
Certificate of Need Laws and Health Care Use during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Mortality
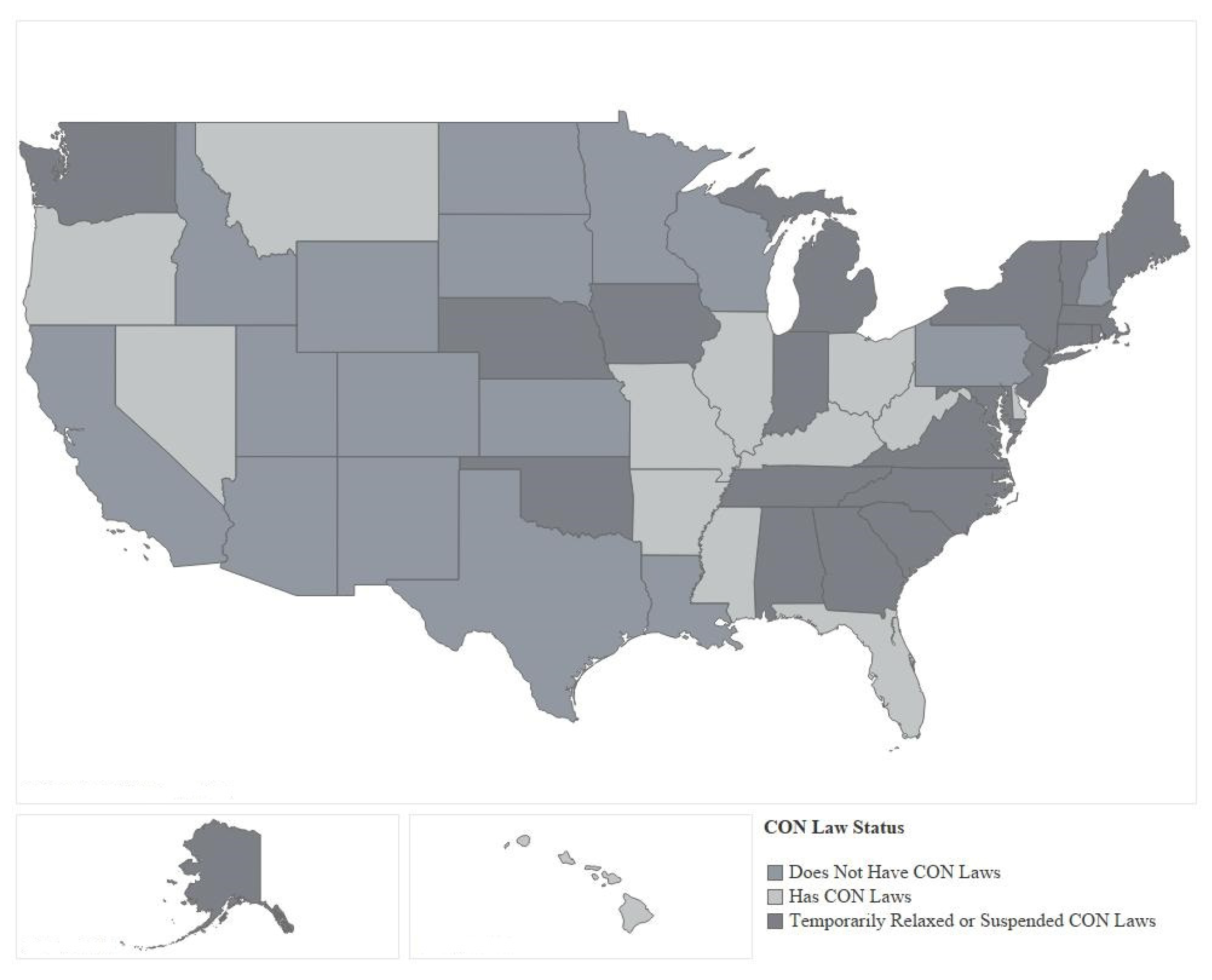
2.2. Certificate of Need Laws
2.3. Hospital Utilization
2.4. Model
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bailey, James. 2018a. The Effect of Certificate of Need Laws on All-Cause Mortality. Health Services Research 53: 49–62. [Google Scholar] [CrossRef] [PubMed]
- Bailey, James. 2018b. Does “Excess Supply” Drive Excessive Health Spending? The Case of Certificate-of-Need Laws. The Journal of Private Enterprise 33: 91–109. [Google Scholar]
- Bailey, James. 2019. Can Health Spending be Reined in Through Supply Restraints? An Evaluation of Certificate-of-Need Laws. Journal of Public Health 27: 7755–60. [Google Scholar] [CrossRef]
- Bayne, Ethan, Conor Norris, and Edward Timmons. 2020. A Primer on Emergency Occupational Licensing Reforms for Combating COVID-19. Arlington: Mercatus Policy Brief, Mercatus Center at George Mason University, March 26. [Google Scholar]
- Chiu, Kevin. 2021. The Impact of Certificate of Need Laws on Heart Attack Mortality: Evidence from County Borders. Journal of Health Economics 79: 1–17. [Google Scholar] [CrossRef]
- Conover, Christopher, and Frank Sloan. 1998. Does Removing Certificate of Need Regulations Lead to a Surge in Health Care Spending? Journal of Health Politics: Policy and Law 23: 455–81. [Google Scholar] [CrossRef]
- Conover, Christopher, and James Bailey. 2020. Certificate of Need Laws: A Systematic Review and Cost-Effectiveness Analysis. BMC Health Services Research 20: 748. [Google Scholar] [CrossRef]
- Cutler, David, Robert Huckman, and Jonathan Kolstad. 2010. Input Constraints and the Efficiency of Entry: Lessons from Cardiac Surgery. American Economic Journal: Economic Policy 2: 51–76. [Google Scholar] [CrossRef]
- DeLia, Derek, Joel Cantor, Amy Tiedemann, and Cecilia Huang. 2009. Effects of Regulation and Competition on Health Care Disparities: The Case of Cardiac Angiography in New Jersey. Journal of Health Politics: Policy and Law 34: 63–91. [Google Scholar] [CrossRef]
- DiSesa, Verdi J., Sean M. O’Brien, Karl F. Welke, Sarah M. Beland, Constance K. Haan, Mary S. Vaughan-Sarrazin, and Eric D. Peterson. 2006. Contemporary Impact of State Certificate of Need Regulations for Cardiac Surgery: An Analysis Using the Society of Thoracic Surgeon’s National Cardiac Surgery Database. Circulation 111: 2122–29. [Google Scholar] [CrossRef] [Green Version]
- Ettner, Susan, Jacqueline Zinn, Haiyong Xu, Heather Ladd, Eugene Nuccio, Dara Sorkin, and Dana Mukamel. 2020. Certificate of Need and the Cost of Competition in Home Healthcare Markets. Home Health Care Services Quarterly 39: 51–64. [Google Scholar] [CrossRef]
- Farzanegan, Mohammad. 2020. Ageing Society and SARS-CoV-2 Mortality: Does Healthcare Absorptive Capacity Matter? Journal of Risk and Financial Management 13: 277. [Google Scholar] [CrossRef]
- Ford, Jon, and David Kaserman. 1993. Certificate of Need Regulation and Entry: Evidence from the Dialysis Industry. Southern Economic Journal 59: 783–91. [Google Scholar] [CrossRef]
- Gungoraydinoglu, Ali, Illke Ӧztekin, and Ӧzde Ӧztekin. 2021. The Impact of COVID-19 and Its Policy Responses on Local Economy and Health Conditions. Journal of Risk and Financial Management 14: 233. [Google Scholar] [CrossRef]
- Haeffele, Stefanie, Anne Hobson, and Virgil Storr. 2020. Coming Back from COVID-19: Lessons in Entrepreneurship from Disaster Recovery Research. Arlington: Mercatus Policy Brief, Mercatus Center at George Mason University, April 29. [Google Scholar]
- Ho, Vivian. 2006. Does Certificate of Need Affect Cardiac Outcomes and Costs? International Journal of Health Care Finance & Economics 6: 300–24. [Google Scholar]
- Ho, Vivian, Meei-Hsiang Ku-Goto, and James Jollis. 2009. Certificate of Need (CON) for Cardiac Care: Controversy Over the Contributions of CON. Health Services Research 44, Pt 1: 483–500. [Google Scholar] [CrossRef]
- Messa, Indu, Robert Meeker, and Suresh Mukherji. 2012. Certificate of Need. Neuroimaging Clinics of North America 22: 443–50. [Google Scholar] [CrossRef]
- Meyers, Molly, and Kathleen Sheehan. 2020. The Impact of Certificate of Need Laws on Emergency Department Wait Times. The Journal of Private Enterprise 35: 59–75. [Google Scholar]
- Mitchell, Matthew. 2016. Do Certificate of Need Laws Limit Spending? Arlington: Mercatus Policy Brief, Mercatus Center at George Mason University, September 29. [Google Scholar]
- Mitchell, Matthew. 2020. First, Do No Harm: Three Ways that Policymakers Can Make It Easier for Healthcare. Arlington: Mercatus Policy Brief, Mercatus Center at George Mason University, March 26. [Google Scholar]
- Mitchell, Matthew, Elise Amez-Droz, and Anna Parsons. 2020. Phasing Out Certificate of Need Laws: A Menu of Options. Arlington: Mercatus Policy Brief, Mercatus Center at George Mason University, February 25. [Google Scholar]
- Popescu, Ioana, Mary Vaughan-Sarrazin, and Gary Rosenthal. 2006. Certificate of Need Regulations Do Not Restrict Access to Coronary Revascularization after Acute Myocardial Infarction. JAMA 295: 2141–47. [Google Scholar] [CrossRef] [Green Version]
- Rivers, Patrick, Myron Fottler, and Mustafa Younis. 2007. Does Certificate of Need Really Contain Hospital Costs in the United States? Health Education Journal 66: 229–44. [Google Scholar] [CrossRef]
- Robinson, Jamie, David Nash, Elizabeth Moxey, and John O’Connor. 2001. Certificate of Need and the Quality of Cardiac Surgery. American Journal of Medical Quality 16: 155–60. [Google Scholar] [CrossRef]
- Rosko, Michael, and Ryan Mutter. 2014. The Association of Hospital Cost-Inefficiency with Certificate-of-Need Regulation. Medical Care Research and Review 71: 280–98. [Google Scholar] [CrossRef] [PubMed]
- Schultz, Olivia, Lewis Shi, and Michael Lee. 2021. Assessing the Efficacy of Certificate of Need Laws Through Total Joint Arthroplasty. Journal for Healthcare Quality 43: E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Stratmann, Thomas, and Christopher Koopman. 2018. Entry Regulation and Rural Health Care: Certificate of Need Laws, Ambulatory Surgical Centers, and Community Hospitals, Mercatus Working Paper. Arlington: Mercatus Center at George Mason University, February 18. [Google Scholar]
- Stratmann, Thomas, and David Wille. 2016. Certificate of Need Laws and Hospital Quality, Mercatus Working Paper. Arlington: Mercatus Center at George Mason University, September 27. [Google Scholar]
- Stratmann, Thomas, and Jake Russ. 2014. Do Certificate of Need Laws Increase Indigent Care? Arlington: Mercatus Policy Brief, Mercatus Center at George Mason University, July 15. [Google Scholar]
- Stratmann, Thomas, and Matthew Baker. 2016. Are Certificate of Need Laws Barriers to Entry? How They Affect Access to MRI, CT, and PET Scans. Mercatus Working Paper. Arlington: Mercatus Center at George Mason University, January 12. [Google Scholar]
- Vaughan-Sarrazin, Mary, Edward Hannan, Carol Gormley, and Gary Rosenthal. 2002. Mortality in Medicare Beneficiaries Following Coronary Artery Bypass Graft Surgery in States with and without Certificate of Need Regulation. JAMA 288: 1859–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Week 10 | |||||||
| Best Case Scenario: Deaths Per 100,000 | |||||||
| State Type | COVID-19 | Natural | Septicemia | Diabetes | Chronic Lower Respiratory Disease | Influenza and/or Pneumonia | Alzheimer’s Disease |
| Reformed CON Laws | 0.0251 | 16.2455 | 0.1949 | 0.3891 | 0.9062 | 0.3492 | 0.7062 |
| Always Had CON Laws | 0.0003 | 18.4625 | 0.1694 | 0.5418 | 1.2618 | 0.4187 | 0.6814 |
| Never Had CON Laws | 0.0023 | 16.3195 | 0.1488 | 0.4965 | 1.0835 | 0.3878 | 0.7207 |
| Week 22 | |||||||
| Best Case Scenario: Deaths Per 100,000 | |||||||
| State Type | COVID-19 | Natural | Septicemia | Diabetes | Chronic Lower Respiratory Disease | Influenza and/or Pneumonia | Alzheimer’s Disease |
| Reformed CON Laws | 0.8131 | 10.9827 | 0.0823 | 0.2467 | 0.4389 | 0.1115 | 0.3787 |
| Always Had CON Laws | 0.3530 | 9.6941 | 0.0394 | 0.2118 | 0.4267 | 0.0877 | 0.3615 |
| Never Had CON Laws | 0.5512 | 10.7314 | 0.0818 | 0.2898 | 0.5580 | 0.0792 | 0.4128 |
| State | Date | Legal Document |
|---|---|---|
| Alabama | 2 April 2020 | 5th Supplemental State of Emergency |
| Alaska | 11 March 2020 | Administrative Order No. 315 |
| Connecticut | 14 March 2020 | Executive Order No. 7B |
| Georgia | 20 March 2020 | Executive Order 3.20.20.2 |
| Indiana | 16 March 2020 | Executive Order 20-04 and Executive Order 20-05 |
| Iowa | 17 March 2020 | Proclamation of Disaster Emergency |
| Maine | 6 April 2020 | Executive Order No. 35 |
| Massachusetts | 24 March 2020 | Order of the Commissioner of Public Health Regarding Determination of Need Approvals Related to COVID-19 |
| Maryland | 3 April 2020 | Sec. 10.24.01.20 Emergency Certificate of Need. (Already established, MHCC Executive Director alerted hospitals of Emergency CON on 3 April) |
| Michigan | 17 March 2020 | Executive Order No. 2020-13 |
| Nebraska | 31 March 2020 | Executive Order No. 20-12 |
| New Jersey | 13 March 2020 | Executive Order No. 103; followed by the Temporary Operational Waivers during a State of Emergency from NJ Commissioner |
| New York | 23 March 2020 | Executive Order 202.10 |
| North Carolina | 12 March 2020 | Executive Order No. 116 (10 March); followed by NC DHHS memo to hospitals (12 March) |
| Oklahoma | 8 April 2020 | Executive Order No. 2020-13 |
| Rhode Island | 10 April 2020 | Executive Order No. 20-21 |
| South Carolina | 19 March 2020 | Executive Order No. 2020-11 |
| Tennessee | 19 March 2020 | Executive Order No. 15 |
| Vermont | 25 March 2020 | Executive Order No. 01-20; followed by GMCB Certificate of Need Bulletin 002 |
| Virginia | 12 March 2020 | Executive Order Amended Number 51 (2020) |
| Washington | 30 March 2020 | Proclamation 20-36 |
| Underlying Cause of Death | ||||||
|---|---|---|---|---|---|---|
| Natural Death | Septicemia | Diabetes | Chronic Lower Respiratory Disease | Influenza or Pneumonia | Alzheimer’s Disease | |
| Reform Trend | 0.0001 (0.0018) | −0.0001 (0.0001) | −0.0002 (0.0001) | −0.0002 (0.0001) | −0.0001 (0.0002) | −0.0001 (0.0002) |
| CON | 1.9719 *** (0.0000) | 0.0727 *** (0.0000) | 0.3716 *** (0.0000) | 0.2764 *** (0.0000) | 0.2022 *** (0.0000) | 0.8039 *** (0.0000) |
| Reform | 5.2513 *** (0.0089) | 0.2938 *** (0.0005) | 0.3128 *** (0.0006) | 0.6830 *** (0.0016) | 0.4461 *** (0.0009) | 0.8963 *** (0.0010) |
| Time Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes |
| State Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes |
| Standard Errors | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) |
| Obs. | 432 | 432 | 432 | 432 | 432 | 432 |
| R2 | 0.8978 | 0.7603 | 0.6658 | 0.6890 | 0.6715 | 0.6401 |
| Underlying Cause of Death | |||||||
|---|---|---|---|---|---|---|---|
| COVID-19 Death | Natural Death | Septicemia | Diabetes | Chronic Lower Respiratory Disease | Influenza or Pneumonia | Alzheimer’s Disease | |
| ReformCON∗Post | −0.3199 (0.8987) | −0.2382 (0.8987) | 0.0040 (0.0187) | −0.0070 (0.0469) | 0.0293 (0.0618) | −0.0143 (0.0370) | 0.0372 (0.0446) |
| Beds | 10.4329 *** (3.0566) | 18.9124 *** (5.2612) | −0.0464 (0.1183) | −0.4915 * (0.2536) | 0.7162 ** (0.3616) | 0.1031 (0.2082) | 0.3003 (0.2335) |
| CON∗Beds | 1.5541 (2.3519) | −6.9342 (5.0495) | 0.1910 * (0.1055) | −0.5667 ** (0.2592) | −0.0293 (0.0618) | 0.2082 (0.2587) | −0.2615 (0.2344) |
| Reform∗Beds | 15.0771 *** (2.5894) | 17.5832 *** (4.2993) | 0.2639 ** (0.1088) | 0.2016 (0.2170) | 0.0198 (0.3050) | 0.8753 *** (0.1879) | 0.5467 ** (0.2159) |
| ReformCON∗Post∗Beds | −19.6168 *** (1.2672) | −29.0114 *** (1.2592) | −0.2052 *** (0.0396) | −0.6635 *** (0.0945) | −0.5879 *** (0.1071) | −0.6718 *** (0.0638) | −0.7261 *** (0.2181) |
| Social-Distancing-Mandate Controls | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Time Trends | Quadratic | Quadratic | Quadratic | Quadratic | Quadratic | Quadratic | Quadratic |
| Time Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| State Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Standard Errors | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) |
| Observations | 936 | 936 | 936 | 936 | 936 | 936 | 936 |
| R2 | 0.77 | 0.77 | 0.69 | 0.60 | 0.70 | 0.64 | 0.61 |
| Underlying Cause of Death | |||||||
|---|---|---|---|---|---|---|---|
| COVID-19 Death | Natural Death | Septicemia | Diabetes | Chronic Lower Respiratory Disease | Influenza or Pneumonia | Alzheimer’s Disease | |
| ReformCON∗Post | −0.4196 (0.4677) | −0.4818 (0.8742) | −0.0040 (0.0185) | 0.0037 (0.0456) | 0.0119 (0.0608) | −0.0159 (0.0370) | 0.0375 (0.0440) |
| Beds | 3.6663 *** (1.2225) | 6.6828 *** (1.9590) | −0.0226 (0.0449) | 0.1842 (0.0890) | −0.2448 * (0.1334) | 0.0325 (0.0812) | 0.1218 (0.0872) |
| CON∗Beds | −0.1229 (1.1398) | −4.0593 * (2.2129) | 0.0671 * (0.0398) | −0.2125 ** (0.0923) | −0.3628 ** (0.1543) | 0.0580 (0.0959) | −0.1031 (0.0865) |
| Reform∗Beds | 8.6279 *** (1.0430) | 10.8012 *** (1.5802) | 0.1293 *** (0.0409) | 0.1515 ** (0.0742) | 0.0732 (0.1111) | 0.4372 *** (0.0739) | 0.2908 *** (0.0832) |
| ReformCON∗Post∗Beds | −10.0872 *** (0.6176) | −14.6622 *** (0.7137) | −0.1048 *** (0.0197) | −0.3188 *** (0.0385) | −0.2806 *** (0.0411) | −0.3585 *** (0.0299) | −0.3725 *** (0.0824) |
| Social-Distancing-Mandate Controls | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Time Trends | Quadratic | Quadratic | Quadratic | Quadratic | Quadratic | Quadratic | Quadratic |
| Time Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| State Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Standard Errors | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) | Cluster (State) |
| Observations | 936 | 936 | 936 | 936 | 936 | 936 | 936 |
| R2 | 0.76 | 0.77 | 0.69 | 0.60 | 0.70 | 0.64 | 0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roy Choudhury, A.; Ghosh, S.; Plemmons, A. Certificate of Need Laws and Health Care Use during the COVID-19 Pandemic. J. Risk Financial Manag. 2022, 15, 76. https://doi.org/10.3390/jrfm15020076
Roy Choudhury A, Ghosh S, Plemmons A. Certificate of Need Laws and Health Care Use during the COVID-19 Pandemic. Journal of Risk and Financial Management. 2022; 15(2):76. https://doi.org/10.3390/jrfm15020076
Chicago/Turabian StyleRoy Choudhury, Agnitra, Sriparna Ghosh, and Alicia Plemmons. 2022. "Certificate of Need Laws and Health Care Use during the COVID-19 Pandemic" Journal of Risk and Financial Management 15, no. 2: 76. https://doi.org/10.3390/jrfm15020076
APA StyleRoy Choudhury, A., Ghosh, S., & Plemmons, A. (2022). Certificate of Need Laws and Health Care Use during the COVID-19 Pandemic. Journal of Risk and Financial Management, 15(2), 76. https://doi.org/10.3390/jrfm15020076