
An Effective Atrial Fibrillation Detection from Short Single-Lead Electrocardiogram Recordings Using MCNN-BLSTM Network



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
- 1.
- CinC2017: The CinC2017 ECG recordings were collected using the AliveCor facility. The officially published training set contains 8528 single-lead recordings. These recordings have different lengths, ranging from 9 s to 61 s. The sampling rate is 300 Hz. This database contains a total of four rhythm types, namely, normal rhythm (N), atrial fibrillation rhythm (A), other rhythms (O), and noise. The detailed content of the database is shown in Table 1.
- 2.
- CPSC2018: The CPSC2018 database includes 6877 recordings collected from the officially issued training set of 11 hospitals, and each sample contains standard 12-lead signals. Here, we use the second lead for testing. The recordings varied in length, ranging from 6 s to 144 s. The sampling rate is 500 Hz. The database contained a total of nine rhythmic types. We organized the data from the CPSC2018 database into three categories: N, AF, and O. Our goal is to screen AF patients based on their short ECG recordings, and the database is detailed in Table 1.
2.2. Methods
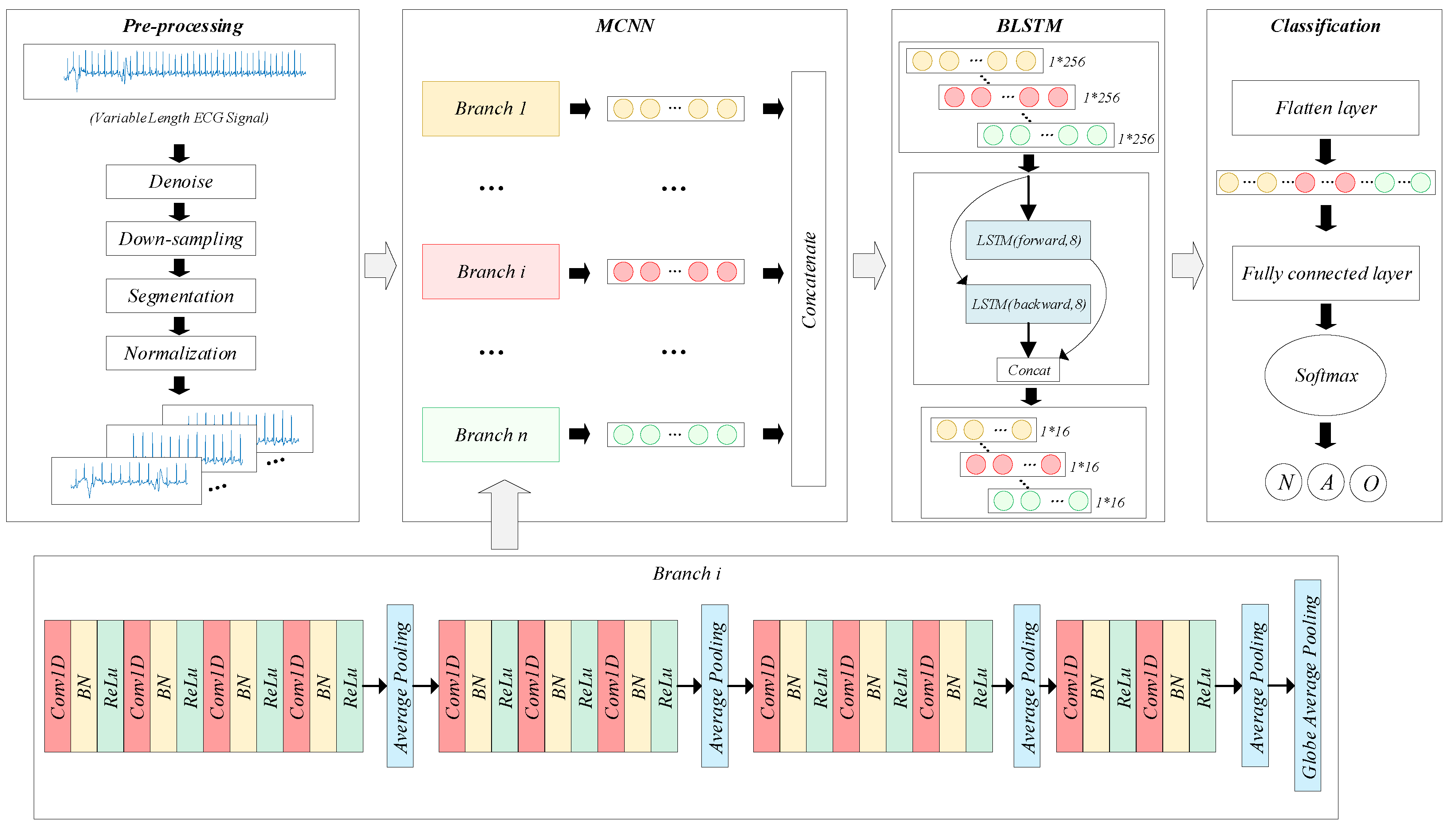
2.2.1. Pre-Processing
2.2.2. Problem Description
2.2.3. Model Architecture
- 1.
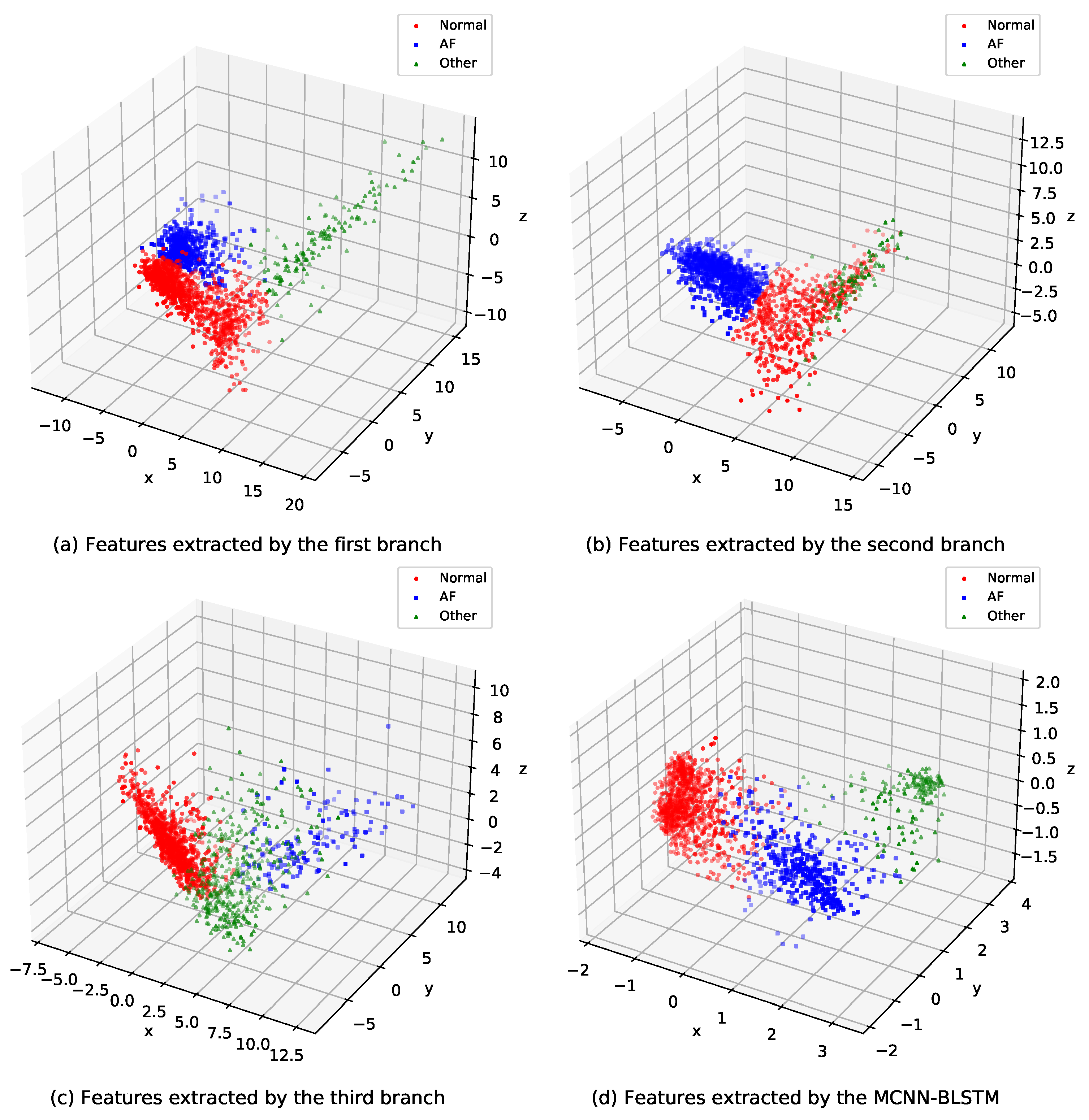
- MCNN: For the MCNN considered in this study, the number n of branches is set based on the slice length l which is chosen as 6 s, 10 s, 15 s, 20 s, 25 s, and 30 s. Thus, , where L is the length of a short ECG recording, and l is the length of each ECG segment. Each short ECG recording has a different length. To make full use of the information from one ECG recording, we adopted the overlapping cutting scheme. The overlapping part is calculated using Equation (1). Thus, the MCNN could extract the entire short ECG recording feature, which improves the inadequacy of the 1-branch CNN (1BCNN) that could not extract all the ECG information.In MCNN, each branch consists of 12 convolutional layers and four pooling layers, grouped by convolutional layers and separated by a pooling layer. Therefore, each 1BCNN consists of four groups of convolutional layers. The number of convolutional layers in the four convolution groups is 4, 3, 3, and 2. The number of filters in the first group is 8, 16, 32, and 32. There are 64 filters in the second group. The third group has 128 filters. The last group of convolutional layers has 256 filters. Output data are processed using batch normalization (BN) [29] to solve the problem of an internal covariate shift. It has the advantage of allowing the model to use a higher learning rate during the training process, which could reduce the possibility of the over-fitting of the layer.In addition, the pooling layer of each group uses average pooling (AP), and the last layer uses global average pooling (GAP). The pooling layer has the advantages of data dimensionality reduction, nonlinear transformation, and expansion of the perception field. In each branch, the pooling layer step size is set to four to quickly reduce the computational complexity and capture the local features between the ECG recordings within a short time window. The last group of convolutions is used by the GAP instead of the AP. GAP [30] mainly performs a pooling of the entire feature map of the last layer to form a feature point. It is mainly proposed to solve the problem of full connection, as there are too many parameters in the full connection operation. One advantage of GAP over a fully connected layer is that it has no parameters that need to be optimized. Thus, overfitting of the layer is avoided. Additionally, GAP can extract spatial information and is more robust to the spatial transformation of the inputs. Let be the activation value of element k in the last convolutional layer on the feature space location . For unit k, the result of the GAP was obtained.
- 2.
- LSTM: LSTM is one kind of recurrent neural network. Unlike the traditional RNN, LSTM can effectively deal with the long-term dependence of temporal signals [31]. The computational process of LSTM is more complex than RNN, and the main computational process is shown following:where , , , and are the forget gate, input gate, output gate, and the cell unit information vector, respectively. W denotes a weight matrix (e.g., is the weight matrix of the input gate), and b denotes an offset vector (e.g., is the offset vector of the input gate). When the forget gate or the input gate is activated, the value stored in cell unit is updated. The output gate controls the value in the cell to be output from the LSTM cell.Compared with LSTM, BLSTM can fetch both the preceding and the following context information, avoiding the disadvantage that LSTM networks can only extract the preceding context information [22]. In this paper, we used BLSTM to consider 256 ECG features of the n segments extracted by the MCNN, the n segments are segmented in the chronological order of the ECG recording. Finally, a layer is used to predict the type of one input ECG recording (normal, AF, or other rhythms).
2.3. Model Training
3. Results
3.1. Evaluation Metrics
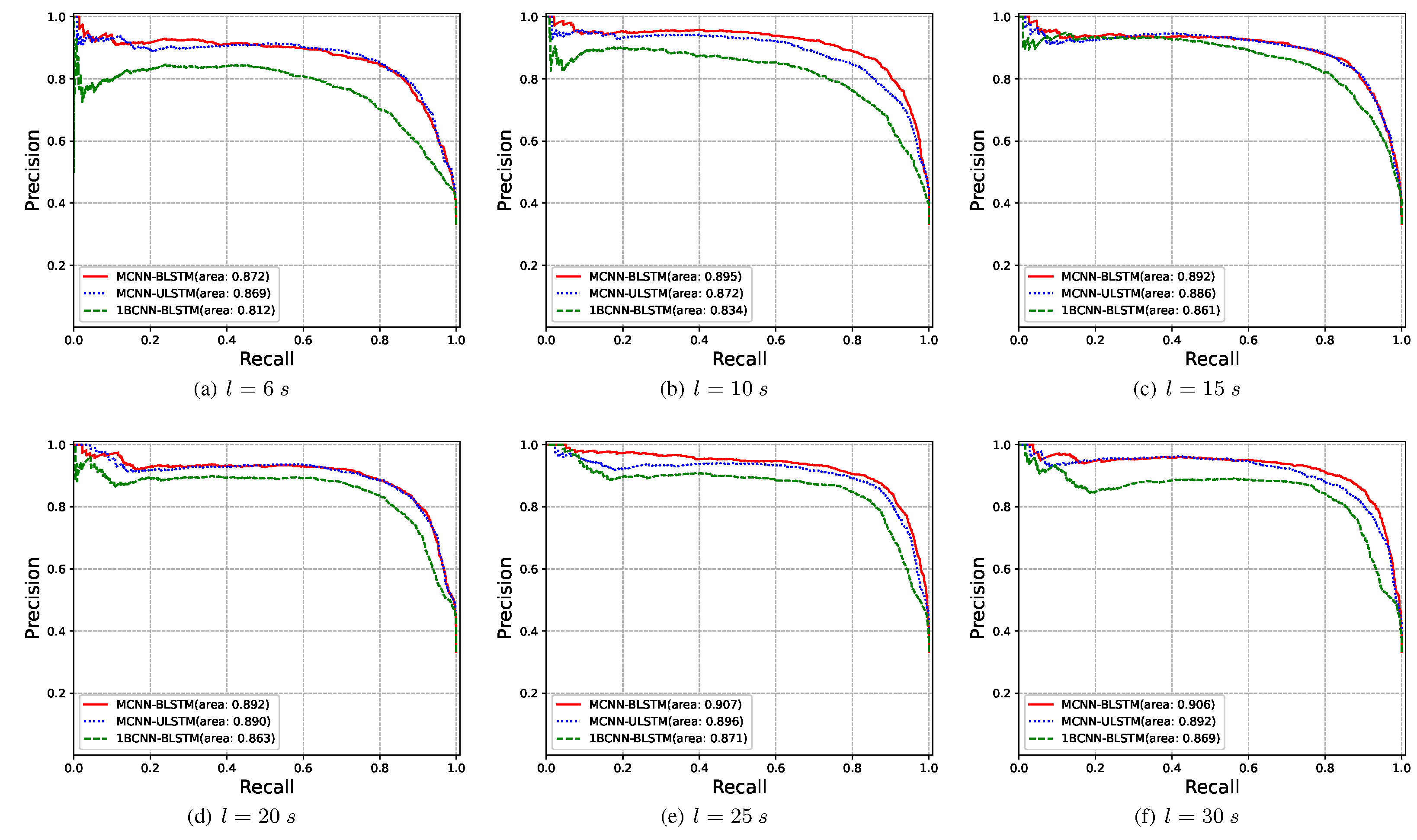
3.2. Ablation Experiments
- 1.
- 1BCNN-BLSTM: The model has the same structure as MCNN-BLSTM, but can only input a single branch ECG signal. When the length L of the segment is longer than the original ECG recording, zero padding is performed for the segment length. When the length of the segment is shorter than the original ECG recording, the ECG segment with the front length L of the original ECG recording is intercepted and used as the input of the model.
- 2.
- MCNN-ULSTM: The model has the same structure as MCNN-BLSTM, but BLSTM was modified to ULSTM to verify the influence of the BLSTM module on atrial fibrillation detection.
3.3. Evaluation the Robustness of the Proposed Model
3.4. Evaluation Results of the Proposed Model Using the CPSC2018 as the Training Data
4. Discussion
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2020, 42, 373–498. [Google Scholar]
- Tiver, K.D.; Quah, J.; Lahiri, A.; Ganesan, A.N.; McGavigan, A.D. Atrial fibrillation burden: An update—The need for a CHA2DS2-VASc-AFBurden score. EP Eur. 2020, 23, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Lima, E.M.; Ribeiro, A.H.; Paixao, G.M.M.; Ribeiro, M.H.; Pinto-Filho, M.M.; Gomes, P.R.; Oliveira, D.M.; Sabino, E.C.; Duncan, B.B.; Giatti, L.; et al. Deep neural network-estimated electrocardiographic age as a mortality predictor. Nat. Commun. 2021, 12, 5117. [Google Scholar] [CrossRef] [PubMed]
- Zungsontiporn, N.; Link, M.S. Newer technologies for detection of atrial fibrillation. BMJ 2018, 363, k3946. [Google Scholar] [CrossRef]
- Vignesh, K.; Lakshman, S.T. Detection of atrial fibrillation using discrete-state Markov models and Random Forests. Comput. Biol. Med. 2019, 113, 103386. [Google Scholar]
- Warrick, P.A.; Nabhan Homsi, M. Ensembling convolutional and long short-term memory networks for electrocardiogram arrhythmia detection. Physiol. Meas. 2018, 39, 114002. [Google Scholar] [CrossRef]
- Lee, H.; Shin, M. Learning Explainable Time-Morphology Patterns for Automatic Arrhythmia Classification from Short Single-Lead ECGs. Sensors 2021, 21, 4331. [Google Scholar] [CrossRef]
- Fang, B.; Chen, J.; Liu, Y.; Wang, W.; Wang, K.; Singh, A.K.; Lv, Z. Dual-channel Neural Network for Atrial Fibrillation Detection from a Single Lead ECG Wave. IEEE J. Biomed. Health Inform. 2021, 1. [Google Scholar] [CrossRef]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2017, 14, e275–e444. [Google Scholar]
- Tang, W.H.; Chang, Y.J.; Chen, Y.J.; Ho, W.H. Genetic algorithm with Gaussian function for optimal P-wave morphology in electrocardiography for atrial fibrillation patients. Comput. Electr. Eng. 2018, 67, 52–57. [Google Scholar] [CrossRef]
- Sadr, N.; Jayawardhana, M.; Pham, T.T.; Tang, R.; Balaei, A.T.; de Chazal, P. A low-complexity algorithm for detection of atrial fibrillation using an ECG. Physiol. Meas. 2018, 39, 064003. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Liu, C.; Wei, S.; Shen, Q.; Zhou, F.; Li, J. A New Entropy-Based Atrial Fibrillation Detection Method for Scanning Wearable ECG Recordings. Entropy 2018, 20, 904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurmaini, S.; Tondas, A.; Darmawahyuni, A.; Rachmatullah, M.N.; Umi Partan, R.; Firdaus, F.; Tutuko, B.; Pratiwi, F.; Juliano, A.H.; Khoirani, R. Robust detection of atrial fibrillation from short-term electrocardiogram using convolutional neural networks. Future Gener. Comput. Syst. 2020, 113, 304–317. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Li, Y.S.; Hwang, B.J.; Hsiao, C.H. Detection of Atrial Fibrillation Using 1D Convolutional Neural Network. Sensors 2020, 20, 2136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhekumuzi, M.M.; Lin, Y.T.; Lin, C.H.; Abbod, M.F.; Shieh, J.S. ECG arrhythmia classification by using a recurrence plot and convolutional neural network. Biomed. Signal Process. Control 2021, 64, 102262. [Google Scholar]
- Kamaleswaran, R.; Mahajan, R.; Akbilgic, O. A robust deep convolutional neural network for the classification of abnormal cardiac rhythm using single lead electrocardiograms of variable length. Physiol. Meas. 2018, 39, 035006. [Google Scholar] [CrossRef]
- Cao, P.; Li, X.; Mao, K.; Lu, F.; Ning, G.; Fang, L.; Pan, Q. A novel data augmentation method to enhance deep neural networks for detection of atrial fibrillation. Biomed. Signal Process. Control 2020, 56, 101675. [Google Scholar] [CrossRef]
- Zhang, H.; He, R.; Dai, H.; Xu, M.; Wang, Z. SS-SWT and SI-CNN: An Atrial Fibrillation Detection Framework for Time-Frequency ECG Signal. J. Healthc. Eng. 2020, 2020, 7526825. [Google Scholar] [CrossRef]
- Fan, X.; Yao, Q.; Cai, Y.; Miao, F.; Sun, F.; Li, Y. Multiscaled Fusion of Deep Convolutional Neural Networks for Screening Atrial Fibrillation From Single Lead Short ECG Recordings. IEEE J. Biomed. Health Inform. 2018, 22, 1744–1753. [Google Scholar] [CrossRef]
- Mehrang, S.; Jafari Tadi, M.; Knuutila, T.; Jaakkola, J.; Jaakkola, S.; Kiviniemi, T.; Vasankari, T.; Airaksinen, J.; Koivisto, T.; Pankaala, M. End-to-end sensor fusion and classification of atrial fibrillation using deep neural networks and smartphone mechanocardiography. Physiol. Meas. 2022, 43, 055004. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.S.; Peimankar, A.; Puthusserypady, S. A deep learning approach for real-time detection of atrial fibrillation. Expert Syst. Appl. 2019, 115, 465–473. [Google Scholar] [CrossRef]
- Lu, P.; Xi, H.; Zhou, B.; Zhang, H.; Lin, Y.; Chen, L.; Gao, Y.; Zhang, Y.; Hu, Y.; Chen, Z. A New Multichannel Parallel Network Framework for the Special Structure of Multilead ECG. J. Healthc. Eng. 2020, 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.D.; Liu, C.; Moody, B.; Lehman, L.w.H.; Silva, I.; Li, Q.; Johnson, A.E.; Mark, R.G. AF classification from a short single lead ECG recording: The PhysioNet/computing in cardiology challenge 2017. Comput. Cardiol. 2017, 44. [Google Scholar] [CrossRef]
- Liu, F.; Liu, C.; Zhao, L.; Zhang, X.; Wu, X.; Xu, X.; Liu, Y.; Ma, C.; Wei, S.; He, Z.; et al. An Open Access Database for Evaluating the Algorithms of Electrocardiogram Rhythm and Morphology Abnormality Detection. J. Med. Imaging Health Inform. 2018, 8, 1368–1373. [Google Scholar] [CrossRef]
- Brij, N.S.; Arvind, K.T. Optimal selection of wavelet basis function applied to ECG signal denoising. Digit. Signal Process. 2006, 16, 275–287. [Google Scholar]
- Aiwiscal. CPSC_Scheme. 2019. Available online: https://github.com/Aiwiscal/CPSC_Scheme (accessed on 2 January 2019).
- Ioffe, S.; Szegedy, C. Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift. arXiv 2015, arXiv:1502.03167. [Google Scholar]
- Lin, M.; Chen, Q.; Yan, S. Network In Network. arXiv 2013, arXiv:1312.4400. [Google Scholar]
- Sak, H.; Senior, A.; Beaufays, F. Long Short-Term Memory Recurrent Neural Network Architectures for Large Scale Acoustic Modeling. arXiv 2014, arXiv:1402.1128. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Duchi, J.; Hazan, E.; Singer, Y. Adaptive Subgradient Methods for Online Learning and Stochastic Optimization. J. Mach. Learn. Res. 2011, 12, 2121–2159. [Google Scholar]
- Gu, J.; Wang, Z.; Kuen, J.; Ma, L.; Shahroudy, A.; Shuai, B.; LIU, T.; Wang, X.; Wang, G.; Cai, J.; et al. Recent advances in convolutional neural networks. Pattern Recognit. 2018, 77, 354–377. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A Simple Way to Prevent Neural Networks from Overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Rohr, M.; Reich, C.; Hohl, A.; Lilienthal, T.; Dege, T.; Plesinger, F.; Bulkova, V.; Clifford, G.; Reyna, M.; Hoog Antink, C. Exploring novel algorithms for atrial fibrillation detection by driving graduate level education in medical machine learning. Physiol. Meas. 2022, 43, 074001. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Database | Rhythm | #Number of Recordings | Time Length(s) | ||
|---|---|---|---|---|---|
| Mean | Min | Max | |||
| PhysioNet/CinC Challenge 2017 | Normal | 5050 | 32.10 | 9.05 | 60.95 |
| AF | 738 | 32.10 | 9.99 | 60.21 | |
| Other | 2456 | 34.39 | 9.13 | 60.86 | |
| Noise | 284 | 24.22 | 9.36 | 60.00 | |
| China Physiological Signal Challenge 2018 | Normal | 918 | 15.43 | 10.00 | 60.00 |
| AF | 1098 | 15.04 | 9.00 | 74.00 | |
| Other | 4861 | 16.25 | 6.00 | 144.00 | |
| Learning Parameter | Values |
|---|---|
| Weight penalty | L2-norm |
| Trade-off parameter | 0.001 |
| Optimizer | SGD |
| Learning rate initial value | 0.10 |
| Dropout proportion | 0.40 |
| Batch size | 32 |
| Momentum coefficient | 0.70 |
| Number of epochs | 100 |
| Predicted | |||
|---|---|---|---|
| Positive | Negative | ||
| Reference | Positive | TP | FN |
| Negative | FP | TN | |
| Input Length | Model | PRE (%) | REC (%) | SPE (%) | F1 (%) | ACC (%) |
|---|---|---|---|---|---|---|
| 6 s | 1BCNN-BLSTM | 67.34 | 67.72 | 83.59 | 66.84 | 74.89 |
| MCNN-ULSTM | 77.23 | 81.81 | 89.68 | 79.10 | 82.60 | |
| MCNN-BLSTM | 76.81 | 80.99 | 89.81 | 78.94 | 82.96 | |
| 10 s | 1BCNN-BLSTM | 71.45 | 73.49 | 85.77 | 71.84 | 77.80 |
| MCNN-ULSTM | 79.20 | 81.17 | 89.49 | 80.10 | 82.96 | |
| MCNN-BLSTM | 85.24 | 80.80 | 89.94 | 82.57 | 85.99 | |
| 15 s | 1BCNN-BLSTM | 78.92 | 76.59 | 87.71 | 77.61 | 81.50 |
| MCNN-ULSTM | 80.38 | 82.74 | 90.84 | 81.45 | 84.78 | |
| MCNN-BLSTM | 82.93 | 80.18 | 91.21 | 81.41 | 85.63 | |
| 20 s | 1BCNN-BLSTM | 74.90 | 81.71 | 89.23 | 76.45 | 81.69 |
| MCNN-ULSTM | 79.74 | 84.12 | 91.11 | 80.92 | 85.39 | |
| MCNN-BLSTM | 80.37 | 84.44 | 91.84 | 82.17 | 85.63 | |
| 25 s | 1BCNN-BLSTM | 75.67 | 81.84 | 90.22 | 77.63 | 82.84 |
| MCNN-ULSTM | 81.89 | 85.63 | 91.84 | 83.59 | 86.17 | |
| MCNN-BLSTM | 85.38 | 83.79 | 92.01 | 84.56 | 87.57 | |
| 30 s | 1BCNN-BLSTM | 74.40 | 82.18 | 90.84 | 76.95 | 82.47 |
| MCNN-ULSTM | 79.69 | 85.10 | 91.51 | 81.51 | 85.57 | |
| MCNN-BLSTM | 84.27 | 84.20 | 92.03 | 84.15 | 87.51 | |
| 61 s | 1BCNN-BLSTM | 83.22 | 82.11 | 90.53 | 82.08 | 86.23 |
| Rhythm | PRE (%) | REC (%) | SPE (%) | F1 (%) | ACC (%) |
|---|---|---|---|---|---|
| Normal | 88.10 | 94.41 | 81.08 | 91.14 | - |
| AF | 87.30 | 74.83 | 98.78 | 80.59 | - |
| Other | 81.69 | 73.01 | 73.43 | 77.11 | - |
| Noise | 66.67 | 66.67 | 98.97 | 66.67 | - |
| Avg. | 80.94 | 77.23 | 88.07 | 78.88 | 85.76 |
| Rhythm | PRE (%) | REC (%) | SPE (%) | F1 (%) | ACC (%) |
|---|---|---|---|---|---|
| Normal | 78.15 | 62.42 | 97.22 | 69.41 | - |
| AF | 81.63 | 89.69 | 96.10 | 85.47 | - |
| Other | 90.41 | 91.91 | 77.18 | 91.15 | - |
| Avg. | 83.40 | 81.34 | 90.17 | 82.01 | 87.50 |
| Source Reference | Model | ||||
|---|---|---|---|---|---|
| Warrick [6] | CNN-LSTM | 90.28 | 82.21 | 73.24 | 81.91 |
| Cao [18] | LSTM | 91.00 | 84.00 | 70.00 | 81.67 |
| Lee [7] | BIT-CNN | 89.73 | 81.06 | 74.45 | 81.75 |
| Fang [8] | VGG | 90.00 | 83.00 | 75.00 | 82.67 |
| Rohr [36] | ECG-RCLSTM-Net | - | - | - | 82.40 |
| Our work | MCNN-BLSTM | 92.02 | 82.03 | 79.62 | 84.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Gu, H.; Gao, J.; Lu, P.; Chen, G.; Wang, Z. An Effective Atrial Fibrillation Detection from Short Single-Lead Electrocardiogram Recordings Using MCNN-BLSTM Network. Algorithms 2022, 15, 454. https://doi.org/10.3390/a15120454
Zhang H, Gu H, Gao J, Lu P, Chen G, Wang Z. An Effective Atrial Fibrillation Detection from Short Single-Lead Electrocardiogram Recordings Using MCNN-BLSTM Network. Algorithms. 2022; 15(12):454. https://doi.org/10.3390/a15120454
Chicago/Turabian StyleZhang, Hongpo, Hongzhuang Gu, Junli Gao, Peng Lu, Guanhe Chen, and Zongmin Wang. 2022. "An Effective Atrial Fibrillation Detection from Short Single-Lead Electrocardiogram Recordings Using MCNN-BLSTM Network" Algorithms 15, no. 12: 454. https://doi.org/10.3390/a15120454
APA StyleZhang, H., Gu, H., Gao, J., Lu, P., Chen, G., & Wang, Z. (2022). An Effective Atrial Fibrillation Detection from Short Single-Lead Electrocardiogram Recordings Using MCNN-BLSTM Network. Algorithms, 15(12), 454. https://doi.org/10.3390/a15120454