Scholar]
- Robinson, AA. Cerebrovascular Disease, Ischaemic Heart Disease, and the Stress of Vehicle Travel. Med. Hypotheses 1989, 30, 101. [Google Scholar]
- Gee, GC; Takeuchi, DT. Traffic Stress, Vehicular Burden Aand Well-Being, A Multilevel Analysis. Soc. Sci. Med 2004, 59, 405–414. [Google Scholar]
- Southworth, M. Urban Forms and Metropolitan Spaces, Berkeley; It Università Degli Studi Di Roma Sapienza, Facoltà Di Ingegneria, April 2nd–3rd, 2007. Available Online: http,//www.Dau.Uniroma1.It/Futureofthecity/Forms_Spaces_Texts/@02Michael.Pdf (accessed January 15, 2009).
- Hede, AJ; Bullen, RB. Aircraft Noise in Australia, A Survey of Community Reaction; National Acoustics Laboratory, Australian Government Publishing Service: Canberra, Australia, 1982. [Google Scholar]
- Fidell, S; Barber, DS; Schultz, TJ. Updating a Dosage-Effect Relationship for the Prevalence of Annoyance Due to General Transportation Noise. J. Acoust. Soc. Amer 1991, 111, 1743–1750. [Google Scholar]
- Meister, EA; Donatelle, RJ. The Impact of Commercial Aircraft Noise on Human Health, A Neighborhood Study in Metropolitan Minnesota. J. Environ. Health 2000, 63, 9–15. [Google Scholar]
- Canada Health. Noise from Civilian Aircraft in the Vicinity of Airports, Implications for Human Health, I. Noise, Stress and Cardiovascular Disease; Ministry of Public Works and Government Services: Ottawa, Canada, 2001. [Google Scholar]
- Rosenlund, M; Berglind, N; Pershagen, G; Jarup, L; Bluhm, G. Increased Prevalence of Hypertension in a Population Exposed to Aircraft Noise. BMJ 2001, 58, 769–773. [Google Scholar]
- Jarup, L; Dudley, ML; Babisch, W; Houthuijs, D; Swart, W; Pershagen, G; Bluhm, G; Katsouyanni, K; Velonakis, M; Cadum, E. Hypertension and Exposure to Noise Near Airports (HYENA), Study Design and Noise Exposure Assessment. Environ. Health Perspect 2005, 113, 1473–1478. [Google Scholar]
- Chipperfield, M. Loud Enough For You? Sydney Morning Herald: Sydney, Australia, 2008. [Google Scholar]
- Australian Government. Ambient Air Quality Standards Setting, An Approach to Heath-Based Hazard Assessment; National Health and Medical Research Council and Environmental Health Committee (Enhealth): Canberra, Australia, 2006. [Google Scholar]
- Janssen, NAH; Lanki, T; Hoek, G; Vallius, M; De Hartog, JJ; van Grieken, R; Pekkanen, J; Brunekreef, B. Associations Between Ambient, Personal, and Indoor Exposure to Fine Particulate Matter Constituents in Dutch and Finnish Panels of Cardiovascular Patients. Occ. Environ. Med 2005, 62, 868–877. [Google Scholar]
- Mauderly, JL; Samet, JM. Is There Evidence for Synergy Among Air Pollutants in Causing Health Effects. Environ Health Perspect 2009, 117, 1–6. [Google Scholar]
- Transportation Emissions & Air Quality: Implications for Public Policy Metropolitan Area Planning Council Workshop Summary: Public Health Perspectives; MAPC: Boston, MA, USA, 2006. Available online: http://www.mapc.org/transportation/Air_Quality/Public_Health_Perspectives.pdf (accessed December 8, 2008).
- Fanning, EW; Froines, JR; Utell, MJ; Lippmann, M; Oberdörster, G; Frampton, M; Godleski, J; Larson, TV. Particulate Matter (PM) Research Centers (1999–2004) and the Role of Interdisciplinary Center-based Research, 2008. Environ Health Perspect. 2008. Available online: http://www.epa.gov/ncer/science/pm/2008sab/ehp_paper.pdf (accessed December 8, 2008).
- Breitner, S; Stölzel, M; Cyrys, J; Pitz, M; Wölke, G; Kreyling, W; Küchenhoff, H; Heinrich, J; Wichmann, H-E; Peters, AA. Short-Term Mortality Rates during a Decade of Improved Air Quality in Erfurt, Germany, 2008. Environ. Health Perspect 2009, 117, 448–454. [Google Scholar]
- Analitis, A; Katsouyanni, K; Dimakopoulou, K; Samoli, E; Nikoloulopoulos, AK; Petasakis, Y; Touloumi, G; Schwartz, J; Anderson, HR; Cambra, K. Short-Term Effects of Ambient Particles on Cardiovascular and Respiratory Mortality. Epidemiology 2006, 17, 230–233. [Google Scholar]
- Dominici, F; McDermott, A; Daniels, M; Zeger, SL; Samet, JM. Revised Analyses of the National Morbidity, Mortality, and Air Pollution Study, Mortality among Residents of 90 Cities. J. Toxicol. Environ. Health A 2005, 68, 1071–1092. [Google Scholar]
- Pope, CA; Young, B; Dockery, DW. Health Effects of Fine Particulate Air Pollution, Lines That Connect. J. Air Waste Manage. Assoc 2006, 56, 709–742. [Google Scholar]
- Samoli, E; Aga, E; Touloumi, G; Nisiotis, K; Forsberg, B; Lefranc, A; Pekkanen, J; Wojtyniak, B; Schindler, C; Niciu, E. Short-Term Effects of Nitrogen Dioxide on Mortality, An Analysis Within the APHEA Project. Eur. Resp. J 2006, 27, 1129–1139. [Google Scholar]
- Samoli, E; Analitis, A; Touloumi, G; Schwartz, J; Anderson, HR; Sunyer, J; Bisanti, L; Zmirou, D; Vonk, JM; Pekkanen, J. Estimating the Exposure–Response Relationships Between Particulate Matter and Mortality Within the APHEA Multicity Project. Environ. Health Perspect 2005, 115, 1578–1583. [Google Scholar]
- WHO Europe. Air Quality Guidelines, Global Update 2005 - Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- Lindgren, A; Stroh, E; Montnemery, P; Nihlen, U; Jakobsson, K; Axmon, A. Traffic-Related Air Pollution Associated with Prevalence of Asthma and COPD/Chronic Bronchitis, A Cross-Sectional Study in Southern Sweden. Int. J. Health Geog 2009, 8, 2–9. [Google Scholar]
- van Roosbroeck, S; Wichmann, J; Janssen, NAH; Hoek, G; van Wijnen, JH; Lebret, E; Brunekreef, B. Long-Term Personal Exposure to Traffic-Related Air Pollution Among School Children, A Validation Study. Sci. Total Environ 2006, 368, 565–573. [Google Scholar]
- Brauer, M; Hoek, G; Van Vliet, P; Meliefste, K; Fischer, P; Gehring, U; Heinrich, J; Cyrys, J; Bellander, T; Lewne, M. Estimating Long-Term Average Particulate Air Pollution Concentrations, Application of Traffic Indicators and Geographic Information Systems. Epidemiology 2003, 14, 228–239. [Google Scholar]
- Levy, JI; Bennett, DH; Melly, SJ; Spengler, JD. Influence of Traffic Patterns on Particulate Matter and Polycyclic Aromatic Hydrocarbon Concentrations in Roxbury, Massachusetts. J. Exposure Sci. Environ. Epi 2003, 13, 364–371. [Google Scholar]
- Rundell, KW; Caviston, R; Hollenbach, AM; Murphy, K. Vehicular Air Pollution, Playgrounds, and Youth Athletic Fields. Inhal. Toxicol 2006, 18, 541–547. [Google Scholar]
- Soliman, ASM; Palmer, GM; Jacko, RB. Development of an Empirical Model to Estimate Real-World Fine Particulate Matter Emission Factors, The Traffic Air Quality Model. J. Air Waste Manage. Assoc 2006, 56, 1540–1549. [Google Scholar]
- Berghmans, P; Bleux, N; Panis, LI; Mishra, VK; Torfs, R; Van Poppel, M. Exposure Assessment of a Cyclist to PM10 and Ultrafine Particles. Sci. Total Environ 2008, 407, 1268–1285. [Google Scholar]
- Bukowski, J. Do Pollution Time-Series Studies Contain Uncontrolled or Residual Confounding by Risk Factors for Acute Health Events? Regul. Toxicol. Pharmacol 2008, 51, 135–140. [Google Scholar]
- Hidas, P; Shiran, GR; Black, JA. An Air Quality Prediction Model Incorporating Traffic, Meteorological and Built Form Factors: The Assessment of Land Use and Transport Strategies in Sydney. Proceedings of 30th International Symposium on Automotive Technology and Automation, Florence, Italy, June 16–19, 1997.
- Government of Canada. Canadian Environmental Sustainability Indicators 2007 - Highlights. Available Online: http//www.Ec.Gc.Ca/Environmentandresources/CESIHL2007/CESIHL2007_E.Cfm (accessed December 8, 2008).
- de Medeiros, APP; Gouveia, N; Pérez Machado, RP; de Souza, MR; Alencar, GP; Novaes, HMD; de Almeida, MF. Traffic Related Air Pollution and Perinatal Mortality, A Case-Control Study. Environ. Health Perspect 2009, 117, 127–132. [Google Scholar]
- Wong, CM; Yang, L; Thach, TQ; Chau, PYK; Chan, KP; Thomas, GN; Lam, TH; Wong, TW; Hedley, AJ; Malik Peiris, JS. Modification by Influenza on Health Effects of Air Pollution in Hong Kong. Environ. Health Perspect 2009, 117, 248–253. [Google Scholar]
- Liu, L; Poon, R; Chen, L; Frescura, A-M; Montuschi, P; Ciabattoni, G; Wheeler, A; Dales, R. Acute Effects of Air Pollution on Pulmonary Function, Airway Inflammation and Oxidative Stress in Asthmatic Children. Environ. Health Perspect 2009, 117, 668–674. [Google Scholar]
- Zeka, A; Zanobetti, A; Schwartz, J. Individual-Level Modifiers of the Effects of Particulate Matter on Daily Mortality. Amer. J. Epidemiol 2006, 163, 849–859. [Google Scholar]
- Parker, JD; Akinbami, LJ; Woodruff, TJ. Air Pollution and Childhood Respiratory Allergies in the United States. Environ. Health Perspect 2009, 117, 140–147. [Google Scholar]
- Costa, G; Pickup, L; Di Martino, V. Commuting - A Further Stress Factor for Working People, Evidence from the European Community. Int. Arch. Occupat. Environ. Health 1988, 60, 371–376. [Google Scholar]
- Whitelegg, J. A Report for Transport & General Workers Union; Eco-Logica Ltd: White Cross, Lancaster, England, 1995. [Google Scholar]
- de Croon, EM; Blonk, RWB; de Zwart, BCH; Frings-Dresen, MHW; Broersen, JPJ. Job Stress, Fatigue, and Job Dissatisfaction in Dutch Lorry Drivers, Towards an Occupation Specific Model of Job Demands and Control. Occupat. Environ. Med 2002, 59, 356–361. [Google Scholar]
- Haworth, N; Heffernan, C; Horne, E. Fatigue in Truck Accidents; Monash University Accident Research Centre. Monash University: Clayton, Victoria, Australia, 1989. [Google Scholar]
- Truck Driver Safety and Health; National Institute for Occupational Health and Safety: Atlanta, GA, USA; Available online: http,//wwwcdcgov/niosh/blog/nsb111907_truck.html (accessed March 11, 2009).
- Gardiner, A; Motorists Spend a Day a Year Behind the Wheel. Herald Sun; Fairfax: Melbourne, Victoria, Australia, 2008. Available online: http://www.news.com.au/heraldsun/story/0,21985,24753344-2862,00.html (accessed 10 December, 2008).
- Besser, L. If Motorways are the Answer, We’ve Been Asking the Wrong Question. Sydney Morning Herald; Fairfax: Sydney, Australia, 2008. Available online: http://www.smh.com.au/news/national/if-motorways-are-the-answer-weve-been-asking-the-wrong-question/2008/12/09/1228584840247.html (accessed December 11, 2008).
- Besser, LM; Marcus, M; Frumkin, H. Commute Time and Social Capital in the U.S. Am. J. Prev. Med 2008, 34, 207–211. [Google Scholar]
- Department of the Environment Water Heritage and the Arts. State of the Environment 2008; Available online: http,//www.environment.gov.au/soe/ (accessed December 10, 2008).
- Morrison, DS; Petticrew, M; Thomson, H. What Are The Most Effective Ways of Improving Population Health Through Transport Interventions? Evidence from Systematic Reviews. J. Epidemiol. Community Health 2003, 57, 327–333. [Google Scholar]
- Cromley, EK; McLafferty, SL. GIS & Public Health; Guilford Press: New York, USA, 2002. [Google Scholar]
- Lu, X. A Framework of Web GIS Based Unified Public Health Information Visualization Platform Computational Science and Its Applications, Volume 3482/2005; Springer: Berlin, Germany, 2005. [Google Scholar]
- Zhan, FB; Brender, JD; Han, Y; Suarez, L; Langlois, PH. GIS-EpiLink, A Spatial Search Tool for Linking Environmental and Health Data. J. Med. Syst 2006, 30, 405–412. [Google Scholar]
- Grigg, M; Alfred, B; Keller, C; Steele, JA. Implementation of an Internet-based Geographic Information System, The Florida Experience. J. Public Health Manage. Pract 2006, 12, 139. [Google Scholar]
- Johnson, R. GIS Technology for Disasters and Emergency Management - An ESRI White Paper May 2000; ESRI: Redlands, California, USA; Available online: http//www.esri.com/library/whitepapers/pdfs/disastermgmt.pdf (accessed March 11, 2009).
- Role of Internet-based GIS in Effective Natural Disaster Management; GIS Development: Noida, India; Available online: http,//www.gisdevelopment.net/technology/gis/techgi0030a.htm (accessed March 11, 2009).
- Yoshitomi, P. The Role of GIS in the Response to the Terrorist Attacks of September 11 in New York City. Kyoto Daigaku Bōsai Kenkyūjo nenpō 2004, 4, 325–329. [Google Scholar]
- Cutchin, MP. The Need for the “New Health Geography” in Epidemiologic Studies of Environment and Health. Health Place 2007, 13, 725–742. [Google Scholar]
- Mazumdar, S; Rushton, G; Smith, BJ; Zimmerman, DL; Donham, KJ. Geocoding Accuracy and the Recovery of Relationships Between Environmental Exposures and Health. Int. J. Health Geog 2008, 7, 13–17. [Google Scholar]
- de Lone, WH; McLean, ER. Information Systems Success, The Quest for the Dependent Variable. Inf. Systems Res 1992, 3, 60–95. [Google Scholar]
- Lofthouse, GE. Megacity Challenges, A Stakeholder Perspective, A Research Project Conducted by GlobeScan and MRC McLean Hazel Sponsored by Siemens; Siemens A.G. Corporate Communications: Munich, Germany.
- Doyon, B; Belanger, D; Gosselin, P. The Potential Impact of Climate Change on Annual and Seasonal Mortality for Three Cities in Quebec, Canada. Int. J. Health Geog 2008, 7, 23. [Google Scholar]
- McMichael, AJ; Woodruff, RE; Hales, S. Climate change and human health, present and future risks. Lancet 2006, 367, 859–869. [Google Scholar]
- Haines, A; Patz, JA. Health Effects of Climate Change. JAMA 2004, 291, 99–103. [Google Scholar]
- Haines, A; McMichael, AJ; Epstein, PR. Environment and Health, 2. Global Climate Change and Health. Can. Med. Assoc. J 2000, 163, 729–734. [Google Scholar]
- Human Health and Climate Change, National Adaptation Research Plan - Human Health, NARP, Final, 2 December 2008; National Climate Change Adaptation Research Facility Australia: Southport, Australia.
- Meehl, GA; Washington, WM; Collins, WD; Arblaster, JM; Hu, A; Buja, LE; Strand, WG; Teng, H. How Much More Global Warming and Sea Level Rise? Science 2005, 307, 1769–1772. [Google Scholar]
- Luber, G; McGeehin, M. Climate Change and Extreme Heat Events. Am. J. Prev. Med 2008, 35, 429–435. [Google Scholar]
- Kinney, PL; O’Neill, MS; Bell, ML; Schwartz, J. Approaches for estimating effects of climate change on heat-related deaths, challenges and opportunities. Environ. Sci. Policy 2008, 11, 87–96. [Google Scholar]
- Medina-Ramon, M; Zanobetti, A; Cavanagh, DP; Schwartz, J. Extreme Temperatures and Mortality, Effect, Modification, and Acclimatization in a Continental Study. Environ. Health Perspect 2006, 114, S161–S161. [Google Scholar]
- Mastrangelo, G; Hajat, S; Fadda, E; Buja, A; Fedeli, U; Spolaore, P. Contrasting Patterns of Hospital Admissions and Mortality During Heat Waves, Are Deaths from Circulatory Disease a Real Excess or an Artifact? Med. Hypotheses 2006, 66, 1025–1028. [Google Scholar]
- Knowlton, K; Rotkin-Ellman, M; King, GM; Margolis, HG; Smith, D; Solomon, G; English, P. The 2006 California Heat Wave, Impacts on Hospitalizations and Emergency Department Visits. Environ. Health Perspect 2009, 117, 61–67. [Google Scholar]
- Diffey, B. Climate Change, Ozone Depletion and the Impact on Ultraviolet Exposure of Human Skin. Phys. Med. Biol 2004, 49, R1–R11. [Google Scholar]
- Beggs, PJ; Bambrick, HJ. Is the Global Rise of Asthma an Early Impact of Anthropogenic Climate Change? Department of Physical Geography, Macquarie University and National Centre for Epidemiology and Population Health: Canberra, Australia, 2005. [Google Scholar]
- Ziska, LH; Epstein, PR; Schlesinger, WH. Rising CO2, Climate Change and Public Health, Exploring the Links to Plant Biology. Environ. Health Perspect 2009, 117, 155–158. [Google Scholar]
- The 2009 Bushfires and Heatwaves in South-Eastern Australia; National Climate Change Adaptation Research Facility: Southport, Australia. Available online: http://www.nccarf.edu.au/national-adaptation-research-plans?q=node/60 (accessed March 18, 2009).
- Bushfire tragedy ‘one of Australia’s darkest days’. The Age; Fairfax: Melbourne, Victoria, Australia, 2009.
- National Adaption Research Plan; National Climate Change Adaptation Research Facility Australia: Southport, Australia; Available online: http,//www.nccarf.edu.au/national-adaptation-research-plans (accessed March 10, 2009).
- Leslie, E; Coffee, N; Frank, L; Owen, N; Bauman, A; Hugo, G. Walkability of Local Communities, Using Geographic Information Systems to Objectively Assess Relevant Environmental Attributes. Health Place 2007, 13, 111–122. [Google Scholar]
- Trevena, LJ; Sainsbury, P; Henderson-Smart, C; Clarke, R; Rubin, G; Cumming, R. Population Health Integration Within a Medical Curriculum - An Eight-part Toolkit. Am. J. Prev. Med 2005, 29, 234–239. [Google Scholar]
- Centre for Built Environment and Health; University of Western Australia, Centre for Built Environment and Health: Crawley, Australia. Available online: http://www.sph.uwa.edu.au/go/C_BEH (accessed March 18, 2009).
- McKinnon, RA; Reedy, J; Handy, SL; Brown Rodgers, AA. Measurement of the Food and Physical Activity Environments - Enhancing Research Relevant to Policy on Diet, Physical Activity, and Weight. Am. J. Prev. Med 2009, 4, S81–S190. [Google Scholar]
- Brownson, RC; Hoehner, CM; Day, K; Forsyth, A; Sallis, JF. Measuring the Built Environment for Physical Activity, State of the Science. Am. J. Prev. Med 2009, 36, S99–S123. [Google Scholar]
- Story, M; Giles-Corti, B; Lazarus, A; Yaroch, L; Cummins, S; Frank, LD; Huang, T-K; Blair, L. Work Group IV, Future Directions for Measures of the Food and Physical Activity Environments. Am. J. Prev. Med 2009, 36, S182–S188. [Google Scholar]
- The Australian National University National Centre for Epidemiology and Population Health. Available online: http://nceph.anu.edu.au/ (accessed March 18, 2009).
- Baume, P; Irvine, S. The Concept of Health. In Public Health, an Introduction; Baume, P, Bauman, A, Eds.; Eriador Press: Sydney, Australia, 1995; pp. 8–17. [Google Scholar]
- Bauman, A. Working across Sectors. In Public Health, An Introduction; Baume, P, Bauman, A, Eds.; Eriador Press: Sydney, Australia, 1995; pp. 54–57. [Google Scholar]
- Frith, J. Environmental Health. In Public Health, an Introduction; Baume, P, Bauman, A, Eds.; Eriador Press: Sydney, Australia, 1995; pp. 104–128. [Google Scholar]
- Black, J. Public Inconvenience, Access and Travel in Seven Sydney Suburbs; Urban Research Unit Research School of Social Sciences, The Australian National University: Canberra, Australia, 1977. [Google Scholar]
- May, T. DISTILLATE, an Introduction - Final Workshop of the DISTILLATE Programme; Distillate: London, UK, 2008; Available online: http,//www.distillate.ac.uk/news/Introduction%20(Tony%20May.ppt (accessed March 18, 2009).
- Human Settlement; Department of Environment and Climate Change: Sydney, Australia; Available online: www.environment.nsw.gov.au/soe/soe2006/chapter2/chp_2.4.htm (accessed December 10, 2008).
- Capon, AG; Blakely, EJ. Checklist for Healthy and Sustainable Communities. N. S. W. Public Health Bull 2007, 18, 51–54. [Google Scholar]
- Buzbee, WW. Urban Form, Health, and the Law’s Limits. Amer. J. Public Health 2003, 93, 1395–1399. [Google Scholar]
- Kearns, A; Beaty, M; Barnett, G. A Social-Ecological Perspective on Health in Urban Environments. N. S. W. Public Health Bull 2007, 18, 48–50. [Google Scholar]
- Integrated Assessment of Health Risks of Environmental Stressors in Europe. Overall Aims. Available online: http://www.intarese.org/about-us/overall-aims.htm (accessed March 18, 2009).
- Collins, A; Greaves, SP. Daytime Population Tracking for Planning and Pollution Exposure Assessment. Proceedings of the 2006 Australian Transport Research Forum, Gold Coast, Australia, 2006; (CD-ROM). [Google Scholar]
- Greaves, SP. Capturing the Spatiotemporal Variability of Fine Particulates in Travel Microenvironments. In Urban Transport XII; Brebbia, CA, Dolezel, V, Eds.; Wessex Institute of Technology Press: Southampton, England, 2006; pp. 849–858. [Google Scholar]
- Issarayangyun, T; Greaves, SP. Analysis of Minute-by-Minute Pollution Exposure inside a Car - a Time-Series Modelling Approach. Transp. Res. D - Transp. Environ 2007, 12, 347–357. [Google Scholar]
- Greaves, SP; Issarayangyun, T; Liu, WQ. Exploring Variability in Pedestrian Exposure to Fine Particulates (PM2.5) Along a Busy Road. Atmos. Environ 2008, 42, 1665–1676. [Google Scholar]
- Wilson, A. Generalised Representation for a Comprehensive Urban and Regional Model. Comput. Environ. Urban Syst 2007, 31, 148–161. [Google Scholar]
- The Melbourne Institute. The Household, Income and Labour Dynamics in Australia (HILDA) Survey; The Melbourne Institute: Melbourne, Australia; Available online: http,//www.melbourneinstitute.com/hilda/ (accessed March 18, 2009).




{kind=link}
{kind=link}
{kind=link}
| CONCEPTS AND DOMAINS | DEFINITIONS / INDICATORS |
|---|---|
| OPPORTUNITY | |
| Social or cultural disadvantage
Resilience |
|
| HEALTH PERCEPTIONS | |
| General health perceptions
Satisfaction with health |
|
| FUNCTIONAL STATUS | |
| Social Function | |
| Limitations in usual roles
Integration Contact Intimacy and sexual function |
|
| Psychological Function Affective Cognitive |
|
| Physical Function Activity restrictions Fitness |
|
| IMPAIRMENT | |
| Symptoms/subjective complaints
Signs Self-reported disease Physiological measures Tissue alterations Diagnoses |
|
| DEATH AND DURATION OF LIFE |
|
| Mechanism | Health Impact | Management/Mitigation/Adaptation |
|---|---|---|
| Economic Growth |
|
|
| Suburbanization |
|
|
| Motorization |
|
|
| Road Congestion |
|
|
| Energy Consumption |
|
|
| Environmental Load |
|
|
| Interaction | Geographical Scale | Main Exposed Group |
|---|---|---|
| Road and rail noise – sleep disturbance, annoyance, stress | Localized - noise attenuates with increasing distance | All groups in population, but greater impact on low – medium socio-economic status |
| Cyclists and ultra fine particulate matter inhalation | Localized – on road | Cyclists especially in morning peak |
| Aircraft noise - sleep disturbance, annoyance, stress | Area surrounding airport within 15–20 NEF | All groups with greater impact on low socio-economic status |
| Leaded petrol and child development | Localized to houses playgrounds on main roads, but note residual lead from paint within houses and gardens | Young children |
| Low density suburbs and stress | Suburban | Lower socio-economic status and those without access to automobile and reliable public transport |
| Car dependency and obesity | Urban, especially suburban | Adults and children |
| Transport emissions and air quality | Metropolitan air-shed | All groups, with dispersal modified by local meteorological conditions |
| Freeways and vehicle emissions and respiratory problems | within 500m – 1000m | All groups, especially young and elderly, and sub-groups |
| Diesel trucks, particulate matter and health | Near sea-ports, along major roads and truck routes | All groups but with a distinct socio-economic dimension |
| Accessibility and quality of life | Local neighborhood with emphasis on street design & pedestrian environments | All groups |
| Footpath design and standards pedestrian injuries | Localized around home to neighborhood activities | All groups but especially young and elderly |
| Poor dwelling design and layout and accidents in home | Household | Young children and elderly |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Black, D.; Black, J. A Review of the Urban Development and Transport Impacts on Public Health with Particular Reference to Australia: Trans-Disciplinary Research Teams and Some Research Gaps. Int. J. Environ. Res. Public Health 2009, 6, 1557-1596. https://doi.org/10.3390/ijerph6051557
Black D, Black J. A Review of the Urban Development and Transport Impacts on Public Health with Particular Reference to Australia: Trans-Disciplinary Research Teams and Some Research Gaps. International Journal of Environmental Research and Public Health. 2009; 6(5):1557-1596. https://doi.org/10.3390/ijerph6051557
Chicago/Turabian StyleBlack, Deborah, and John Black. 2009. "A Review of the Urban Development and Transport Impacts on Public Health with Particular Reference to Australia: Trans-Disciplinary Research Teams and Some Research Gaps" International Journal of Environmental Research and Public Health 6, no. 5: 1557-1596. https://doi.org/10.3390/ijerph6051557
APA StyleBlack, D., & Black, J. (2009). A Review of the Urban Development and Transport Impacts on Public Health with Particular Reference to Australia: Trans-Disciplinary Research Teams and Some Research Gaps. International Journal of Environmental Research and Public Health, 6(5), 1557-1596. https://doi.org/10.3390/ijerph6051557