Obesity, Physical Activity and Sedentary Behavior Amongst British and Saudi Youth: A Cross-Cultural Study


Abstract
:1. Introduction
2. Methods
2.1. Locations
2.2. Participants
2.3. Lifestyle Questionnaire
2.4. BMI Measurement
2.5. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| Variable | Al-Ahsa | Birmingham | Coventry | |||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| N | 600 | 538 | 308 | 329 | 277 | 238 |
| Age (yrs) | 16.60 ± 0.60 | 16.51 ± 0.67 | 15.59 ± 0.75 | 15.55 ± 0.74 | 15.32 ± 0.57 | 15.22 ± 0.46 |
| Weight (kg) | 67.46 ± 20.49 | 58.02 ± 17.61 | 65.68 ± 12.71 | 59.09 ± 11.98 | 62.96 ± 15.09 | 55.55 ± 10.32 |
| Height (cm) | 167.68 ± 6.81 | 154.89 ± 5.42 | 171.52 ± 7.97 | 161.93 ± 6.96 | 171.77 ± 8.53 | 161.08 ± 7.04 |
| BMI (kg/m2) | 23.90 ± 6.75 | 24.14 ± 7.09 | 22.26 ± 3.70 | 22.50 ± 4.12 | 21.38± 4.89 | 21.46 ± 3.38 |
| Time spent on TV (hrs/day) | 2.51 ± 1.81 | 2.61 ± 1.91 | 2.67 ± 1.73 | 2.81 ± 1.72 | 2.72 ± 1.72 | 2.88 ± 1.63 |
| Time spent on computer (hrs/day) | 2.48 ± 2.07 | 3.18 ± 2.40 | 2.55 ± 1.70 | 2.84 ± 1.73 | 2.79 ± 1.88 | 2.95 ± 1.88 |
| Sedentary activity (hrs/day) (TV+computer) | 4.99 ± 3.02 | 5.78 ± 2.57 | 5.22 ± 2.82 | 5.65 ± 2.66 | 5.50 ± 2.74 | 5.87 ± 2.81 |
| Total METs-min/week (vigorous) | 1759 ± 2042 | 129 ± 244 | 3268 ± 2547 | 1172 ± 1315 | 3531 ± 2691 | 1488 ± 1610 |
| Total METs-min/week (moderate) | 692 ± 782 | 570 ± 503 | 1478 ± 1010 | 1452 ± 1053 | 1309 ± 919 | 1488 ± 1020 |
| Total METs-min/week | 2337 ± 2323 | 565 ± 630 | 4710 ± 2950 | 2617 ± 1883 | 4804 ± 3048 | 2968 ±2 178 |
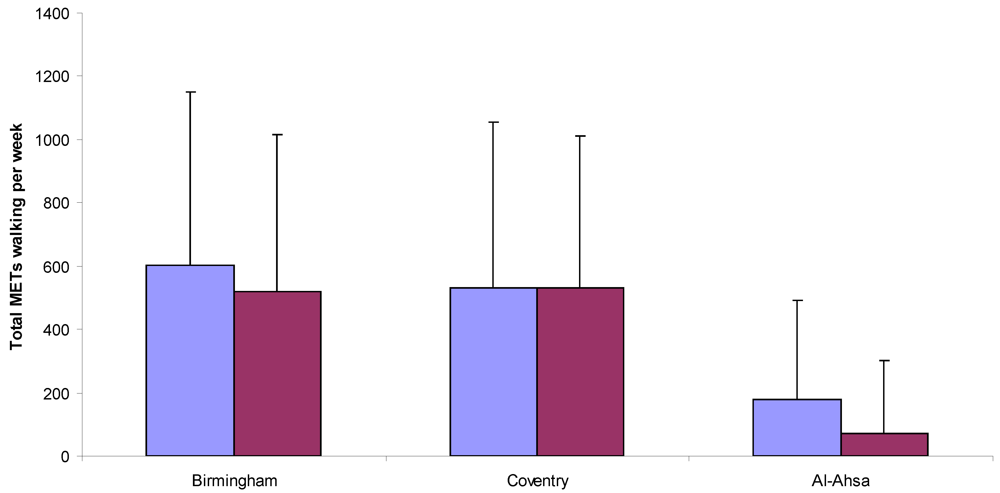
3.1. Differences in Physical Activity Levels
| City | Gender | N | Physical Activity Index (METs-min/week) | ||
|---|---|---|---|---|---|
| Inactive | Minimally Active | Active | |||
| Birmingham | Males | 308 | 6.5% | 11.7% | 81.8% |
| Females | 328 | 13.7% | 22.9% | 63.4% | |
| Total | 636 | 10.2% | 17.5% | 72.3% | |
| Coventry | Males | 277 | 6.5% | 10.1% | 83.4% |
| Females | 237 | 11% | 19% | 70% | |
| Total | 514 | 8.6% | 14.2% | 77.2% | |
| Al-Ahsa | Males | 576 | 34.5% | 19.6% | 45.8% |
| Females | 531 | 81.4% | 14.1% | 4.5% | |
| Total | 1,107 | 57 % | 17% | 26% | |


3.2. Differences in Sedentary Behavior—(TV Viewing + Computer Usage)
3.3. Differences in BMI Classifications
| City | Gender | N | Body Mass Index (kg/m2) | |||
|---|---|---|---|---|---|---|
| Normal | Overweight | Obese | Overweight/obese | |||
| Birmingham | Males | 308 | 73.4% | 20.5% | 6.1% | 26.6% |
| Females | 329 | 73.3% | 19.5% | 7.2% | 26.7% | |
| Total | 637 | 73.3% | 19.9% | 6.8% | 26.7% | |
| Coventry | Males | 264 | 78.5% | 14.4% | 6.1% | 20.5% |
| Females | 197 | 82.2% | 14.7% | 3% | 17.8% | |
| Total | 461 | 80.7% | 14.5% | 4.8% | 19.3% | |
| Al-Ahsa | Males | 580 | 63.6% | 16.9% | 19.5% | 36.4% |
| Females | 538 | 63.4% | 19.5% | 17.1% | 36.6% | |
| Total | 1,118 | 63.5% | 18.2% | 18.3% | 36.5% | |
3.4. Associations Between Physical Activity, Sedentary Behavior and BMI
4. Discussion
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Department of HealthPhysical ActivityHealth Improvement and ProtectionAt Least Five a Week: Evidence on the Impact of Physical Activity and Its Relationship to Health. A Report from the Chief Medical Officer; Department of Health: London, UK, 2004.
- The Sedentary Behaviour & Obesity Expert Working Group, Sedentary Behaviour and Obesity: Review of the Current Scientific Evidence; Department of Health: London, UK, 2010.
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W., III. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar]
- World Health Organization, Global Recommendations on Physical Activity for Health; WHO Press: Geneva, Switzerland, 2010.
- Department of HealthPhysical ActivityHealth Improvement and ProtectionStart Active, Stay Active: A Report on Physical Activity from the Four Home Countries’ Chief Medical Officers; Department of Health: London, UK, 2011.
- Kesaniemi, A.; Riddoch, C.J.; Reeder, B.; Blair, S.N.; Sorensen, T.I.A. Advancing the future of physical activity guidelines in Canada: An independent expert panel interpretation of the evidence. Int. J. Behav. Nutr. Phys. Act. 2010, 7. [Google Scholar]
- U.S. Department of Health & Human Services, Physical Activity Guidelines for Americans; U.S. Department of Health & Human Services: Hatsville, MD, USA, 2008.
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.I.; Gortmaker, S.I. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar]
- Sassi, F.; Devaux, M.; Cecchini, M.; Rusticelli, E. The Obesity Epidemic: Analysis of Past and Projected Future Trends in Selected OECD Countries; Organisation for Economic Co-operation and Development (OECD), Directorate for Employment, Labour and Social Affairs, Health Committee: Paris, France, 2009. [Google Scholar]
- WHO, Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2005.
- Finucane, M.M.; Stevens, G.A.; Cowan, M.J.; Danaei, G.; Lin, J.K.; Paciorek, C.J.; Singh, G.M.; Gutierrez, H.R.; Lu, Y.; Bahalim, A.N.; et al. National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 2011, 377, 557–567. [Google Scholar]
- Lobstein, T.; Leach, R. Tackling Obesities: Future Choices—International Comparisons of Obesity Trends, Determinants and Responses—Evidence Review; Government Office for Science: London, UK, 2007. [Google Scholar]
- Al-Hazzaa, H.M.; Musaiger, A.O. Physical activity patterns and eating habits of adolescents living in major Arab cities. The Arab Teens Lifestyle Study. Saudi Med. J. 2010, 31, 210–211. [Google Scholar]
- WHO, The World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002.
- Physical Activity Guidelines Advisory Committee, Physical Activity Guidelines Advisory Committee Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2008.
- Ekelund, U.; Anderssen, S.A.; Froberg, K.; Sardinha, L.B.; Andersen, L.B.; Brage, S. European Youth Heart Study Group. Independent associations of physical activity and cardiorespiratory fitness with metabolic risk factors in children: The European Youth Heart Study. Diabetologia 2007, 50, 1832–1840. [Google Scholar] [CrossRef] [Green Version]
- Sedentary Behaviour and Obesity Expert Working Group, Sedentary Behaviour and Obesity: Review of the Current Scientific Evidence; Department of Health: London, UK, 2010.
- Chief Medical Officer, At Least Five A Week: Evidence on the Impact of Physical Activity and Its Relationship to Health; Department of Health: London, UK, 2004.
- Reilly, J.J. Tackling the obesity epidemic: New approaches. Arch. Dis. Child. 2006, 91, 724–726. [Google Scholar]
- Gardner, D.S.L.; Hosking, J.; Metcalf, B.S. Contribution of early weight gain to childhood overweight and metabolic health. Pediatrics 2009, 123, e67–e73. [Google Scholar]
- Reilly, J.J.; Okely, A.D.; Almond, L.; Cardon, G.; Prosser, L.; Hubbard, J. Making the Case for UK Physical Activity Guidelines for Early Years: Recommendations and Draft Summary Statements based on the Current Evidence; Working Paper; Department of Health: London, UK, 2010. [Google Scholar]
- Al-Nozha, M.M.; Al-Hazzaa, H.M.; Arafah, M.R.; Al-Khadra, A.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Khan, N.B.; Al-Marzouki, K.; Al-Harthi, S.S.; Abdullah, M.; Al-Shahid, M.S. Prevalence of physical activity and inactivity among Saudis aged 30–70 years: Population-based cross-sectional study. Saudi Med. J. 2007, 28, 559–568. [Google Scholar]
- Al-Hazzaa, H. Prevalence of physical inactivity in Saudi Arabia: A brief review. East. Med. Health J. 2004, 10, 663–670. [Google Scholar]
- James, P.T. Obesity: The worldwide epidemic. Clin. Dermatol. 2004, 22, 276–280. [Google Scholar]
- El Mouzan, M.I.; Foster, P.J.; Al Herbish, A.S.; Al Salloum, A.A.; Al Omer, A.A.; Qurachi, M.M.; Kecojevic, T. Prevalence of overweight and obesity in Saudi children and adolescents. Ann. Saudi Med. 2010, 30, 203–208. [Google Scholar]
- Office of National Statistics, Local Area Statistics: Birmingham; Office of National Statistics: London, UK, 2011.
- Office of National Statistics, Local Area Statistics: Coventry; Office of National Statistics: London, UK, 2011.
- Central Department of Statistics and Information, Demographic Research Bulletin 2004; Central Department of Statistics and Information: Riyadh, Saudi Arabia, 2005.
- Al-Hazzaa, H.; Al-Ahmadi, M. A self-reported questionnaire for the assessment of physical activity in youth 15-25 years: Development, reliability and construct validity. Arab J. Food Nutr. 2003, 4, 279–291. [Google Scholar]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Musaiger, A.O. Convergent validity of the Arab Teens Lifestyle Study (ATLS) physical activity questionnaire. Int. J. Environ. Res. Pub. Health 2011, 8, 3810–3820. [Google Scholar]
- Del Greco, L.; Walop, W.; Eastridge, L. Questionnaire development: 3. Translation. Can. Med. Assoc. J. 1987, 136, 817–818. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O'Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O.; Jacobs, D.R.; Leon, A.S. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sport Exerc. 2000, 32, s498–s516. [Google Scholar]
- Ridley, K.; Ainsworth, B.E.; Olds, T.S. Development of a compendium of energy expenditures for youth. Int. J. Behav. Nutr. Phy. Act. 2008, 5, 1–8. [Google Scholar]
- Bauman, A.; Bull, F.; Chey, T.; Craig, C.L.; Ainsworth, B.E.; Sallis, J.F.; Bowles, H.R.; Hagstromer, M.; Sjostrom, M.; Pratt, M. The international prevalence study on physical activity: Results from 20 countries. Int. J. Behav. Nutr. Phy. Act. 2009, 6. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br. Med. J. 2000, 320, 1240–1243. [Google Scholar]
- IBM SPSS Statistics 19 Core System User’s Guide. 2010 SPSS Inc., Chicago, IL.
- Jones, A.P.; Bentham, G.; Foster, C.; Hillsdon, M.; Panter, J. Tackling Obesities: Future Choices—Obesogenic Environment—Evidence Review; Government Office for Science: London, UK, 2007. [Google Scholar]
- Al-Hazzaa, H. The public health burden of physical inactivity in Saudi Arabia. J. Fam. Comm. Med. 2004, 11, 45–51. [Google Scholar]
- Al-Hazzaa, H. Rising trends in BMI of Saudi adolescents: Evidence from three national cross sectional studies. Asia Pac. J. Clin. Nutr. 2007, 16, 462–466. [Google Scholar]
- Coventry City Council, State of the City 2011; Coventry City Council: Coventry, UK, 2011.
- Saelens, B.E.; Sallis, J.F.; Frank, D. Environmental correlates of walking and cycling: Findings from the transportation, urban design and planning literature. Ann. Behav. Med. 2003, 25, 80–91. [Google Scholar]
- Van Dyck, D.; Cardon, G.; Deforche, B.; Owen, N.; de Bourdeaudhuij, I. Relationships between neighbourhood walkability and adults’ physical activity: How important is residential self-selection? Health Place 2011, 17, 1011–1014. [Google Scholar] [CrossRef]
- Amin, T.T.; Al-Sultan, A.I.; Ali, A. Overweight and obesity and their relation to dietary habits and socio-demographic characteristics among male primary school children in Al-Ahsa, Kingdom of Saudi Arabia. Eur. J. Nutr. 2008, 47, 310–318. [Google Scholar]
- Al-Nuaim, A.R.; Al-Mazrou, Y.; Al-Rubean, K.; Al-Attas, O.; Khoja, T.; Al-Daghari, N. National Chronic Metabolic Diseases Survey Part II. The Prevalence at National and Regional level. The Sociodemographic, Clinical and Chemical Characteristics, in-Depth Analysis; Ministry of Health and King Saud University: Riyadh, Saudi Arabia, 1997. [Google Scholar]
- Al Qauhiz, N.M. Obesity among Saudi female university students: Dietary habits and health behaviours. J. Egypt Public Health Assoc. 2010, 85, 45–59. [Google Scholar]
- Alhyas, L.; McKay, A.; Balasanthiran, A.; Majeed, A. Prevalences of overweight, obesity, hyperglycaemia, hypertension and dyslipidaemia in the Gulf: Systematic review. J. Roy. Soc. Med. 2011, 2. [Google Scholar]
- Wang, F.; Lobstein, T. Worldwide trends in childhood overweight and obesity. Int. J. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar]
- Adamo, K.B.; Onywera, V.O.; Sheel, A.W.; Boit, M.; Waudo, J.; Tremblay, M. Child obesity and fitness levels among Kenyan and Canadian children from urban and rural environments: A KIDS-CAN Research Alliance Study. Int. J. Pediatr. Obes. 2011, 6, e225–e232. [Google Scholar]
- Washi, S.A.; Ageib, M.B. Poor diet quality and food habits are related to impaired nutritional status in 13- to 18-year-old adolescents in Jeddah. Nutr. Res. 2010, 30, 527–534. [Google Scholar]
- Gillis, L.J.; Bar-Or, O. Food away from home, sugar-sweetened drink consumption and juvenile obesity. J. Am. Coll. Nutr. 2003, 22, 539–545. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Al-Nakeeb, Y.; Lyons, M.; Collins, P.; Al-Nuaim, A.; Al-Hazzaa, H.; Duncan, M.J.; Nevill, A. Obesity, Physical Activity and Sedentary Behavior Amongst British and Saudi Youth: A Cross-Cultural Study. Int. J. Environ. Res. Public Health 2012, 9, 1490-1506. https://doi.org/10.3390/ijerph9041490
Al-Nakeeb Y, Lyons M, Collins P, Al-Nuaim A, Al-Hazzaa H, Duncan MJ, Nevill A. Obesity, Physical Activity and Sedentary Behavior Amongst British and Saudi Youth: A Cross-Cultural Study. International Journal of Environmental Research and Public Health. 2012; 9(4):1490-1506. https://doi.org/10.3390/ijerph9041490
Chicago/Turabian StyleAl-Nakeeb, Yahya, Mark Lyons, Peter Collins, Anwar Al-Nuaim, Hazzaa Al-Hazzaa, Michael J. Duncan, and Alan Nevill. 2012. "Obesity, Physical Activity and Sedentary Behavior Amongst British and Saudi Youth: A Cross-Cultural Study" International Journal of Environmental Research and Public Health 9, no. 4: 1490-1506. https://doi.org/10.3390/ijerph9041490
APA StyleAl-Nakeeb, Y., Lyons, M., Collins, P., Al-Nuaim, A., Al-Hazzaa, H., Duncan, M. J., & Nevill, A. (2012). Obesity, Physical Activity and Sedentary Behavior Amongst British and Saudi Youth: A Cross-Cultural Study. International Journal of Environmental Research and Public Health, 9(4), 1490-1506. https://doi.org/10.3390/ijerph9041490