Economic Evaluation and Transferability of Physical Activity Programmes in Primary Prevention: A Systematic Review

Abstract
:1. Introduction
2. Methods
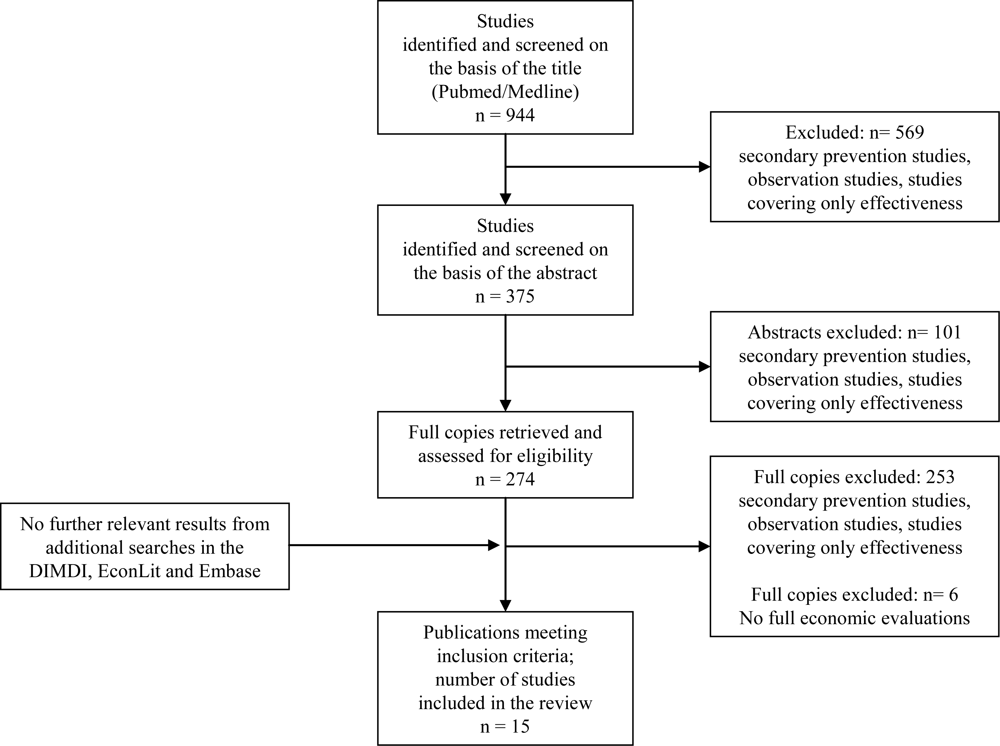
2.1. Search Process
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Criteria
2.4. Study Characteristics and Key Findings
2.5. Clinical and Economic Evidence
2.6. Transferability
3. Results
3.1. Study Characteristics and Key Findings
3.2. Clinical and Economic Evidence in the Special Country Context
3.3. Transferability
4. Discussion
5. Conclusions
Acknowledgments
Appendix


{kind=link}
| Author's name (year) | Is the study clearly described? | Are competing alternatives clearly described? | Is a well-defined research question posed in answerable form? | Is the economic study design appropriate to the stated objective? | Is the chosen time horizon appropriate in order to include relevant costs and consequences?2 | Is the actual perspective chosen appropriate? | Are all important and relevant costs for each alternative identified? | Are all costs measured appropriately in physical units? | Are costs valued appropriately? | Are all important and relevant outcomes for each alternative identified? | Are all outcomes measured appropriately? | Are outcomes valued appropriately`? | Is an incremental analysis of costs and outcomes for each alternative performed? | Are all future costs and outcomes discounted appropriately?3 | Are all important variables, whose values are uncertain, appropriately subjected to sensitivity analysis? | Do the conclusions follow from the data reported? | Does the study discuss the generalisability of the results to other settings and patient/ client groups? | Does the article indicate that there is no potential conflict of study researcher(s) and funder(s)? | Are ethical and distributional issues discussed appropriately? | Economic evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dzator et al. (2004) [51] | 0,5 | 1,0 | 1,0 | 1,0 | 0,5 | 0,0 | 0,5 | 0,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 0,74 |
| Elley et al. (2004) [38] | 1,0 | 0,5 | 1,0 | 1,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 0,0 | 0,87 |
| Finkelstein et al. (2002) [40] | 1,0 | 0,5 | 1,0 | 1,0 | 0,5 | 0,0 | 0,5 | 0,0 | 0,5 | 1,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 1,0 | 0,74 |
| Robertson et al. (2001a) [50] | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 0,92 |
| Robertson et al. (2001b) [49] | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 0,0 | 0,89 |
| Robertson et al. (2001c) [48] | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 0,89 |
| Stevens et al. (1998) [42] | 1,0 | 1,0 | 1,0 | 0,5 | 0,0 | 0,0 | 0,0 | 0,0 | 0,0 | 1,0 | 1,0 | 1,0 | 0,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 0,61 |
| The Writing Group (2001) [47] | 1,0 | 1,0 | 0,5 | 0,0 | 1,0 | 0,0 | 0,0 | 0,0 | 0,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 0,0 | 0,5 | 0,0 | 1,0 | 0,0 | 0,47 |
| Proper et al. (2004) [41] | 1,0 | 1,0 | 0,5 | 1,0 | 0,0 | 0,5 | 1,0 | 0,0 | 0,5 | 1,0 | 1,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 0,74 |
| Shepard (1992) [37] | 0,5 | 0,5 | 0,5 | 1,0 | 1,0 | 0,0 | 0,5 | 0,5 | 0,5 | 1,0 | 0,5 | 0,5 | 0,0 | 0,0 | 0,0 | 1,0 | 0,5 | 0,0 | 1,0 | 0,50 |
| Chen et al. (2008) [36] | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 0,0 | 1,0 | 0,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 1,0 | 0,5 | 1,0 | 1,0 | 0,74 |
| Dalziel K, Segal L (2006) [44] | 1,0 | 0,5 | 1,0 | 1,0 | 1,0 | 0,5 | 0,5 | 0,5 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 1,0 | 0,0 | 0,79 |
| Lindgren P et al. (2003) [43] | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 0,5 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 0,5 | 1,0 | 0,0 | 0,82 |
| Munro et al. (2004) [39] | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,0 | 1,0 | 1,0 | 0,5 | 1,0 | 0,0 | 0,84 |
| Sims J et al. (2004) [45] | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 0,5 | 0,5 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 1,0 | 0,5 | 1,0 | 0,0 | 0,82 |
| Author (year) | Main Limitations with respect to transferability |
|---|---|
| Dzator et al. (2004) [51] | duration of the intervention relatively short (16 weeks); higher economic status was over-represented in the study (potential bias); responders more motivated than non responders (selection bias); perspective not stated; only costs were discounted; price year not stated; high clinical and moderate economic evidence |
| Elley et al. (2004) [38] | control group may have taken part in exercise trial (potential bias); 1/3 of eligible participants did not participate (selection bias); large 95%CIs and imprecision around changes in major offset costs, especially healthcare utilisation costs and productivity costs (an overall cost-effectiveness from societal perspective could not be calculated); only costs were discounted; moderate clinical and high economic evidence |
| Finkelstein et al. (2002) [40] | baseline comparability of two groups not discussed; uninsured, low income women (US specific sample); no control group with no intervention; no discussion about women not taking part in interventions; no sensitivity analysis; perspective not stated; costs for single unit are not stated; price year not stated; only effects discounted; moderate clinical and moderate economic evidence |
| Robertson et al. (2001a) [50] | district nurse (potential instructor bias); only cost-saving for people older than 80 years; costs could be different in an urban area (e.g., less transport costs); high clinical and high economic evidence |
| Robertson et al. (2001b) [49] | general practice nurse (potential instructor bias); costs could be different in an urban area (e.g., less transport costs); no randomisation; moderate clinical and high economic evidence |
| Robertson et al. (2001c) [48] | research physiotherapist (potential instructor bias); costs could be different in an urban area (e.g., less transport costs); no discounting; high clinical and high economic evidence |
| Stevens et al. (1998) [42] | perspective not stated; no explanation for choice of comparator; no data on effectiveness; exercise development officer (potential therapist bias); short intervention time (10 weeks); unit costs could be halved with a better recruitment strategy; ICER not stated; perspective not stated; physical units not stated; no discount rate; price year not stated; valuation of the costs not mentioned; high clinical and moderate economic evidence |
| The Writing Group (2001) [47] | only effects are differentiated; not significantly effective for men; perspective not stated; discount rate not stated; physical units not stated; sensitivity analysis not stated; cost measurement and valuation not stated; high clinical and low economic evidence |
| Proper et al. (2004) [41] | large CIs of CE-Ratios (not statistical significant);health care costs only accountable by municipal service; underpowered trial= 94–167; potential other benefits excluded like employer turnover, productivity, commitment; CBA is a CEA (no monetary valuing of the benefits); price year not stated; physical units not stated; high clinical and moderate economic evidence |
| Shepard (1992) [37] | costs not stated explicitly; study years not stated appropriately; no randomisation of the study population; not all items of programme costs calculated; CEA and CBA are not explained adequately; no further description of the target population; ICER not stated; perspective not stated; no discounting; physical units not clearly stated; sensitivity analysis not stated; moderate clinical and low economic evidence |
| Chen et al. (2008) [36] | perspective not stated; physical units not stated; no sensitivity analyses; short time horizon; valuation of utilisation not stated; only programme costs included; high clinical and moderate economic evidence |
| Lindgren P et al. (2003) [43] | only 60 year old men - transferability to other ages unclear; Markov Model uses risk factors taken from Framingham (calculated for UK and Germany); only Human Capital approach; Physical activity programme not described; high clinical and high economic evidence |
| Dalziel K, Segal L (2006) [44] | based on many assumptions; wide range of ICER; short follow up period in the primary clinical trial (Elley et al.2004);moderate clinical and moderate to high economic evidence |
| Munro et al. (2004) [39] | SF-36 non responders were assumed having no health benefit; benefit by participants in exercise programmes greater than the suggests (potential selection bias); exclusion of the top 20% (selection bias); participation rate and levels of missing data are correlated; low recruitment rate; follow-up period too short for mortality and admission rates; no discounting; moderate clinical and high economic evidence |
| Sims J et al. (2004) [45] | method of discounting not explained; model and costs not described in detail; no indirect costs; percentage of patients to become active assumed; moderate clinical and high economic evidence |
| Author (year published) [Ref.] | Study design/Type of EconA | Type of physical exercise intervention/alternative/length of intervention | Outcomes | Study Population: n/age (range or mean)/exclusion and/or inclusion criteria | Country/setting/year of study | Economic key findings | EURO conversion (2008) | Clin.*/ econ. evidence (h, l, m)** |
|---|---|---|---|---|---|---|---|---|
| Dzator et al. (2004) [51] | RCT/CEA | Self-directed intervention of PA and nutrition delivered by mail (low level) or by mail and group sessions (high level)/no intervention/16 weeks | Change in BMI, total and HDL cholesterol, blood pressure, PA (W/kg), nutrition fat intake | 137 couples/all ages/IN: cohabitation for the first time, living together for < 2 years, no pregnancy for length of study/EX: CHD, severe asthma, diabetes | Australia/ home/ n.s. | 1-year follow up: Average incremental costs/unit change in outcome variables:1) high intervention: AUD460; 2) low intervention: AUD459; 3) control: AUD462 | No year of intervention | 1+/m |
| Elley et al. (2004) [38] | Cluster RCT/CEA | Green Prescription: verbal and written exercise advice by GP and telephone exercise specialist/usual care/1 year | Total energy expended (change in PA), QALY | 878/40-79 years/IN: less active (<2.5 hours of moderate activity per week) | New Zealand/ GPP/ 2000–2002 | 1) Monthly CER: NZD11/kcal/kg/day; 2) ICER: NZD1,756/ converted sedentary adult to an active state in 12 months | 1) €8; 2) €1,268 | 1−/h |
| Finkelstein et al. (2002) [40] | RCT/CEA | WISEWOMAN Project: screening and counselling (e.g., walking, dance, chair-aerobics, weight training)/MI vs. EI/1 year | Risk of CHD, LYG | 1586 women/40–64 years/IN: uninsured or underinsured with low annual income/take part in NBCCED-programme | USA/ community and healthcare sites/1996 | 1) IC of EI per person: USD191; 2) ICER: USD637/ 1%point additional decrease in 10 year probability of CHD for EI compared with MI; 3) nearly USD5,000/ LYG (n.sig.) | Apy (1996): 1) €226; 2) ICER: €753; 3) €5,911 | 1−/m |
| Robertson et al. (2001a) [50] | RCT/CEA | Otago: Individually home-based PA by district nurse/usual care/1 year | Falls and injuries | 240/≥75 years/invited by GP/EX: abasia, receiving physiotherapy | New Zealand/ GPP/ 1998 | 1) ICER: NZD1,803/ fall prevented; 2) NZD7,471/ injurious fall prevented (cost saving for people older than 80 years) | 1) €1,423; 2) €5,898 | 1+/h |
| Robertson et al.(2001b)[49] | CT/CEA | Otago: Individually home-based PA by general practicenurse/usualcare/1 year | Falls and injuries | 450/≥80 years/invited by GP/EX: abasia, receiving physiotherapy | New Zealand/ GPP/ 1998 | 1) ICER: NZD1,519/ fall prevented;2) NZD3,404/ injurious fall prevented | 1) €1,202;2)€2,694; | 2+/h |
| Robertson et al. (2001c) [48] | RCT/CEA | Otago: Individually home-based PA by physiotherapist/usual care/2 years | Falls and injuries | 233 women/≥80 years/invited by GP/EX: abasia, receiving physiotherapy | New Zealand/ GPP, home/ 1995–1997 | 1) ICER: NZD314/ fall prevented (1 year); NZD265/ fall prevented (2 years) 2) NZD457/ injurious fall prevented (1year); NZD 426/ injurious fall prevented (2 years) | 1) €261; €220 2) €379; €353 | 1+/h |
| Stevens et al. (1998) [42] | RCT/CEA | Individual PA by exercise development officer/ EI vs MI/10 weeks | PA, number of sedentary people | 714 participants/45–74 years/four subgroups (sedentary, low/high intermediate, active)/2 GPP/EX: disabled, CHD | UK/GPP/n.s. | 1) £623/ one sedentary person doing more PA; 2) £2,498/ moving someone who is active but below min level | No year of intervention | 1+/m |
| The Writing Group (2001) [47] | RCT/costs, effects (CEA) | PA counselling with current recommended care/usual care/2 years | Cardio-respiratory fitness, self-reported PA | 874/35–75 years/IN: inactive, in primary care, in stable health, EX: chronic diseases, CHD | USA/GPP/ 1995–1997 | 1) For 2 years: IC/ participant of assistance intervention: USD500; 2) IC of counselling intervention/ participant: USD1,100 | Apy (1996): 1) €591; 2) €1,300 | 1++/l |
| Proper et al. (2004) [41] | RCT/CBA, CEA | Worksite PA counselling/EI vs. MI/9 months | Sick leave, PA, cardiovascular fitness | 299/44 years/IN: civil servants from three municipal services, performing office work at least 24 hours a week | Netherlands/ municipal services/ 2000–2001 | CER without (with) imputation of effect data: 1) €5 (€3)/ extra energy expenditure (kcal/day); 2) €235 (€46)/ beat per minute of decrease in submaximale heart rate; 3) total net costs (9 months): €305; 4) benefits from sick leave reduction (1 year later): €635 | Apy (2000): 1) €6 (€3); 2) €267 (€52); 3) €346; 4) €721 | 1+/m |
| Shepard (1992) [37] | CT/CBA, CEA | Employee fitness programme (rhythmic, aerobic type activity, stretching, cardio-respiratory activity)/no intervention/12 years | PA, absenteeism, corporate commitment | 534/age n.s./office workers of two major insurance companies | Canada/ company/ 1977–1990 | 1) Programme benefits/worker/year (participation rate of 20%): CAD679; 2) ROI: CAD7; 3) Cost-benefit: CAD5 to 1 | 1) €757; 2) €8; 3) €5 to 1 | 2-/l |
| Chen et al. (2008) [36] | Cluster RCT/CUA | Walking/no intervention/12 weeks | Health service utilisation, QALY | 98/>65 years | Taiwan/community/n.s. | ICER: USD15,103/ QALY gained | No year of intervention | 1−/m |
| Dalziel/ Segal (2006) [44] | Cluster RCT/CUA (Markov Model) | Green Prescription: verbal and written exercise advice by GP and telephone exercise specialist/usual care/1 year | Lifestyle change, activity change, QALYs | 878/40–79 years/42 GPP/IN: less active | New Zealand/ GPP/ 2000–2002 | ICER: NZD2,053/ QALY gained (lifetime) | €1,483 | 1−/m |
| Lindgren et al. (2003) [43] | RCT/CEA, CUA (Markov Model) | Dietary advice by dietician and exercise instructions by physician/usual care/18 months | Physiological factors, QALYs, LYG | 813 men/60 years/EX: CHD, diabetes, severe illness, no cholesterol, regular use of drugs | Sweden/ community/ 1992 | ICER (declining effect of intervention): 1) Diet: SEK127,065/ LYG (SEK130,505/ QALY gained); 2) Exercise: SEK180,470/ LYG (SEK191,750/ QALY gained); 3) Exercise+diet: SEK201,375/ LYG (SEK201,375/ QALY gained) | 1) €15,274 (€15,687); 2) €21,693 (€23,049); 3) €24,206 (€24,206) | 1+/h |
| Munro et al. (2004) [39] | Cluster RCT/CUA | Free exercise classes (e.g., bowling, swimming, country walking, and tea dances) by qualified exercise leader/usual care/2 years | Mortality, hospital service use, health status, QALY | 6420/>65 years/EX: PA score in the top 20%, patients who were unsuitable for exercise | UK/ community/ 2003–2004 | ICER: €17,172/ QALY gained | ICER: €18,364 | 1−/h |
| Sims et al. (2004) [45] | Cluster RCT/CEA, CUA (Model) | Active Script Programme (ASP): training and support of GPs who deliver advice on PA/usual care/2 years | Number of advising GPs, patients becoming active or accruing health benefit, DALYs/deaths averted | 670 GPs/practice population/20–75 years, sedentary | Australia/ GPP/ community/ 1999–2000, 2000–2001 | 1) AUD69/ patient to become more active (short term); 2) AUD138/ patient to accrue a health benefit; 3) AUD3,647/ DALY saved; 4) AUD48,924/ premature death averted | 1) €62; 2) €123; 3) €3,258; 4) €48,708 | 1−/h |
References and Notes
- World Health Organization (WHO) European Region. Health 2: The Health Policy Framework for the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- World Health Organization (WHO) Physical Activity.
- Konig, D; Bonner, G; Berg, A. The role of adiposity and inactivity in primary prevention of cardiovascular disease. Herz 2007, 32, 553–559. [Google Scholar]
- Fuchs, R. Sport, Gesundheit und Public Health [in German], 1st ed; Hogrefe: Göttingen, Bern, Toronto, Seattle, 2003; p. 273. [Google Scholar]
- Colberg, SR. Physical activity, insulin action, and diabetes prevention and control. Curr. Diabetes Rev 2007, 3, 176–184. [Google Scholar]
- Goldstein, LB; Adams, R; Alberts, MJ; Appel, LJ; Brass, LM; Bushnell, CD; Culebras, A; Degraba, TJ; Gorelick, PB; Guyton, JR; Hart, RG; Howard, G; Kelly-Hayes, M; Nixon, JV; Sacco, RL. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council and the Quality of Care and Outcomes Research Interdisciplinary Working Group: the American Academy of Neurology affirms the value of this guideline. Stroke 2006, 37, 1583–1633. [Google Scholar]
- Karmisholt, K; Gyntelberg, F; Gotzche, PC. Physical activity for primary prevention of disease. Systematic reviews of randomised clinical trials. Dan. Med. Bull 2005, 52, 86–89. [Google Scholar]
- Lakka, TA; Laaksonen, DE. Physical activity in prevention and treatment of the metabolic syndrome. Appl. Physiol. Nutr. Metab 2007, 32, 76–88. [Google Scholar]
- Schuler, G. Primary and secondary prevention: physical activity. Z. Kardiol 2002, 91, 30–39. [Google Scholar]
- Unsworth, J; Mode, A. Preventing falls in older people: risk factors and primary prevention through physical activity. Br. J. Community Nurs 2003, 8, 214–220. [Google Scholar]
- Gardner, MM; Robertson, MC; Campbell, AJ. Exercise in preventing falls and fall related injuries in older people: a review of randomised controlled trials. Br. J. Sports Med 2000, 34, 7–17. [Google Scholar]
- Biddle, S; Fox, KR; Boutcher, SH. Physical Activity and Psychological Well Being, 1st ed; Routledge: London, UK, 2000; p. 224. [Google Scholar]
- Avenell, A; Broom, J; Brown, TJ; Poobalan, A; Aucott, L; Stearns, SC; Smith, WC; Jung, RT; Campbell, MK; Grant, AM. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technol Assess 2004, 8. [Google Scholar]
- Ebrahim, S. Cost-effectiveness of stroke prevention. Br. Med. Bull 2000, 56, 557–570. [Google Scholar]
- Hill, JO; Sallis, JF; Peters, JC. Economic analysis of eating and physical activity: a next step for research and policy change. Am. J. Prev. Med 2004, 27, 111–116. [Google Scholar]
- Kouris-Blazos, A; Wahlqvist, ML. Health economics of weight management: evidence and cost. Asia Pac. J. Clin. Nutr 2007, 16, 329–338. [Google Scholar]
- Piirtola, M; Isoaho, R; Kivela, SL. Physical exercise is an advantageous and effective way to prevent falls and injuries due to falls. Duodecim 2003, 119, 599–604. [Google Scholar]
- Gordon, NF; English, CD; Contractor, AS; Salmon, RD; Leighton, RF; Franklin, BA; Haskell, WL. Effectiveness of three models for comprehensive cardiovascular disease risk reduction. Am. J. Cardiol 2002, 89, 1263–1268. [Google Scholar]
- Hagberg, LA; Lindholm, L. Is promotion of physical activity a wise use of societal resources? Issues of cost-effectiveness and equity in health. Scand. J. Med. Sci. Sports 2005, 15, 304–312. [Google Scholar]
- Matrix research and consultancy NICE Rapid review of the economic evidence of physical interventions. Available online: http://www.nice.org.uk/nicemedia/pdf/Physical_Activity_Economic_Review_April2006.pdf (accessed February 2008).
- Shepard, RJ. Current Perspectives on the Econommics of Fitness and Sport with Particular Reference to Worksite Progammes. Sports Med 1989, 7, 286–309. [Google Scholar]
- Institute for Quality and Efficiency in Health Care (Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG)). Allgemeine Methoden, Entwurf für Version 2.0 vom 19.12.2006 [in German]; Institute for Quality and Efficiency in Health Care (Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG)): Cologne, Germany, 2006. [Google Scholar]
- Moher, D; Liberati, A; Tetzlaff, J; Altman, DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J. Clin. Epidemiol 2009, 62, 1006–1012. [Google Scholar]
- Statistics Directorate (OECD). Purchasing Power Parities (PPP). Available online: http://www.oecd.org/department/0,3355,en_2649_34357_1_1_1_1_1,00.html (accessed February 2008).
- Organisation for Economic Co-operation and Development (OECD). Consumer Price Indices. Available online: http://stats.oecd.org/wbos/default.aspx (accessed February 2008).
- Institute for Quality and Efficiency in Health Care (IQWiG). Allgemeine Methoden, Entwurf für Version 3.0 vom 15.11.2007 [in German]; Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG): Cologne, Germany, 2007. [Google Scholar]
- Oostenbrink, JB; Koopmanschap, MA; Rutten, FF. Standardisation of costs: the Dutch Manual for Costing in economic evaluations. Pharmacoeconomics 2002, 20, 443–454. [Google Scholar]
- National Institute for Clinical Excellence (NICE). Guideline Development Methods: Information for National Collaborating Centres and Guideline Developers; National Institute for Clinical Excellence: London, UK, 2004. [Google Scholar]
- Feinstein, A. Clinical Epidemiology: The Architecture of Clinical Research; Saunders: Philadelphia, PA, USA, 1985. [Google Scholar]
- Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG). Allgemeine Methoden, Entwurf für Version 3.0 vom 15.11.2007; Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG): Cologne, Germany, 2007. [Google Scholar]
- Drummond, MF; Jefferson, TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ 1996, 313, 275–283. [Google Scholar]
- Evers, S; Goossens, M; de Vet, H; van Tulder, M; Ament, A. Criteria list for assessment of methodological quality of economic evaluations: Consensus on Health Economic Criteria. Int. J. Technol. Assess Health Care 2005, 21, 240–245. [Google Scholar]
- Siegel, JE; Weinstein, MC; Russell, LB; Gold, MR. Recommendations for reporting cost-effectiveness analyses. Panel on Cost-Effectiveness in Health and Medicine. JAMA 1996, 276, 1339–1341. [Google Scholar]
- Chiou, C; Hay, J; Wallace, J; Bloom, B; Neumann, P; Sullivan, S. Development and validation of a grading system for the quality of cost-effectiveness studies. Med. Care 2003, 41, 32–44. [Google Scholar]
- Welte, R; Feenstra, T; Jager, H; Leidl, R. A decision chart for assessing and improving the transferability of economic evaluation results between countries. Pharmacoeconomics 2004, 22, 857–876. [Google Scholar]
- Chen, IJ; Chou, CL; Yu, S; Cheng, SP. Health services utilization and cost utility analysis of a walking program for residential community elderly. Nurs. Econ 2008, 26, 263–269. [Google Scholar]
- Shephard, RJ. Long term impact of a fitness programme—the Canada Life Study. Ann. Acad. Med. Singapore 1992, 21, 63–68. [Google Scholar]
- Elley, R; Kerse, N; Arroll, B; Swinburn, B; Ashton, T; Robinson, E. Cost-effectiveness of physical activity counselling in general practice. N. Z. Med. J 2004, 117, U1216. [Google Scholar]
- Munro, JF; Nicholl, JP; Brazier, JE; Davey, R; Cochrane, T. Cost effectiveness of a community based exercise programme in over 65 year olds: cluster randomised trial. J. Epidemiol. Community Health 2004, 58, 1004–1010. [Google Scholar]
- Finkelstein, EA; Troped, PJ; Will, JC; Palombo, R. Cost-effectiveness of a cardiovascular disease risk reduction program aimed at financially vulnerable women: the Massachusetts WISEWOMAN project. J. Womens Health Gend. Based Med 2002, 11, 519–526. [Google Scholar]
- Proper, KI; de Bruyne, MC; Hildebrandt, VH; van der Beek, AJ; Meerding, WJ; van Mechelen, W. Costs, benefits and effectiveness of worksite physical activity counseling from the employer’s perspective. Scand. J. Work Environ. Health 2004, 30, 36–46. [Google Scholar]
- Stevens, W; Hillsdon, M; Thorogood, M; McArdle, D. Cost-effectiveness of a primary care based physical activity intervention in 45–74 year old men and women: a randomised controlled trial. Br. J. Sports Med 1998, 32, 236–241. [Google Scholar]
- Lindgren, P; Fahlstadius, P; Hellenius, ML; Jonsson, B; de Faire, U. Cost-effectiveness of primary prevention of coronary heart disease through risk factor intervention in 60-year-old men from the county of Stockholm--a stochastic model of exercise and dietary advice. Prev. Med 2003, 36, 403–409. [Google Scholar]
- Dalziel, K; Segal, L; Elley, CR. Cost utility analysis of physical activity counselling in general practice. Aust. N. Z. J. Public Health 2006, 30, 57–63. [Google Scholar]
- Sims, J; Huang, N; Pietsch, J; Naccarella, L. The Victorian Active Script Programme: promising signs for general practitioners, population health, and the promotion of physical activity. Br. J. Sports Med 2004, 38, 19–25. [Google Scholar]
- Sevick, MA; Dunn, AL; Morrow, MS; Marcus, BH; Chen, GJ; Blair, SN. Cost-effectiveness of lifestyle and structured exercise interventions in sedentary adults: results of project ACTIVE. Am. J. Prev. Med 2000, 19, 1–8. [Google Scholar]
- The Writing Group for Activity Counselling Trail Research Group Effects of physical activity counseling in primary care: the Activity Counseling Trial: a randomized controlled trial. JAMA 2001, 286, 677–687.
- Robertson, MC; Devlin, N; Scuffham, P; Gardner, MM; Buchner, DM; Campbell, AJ. Economic evaluation of a community based exercise programme to prevent falls. J. Epidemiol. Community Health 2001c, 55, 600–606. [Google Scholar]
- Robertson, MC; Gardner, MM; Devlin, N; McGee, R; Campbell, AJ. Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 2: Controlled trial in multiple centres. BMJ 2001b, 322, 701–704. [Google Scholar]
- Robertson, MC; Devlin, N; Gardner, MM; Campbell, AJ. Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 1: Randomised controlled trial. BMJ 2001a, 322, 697–701. [Google Scholar]
- Dzator, JA; Hendrie, D; Burke, V; Gianguilio, N; Gillam, HF; Beilin, LJ; Houghton, S. A randomized trial of interactive group sessions achieved greater improvements in nutrition and physical activity at a tiny increase in cost. J. Clin. Epidemiol 2004, 57, 610–619. [Google Scholar]
- Shephard, RJ. Economics of the fitness industries. The Canadian scene since 1966. J. Sports Med. Phys. Fitness 1982, 22, 245–258. [Google Scholar]
- Shephard, RJ; Corey, P; Renzland, P; Cox, M. The impact of changes in fitness and lifestyle upon health care utilization. Can. J. Public Health 1983, 74, 51–54. [Google Scholar]
- Smith, DH; Gravelle, H. The practice of discounting in economic evaluations of healthcare interventions. Int. J. Technol. Assess Health Care 2001, 17, 236–243. [Google Scholar]
- Breucker, G. Kriterien und Beispiele guter Praxis—betrieblicher Gesundheitsförderung in Klein- und Mittelunternehmen (KMU) [in German]. Available online: http://www.dnbgf.de/fileadmin/texte/Downloads/uploads/dokumente/KRITERIEN__DEU_.PDF (accessed February 2008).
- Deutsches Netzwerk für Betriebliche Gesundheitsförderung (DNBGF) Positionspapier zum Forum Großunternehmen im DNBGF [in German]. Available online: http://www.dnbgf.de/fileadmin/texte/BGF/DNBGF_Positionspapier_Grossunternehmen.pdf (accessed February 2008).
- Graf von der Schulenburg, JM; Greiner, W; Jost, F; Klusen, N; Kubin, M; Leidl, R; Mittendorf, T; Rebscher, H; Schoeffski, O; Vauth, C; Volmer, T; Wahler, S; Wasem, J; Weber, C. German recommendations on health economic evaluation: third and updated version of the Hanover Consensus. Value Health 2008, 11, 539–544. [Google Scholar]
- Byford, S; Raftery, J. Economics notes: Perspectives in economic evaluation. BMJ 1998, 316, 1529–1530. [Google Scholar]
- Gold, MR; Russell, LB; Siegel, JE. Cost-Effectiveness in Health and Medicine, 1st ed; Oxford University Press: New York, NY, USA, 1996; p. 456. [Google Scholar]
- Adam, T; Koopmanschap, MA; Evans, DB. Cost-effectiveness analysis: can we reduce variability in costing methods? Int. J. Technol. Assess Health Care 2003, 19, 407–420. [Google Scholar]
- Statistics New Zealand. Work Stoppages—September 2005 Quarter. Available online: http://www.stats.govt.nz/cmsapp/templates/sws/hotOffThePress.aspx?NRMODE=Published&NRORIGINALURL=%2fstore%2f2006%2f01%2fwork-stoppages-sep05qtr-hotp%2ehtm%3fpage%3dpara003Master&NRNODEGUID=%7b0AD3D9A1-5184-4C19-A61C-C5F7750EA4A2%7d&NRCACHEHINT=NoModifyGuest&page=para003Master (accessed March 2008).
- BKK Bundesverband. BKK-Gesundheitsreport 2005. Available online: http://www.bkk.de/fileadmin/user_upload/PDF/Arbeitgeber/gesundheitsreport/Gesundheitsreport2005.pdf (accessed February 2008).
- BKK Bundesverband. BKK-Gesundheitsreport 2006. Available online: http://www.bkk.de/fileadmin/user_upload/PDF/Arbeitgeber/gesundheitsreport/BKK_Gesundheitsreport_2006.pdf (accessed April 2008).
- Koopmanschap, MA; Rutten, FF. A practical guide for calculating indirect costs of disease. Pharmacoeconomics 1996, 10, 460–466. [Google Scholar]
- Koopmanschap, MA; Rutten, FF; van Ineveld, BM; van Roijen, L. The friction cost method for measuring indirect costs of disease. J. Health Econ 1995, 14, 171–189. [Google Scholar]
- van Roijen, L; Koopmanschap, MA; Rutten, FF; van der Maas, PJ. Indirect costs of disease; an international comparison. Health Policy 1995, 33, 15–29. [Google Scholar] [Green Version]
- Flood, C. Profiles of six health care systems: Canada, Australia, The Netherlands, New Zealand, the UK, and the US. Available online: http://www.parl.gc.ca/37/1/parlbus/commbus/senate/com-e/soci-e/rep-e/volume3ver1-e.pdf (accessed March 2008).
- World Health Organization (WHO). Diet, physical activity and health. Available online: http://www.who.int/gb/ebwha/pdf_files/EB109/eeb10914.pdf (accessed February 2008).
- Fretheim, A; Oxman, AD. International variation in prescribing antihypertensive drugs: its extent and possible explanations. BMC Health Serv. Res 2005, 5, 21. [Google Scholar]
- Fuchs, R. Sport, Gesundheit und Public Health [in German]; Hogrefe: Göttingen, Bern, Toronto, Seattle, 2003; Volume 1. [Google Scholar]
- World Health Organization (WHO). European Health Report—Public Health Action for Healthier Children and Populations; WHO: Copenhagen, Denmark, 2005. [Google Scholar]
- OECD Health Data 2007 Statistics and Indicators for 30 Countries; OECD Health Division: Paris, France, 2007.
- Andersen, RM. Revisiting the behavioral model and access to medical care: does it matter? J. Health Soc. Behav 1995, 36, 1–10. [Google Scholar]
- Bradley, EH; McGraw, SA; Curry, L; Buckser, A; King, KL; Kasl, SV; Andersen, R. Expanding the Andersen model: the role of psychosocial factors in long-term care use. Health Serv. Res 2002, 37, 1221–1242. [Google Scholar]
- Lengerke, VT; Wolfenstetter, SB; John, J. Obesity associated utilization of health care in Germany [in German]. In Weighted Genes: Obesity between Predisposition and Self-Responsibility [Gewichtige Gene: Adipositas zwischen Prädisposition und Eigenverantwortung]; Hilbert, A, Dabrock, P, Eds.; Huber: Bern, Switzerland, 2008. [Google Scholar]
- Johnson, JA; Luo, N; Shaw, JW; Kind, P; Coons, SJ. Valuations of EQ-5D health states: are the United States and United Kingdom different? Med. Care 2005, 43, 221–228. [Google Scholar]
- Johnson, JA; Ohinmaa, A; Murti, B; Sintonen, H; Coons, SJ. Comparison of Finnish and U.S.-based visual analog scale valuations of the EQ-5D measure. Med. Decis. Making 2000, 20, 281–289. [Google Scholar]
- Ellert, U; Kurth, BM. Methodological views on the SF-36 summary scores based on the adult German population. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz ISO 2004, 47, 1027–1032. [Google Scholar]
- Scott, KM; Sarfati, D; Tobias, MI; Haslett, SJ. A challenge to the cross-cultural validity of the SF-36 health survey: factor structure in Maori, Pacific and New Zealand European ethnic groups. Soc. Sci. Med 2000, 51, 1655–1664. [Google Scholar]
- Ware, JE, Jr; Kosinski, M; Gandek, B; Aaronson, NK; Apolone, G; Bech, P; Brazier, J; Bullinger, M; Kaasa, S; Leplege, A; Prieto, L; Sullivan, M. The factor structure of the SF-36 Health Survey in 10 countries: results from the IQOLA Project. International Quality of Life Assessment. J. Clin. Epidemiol 1998, 51, 1159–1165. [Google Scholar]
- The World Bank Country Groups. Available online: http://web.worldbank.org/WBSITE/EXTERNAL/DATASTATISTICS/0,,contentMDK:20421402~pagePK:64133150~piPK:64133175~theSitePK:239419,00.html#High_income (accessed January 2010).
- Centre for Reviews and Dissemination. CRD’s Guidance for Undertaking Reviews in Health Care; University of York: York, UK, 2008. [Google Scholar]
- Pelletier, KR. A review and analysis of the clinical- and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: 1998–2000 update. Am. J .Health Promot 2001, 16, 107–116. [Google Scholar]
- Tucker, P; Gilliland, J. The effect of season and weather on physical activity: a systematic review. Public Health 2007, 121, 909–922. [Google Scholar]
- Plotnikoff, RC; Mayhew, A; Birkett, N; Loucaides, CA; Fodor, G. Age, gender, and urban-rural differences in the correlates of physical activity. Prev. Med 2004, 39, 1115–1125. [Google Scholar]
- Shephard, RJ; Corey, P; Renzland, P; Cox, M. The influence of an employee fitness and lifestyle modification program upon medical care costs. Can. J. Public Health 1982, 73, 259–263. [Google Scholar]
- Drummond, MF; Sculpher, M; Torrance, GW; O′Brien, BJ; Stoddart, GL. Methods for Economic Evaluation of Health Care Programmes, 3rd ed; Oxford University Press: Oxford, UK, New York, NY, USA, 2005; p. 396. [Google Scholar]
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Wolfenstetter, S.B.; Wenig, C.M. Economic Evaluation and Transferability of Physical Activity Programmes in Primary Prevention: A Systematic Review. Int. J. Environ. Res. Public Health 2010, 7, 1622-1648. https://doi.org/10.3390/ijerph7041622
Wolfenstetter SB, Wenig CM. Economic Evaluation and Transferability of Physical Activity Programmes in Primary Prevention: A Systematic Review. International Journal of Environmental Research and Public Health. 2010; 7(4):1622-1648. https://doi.org/10.3390/ijerph7041622
Chicago/Turabian StyleWolfenstetter, Silke B., and Christina M. Wenig. 2010. "Economic Evaluation and Transferability of Physical Activity Programmes in Primary Prevention: A Systematic Review" International Journal of Environmental Research and Public Health 7, no. 4: 1622-1648. https://doi.org/10.3390/ijerph7041622
APA StyleWolfenstetter, S. B., & Wenig, C. M. (2010). Economic Evaluation and Transferability of Physical Activity Programmes in Primary Prevention: A Systematic Review. International Journal of Environmental Research and Public Health, 7(4), 1622-1648. https://doi.org/10.3390/ijerph7041622