Can Intensive Use of Alcohol-Based Hand Rubs Lead to Passive Alcoholization?

Abstract
:1. Introduction
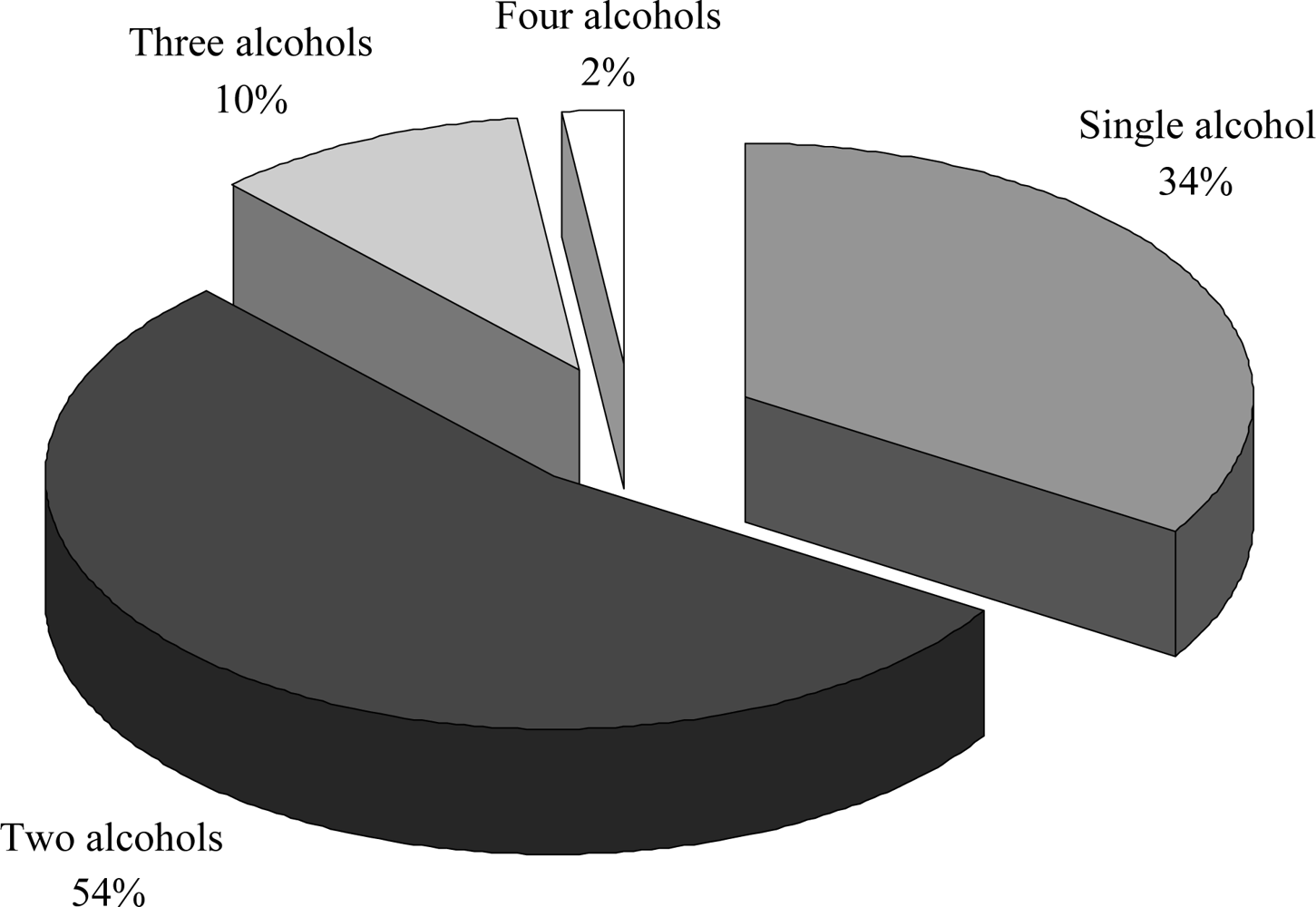
2. Alcohol-Based Hands Rubs
3. Intentional Alcohol Intake
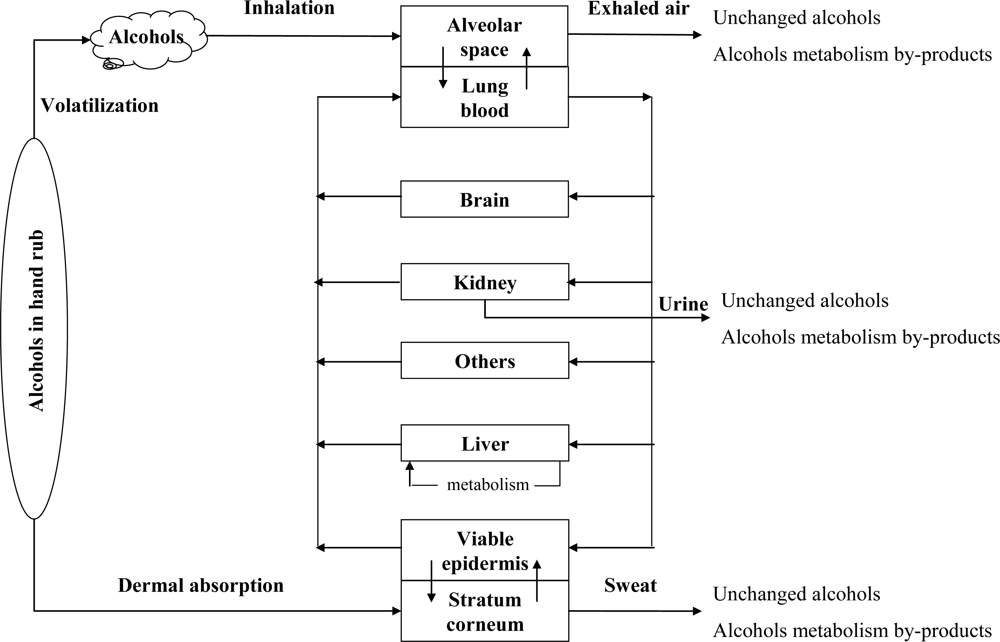
4. Unintentional Alcohol Intake
5. Risk Assessment
6. Conclusions
References
- Rotter, ML. Arguments for alcoholic hand disinfection. J. Hosp. Infect 2001, 48, S4–S8. [Google Scholar]
- Kampf, G. State-of-the-art hand hygiene in community medicine. Int. J. Hyg. Environ. Health 2003, 206, 465–472. [Google Scholar]
- Kampf, G; Kramer, A. Epidemiologic background of hand hygiene and evaluation of the most important agents for scrubs and rubs. Clin. Microbiol. Rev 2004, 17, 863–893. [Google Scholar]
- Girou, E; Loyeau, S; Legrand, P; Oppein, F; Brun-Buisson, C. Efficacy of handrubbing with alcohol based solution versus standard handwashing with antiseptic soap: randomised clinical trial. BMJ 2002, 325, 362–365. [Google Scholar]
- Kac, G; Podglajen, I; Gueneret, M; Vaupré, S; Bissery, A; Meyer, G. Microbiological evaluation of two hand hygiene procedures achieved by healthcare workers during routine patient care: a randomized study. J. Hosp. Infect 2005, 60, 32–39. [Google Scholar]
- Messina, MJ; Brodell, LA; Brodell, RT; Mostow, EN. Hand hygiene in the dermatologist’s office: To wash or to rub? J. Am. Acad. Dermatolo 2008, 59, 1043–1049. [Google Scholar]
- Boyce, JM. Using alcohol for hand antisepsis: dispelling old myths. Infect. Control Hosp. Epidemiol 2000, 21, 438–441. [Google Scholar]
- Kampf, G; Rudolf, M; Labadie, JC; Barrett, SP. Spectrum of antimicrobial activity and user acceptability of the hand disinfectant agent Sterillium “Gel”. J. Hosp. Infect 2002, 52, 141–147. [Google Scholar]
- Kampf, G; Löffler, H. Dermatological aspects of a successful introduction and continuation of alcohol-based hand rubs for hygienic hand disinfection. J. Hosp. Infect 2003, 55, 1–7. [Google Scholar]
- Kampf, G; Muscatiello, M. Dermal tolerance of Sterillium®, a propanol-based hand rub. J. Hosp. Infect 2003, 55, 295–298. [Google Scholar]
- Voss, A; Widmer, AF. No time for handwashing!? Handwashing versus alcoholic rub: can we afford 100% compliance? Infect. Control Hosp. Epidemiol 1997, 3, 205–208. [Google Scholar]
- Boyce, JM; Pittet, D. Guideline for hand hygiene in health-care settings. Am. J. Infect. Control 2002, 30, 1–46. [Google Scholar]
- Cargiulo, T. Understanding the health impact of alcohol dependence. Am. J. Health Syst. Pharm 2007, 64, S5–S11. [Google Scholar]
- International Agency for Research on Cancer (IARC). Alcohol drinking. IARC Monogr. Eval. Carcinog. Hum 1988, 44, 1–8. [Google Scholar]
- Kramer, A; Below, H; Bieber, N; Kampf, G; Toma, CD; Huebner, NO; Assadian, O. Quantity of ethanol absorption after excessive hand disinfection using three commercially available hand rubs is minimal and below toxic levels for humans. BMC Infect. Dis 2007, 7, 117. [Google Scholar]
- Price, PB. Bacteriology of normal skin: a new quantitative test applied to a study of the bacterial flora and the disinfectant action of mechanical cleansing. J. Infect. Dis 1939, 63, 301–318. [Google Scholar]
- Larson, EL; Morton, HE. Disinfection, Sterilization and Preservation; Block, SS, Ed.; Lea & Febiger: Philadelphia, PA, USA, 1991; pp. 191–203. [Google Scholar]
- Ali, Y; Dolan, MJ; Fendler, EJ; Larson, EL. Disinfection, Sterilization, and Preservation, 5th ed; Block, SS, Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001; pp. 229–254. [Google Scholar]
- WHO guidelines on hand hygiene in health care; World Health Organization: Geneva, Switzerland, 2009.
- Hazardous Substances Data Bank. Aminomethylpropanol; US National Library of Medecine: Bethesda, MD, USA, 2002. [Google Scholar]
- Hazardous Substances Data Bank. Benzyl alcohol; US National Library of Medecine: Bethesda, MD, USA, 2009. [Google Scholar]
- International Programme on Chemical Safety. Environmental Health Criteria 103: 2-propanol; World Health Organization: Geneva, Switzerland, 1990. [Google Scholar]
- Institut National de Recherche et de Sécurité. N-propanol; fiche toxicologique FT 211; INRS: Paris, France, 2004. [Google Scholar]
- Institut National de Recherche et de Sécurité. Ethanol; fiche toxicologique FT 48; INRS: Paris, France, 2007. [Google Scholar]
- Institut National de Recherche et de Sécurité. 2-Phenoxyethanol; fiche toxicologique FT 269; INRS: Paris, France, 2008. [Google Scholar]
- Société Française d'Hygiène Hospitalière. Liste positive désinfectants 2008. Hygienes 2008, 16, 95–118. [Google Scholar]
- Dyer, DL; Gerenraich, KB; Wadhams, PS. Testing a new alcohol-free hand sanitizer to combat infection. AORN J 1998, 68, 239–251. [Google Scholar]
- Kampf, G. The six golden rules to improve compliance in hand hygiene. J. Hosp. Infect 2004, 56, 3–5. [Google Scholar]
- Pittet, D. Compliance with hand disinfection and its impact on hospital-acquired infections. J. Hosp. Infect 2001, 48, S40–S46. [Google Scholar]
- Pittet, D; Hugonnet, S; Harbarth, S; Mourouga, P; Sauvan, V; Touveneau, S; Perneger, TV. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Lancet 2000, 356, 1307–1312. [Google Scholar]
- Scheithauser, S; Haefner, H; Schwarz, T; Schulze-Steinen, H; Schiefer, J; Koch, A; Engels, A; Lemmen, SW. Compliance with hand hygiene on surgical, medical, and neurologic intensive care units: Direct observation versus calculated disinfectant usage. Am. J. Infect. Control 2009, 37, 835–841. [Google Scholar]
- Erasmus, V; Daha, TJ; Brug, H; Richardus, JH; Behrendt, MD; Vos, MC; van Beeck, EF. Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infect. Control Hosp. Epidemiol 2010, 31, 283–294. [Google Scholar]
- Rehm, J; Room, R; Graham, K; Monteiro, M; Gmel, G; Sempos, CT. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: an overview. Addiction 2003, 98, 1209–1228. [Google Scholar]
- WHO Expert Committee on Problems Related To Alcohol Consumption; World Health Organization: Geneva, Switzerland, 2006.
- Anonymous. Diagnostic and Statistical Manual of Mental Disorders, 4th ed; American Psychatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Fadda, F; Rossetti, ZL. Chronic ethanol consumption: from neuroadaptation to neurodegeneration. Prog. Neurobiol 1998, 56, 385–431. [Google Scholar]
- Gerlich, MG; Krämer, A; Gmel, G; Maggiorini, M; Lüscher, TF; Rickli, H; Kleger, GR; Rehm, J. Patterns of alcohol consumption and acute myocardial infarction: a case-crossover analysis. Eur. Addict. Res 2009, 15, 143–149. [Google Scholar]
- Murray, RP; Connett, JE; Tyas, SL; Bond, R; Ekuma, O; Silversides, CK; Barnes, GE. Alcohol volume, drinking pattern, and cardiovascular disease morbidity and mortality: is there a U-shaped function? Am. J. Epidemiol 2002, 155, 242–248. [Google Scholar]
- Sesso, HD; Cook, NR; Buring, JE; Manson, JE; Gaziano, JM. Alcohol consumption and the risk of hypertension in women and men. Hypertension 2008, 51, 1080–1087. [Google Scholar]
- Mancinelli, R; Binetti, R; Ceccanti, M. Woman, alcohol and environment: emerging risks for health. Neurosci. Biobehav. Rev 2007, 31, 246–253. [Google Scholar]
- Connor, PD; Streissguth, AP. Effects of prenatal exposure to alcohol across the life span. Alcohol Health Res. World 1996, 20, 170–174. [Google Scholar]
- Mello, T; Ceni, E; Surrenti, C; Galli, A. Alcohol induced hepatic fibrosis: role of acetaldehyde. Mol. Aspects Med 2008, 29, 17–21. [Google Scholar]
- Clark, DB; Thatcher, DL; Tapert, SF. Alcohol, psychological dysregulation, and adolescent brain development. Alcohol. Clin. Exp. Res 2008, 32, 375–385. [Google Scholar]
- Guerri, C; Pascual, M. Mechanisms involved in the neurotoxic, cognitive, and neurobehavioral effects of alcohol consumption during adolescence. Alcohol 2010, 44, 15–26. [Google Scholar]
- Martin, PR; Singleton, CK; Hiller-Sturmhöfel, S. The role of thiamine deficiency in alcoholic brain disease. Alcohol Res. Health 2003, 27, 134–142. [Google Scholar]
- Singleton, CK; Martin, PR. Molecular mechanisms of thiamine utilization. Curr. Mol. Med 2001, 1, 197–207. [Google Scholar]
- Kopelman, MD; Thomson, AD; Guerrini, I; Marshall, EJ. The Korsakoff Syndrome: clinical aspects, psychology and treatment. Alcohol Alcohol 2009, 44, 148–154. [Google Scholar]
- Adams, SL; Harris, J; Haigh, C. Heavy alcohol consumption increased risk for prostate cancer. Hem/Onc Today 2009, 10, 25. [Google Scholar]
- Altieri, A; Garavello, W; Bosetti, C; Gallus, S; La Vecchia, C. Alcohol consumption and risk of laryngeal cancer. Oral Oncol 2005, 41, 956–965. [Google Scholar]
- Bagnardi, V; Blangiardo, M; La Vecchia, C; Corrao, G. Alcohol consumption and the risk of cancer: a meta-analysis. Alcohol Res. Health 2001, 25, 263–270. [Google Scholar]
- Heinen, MM; Verhage, BAJ; Ambergen, TAW; Goldbohm, RA; van den Brandt, PA. Alcohol consumption and risk of pancreatic cancer in the Netherlands cohort study. Am. J. Epidemiol 2009, 169, 1233–1242. [Google Scholar]
- Park, JY; Mitrou, PN; Dahm, CC; Luben, RN; Wareham, NJ; Khaw, KT; Rodwell, SA. Baseline alcohol consumption, type of alcoholic beverage and risk of colorectal cancer in the European prospective investigation into cancer and nutrition-Norfolk study. Cancer Epidemiol 2009, 33, 347–354. [Google Scholar]
- International Guide for Monitoring Alcohol Consumption and Related Harm; World Health Organization: Geneva, Switzerland, 2000.
- Brugnone, F; Perbellini, L; Apostoli, P; Bellomi, M; Caretta, D. Isopropanol exposure: environmental and biological monitoring in a printing works. Br. J. Ind. Med 1983, 40, 160–168. [Google Scholar]
- Ekberg, K; Barregård, L; Hagberg, S; Sällsten, G. Chronic and acute effects of solvents on central nervous system functions in floorlayers. Br. J. Ind. Med 1986, 43, 101–106. [Google Scholar]
- Nordling Nilson, L; Sällsten, G; Hagberg, S; Bäckman, L; Barregård, L. Influence of solvent exposure and aging on cognitive functioning: an 18 year follow up of formerly exposed floor layers and their controls. Occup. Environ. Med 2002, 59, 49–57. [Google Scholar]
- Nordling Nilson, L; Barregård, L; Sällsten, G; Hagberg, S. Self-reported symptoms and their effects on cognitive functioning in workers with past exposure to solvent-based glues: an 18-year follow-up. Int. Arch. Occup. Environ. Health 2007, 81, 69–79. [Google Scholar]
- Tonini, S; Dellabianca, A; Costa, CM; Lanfranco, A; Scafa, F; Candura, SM. Irritant vocal cord dysfunction and occupational bronchial asthma: differential diagnosis in a health care worker. Int. J. Occup. Med. Environ. Health 2009, 22, 401–406. [Google Scholar]
- Anonymous. Les expositions aux risques professionnels des personnels soignants en 2003-Premières informations synthèses; Direction de l'Animation de la Recherche, des Etudes et des Statistiques (DARES): Paris, France, 2009. [Google Scholar]
- Seitz, HK; Becker, P. Alcohol metabolism and cancer risk. Alcohol Res. Health 2007, 30, 38–47. [Google Scholar]
- International Programme on Chemical Safety. Environmental Health Criteria 102: 1-propanol; World Health Organization: Geneva, Switzerland, 1990. [Google Scholar]
- Clayton, GD; Clayton, FE. Patty’s Industrial Hygiene and Toxicology, 5th ed; John Wiley and Sons: New York, NY, USA, 2001; Volume 6, pp. 382–394. [Google Scholar]
- Hazardous Substances Data Bank. N-propanol; US National Library of Medecine: Bethesda, MD, USA, 2001. [Google Scholar]
- Hazardous Substances Data Bank. Isopropanol; US National Library of Medecine: Bethesda, MD, USA, 2001. [Google Scholar]
- International Programme on Chemical Safety. Screening Information Data Set: 2-Propanol; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Miller, MA; Rosin, A; Levsky, ME; Patel, MM; Gregory, TJD; Crystal, CS. Does the clinical use of ethanol-based hand sanitizer elevate blood alcohol levels? A prospective study. Am. J. Emerg. Med 2006, 24, 815–817. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Compounds | Molecular weight (g/mol) | Structural formula | Water solubility at 25°C (mg/L) | Henry’s constant at 25°C (atm.m3/mol) |
|---|---|---|---|---|
| Ethanol | 46.07 | CH3-CH2OH | Fully miscible | 5 × 10−6 |
| n-Propanol | 60.1 | CH3-CH2-CH2OH | Fully miscible | 7.41 × 10−6 |
| Isopropanol | 60.1 | CH3-CH2OH-CH3 | Fully miscible | 8.10 × 10−6 |
| Aminomethylpropanol | 89.14 | CH3-C(CH3)(NH2)-CH2OH | Fully miscible | 6.48 × 10−10 |
| Benzylalcohol | 108.14 | Ph-CH2OH | 42.9 | 3.37 × 10−7 |
| Phenoxyethanol | 138.17 | Ph-O-CH2-CH2OH | 26,700 | 4.72 × 10−8 |
| Compounds | 1 | 2 | 3 | 4 | Total |
|---|---|---|---|---|---|
| Ethanol | 25% | 46% | 29% | 25% | 39% |
| n-Propanol | 6% | 9% | 0% | 25% | 8% |
| Isopropanol | 71% | 39% | 21% | 25% | 40% |
| Aminomethylpropanol | 0% | 0% | 14% | 0% | 2% |
| Benzyl alcohol | 0% | 0% | 7% | 0% | 1% |
| Phenoxyethanol | 0% | 6% | 29% | 25% | 9% |
| Main chronic diseases | References (selection) |
|---|---|
| Liver cirrhosis | [42] |
| Fetal Alcohol Syndrome (FAS) | [40,41] |
| Cancer | [14,48–53] |
| Cardiovascular disorders | [37–39] |
| Neurological disorders | [43–47] |
| Compounds | Country | 8-hour time-weighted average (TWA) | 15 min short-term exposure level (STEL) | ||
|---|---|---|---|---|---|
| ppm | mg/m3 | ppm | mg/m3 | ||
| Ethanol | France | 1,000 | 1,950 | 5,000 | 9,500 |
| United States | 1,000 | 1,950 | ND | ND | |
| n-Propanol | France | 200 | 500 | ND | ND |
| United States | 200 | 500 | 250 | 625 | |
| Isopropanol | France | 400 | 980 | ND | ND |
| United States | 400 | 980 | 500 | 1,225 | |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Bessonneau, V.; Clément, M.; Thomas, O. Can Intensive Use of Alcohol-Based Hand Rubs Lead to Passive Alcoholization? Int. J. Environ. Res. Public Health 2010, 7, 3038-3050. https://doi.org/10.3390/ijerph7083038
Bessonneau V, Clément M, Thomas O. Can Intensive Use of Alcohol-Based Hand Rubs Lead to Passive Alcoholization? International Journal of Environmental Research and Public Health. 2010; 7(8):3038-3050. https://doi.org/10.3390/ijerph7083038
Chicago/Turabian StyleBessonneau, Vincent, Michel Clément, and Olivier Thomas. 2010. "Can Intensive Use of Alcohol-Based Hand Rubs Lead to Passive Alcoholization?" International Journal of Environmental Research and Public Health 7, no. 8: 3038-3050. https://doi.org/10.3390/ijerph7083038
APA StyleBessonneau, V., Clément, M., & Thomas, O. (2010). Can Intensive Use of Alcohol-Based Hand Rubs Lead to Passive Alcoholization? International Journal of Environmental Research and Public Health, 7(8), 3038-3050. https://doi.org/10.3390/ijerph7083038