
A Novel Approach for Cognitive Clustering of Parkinsonisms through Affinity Propagation



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. MMSE Assessment
2.3. Statistical Analysis
2.3.1. Residuals Calculation
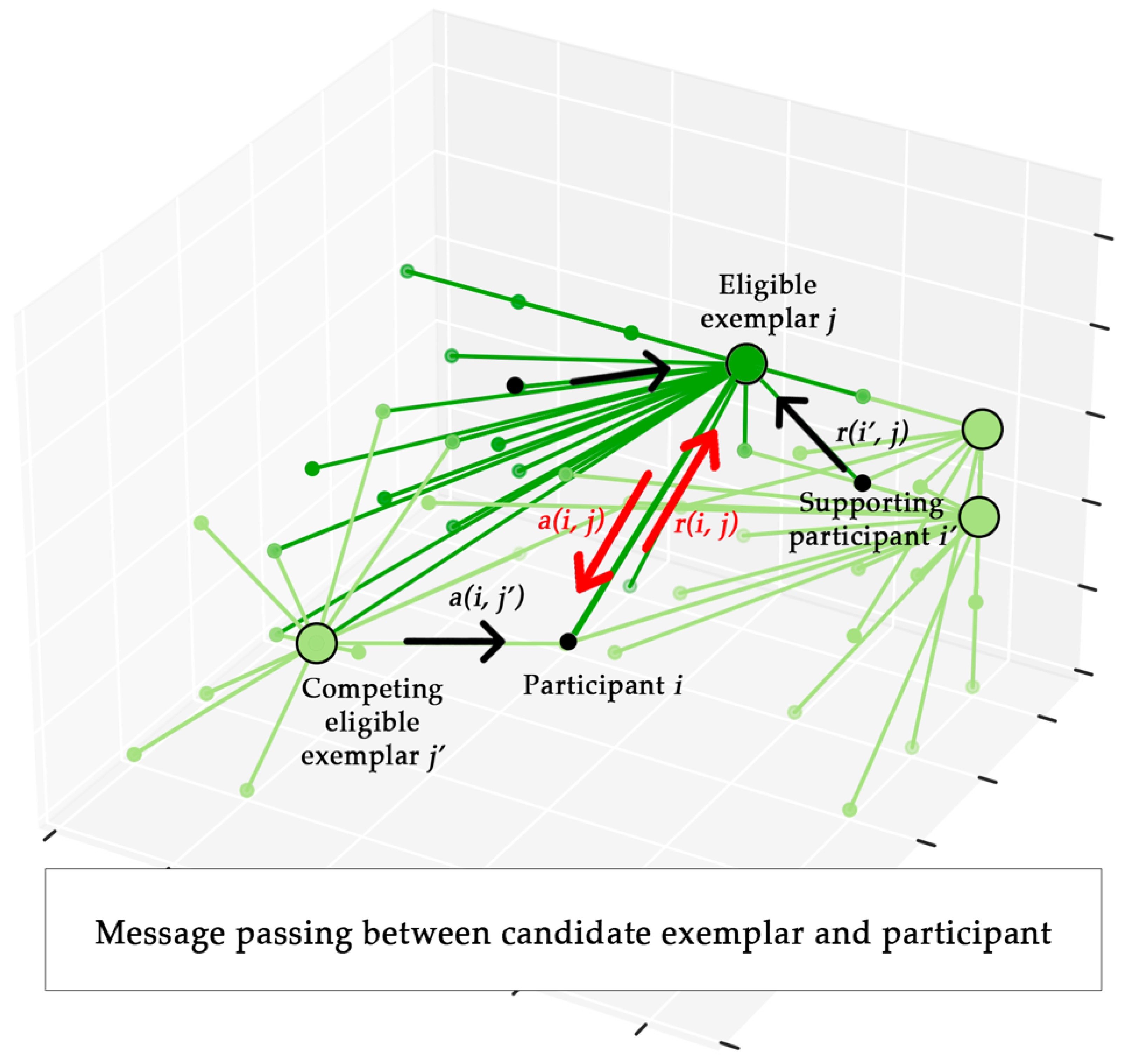
2.4. Affinity Propagation
| Algorithm 1 | Cognitive clustering of regression residuals trough Affinity Propagation |
| Input: | MMSE subscale scores matrix Y(n × m), covariates matrix X(k), damping factor d |
| Output: | Number of exemplars ex, cluster assignment vector ξ |
| 1: | initialization: E(n × m), matrix of regression residuals; S(n × n), matrix of similarities; p(n × 1), preference vector of Affinity Propagation; |
| 2: | forj = 1 to m do |
| 3: | fitj = ols(yj ~ x1 + … + xk); fitted model of the j-th column in Y, with x1, …, xk as the columns in X |
| 4: | for i = 1 to n−1 do |
| 5: | eij = yij—fitj.predict(yij); regression residual = the difference between yij and its prediction by fitj |
| 6: | fori = 1 to n do |
| 7: | for j = 1 to m do |
| 8: | for z = 1 to m do |
| 9: | sij = −; negative squared Euclidean distance between eiz and ejz |
| 10: | pi = Smin OR pi = Smedian |
| 11: | ap = AffinityPropagation(S, p, d); |
| 12: | ex = size(ap.exemplars); |
| 13: | ξ = ap.cluster_membership; |
2.5. Clustering Accuracy Assessment
3. Results
3.1. Statistical Analysis
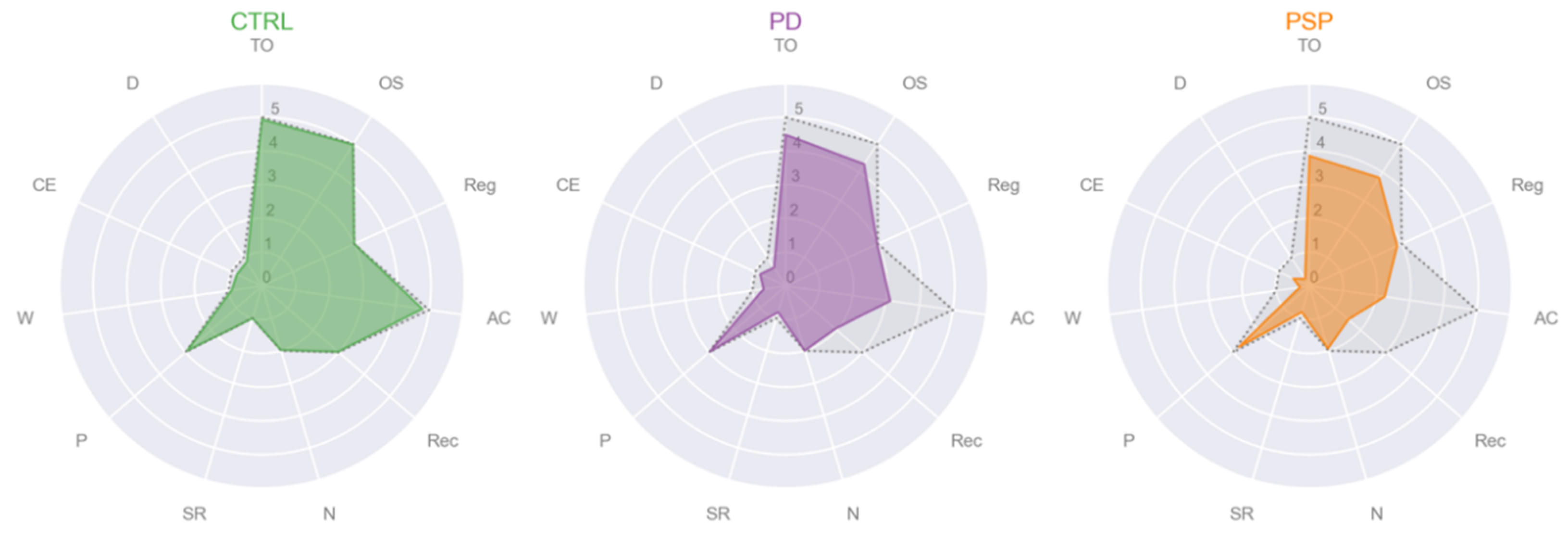
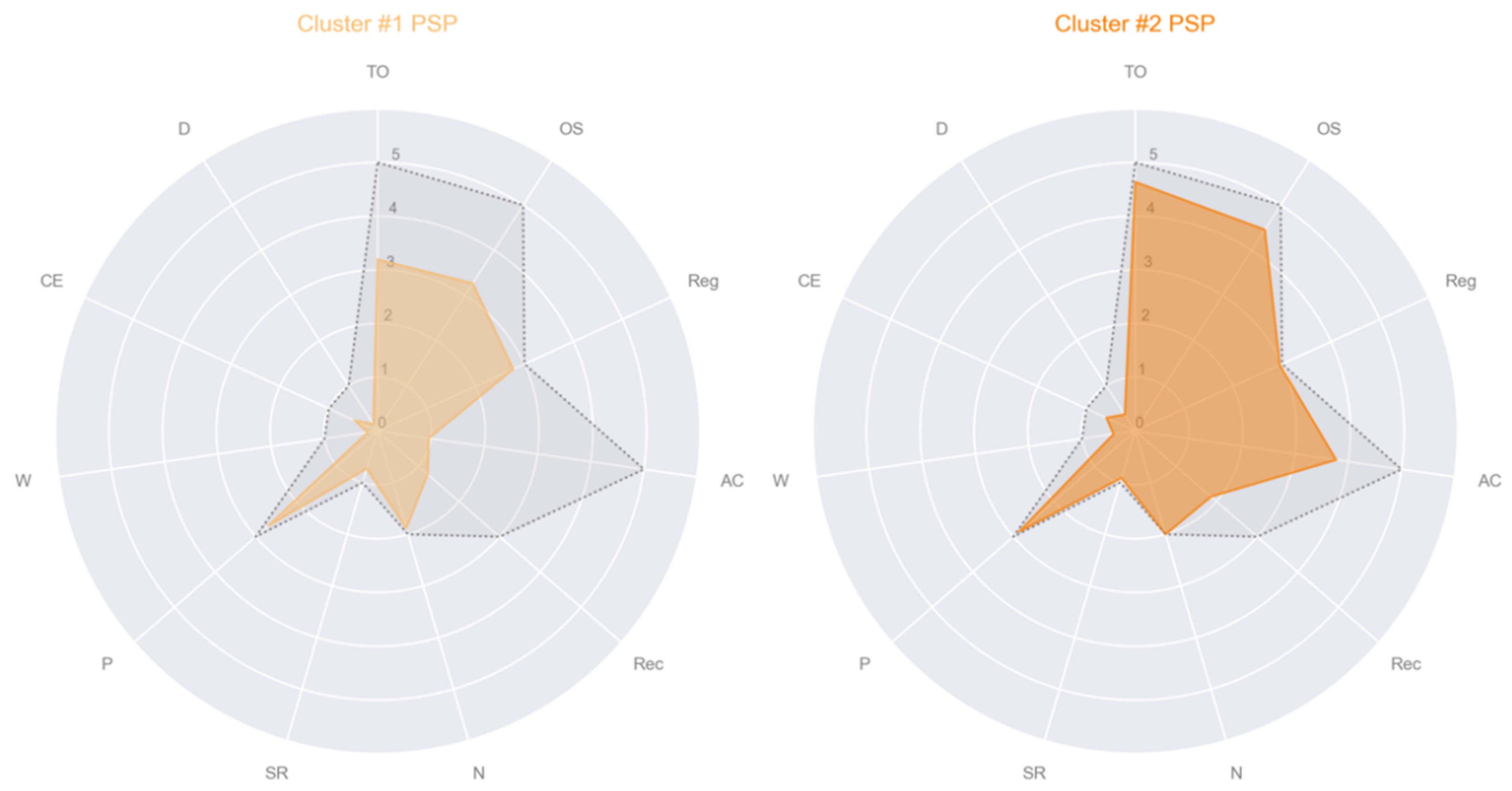
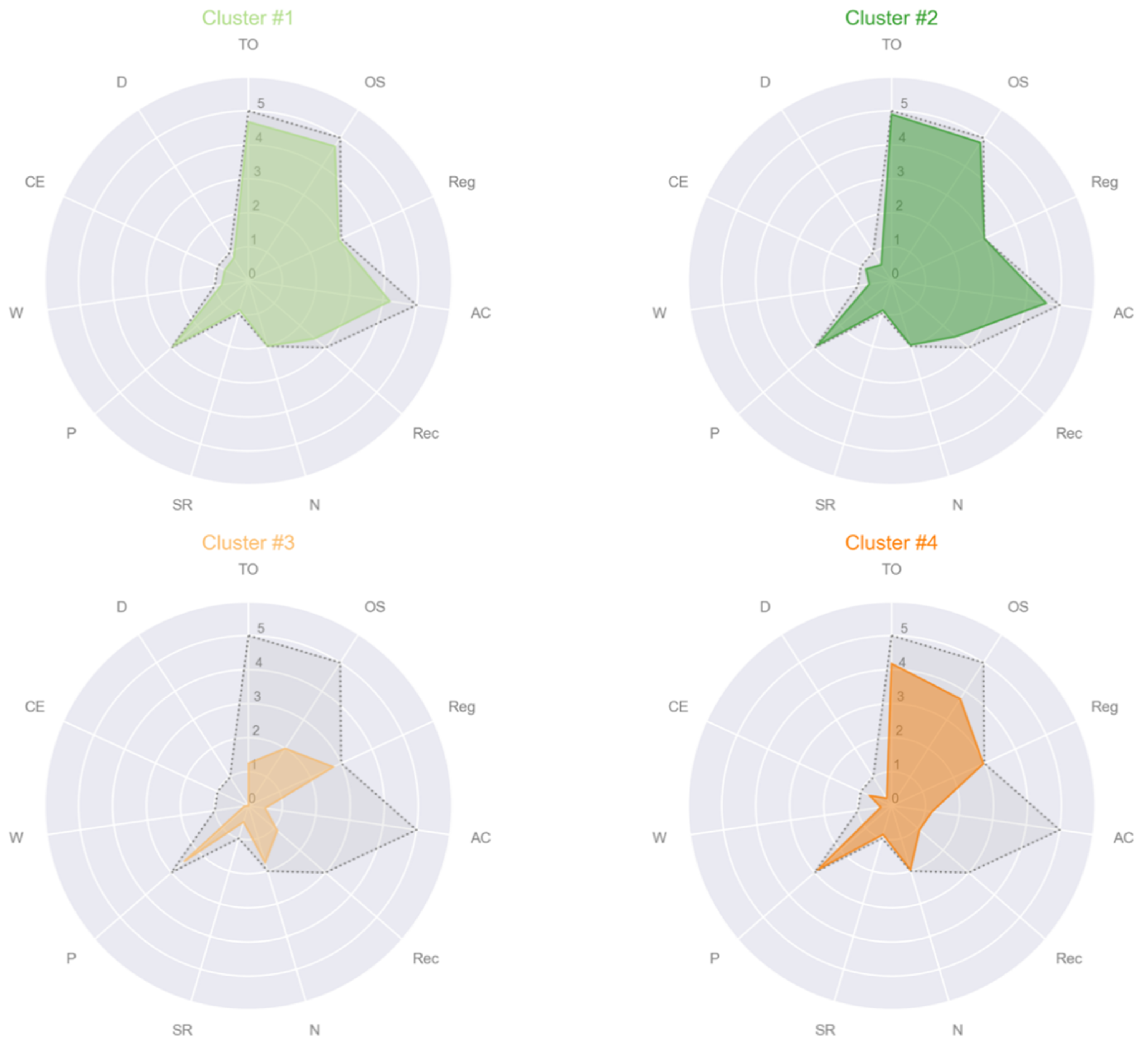
3.2. Cluster Analysis
- Cluster #1 CTRL: male, age 62, education 16, MMSE subscales = [5, 5, 3, 5, 3, 2, 1, 3, 1, 1, 1];
- Cluster #1 PD: male, age 43, education 13, MMSE subscales = [5, 5, 3, 4, 3, 2, 1, 3, 1, 1, 1];
- Cluster #2 PD: female, age 61, education 8, MMSE subscales = [5, 5, 3, 5, 3, 2, 1, 3, 1, 1, 1];
- Cluster #1 PSP: male, age 57, education 17, MMSE subscales = [5, 5, 3, 2, 1, 2, 1, 3, 0, 1, 0];
- Cluster #2 PSP: male, age 78, education 13, MMSE subscales = [5, 5, 3, 5, 2, 2, 1, 3, 0, 1, 0];
- Cluster #1: CTRL, female, age 59, education 16, MMSE subscales = [5, 5, 3, 5, 3, 2, 1, 3, 1, 1, 1];
- Cluster #2: PD, female, age 61, education 8, MMSE subscales = [5, 5, 3, 5, 3, 2, 1, 3, 1, 1, 1];
- Cluster #3: PD, female, age 70, education 5, MMSE subscales = [1, 2, 3, 1, 1, 2, 1, 3, 0, 0, 0];
- Cluster #4: PSP, male, age 78, education 8, MMSE subscales = [4, 4, 3, 1, 1, 2, 1, 3, 0, 1, 0].
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
 |
 |
 |
 |
 |
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| R2 | F | Intercept (β0, p-Value) | Age (β1, p-Value) | Sex (β2, p-Value) | Education (β3, p-Value) | |
|---|---|---|---|---|---|---|
| TO | 0.193 | 10.8 | 4.9218, <0.001 | −0.0162, 0.104 | −0.1011, 0.563 | 0.0739, <0.001 |
| OS | 0.309 | 20.3 | 4.0724, <0.001 | −0.0142, 0.110 | 0.1743, 0.264 | 0.0983, <0.001 |
| Reg | 0.074 | 3.6 | 3.0925, <0.001 | −0.0029, 0.331 | −0.0489, 0.344 | 0.0118, 0.039 |
| AC | 0.312 | 20.6 | 3.6018, 0.004 | −0.0267, 0.080 | −0.0646, 0.809 | 0.1675, <0.001 |
| Rec | 0.114 | 5.8 | 2.9579, <0.001 | −0.0159, 0.092 | −0.1284, 0.437 | 0.0426, 0.020 |
| N | 0.083 | 4.1 | 1.7130, <0.001 | 0.0010, 0.598 | 0.0586, 0.085 | 0.0106, 0.005 |
| SR | 0.022 | 1 | 0.7640, 0.004 | 0.0007, 0.821 | −0.0240, 0.674 | 0.0098, 0.119 |
| P | 0.071 | 3.4 | 3.1548, <0.001 | −0.0069, 0.089 | 0.0584, 0.410 | 0.0111, 0.153 |
| W | 0.252 | 15.3 | 1.2908, <0.001 | −0.0125, 0.003 | −0.0789, 0.278 | 0.0283, <0.001 |
| CE | 0.150 | 8 | 0.9553, 0.004 | −0.0054, 0.183 | −0.0788, 0.270 | 0.0253, 0.010 |
| D | 0.379 | 27.7 | 1.3470, <0.001 | −0.0180, <0.001 | 0.0741, 0.271 | 0.0321, <0.001 |
References
- Tryon, R.C. Cluster analysis. Edwards Brothers. Ann. Arbor Mich. 1939, 122. [Google Scholar]
- Le, N.Q.K.; Do, D.T.; Chiu, F.Y.; Yapp, E.K.Y.; Yeh, H.Y.; Chen, C.Y. XGBoost Improves Classification of MGMT Promoter Methylation Status in IDH1 Wildtype Glioblastoma. J. Pers. Med. 2020, 10, 128. [Google Scholar] [CrossRef]
- Ho Thanh Lam, L.; Le, N.H.; Van Tuan, L.; Tran Ban, H.; Nguyen Khanh Hung, T.; Nguyen, N.T.K.; Huu Dang, L.; Le, N.Q.K. Machine Learning Model for Identifying Antioxidant Proteins Using Features Calculated from Primary Sequences. Biology 2020, 9, 325. [Google Scholar] [CrossRef]
- Johnson, S.C. Hierarchical clustering schemes. Psychometrika 1967, 32, 241–254. [Google Scholar] [CrossRef]
- Ward, J.H., Jr. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Rao, M. Cluster analysis and mathematical programming. J. Am. Stat. Assoc. 1971, 66, 622–626. [Google Scholar] [CrossRef]
- Steinhaus, H. Sur la division des corp materiels en parties. Bull. Acad. Pol. Sci. 1956, 1, 801. [Google Scholar]
- Brusco, M.J.; Steinley, D.; Stevens, J.; Cradit, J.D. Affinity propagation: An exemplar-based tool for clustering in psychological research. Br. J. Math. Stat. Psychol. 2019, 72, 155–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, D.N.; Goldstein, G. Cluster Analysis in Neuropsychological Research; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Morris, R.; Blashfield, R.; Satz, P. Neuropsychology and cluster analysis: Potentials and problems. J. Clin. Exp. Neuropsychol. 1981, 3, 79–99. [Google Scholar] [CrossRef]
- Cotrena, C.; Damiani Branco, L.; Ponsoni, A.; Milman Shansis, F.; Paz Fonseca, R. Neuropsychological Clustering in Bipolar and Major Depressive Disorder. J. Int. Neuropsychol. Soc. 2017, 23, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Hermens, D.F.; Hodge, M.A.R.; Naismith, S.L.; Kaur, M.; Scott, E.; Hickie, I.B. Neuropsychological clustering highlights cognitive differences in young people presenting with depressive symptoms. J. Int. Neuropsychol. Soc. 2011, 17, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Burdick, K.; Russo, M.; Frangou, S.; Mahon, K.; Braga, R.; Shanahan, M.; Malhotra, A. Empirical evidence for discrete neurocognitive subgroups in bipolar disorder: Clinical implications. Psychol. Med. 2014, 44, 3083. [Google Scholar] [CrossRef] [Green Version]
- Lewandowski, K.; Sperry, S.; Cohen, B.; Öngür, D. Cognitive variability in psychotic disorders: A cross-diagnostic cluster analysis. Psychol. Med. 2014, 44, 3239. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Lim, T.S.; Lee, H.Y.; Moon, S.Y. Clustering mild cognitive impairment by mini-mental state examination. Neurol. Sci. 2014, 35, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.L.; Stage, E.C., Jr.; Lane, K.A.; Gao, S.; Risacher, S.L.; Goukasian, N.; Saykin, A.J.; Carrillo, M.C.; Dickerson, B.C.; Rabinovici, G.D.; et al. Neurodegenerative Patterns of Cognitive Clusters of Early-Onset Alzheimer’s Disease Subjects: Evidence for Disease Heterogeneity. Dement. Geriatr. Cogn. Disord. 2019, 48, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Alashwal, H.; El Halaby, M.; Crouse, J.J.; Abdalla, A.; Moustafa, A.A. The Application of Unsupervised Clustering Methods to Alzheimer’s disease. Front. Comput. Neurosci. 2019, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Van Rooden, S.M.; Heiser, W.J.; Kok, J.N.; Verbaan, D.; Van Hilten, J.J.; Marinus, J. The identification of Parkinson’s disease subtypes using cluster analysis: A systematic review. Mov. Disord. 2010, 25, 969–978. [Google Scholar] [CrossRef]
- Mu, J.; Chaudhuri, K.R.; Bielza, C.; de Pedro-Cuesta, J.; Larrañaga, P.; Martinez-Martin, P. Parkinson’s Disease Subtypes Identified from Cluster Analysis of Motor and Non-motor Symptoms. Front. Aging Neurosci. 2017, 9. [Google Scholar] [CrossRef]
- Liu, P.; Feng, T.; Wang, Y.-j.; Zhang, X.; Chen, B. Clinical heterogeneity in patients with early-stage Parkinson’s disease: A cluster analysis. J. Zhejiang Univ. Sci. B 2011, 12, 694. [Google Scholar] [CrossRef]
- van Rooden, S.M.; Colas, F.; Martinez-Martin, P.; Visser, M.; Verbaan, D.; Marinus, J.; Chaudhuri, R.K.; Kok, J.N.; van Hilten, J.J. Clinical subtypes of Parkinson’s disease. Mov. Disord. 2011, 26, 51–58. [Google Scholar] [CrossRef]
- Erro, R.; Vitale, C.; Amboni, M.; Picillo, M.; Moccia, M.; Longo, K.; Santangelo, G.; De Rosa, A.; Allocca, R.; Giordano, F.; et al. The heterogeneity of early Parkinson’s disease: A cluster analysis on newly diagnosed untreated patients. PLoS ONE 2013, 8, e70244. [Google Scholar] [CrossRef]
- Ma, L.Y.; Chan, P.; Gu, Z.Q.; Li, F.F.; Feng, T. Heterogeneity among patients with Parkinson’s disease: Cluster analysis and genetic association. J. Neurol. Sci. 2015, 351, 41–45. [Google Scholar] [CrossRef]
- Pont-Sunyer, C.; Hotter, A.; Gaig, C.; Seppi, K.; Compta, Y.; Katzenschlager, R.; Mas, N.; Hofeneder, D.; Brücke, T.; Bayés, A. The Onset of Nonmotor Symptoms in Parkinson’s disease (The ONSET PD S tudy). Mov. Disord. 2015, 30, 229–237. [Google Scholar] [CrossRef]
- Jin, X.; Han, J. K-Means Clustering; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Steinley, D.; Brusco, M.J. Evaluating mixture modeling for clustering: Recommendations and cautions. Psychol. Methods 2011, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Milligan, G.W.; Cooper, M.C. An examination of procedures for determining the number of clusters in a data set. Psychometrika 1985, 50, 159–179. [Google Scholar] [CrossRef]
- Frey, B.J.; Dueck, D. Clustering by passing messages between data points. Science 2007, 315, 972–976. [Google Scholar] [CrossRef] [Green Version]
- Mézard, M. Where are the exemplars? Science 2007, 315, 949–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thavikulwat, P. Affinity Propagation: A Clustering Algorithm for Computer-Assisted Business Simulations and Experiential Exercises. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.490.7628&rep=rep1&type=pdf (accessed on 3 February 2021).
- Hoglinger, G.U.; Respondek, G.; Stamelou, M.; Kurz, C.; Josephs, K.A.; Lang, A.E.; Mollenhauer, B.; Muller, U.; Nilsson, C.; Whitwell, J.L.; et al. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov. Disord. 2017, 32, 853–864. [Google Scholar] [CrossRef]
- Quattrone, A.; Morelli, M.; Nigro, S.; Quattrone, A.; Vescio, B.; Arabia, G.; Nicoletti, G.; Nistico, R.; Salsone, M.; Novellino, F.; et al. A new MR imaging index for differentiation of progressive supranuclear palsy-parkinsonism from Parkinson’s disease. Parkinsonism Relat. Disord. 2018, 54, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, G.; Morelli, M.; Quattrone, A.; Chiriaco, C.; Vaccaro, M.G.; Gulla, D.; Rocca, F.; Caracciolo, M.; Novellino, F.; Sarica, A.; et al. In vivo evidence for decreased scyllo-inositol levels in the supplementary motor area of patients with Progressive Supranuclear Palsy: A proton MR spectroscopy study. Parkinsonism Relat. Disord. 2019, 62, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.G.; Holden, S.K.; Litvan, I.; McKeith, I.; Stebbins, G.T.; Taylor, J.P. Evolution of diagnostic criteria and assessments for Parkinson’s disease mild cognitive impairment. Mov. Disord. 2018, 33, 503–510. [Google Scholar] [CrossRef] [Green Version]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Vaccaro, M.G.; Sarica, A.; Quattrone, A.; Chiriaco, C.; Salsone, M.; Morelli, M.; Quattrone, A. Neuropsychological assessment could distinguish among different clinical phenotypes of progressive supranuclear palsy: A Machine Learning approach. J. Neuropsychol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Carpinelli Mazzi, M.; Iavarone, A.; Russo, G.; Musella, C.; Milan, G.; D’Anna, F.; Garofalo, E.; Chieffi, S.; Sannino, M.; Illario, M.; et al. Mini-Mental State Examination: New normative values on subjects in Southern Italy. Aging Clin. Exp. Res. 2020, 32, 699–702. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Grigoletto, F.; Zappalà, G.; Anderson, D.W.; Lebowitz, B.D. Norms for the Mini-Mental State Examination in a healthy population. Neurology 1999, 53, 315. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Harris, C.R.; Millman, K.J.; van der Walt, S.J.; Gommers, R.; Virtanen, P.; Cournapeau, D.; Wieser, E.; Taylor, J.; Berg, S.; Smith, N.J. Array programming with NumPy. Nature 2020, 585, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- McKinney, W. Data structures for statistical computing in python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; pp. 51–56. [Google Scholar]
- Seabold, S.; Perktold, J. Statsmodels: Econometric and statistical modeling with python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; p. 61. [Google Scholar]
- Hutcheson, G.D. Ordinary least-squares regression. In L. Moutinho and GD Hutcheson, the SAGE Dictionary of Quantitative Management Research; Sage: Southend Oaks, CA, USA, 2011; pp. 224–228. [Google Scholar]
- Brusco, M.J.; Köhn, H.-F. Exemplar-based clustering via simulated annealing. Psychometrika 2009, 74, 457–475. [Google Scholar] [CrossRef]
- Rousseeuw, P.J. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. J. Comput. Appl. Math. 1987, 20, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Dueck, D. Affinity Propagation: Clustering Data by Passing Messages. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, September 2009. [Google Scholar]
- Brusco, M.J.; Shireman, E.; Steinley, D. A comparison of latent class, K-means, and K-median methods for clustering dichotomous data. Psychol. Methods 2017, 22, 563–580. [Google Scholar] [CrossRef] [PubMed]
- Starczewski, A. A new validity index for crisp clusters. Pattern Anal. Appl. 2017, 20, 687–700. [Google Scholar] [CrossRef] [Green Version]






| CTRL (44) | PD (49) | PSP (48) | p-Value | Post-Hoc | |
|---|---|---|---|---|---|
| Age | 62.6 ± 11.5 | 66.7 ± 9.38 | 70.1 ± 8.32 | 0.002 a | CTRL < PSP b |
| Female, n | 25 | 22 | 22 | N.S. c | |
| Education | 12.5 ± 4.78 | 9.27 ± 4.74 | 7.38 ± 5.05 | <0.001 a | CTRL > PD b, PSP b |
| Total MMSE | 29.2 ± 1.46 | 24.8 ± 5.08 | 20.8 ± 5.27 | <0.001 d | CTRL > PD e, PSP e; PD > PSP e |
| TO | 4.93 ± 0.45 (0.241 ± 0.57) | 4.49 ± 1.04 (0.100 ± 1.010) | 3.85 ± 1.38 (−0.321 ± 1.250) | 0.01 d | CTRL > PSP e |
| OS | 4.98 ± 0.15 (0.31 ± 0.567) | 4.29 ± 1.15 (−0.025 ± 0.992) | 3.81 ± 1.21 (−0.259 ± 0.999) | 0.003 d | CTRL > PSP e |
| Reg | 3.00 ± 0 (0.008 ± 0.084) | 2.98 ± 0.143 (0.042 ± 0.142) | 2.85 ± 0.50 (−0.050 ± 0.485) | N.S.d | N.A. |
| AC | 4.80 ± 0.60 (0.854 ± 0.846) | 3.14 ± 1.90 (−0.167 ± 1.590) | 2.25 ± 1.77 (−0.616 ± 1.690) | <0.001 d | CTRL > PD e, PSP e |
| Rec | 2.98 ± 0.15 (0.66 ± 0.39) | 1.96 ± 1.08 (−0.165 ± 0.970) | 1.52 ± 0.9 (−0.441 ± 1.010) | <0.001 d | CTRL > PD e, PSP e |
| N | 1.98 ± 0.15 (−0.02 ± 0.14) | 2.00 ± 0 (0.030 ± 0.058) | 1.94 ± 0.32 (−0.015 ± 0.303) | N.S. d | N.A. |
| SR | 1.00 ± 0 (0.10 ± 0.04) | 0.82 ± 0.39 (−0.055 ± 0.403) | 0.81 ± 0.39 (−0.038 ± 0.384) | 0.03 d | CTRL > PD e |
| P | 2.93 ± 0.45 (−0.02 ± 0.43) | 2.98 ± 0.143 (0.088 ± 0.163) | 2.77 ± 0.55 (−0.074 ± 0.540) | N.S.d | N.A. |
| W | 0.91 ± 0.30 (0.16 ± 0.30) | 0.67 ± 0.47 (0.065 ± 0.394) | 0.29 ± 0.46 (−0.210 ± 0.465) | <0.001 d | CTRL > PSP e; PD > PSP e |
| CE | 0.82 ± 0.40 (−0.003 ± 0.410) | 0.84 ± 0.37 (0.123 ± 0.344) | 0.52 ± 0.50 (−0.120 ± 0.454) | 0.01 d | PD > PSP e |
| D | 0.84 ± 0.37 (0.111 ± 0.270) | 0.65 ± 0.48 (0.083 ± 0.394) | 0.25 ± 0.44 (−0.185 ± 0.421) | <0.001 d | CTRL > PSP e; PD > PSP e |
| Median Preference | Minimum Preference | |||
|---|---|---|---|---|
| Group | #Clusters | Silhouette Index | #Clusters | Silhouette Index |
| CTRL | 8 | 0.302 | 1 | N.A. |
| PD | 7 | 0.375 | 2 | 0.675 |
| PSP | 6 | 0.387 | 2 | 0.677 |
| CTRL + PD + PSP | 16 | 0.237 | 4 | 0.601 |
| Cluster #1 (68) | Cluster #2 (30) | Cluster #3 (8) | Cluster #4 (34) | p-Value | Post-Hoc | |
|---|---|---|---|---|---|---|
| Age | 62.4 ± 10.1 | 71.3 ± 9.94 | 70.4 ± 7.93 | 69.8 ± 7.64 | <0.001 a | 1 < 2,4 b |
| Female, n | 33 | 14 | 5 | 17 | N.S. c | N.A. |
| Education | 12.1 ± 5.23 | 6.60 ± 3.23 | 5.5 ± 2.67 | 8.59 ± 4.99 | <0.001 a | 1 > 2,3,4 e |
| Total MMSE | 27.3 ± 3.93 | 27.7 ± 1.95 | 12.6 ± 2.92 | 20.1 ± 3.57 | <0.001 d | 1 > 3,4 e 2 > 1,3,4 e 4 > 3 e |
| TO | 4.68 ± 0.74 (0.026 ± 0.565) | 4.9 ± 0.55 (0.800 ± 0.550) | 1.25 ± 1.04 (−2.800 ± 0.842) | 4.18 ± 0.97 (−0.099 ± 0.888) | <0.001 d | 1 > 3 e 2 > 1,3,4 e 4 > 3 e |
| OS | 4.71 ± 0.69 (0.067 ± 0.472) | 4.83 ± 0.46 (0.856 ± 0.487) | 2 ± 0.76 (−1.85 ± 0.43) | 3.74 ± 1.24 (−0.454 ± 1.02) | <0.001 d | 1 > 3,4 e 2 > 1,3,4 e 4 > 3 e |
| Reg | 2.93 ± 0.39 (−0.056 ± 0.372) | 3 ± 0 (0.108 ± 0.040) | 2.75 ± 0.46 (−0.139 ± 0.472) | 2.97 ± 0.17 (0.049 ± 0.162) | 0.016 d | 2 > 1 e |
| AC | 4.21 ± 1.33 (0.345 ± 0.636) | 4.60 ± 0.72 (1.89 ± 0.619) | 0.50 ± 0.76 (−2.06 ± 1.11) | 1.21 ± 0.99 (−1.88 ± 0.767) | <0.001 d | 1 > 3,4 e 2 > 1,3,4 e |
| Rec | 2.59 ± 0.69 (0.3 ± 0.637) | 2.50 ± 0.73 (0.021 ± 0.18) | 1.13 ± 0.83 (−0.775 ± 0.993) | 1.09 ± 0.93 (−0.937 ± 0.889) | <0.001 d | 1 > 3,4 e 2 > 3,4 e |
| N | 2 ± 0 (0.007 ± 0.050) | 1.97 ± 0.183 (0.056 ± 0.302) | 1.75 ± 0.71 (−0.173 ± 0.675) | 1.97 ± 0.17 (0.008 ± 0.16) | N.S. d | N.A. |
| SR | 0.89 ± 0.31 (0.005 ± 0.300) | 0.9 ± 0.30 (0.072 ± 0.532) | 0.50 ± 0.53 (−0.337 ± 0.535) | 0.88 ± 0.33 (0.019 ± 0.331) | 0.025 d | 3 < 1,2,4 e |
| P | 2.94 ± 0.29 (−0.007 ± 0.268) | 2.90 ± 0.55 (0.201 ± 0.484) | 2.50 ± 0.76 (−0.312 ± 0.748) | 2.88 ± 0.41 (0.024 ± 0.416) | N.S.d | N.A. |
| W | 0.74 ± 0.41 (0.061 ± 0.316) | 0.67 ± 0.479 (0.218 ± 0.38) | 0.12 ± 0.35 (−0.333 ± 0.386) | 0.32 ± 0.47 (−0.22 ± 0.437) | <0.001 d | 1 > 3,4 e 2 > 3,4 e |
| CE | 0.76 ± 0.43 (−0.039 ± 0.376) | 0.83 ± 0.379 (0.178 ± 0.45) | 0 ± 0 (−0.605 ± 0.075) | 0.71 ± 0.46 (0.029 ± 0.418) | <0.001 d | 1 > 3 e 2 > 1,3 e 4 > 3 e |
| D | 0.79 ± 0.41 (0.070 ± 0.297) | 0.57 ± 0.50 (0.178 ± 0.450) | 0 ± 0 (−0.358 ± 0.212) | 0.26 ± 0.45 (−0.213 ± 0.402) | <0.001 d | 1 > 3,4 e 2 > 3,4 e |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarica, A.; Vaccaro, M.G.; Quattrone, A.; Quattrone, A. A Novel Approach for Cognitive Clustering of Parkinsonisms through Affinity Propagation. Algorithms 2021, 14, 49. https://doi.org/10.3390/a14020049
Sarica A, Vaccaro MG, Quattrone A, Quattrone A. A Novel Approach for Cognitive Clustering of Parkinsonisms through Affinity Propagation. Algorithms. 2021; 14(2):49. https://doi.org/10.3390/a14020049
Chicago/Turabian StyleSarica, Alessia, Maria Grazia Vaccaro, Andrea Quattrone, and Aldo Quattrone. 2021. "A Novel Approach for Cognitive Clustering of Parkinsonisms through Affinity Propagation" Algorithms 14, no. 2: 49. https://doi.org/10.3390/a14020049
APA StyleSarica, A., Vaccaro, M. G., Quattrone, A., & Quattrone, A. (2021). A Novel Approach for Cognitive Clustering of Parkinsonisms through Affinity Propagation. Algorithms, 14(2), 49. https://doi.org/10.3390/a14020049