Change of Exposure Response over Time and Long-Term Risk of Silicosis among a Cohort of Chinese Pottery Workers


Abstract
:1. Introduction
2. Methods
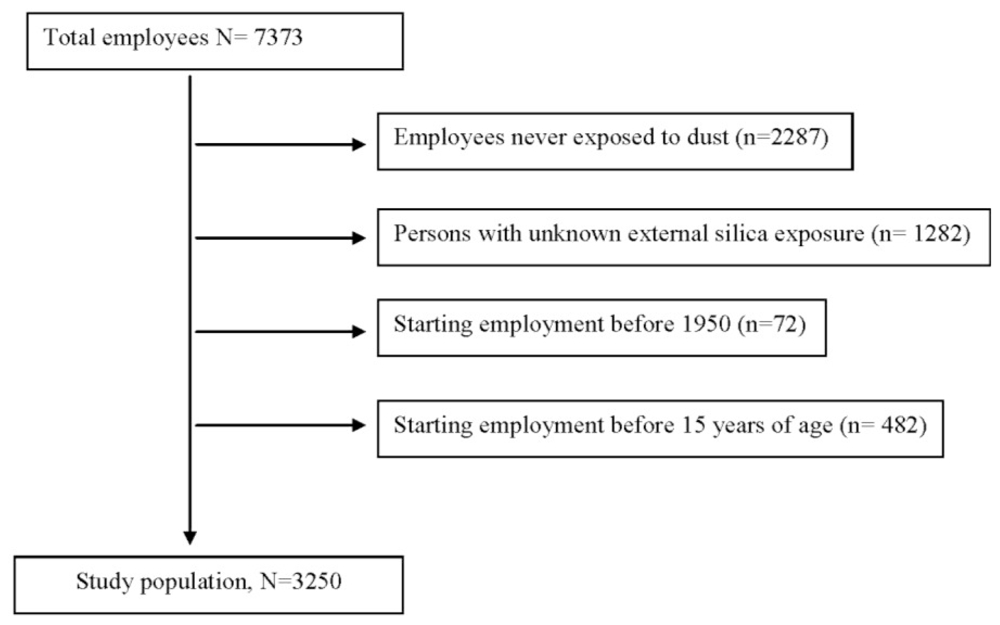
2.1. Design and Study Population
- Starting-date of employment after January 1, 1950 and aged over 15 years
- Minimum employment of 1 year
- Without unknown external silica dust exposure
2.2. Ascertainment of Incident Cases of Silicosis
2.3. Occupational Exposure Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
References
- Hunter, D. Diseases of Occupations, 6th ed; Hodder and Stoughton: London, UK, 1978. [Google Scholar]
- Information Note of International Labour Office (ILO). Proceedings of Thirteenth Session of the Joint ILO/WHO Committee on Occupational Health, Geneva, Switzerland, 9–12 December 2003.
- Silica, Some Silicates, Coal Dust, and Para-Aramid Fibrils. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; WHO: Lyon, UK, 1997; Volume 68.
- Chen, W; Zhuang, Z; Attfield, M; Chen, BT; Gao, P; Harrison, JC; Fu, C; Chen, JQ; Wallace, WE. Exposure to silica and silicosis among tin miners in China: Exposure-response analyses and risk assessment. Occup. Environ. Med 2001, 58, 31–37. [Google Scholar]
- Rice, FL; Park, R; Stayner, L; Smith, R; Gilbert, S; Checkoway, H. Crystalline silica exposure and lung cancer mortality in diatomaceous earth industry workers: A quantitative risk assessment. Occup. Environ. Med 2001, 58, 38–45. [Google Scholar]
- Steenland, K; Mannetje, A; Boffetta, P; Stayner, L; Attfield, M; Chen, J; Dosemeci, M; DeKlerk, N; Hnizdo, E; Koskela, R; et al. International agency for research on cancer. Pooled exposure-response analyses and risk assessment for lung cancer in 10 cohorts of silica-exposed workers: An IARC multicentre study. Cancer Causes Control 2001, 12, 773–784. [Google Scholar]
- Mannetje, A; Steenland, K; Attfield, M; Boffetta, P; Checkoway, H; DeKlerk, N; Koskela, RS. Exposure-response analysis and risk assessment for silica and silicosis mortality in a pooled analysis of six cohorts. Occup. Environ. Med 2002, 59, 723–728. [Google Scholar]
- Attfield, M; Costello, J. Quantitative exposure-response for silica dust and lung cancer in Vermont granite workers. Am. J. Ind. Med 2004, 45, 129–138. [Google Scholar]
- Chen, W; Bochmann, F; Sun, Y. Effects of work related confounders on the association between silica exposure and lung cancer: A nested case-control study among Chinese miners and pottery workers. Int. Arch. Occup. Environ. Health 2007, 80, 320–326. [Google Scholar]
- Mannetje, A; Steenland, K; Checkoway, H; Koskela, RS; Koponen, M; Attfield, M; Chen, J; Hnizdo, E; DeKlerk, N; Dosemeci, M. Development of quantitative exposure data for a pooled exposure-response analysis of 10 silica cohorts. Am. J. Ind. Med 2002, 42, 73–86. [Google Scholar]
- Sun, Y; Bochmann, F. Lifetime risk of silicosis death for quartz exposed workers among German population. Occup. Environ. Med 2004, 6, 374–375. [Google Scholar]
- Chen, J; McLaughlin, JK; Zhang, JY; Stone, BJ; Luo, J; Chen, RA; Dosemeci, M; Rexing, SH; Wu, Z; Hearl, FJ; et al. Mortality among dust-exposed Chinese miners and pottery workers. J. Occup. Med 1992, 34, 311–316. [Google Scholar]
- McLaughlin, JK; Chen, JQ; Dosemeci, M; Chen, RA; Rexing, SH; Wu, Z; Hearl, FJ; McCawley, MA; Blot, WJ. A nested case-control study of lung cancer among silica exposed workers in China. Br. J. Ind. Med 1992, 49, 167–171. [Google Scholar]
- Dosemeci, M; Chen, JQ; Hearl, F; Chen, RG; McCawley, M; Wu, Z; McLaughlin, JK; Peng, KL; Chen, AL; Rexing, SH; et al. Estimating historical exposure to silica among mine and pottery workers in the People’s Republic of China. Am. J. Ind. Med 1993, 24, 55–66. [Google Scholar]
- Chen, W; Hnizdo, E; Chen, JQ; Attfield, MD; Gao, P; Hearl, F; Lu, J; Wallace, WE. Risk of silicosis in cohorts of Chinese tin and tungsten miners, and pottery workers (I): An epidemiological study. Am. J. Ind. Med 2005, 48, 1–9. [Google Scholar]
- Zhuang, Z; Hearl, FJ; Odencrantz, J; Chen, W; Chen, BT; Chen, JQ; McCawley, MA; Gao, P; Soderholm, SC. Estimating historical respirable crystalline silica exposures for Chinese pottery workers and iron/copper, tin, and tungsten miners. Ann. Occup. Hyg 2001, 45, 631–642. [Google Scholar]
- Sun, Y; Chen, W; Yang, L; Bochmann, F. Quantitative Assessment of Historical Silica Dust Exposure among a Cohort of Chinese Pottery Workers, Tungsten Miners and Tin Miners. Proceedings of the 21th EPICOH Conference, Taipei, Taiwan, 20–25 April 2010.
- Ulm, K; Salanti, G. Estimation of the general threshold limit values for dust. Int. Arch. Occup. Environ. Health 2003, 76, 233–240. [Google Scholar]
- Wood, J; Richardson, D; Wing, S. A simple program to create exact person-time data in cohort analyses. Int. J. Epidemiol 1997, 26, 395–399. [Google Scholar]
- Statistical Analysis System Software, version 92; SAS Institute: Cary, NC, USA, 2008.
- Nelson, G; Girdler-Brown, B; Ndlovu, N; Murray, J. Three decades of silicosis: Disease trends at autopsy in South African gold miners. Environ. Health Perspect 2010, 118, 421–426. [Google Scholar]
- Steenland, K; Deddens, JA. A practical guide to dose-response analyses and risk assessment in occupational epidemiology. Epidemiology 2004, 15, 63–70. [Google Scholar]
- Sielken, RL; Valdez-Flores, C. Life-table calculations of excess risk for incidence versus mortality: Ethylene oxide case study. Regul. Toxicol. Pharmacol 2009, 55, 82–89. [Google Scholar]
- Hnizdo, E; Murray, J; Sluis-Cremer, GK; Thomas, RG. Correlation between radiological and pathological diagnosis of silicosis: An autopsy population based study. Am. J. Ind. Med 1993, 24, 427–445. [Google Scholar]
- Corbett, EL; Murray, J; Churchyard, GJ; Herselman, PC; Clayton, TC; de Cock, KM; Hayes, RJ. Use of miniradiographs to detect silicosis. Comparison of radiological with autopsy findings. Am. J. Respir. Crit. Care Med 1999, 160, 2012–2017. [Google Scholar]
- Meyer, JD; Islam, SS; Ducatman, AM; McCunney, RJ. Prevalence of small lung opacities in populations unexposed to dusts. A literature analysis. Chest 1997, 111, 404–410. [Google Scholar]
- Epstein, DM; Miller, WT; Bresnitz, EA; Levine, MS; Gefter, WB. Application of ILO classification to a population without industrial exposure: Finding to be differentiated from pneumoconiosis. Am. J. Roentgenol 1984, 142, 52–58. [Google Scholar]



{kind=link}
{kind=link}
| Potteries | ||
|---|---|---|
| N | 3,250 | |
| Age (years) | Start of follow-up: mean (SD) | 25.5 (6.5) |
| End of follow-up: mean (SD) | 60.3 (10.6) | |
| Sex (% female) | 24.4 | |
| Follow-up-duration (years) | Mean (SD) | 34.8 (8.9) |
| Median (range) | 36.6 (1.1–45) | |
| Silicosis | n (%) | 504 (15.5) |
| Smoking | Information available (%) | 99.9 |
| Non-smoker (%) | 39.6 | |
| Ex-smoker (%) | 28.6 | |
| Smoker (%) | 31.8 |
| Total dust | Respirable crystalline silica dust | |
|---|---|---|
| Long-term average exposure (mg/m3) | ||
| Mean (SD) | 6.1 (4.8) | 0.27 (0.19) |
| Median (min.–max.) | 4.8 (0–36.7) | 0.22 (0–1.16) |
| Highest exposure ever* (mg/m3) | ||
| Mean (SD) | 23.5 (11.6) | 0.73 (0.34) |
| Median (min.–max.) | 23.8 (0–65.8) | 0.74 (0–1.95) |
| Cumulative exposure (mg/m3-year) | ||
| Mean (SD) | 226.4 (171.0) | 7.32 (5.22) |
| Median (min.–max.) | 183.7 (0–861.7) | 6.20 (0–26.6) |
| Exposure duration (years) | ||
| Mean (SD) | 27.8 (7.4) | |
| Median (min.–max.) | 27.8 (1.1–46.4) | |
| No. of silicosis | Person-years | β | 95% CI | ||
|---|---|---|---|---|---|
| Intercept | −11.58 | −13.56, −9.58 | |||
| Age at first exposure (years) | ≤20 | 210 | 49,286 | 0 | – |
| 20–30 | 225 | 54,441 | 0.03 | −0.16, 0.22 | |
| >30 | 69 | 9,272 | 0.51 | 0.24, 0.78 | |
| Sex | female | 39 | 29,031 | 0 | – |
| male | 465 | 83,960 | 1.31 | 0.95, 1.66 | |
| Smoking | never | 135 | 47,839 | 0 | – |
| ever | 369 | 65,159 | 0.18 | −0.04, 0.39 | |
| Highest total dust exposure ever (mg/m3)* | 1. tertile | 166 | 46,256 | 0 | – |
| 2. tertile | 150 | 38,424 | 0.01 | −0.22, 0.25 | |
| 3. tertile | 188 | 28,319 | 0.37 | 0.01, 0.64 | |
| Time since the first exposure (years) | 0–9 | 1 | 21,463 | 0 | – |
| 10–19 | 30 | 31,597 | 2.92 | 0.92, 4.91 | |
| 20–29 | 208 | 29,510 | 4.90 | 2.93, 6.86 | |
| 30–39 | 244 | 20,657 | 5.44 | 3.48, 7.41 | |
| ≥40 | 21 | 9,771 | 3.84 | 1.83, 5.85 | |
| Long-term average total dust exposure ** | 1. quintile | 100 | 28,167 | 0 | – |
| 2. quintile | 100 | 17,902 | 0.37 | 0.09, 0.66 | |
| 3. quintile | 102 | 19,089 | 0.48 | 0.19, 0.77 | |
| 4. quintile | 101 | 15,132 | 0.66 | 0.34, 0.97 | |
| 5. quintile | 101 | 32,709 | 0.05 | −0.30, 0.40 | |
| No. of silicosis | Person-years | β | 95% CI | ||
|---|---|---|---|---|---|
| Intercept | −13.99 | −16.41, −11.56 | |||
| Age at first exposure (years) | ≤20 | 67 | 61,766 | 0 | – |
| 20–30 | 390 | 36,849 | 0.02 | −0.17, 0.21 | |
| >30 | 47 | 14,384 | 0.48 | −0.21, 0.75 | |
| Sex | female | 39 | 29,031 | 0 | – |
| male | 465 | 83,960 | 1.40 | 1.04, 1.76 | |
| Smoking | Never | 135 | 47,839 | 0 | – |
| ever | 369 | 65,159 | 0.16 | −0.06, 0.37 | |
| Highest silica exposure ever (mg/m3)* | <0.10 | 2 | 8,386 | 0 | – |
| 0.1–0.5 | 194 | 45,524 | 2.08 | 0.66, 3.50 | |
| >0.5–1.0 | 283 | 50,849 | 2.30 | 0.87, 3.73 | |
| >1.0 | 25 | 8,237 | 1.27 | −0.22, 2.76 | |
| Time since the first exposure (years) | 0–9 | 1 | 21,463 | 0 | – |
| 10–19 | 30 | 31,597 | 2.95 | 0.96, 4.94 | |
| 20–29 | 208 | 29,510 | 4.99 | 3.02, 6.95 | |
| 30–39 | 244 | 20,657 | 5.58 | 3.61, 7.55 | |
| ≥40 | 21 | 9,771 | 3.96 | 1.95, 5.97 | |
| Long-term average silica exposure (mg/m3) | <0.05 | 18 | 10,657 | 0 | – |
| 0.05–<0.10 | 35 | 9,811 | 0.24 | −0.33, 0.82 | |
| 0.10–<0.15 | 63 | 11,500 | 0.40 | −0.13, 0.93 | |
| 0.15–<0.20 | 85 | 14,459 | 0.59 | 0.07, 1.11 | |
| 20–<0.30 | 133 | 21,977 | 0.75 | 0.24, 1.27 | |
| 0.30–<0.40 | 95 | 16,155 | 0.84 | 0.29, 1.38 | |
| >=0.40 | 75 | 28,439 | 0.50 | −0.07, 1.07 | |
| 0.05 mg/m3 increase | 0.07 | 0.02, 0.11 | |||
| Highest silica exposure ever (mg/m3)* | Long-term average silica exposure (mg/m3)
| ||||
|---|---|---|---|---|---|
| 0 | 0.05 | 0.10 | 0.15 | 0.20 | |
| Long-term “excess” risk (compared to baseline) | |||||
| <0.1 | 0.9/1,000 | 1.9/1,000 | |||
| 0.1–0.5 | 138/1,000 | 147/1,000 | 157/1,000 | ||
| >0.5–1.0 | 179/1,000 | 191/1,000 | |||
| Long-term risk | |||||
| <0.1 | 13.6/1,000 | 14.5/1,000 | 15.5/1,000 | ||
| 0.1–0.5 | 152/1,000 | 161/1,000 | 171/1,000 | ||
| >0.5–1.0 | 193/1,000 | 205/1,000 | |||
© 2011 by the authors; licensee MDPI, Basel, Switzerland This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sun, Y.; Bochmann, F.; Morfeld, P.; Ulm, K.; Liu, Y.; Wang, H.; Yang, L.; Chen, W. Change of Exposure Response over Time and Long-Term Risk of Silicosis among a Cohort of Chinese Pottery Workers. Int. J. Environ. Res. Public Health 2011, 8, 2923-2936. https://doi.org/10.3390/ijerph8072923
Sun Y, Bochmann F, Morfeld P, Ulm K, Liu Y, Wang H, Yang L, Chen W. Change of Exposure Response over Time and Long-Term Risk of Silicosis among a Cohort of Chinese Pottery Workers. International Journal of Environmental Research and Public Health. 2011; 8(7):2923-2936. https://doi.org/10.3390/ijerph8072923
Chicago/Turabian StyleSun, Yi, Frank Bochmann, Peter Morfeld, Kurt Ulm, Yuewei Liu, Heijiao Wang, Lei Yang, and Weihong Chen. 2011. "Change of Exposure Response over Time and Long-Term Risk of Silicosis among a Cohort of Chinese Pottery Workers" International Journal of Environmental Research and Public Health 8, no. 7: 2923-2936. https://doi.org/10.3390/ijerph8072923
APA StyleSun, Y., Bochmann, F., Morfeld, P., Ulm, K., Liu, Y., Wang, H., Yang, L., & Chen, W. (2011). Change of Exposure Response over Time and Long-Term Risk of Silicosis among a Cohort of Chinese Pottery Workers. International Journal of Environmental Research and Public Health, 8(7), 2923-2936. https://doi.org/10.3390/ijerph8072923