A Novel Methodology to Evaluate Health Impacts Caused by VOC Exposures Using Real-Time VOC and Holter Monitors

Abstract
:1. Introduction
2. Method
2.1. Study Design
2.2. Subjects
2.3. HRV Analysis
2.4. TVOC Monitoring
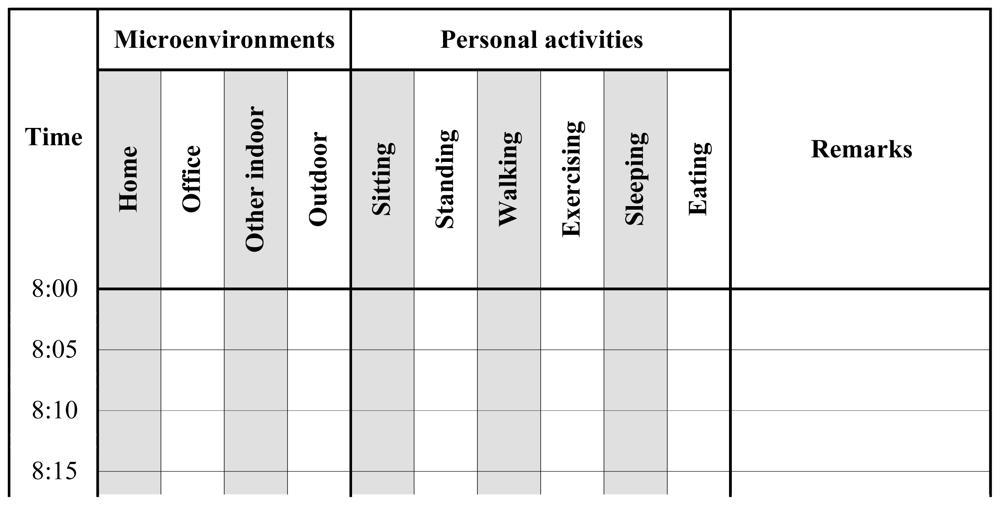
2.5. Time-Activity Pattern
3. Results and Discussion
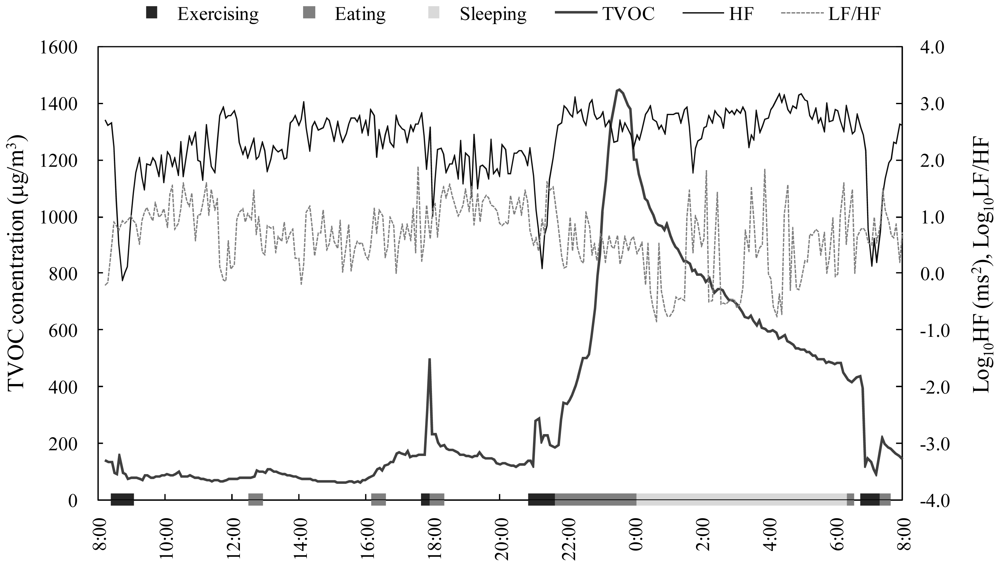
3.1. Time Series Data
3.2. Statistical Summary
3.3. Bivariate Analysis
4. Conclusions
Acknowledgements
References and Notes
- Jones, AP. Indoor air quality and health. Atmos. Environ 1999, 33, 4435–4564. [Google Scholar]
- Cooke, TF. Indoor air pollutants: A literature reviews. Rev. Environ. Health 1991, 9, 137–160. [Google Scholar]
- Becher, R; Hongslo, JK; Jantunen, MJ; Dybing, E. Environmental chemicals relevant for respiratory hypersensitivity: The indoor environment. Toxicol. Lett 1996, 86, 155–162. [Google Scholar]
- Kostiainen, R. Volatile organic-compounds in the indoor air of normal and sick houses. Atmos. Environ 1995, 29, 693–702. [Google Scholar]
- Ten Brinke, J; Selvin, S; Hodgson, AT; Fisk, WJ; Mendell, MJ; Koshland, CP; Daisey, JM. Development of new volatile organic compound (VOC) exposure metrics and their relationship to “sick building syndrome” symptoms. Indoor Air 1998, 8, 140–152. [Google Scholar]
- Kjaergaard, SK; Mølhave, L; Pedersen, OF. Human reactions to a mixture of indoor air volatile organic-compounds. Atmos. Environ 1991, 25A, 1417–1426. [Google Scholar]
- Shinohara, N; Mizukoshi, A; Yanagisawa, Y. Identification of responsible volatile chemicals that induce hypersensitive reactions to multiple chemical sensitivity patients. J. Expo. Anal. Environ. Epidemiol 2004, 14, 84–91. [Google Scholar]
- Edwards, RD; Jurvelin, J; Koistinen, K; Saarela, K; Jantunen, M. VOC source identification from personal and residential indoor, outdoor and workplace microenvironment samples in EXPOLIS-Helsinki, Finland. Atmos. Environ 2001, 35, 4829–4841. [Google Scholar]
- Saarela, K; Tirkkonen, T; Laine-Ylijoki, J; Jurvelin, J; Nieuwenhuijsen, MJ; Jantunen, M. Exposure of population and microenvironmental distributions of volatile organic compound concentrations in the EXPOLIS study. Atmos. Environ 2003, 37, 5563–5575. [Google Scholar]
- Smith, D; Spanel, P. Selected ion flow tube mass spectrometry (SIFT-MS) for on-line trace gas analysis. Mass Spectrom. Rev 2005, 24, 661–700. [Google Scholar]
- Amann, A; Spanel, P; Smith, D. Breath analysis: The approach towards clinical applications. Mini Rev. Med. Chem 2007, 7, 115–129. [Google Scholar]
- King, J; Kupferthaler, A; Unterkofler, K; Koc, H; Teschl, S; Teschl, G; Miekisch, W; Schubert, J; Hinterhuber, H; Amann, A. Isoprene and acetone concentration profiles during exercise on an ergometer. J. Breath Res 2009, 3, 027006. [Google Scholar]
- King, J; Mochalski, P; Kupferthaler, A; Unterkofler, K; Koc, H; Filipiak, W; Teschl, S; Hinterhuber, H; Amann, A. Dynamic profiles of volatile organic compounds in exhaled breath as determined by a coupled PTR-MS/GC-MS study. Physiol. Meas 2010, 31, 1169–1184. [Google Scholar]
- Coy, JD; Bigelow, PL; Buchan, RM; Tessari, JD; Parnell, JO. Field evaluation of a portable photoionization detector for assessing exposure to solvent mixtures. Am. Ind. Hyg. Assoc. J 2000, 61, 268–274. [Google Scholar]
- Peng, FM; Xie, PH; Shi, YG; Wang, JD; Liu, WQ; Liu, HY. Photoionization detector for portable rapid GC. Chromatographia 2007, 65, 331–336. [Google Scholar]
- RAE Systems, Application & Technical Notes, 3rd ed; RAE Systems: San Jose, CA, USA, 2005.
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart. J 1996, 17, 534–381.
- Malliani, A; Lombardi, F; Pagani, M. Power spectral analysis of heart rate variability: a tool to explore neural regulatory mechanisms. Br. Heart J 1994, 71, 1–2. [Google Scholar]
- Oka, T; Matsukura, M; Okamoto, M; Harada, N; Kitano, T; Miike, T; Futatsuka, M. Autonomic nervous functions in fetal type Minamata disease patients: Assessment of heart rate variability. Tohoku J. Exp. Med 2002, 198, 215–221. [Google Scholar]
- Steinhauer, SR; Morrow, LA; Condray, R; Scott, AJ. Respiratory sinus arrhythmia in persons with organic solvent exposure: Comparisons with anxiety patients and controls. Arch. Environ. Health 2001, 56, 175–180. [Google Scholar]
- Kazuma, N; Otsuka, K; Matsuoka, I; Murata, M. Heart rate variability during 24 hours in asthmatic children. Chronobiol. Int 1997, 14, 597–606. [Google Scholar]
- Yoshiuchi, K; Quigley, KS; Ohashi, K; Yamamoto, Y; Natelson, BH. Use of time-frequency analysis to investigate temporal patterns of cardiac autonomic response during head-up tilt in chronic fatigue syndrome. Auton. Neurosci 2004, 113, 55–62. [Google Scholar]
- Liao, DP; Creason, J; Shy, C; Williams, R; Watts, R; Zweidinger, R. Daily variation of particulate air pollution and poor cardiac autonomic control in the elderly. Environ. Health Perspect 1999, 107, 521–525. [Google Scholar]
- Chan, CC; Chuang, KJ; Shiao, GM; Lin, LY. Personal exposure to submicrometer particles and heart rate variability in human subjects. Environ. Health Perspect 2004, 112, 1063–1067. [Google Scholar]
- Chuang, KJ; Chan, CC; Chen, NT; Su, TC; Lin, LY. Effects of particle size fractions on reducing heart rate variability in cardiac and hypertensive patients. Environ. Health Perspect 2005, 113, 1693–1697. [Google Scholar]
- Riojas-Rodriguez, H; Escamilla-Cejudo, JA; Gonzalez-Hermosillo, JA; Tellez-Rojo, MM; Vallejo, M; Santos-Burgoa, C; Rojas-Bracho, L. Personal PM2.5 and CO exposures and heart rate variability in subjects with known ischemic heart disease in Mexico City. J. Expo. Sci. Environ. Epidemiol 2006, 16, 131–137. [Google Scholar]
- Power, KL; Balmes, J; Solomon, C. Controlled exposure to combined particles and ozone decreases heart rate variability. J. Occup. Environ. Med 2008, 50, 1253–1260. [Google Scholar]
- Wu, SW; Deng, FR; Niu, J; Huang, QS; Liu, YC; Gu, XB. Association of Heart Rate Variability in Taxi Drivers with Marked Changes in Particulate Air Pollution in Beijing in 2008. Environ. Health Perspect 2010, 118, 87–91. [Google Scholar]
- Pope, CA; Eatough, DJ; Gold, DR; Pang, YB; Nielsen, KR; Nath, P; Verrier, RL; Kanner, RE. Acute exposure to environmental tobacco smoke and heart rate variability. Environ. Health Perspect 2001, 109, 711–716. [Google Scholar]
- Sandstrom, M; Lyskov, E; Hornsten, R; Mild, KH; Wiklund, U; Rask, P; Klucharev, V; Stenberg, B; Bjerle, P. Holter ECG monitoring in patients with perceived electrical hypersensitivity. Int. J. Psychophysiol 2003, 49, 227–235. [Google Scholar]
- Belova, NY; Mihaylov, SV; Piryova, BG. Wavelet transform: A better approach for the evaluation of instantaneous changes in heart rate variability. Auton. Neurosci 2007, 131, 107–122. [Google Scholar]
- Casadei, B; Cochrane, S; Johnston, J; Conway, J; Sleight, P. Pitfalls in the interpretation of spectral-analysis of the heart-rate-variability during exercise in humans. Acta Physiol. Scand 1995, 153, 125–131. [Google Scholar]
- Lu, CL; Zou, XP; Orr, WC; Chen, JDZ. Postprandial changes of sympathovagal balance measured by heart rate variability. Dig. Dis. Sci 1999, 44, 857–861. [Google Scholar]
- Baharav, A; Kotagal, S; Gibbons, V; Rubin, BK; Pratt, G; Karin, J; Akselrod, S. Fluctuations in autonomic nervous activity during sleep displayed by power spectrum analysis of heart-rate-variability. Neurology 1995, 45, 1183–1187. [Google Scholar]
- Buszewski, B; Kesy, M; Ligor, T; Amann, A. Human exhaled air analytics: Biomarkers of diseases. Biomed. Chromatogr 2007, 21, 553–566. [Google Scholar]
- Ligor, T; Ligor, M; Amann, A; Ager, C; Bachler, M; Dzien, A; Buszewski, B. The analysis of healthy volunteers’ exhaled breath by the use of solid-phase microextraction and GC-MS. J. Breath Res 2008, 2, 046006. [Google Scholar]
- Ligor, M; Ligor, T; Bajtarevic, A; Ager, C; Pienz, M; Klieber, M; Denz, H; Fiegl, M; Hilbe, W; Weiss, W; Lukas, P; Jamnig, H; Hackl, M; Buszewski, B; Miekisch, W; Schubert, J; Amann, A. Determination of volatile organic compounds in exhaled breath of patients with lung cancer using solid phase microextraction and gas chromatography mass spectrometry. Clin. Chem. Lab. Med 2009, 47, 550–560. [Google Scholar]



{kind=link}
{kind=link}
| n a | Mean ± SD b | CV (%) c | |
|---|---|---|---|
| TVOC exposure concentration (μg/m3) | |||
| Total | 7 | 176 ± 130 | 74 |
| Home | 7 | 299 ± 267 | 89 |
| Office | 6 | 99 ± 21 | 21 |
| Other indoor | 5 | 197 ± 118 | 60 |
| Outdoor | 6 | 154 ± 72 | 47 |
| HRV | |||
| HF (msec2) | 7 | 104.2 ± 89.0 | 85 |
| LF/HF | 7 | 15.3 ± 19.0 | 124 |
| Subjects | −c | +d | |||||||
|---|---|---|---|---|---|---|---|---|---|
| a | b | c | d | e | f | g | |||
| Sex (M: male, F: female) | M | M | F | M | F | M | F | ||
| Age (years) | 24 | 22 | 22 | 23 | 48 | 33 | 54 | ||
| TVOC vs HF | −0.41**a | −0.04 | −0.00 | 0.02 | −0.15 | −0.01 | −0.08 | 6(1) | 1(0) |
| ΔTVOC vs HF | −0.27** | −0.63** | −0.26** | −0.08 | −0.19*b | −0.32** | −0.26 ** | 7(6) | 0(0) |
| d+TVOC vs HF | −0.11 | −0.53** | −0.15 | −0.06 | −0.04 | −0.12 | −0.43 ** | 7(2) | 0(0) |
| d−TVOC vs HF | 0.41** | 0.66** | 0.18 | 0.16 | 0.29* | 0.23 | 0.33 ** | 0(0) | 7(4) |
| TVOC vs LF/HF | 0.37** | 0.05 | −0.16* | 0.15 | 0.10 | 0.01 | −0.17 * | 2(2) | 5(1) |
| ΔTVOC vs LF/HF | 0.20*b | 0.39** | 0.07 | 0.18* | 0.18* | −0.27** | 0.36 ** | 1(1) | 6(5) |
| d+TVOC vs LF/HF | 0.15 | 0.28* | −0.00 | 0.24* | 0.14 | −0.18 | 0.46 ** | 2(0) | 5(3) |
| d−TVOC vs LF/HF | −0.30* | −0.46** | 0.01 | −0.18 | −0.07 | 0.13 | −0.45 ** | 5(3) | 2(0) |
| Temperature vs HF | 0.64** | −0.14 | −0.15 | 0.07 | −0.20 | 0.10 | 0.14 | 3(0) | 4(1) |
| RH vs HF | −0.51** | 0.11 | −0.08 | −0.00 | 0.29 | −0.00 | 0.10 | 4(1) | 3(0) |
| Temperature vs LF/HF | −0.44** | 0.14 | 0.17* | −0.05 | −0.00 | 0.30** | −0.25 ** | 4(2) | 3(2) |
| RH vs LF/HF | 0.31** | −0.07 | −0.01 | 0.07 | 0.00 | −0.21** | −0.35 ** | 4(2) | 3(1) |
| Home (n = 7) | Office (n = 6) | Other indoor (n = 5) | Outdoor (n = 4) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Range | Median | − a | + b | Range | Median | − | + | Range | Median | − | + | Range | Median | − | + | |
| TVOC vs HF | 0.98 | 0.22 | 0 | 1 | 0.85 | −0.28 | 4 | 0 | 1.11 | 0.19 | 0 | 0 | 0.63 | 0.17 | 0 | 0 |
| ΔTVOC vs HF | 0.96 | −0.24 | 3 | 0 | 0.42 | −0.26 | 4 | 0 | 1.04 | −0.40 | 2 | 0 | 1.08 | 0.22 | 0 | 0 |
| TVOC vs LF/HF | 0.54 | −0.12 | 1 | 0 | 0.41 | 0.10 | 0 | 2 | 1.31 | 0.09 | 1 | 0 | 0.62 | −0.03 | 0 | 0 |
| ΔTVOC vs LF/HF | 0.99 | 0.27 | 0 | 1 | 0.45 | 0.14 | 1 | 2 | 1.34 | 0.34 | 0 | 2 | 0.80 | −0.05 | 0 | 0 |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Mizukoshi, A.; Kumagai, K.; Yamamoto, N.; Noguchi, M.; Yoshiuchi, K.; Kumano, H.; Yanagisawa, Y. A Novel Methodology to Evaluate Health Impacts Caused by VOC Exposures Using Real-Time VOC and Holter Monitors. Int. J. Environ. Res. Public Health 2010, 7, 4127-4138. https://doi.org/10.3390/ijerph7124127
Mizukoshi A, Kumagai K, Yamamoto N, Noguchi M, Yoshiuchi K, Kumano H, Yanagisawa Y. A Novel Methodology to Evaluate Health Impacts Caused by VOC Exposures Using Real-Time VOC and Holter Monitors. International Journal of Environmental Research and Public Health. 2010; 7(12):4127-4138. https://doi.org/10.3390/ijerph7124127
Chicago/Turabian StyleMizukoshi, Atsushi, Kazukiyo Kumagai, Naomichi Yamamoto, Miyuki Noguchi, Kazuhiro Yoshiuchi, Hiroaki Kumano, and Yukio Yanagisawa. 2010. "A Novel Methodology to Evaluate Health Impacts Caused by VOC Exposures Using Real-Time VOC and Holter Monitors" International Journal of Environmental Research and Public Health 7, no. 12: 4127-4138. https://doi.org/10.3390/ijerph7124127
APA StyleMizukoshi, A., Kumagai, K., Yamamoto, N., Noguchi, M., Yoshiuchi, K., Kumano, H., & Yanagisawa, Y. (2010). A Novel Methodology to Evaluate Health Impacts Caused by VOC Exposures Using Real-Time VOC and Holter Monitors. International Journal of Environmental Research and Public Health, 7(12), 4127-4138. https://doi.org/10.3390/ijerph7124127