
Process Mining the Performance of a Real-Time Healthcare 4.0 Systems Using Conditional Survival Models

Abstract
:1. Introduction
2. Methods
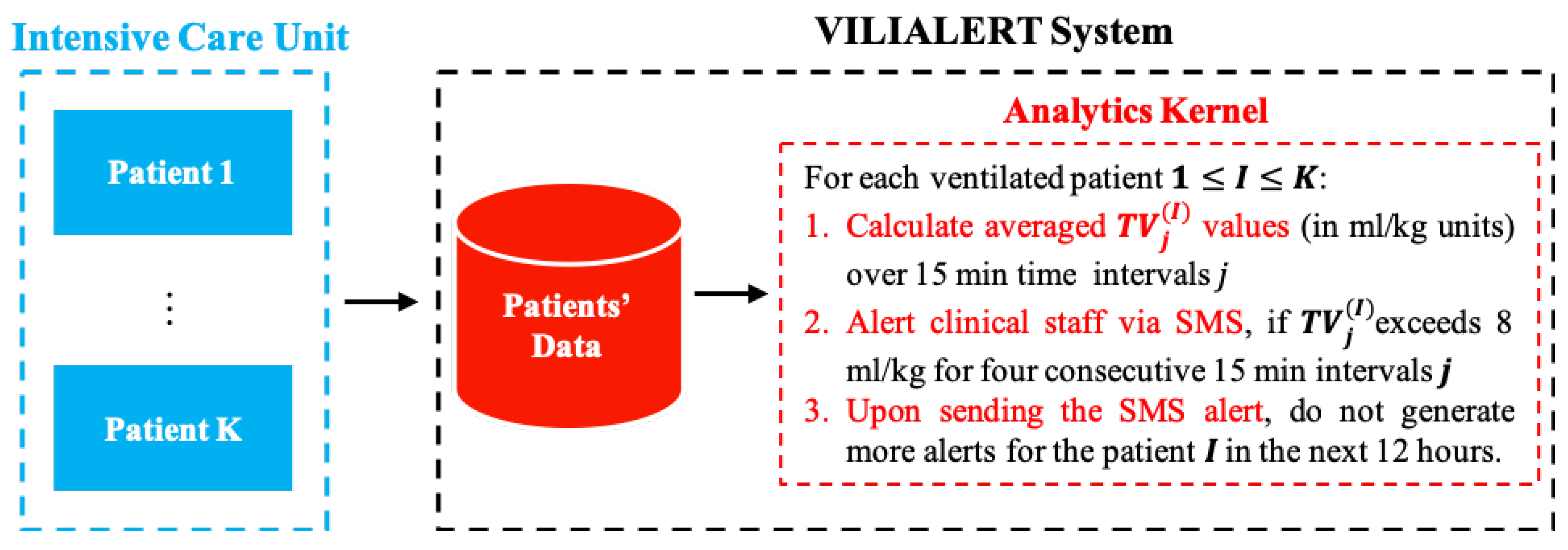
2.1. The VILIAlert System Architecture
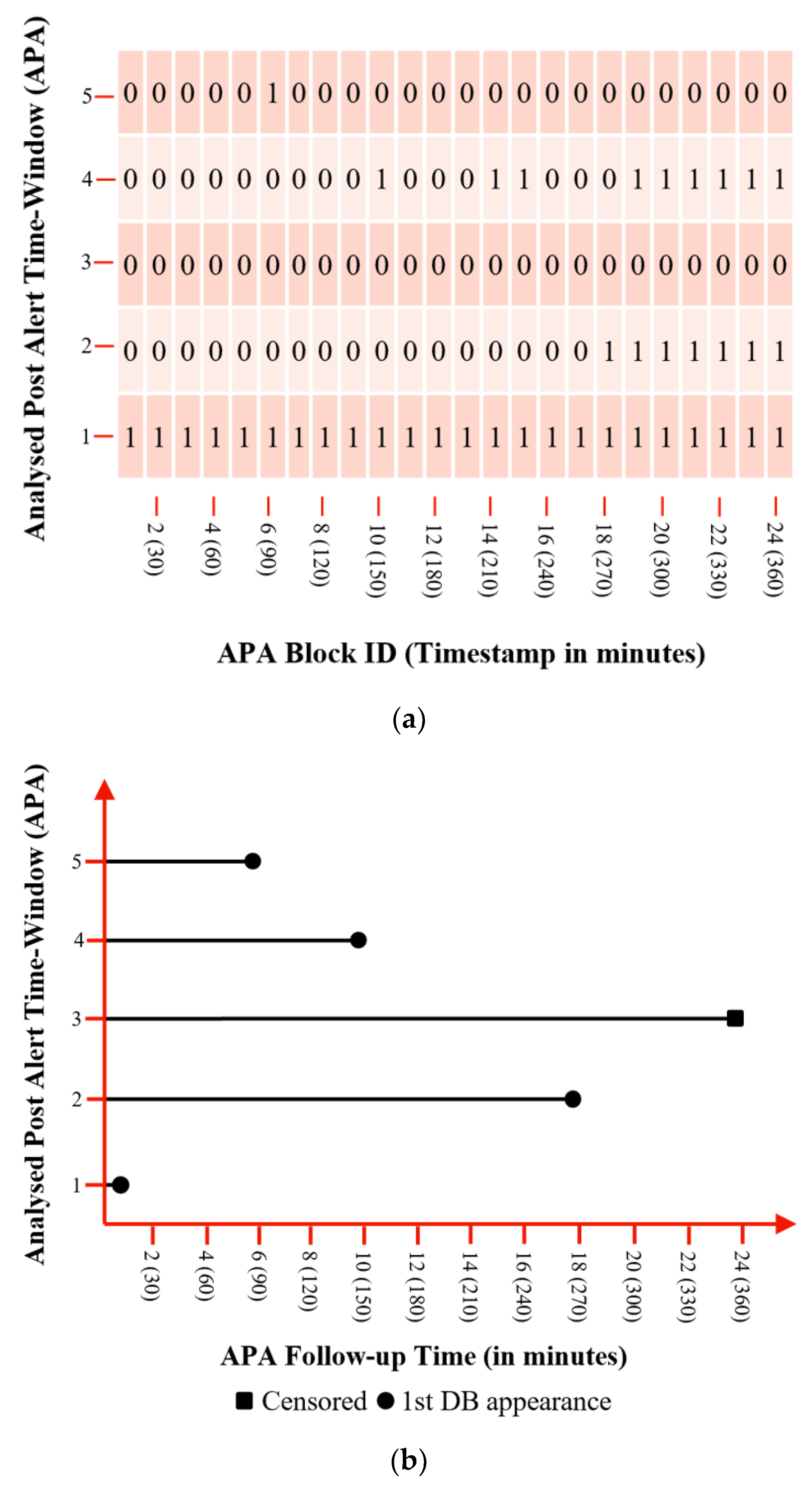
2.2. Survival Analysis Approach for Performance Estimation and Quality of Mechanical Ventilation Evaluation
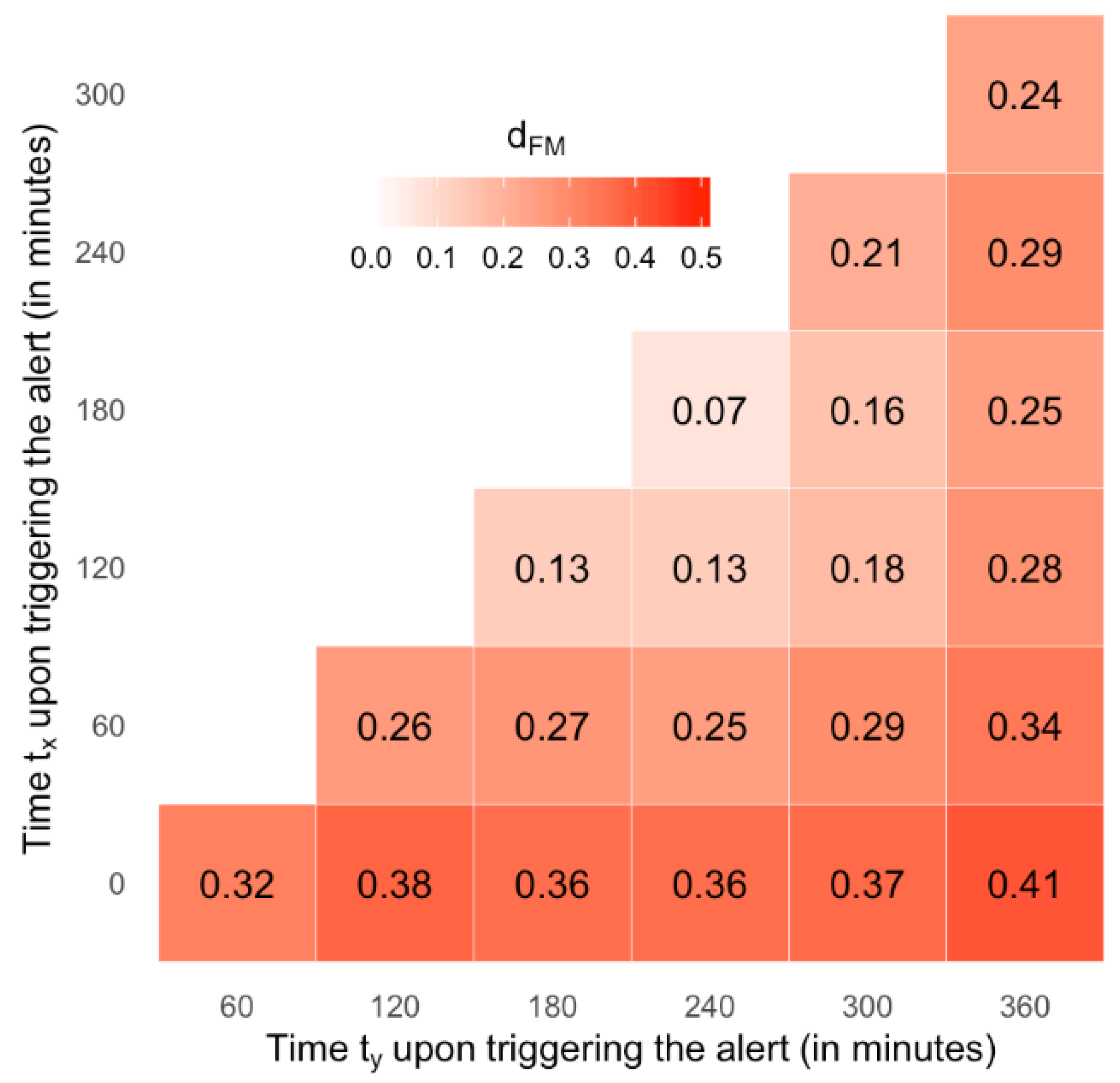
- suggests very small differences;
- suggests small differences;
- suggests moderate differences, and;
- suggests considerable differences between the two genders.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| APA | Analysed Post Alert Time Window |
| AUC | Area Under the receiver operator characteristic Curve |
| CDFS | Conditional Defect Free Survival probability |
| CDS | Clinical Decision Support System |
| CI | Confidence Interval |
| DB | Defective Blocks |
| DFS | Defect Free Survival probability |
| EMR | Electronic Medical Record |
| HL7 | Health Level 7 |
| IBW | Ideal Body Weight |
| ICU | Intensive Care Unit |
| KM | Kaplan-Meier |
| LPV | Lung Protective Ventilation |
| NDB | Non-Defective Blocks |
| RMSE | Root Mean Square Error |
| SF | Shared Frailty |
| SPC | Statistical Process Control |
| TV | Tidal Volume in ml/inspiration units |
| TV15 | Averaged TV values, calculated over 15 min time intervals |
| VILI | Ventilator Induced Lung Injury |
References
- Rojas, E.; Munoz-Gama, J.; Sepúlveda, M.; Capurro, D. Process mining in healthcare: A literature review. J. Biomed. Inform. 2016, 61, 224–236. [Google Scholar] [CrossRef]
- Plathong, K.; Surakratanasakul, B. A study of integration Internet of Things with health level 7 protocol for real-time healthcare monitoring by using cloud computing. In Proceedings of the 10th Biomedical Engineering International Conference (BMEiCON), Hokkaido, Japan, 31 August–2 September 2017. [Google Scholar]
- Health Level Seven International. About HL7. Available online: https://bit.ly/2tkavDk (accessed on 5 February 2019).
- Zhang, J.; Xu, W.; Guo, J.; Gao, S. A temporal model in electronic health record search. Knowl.-Based Syst. 2017, 126, 56–67. [Google Scholar] [CrossRef]
- Amato, F.; de Pietro, G.; Esposito, M.; Mazzocca, N. An integrated framework for securing semi-structural health records. Knowl.-Based Syst. 2015, 79, 99–117. [Google Scholar] [CrossRef]
- Novakovic, A.; Marshall, A.H. Introducing the DM-P approach for analysing the performances of real-time clinical decision support systems. Knowl.-Based Syst. 2020, 198, 105877. [Google Scholar] [CrossRef]
- Ghassemi, M.; Celi, L.A.; Stone, D.J. State of the art review: The data revolution in critical care. Crit. Care 2015, 19, 118. [Google Scholar] [CrossRef] [Green Version]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-Induced Lung Injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [Green Version]
- Determann, R.M.; Royakkers, A.; Wolthuis, E.K.; Vlaar, A.P.; Choi, G.; Paulus, F.; Hofstra, J.J.; de Graaff, M.J.; Korevaar, J.C.; Schultz, M.J. Ventilation with lower tidal volumes as compared with conventional tidal volumes for patients without acute lung injury: A preventive randomized controlled trial. Crit. Care 2010, 14, R1. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.B.P.; Barbas, C.S.V.; Medeiros, D.M.; Magaldi, R.B.; Schettino, G.P.; Lorenzi-Filho, G.; Kairalla, R.A.; Deheinzelin, D.; Munoz, C.; Oliveira, R.; et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N. Engl. J. Med. 1998, 338, 347–354. [Google Scholar] [CrossRef]
- Putensen, C.; Theuerkauf, N.; Zinserling, J.; Wrigge, H.; Pelosi, P. Meta-analysis: Ventilation strategies and outcomes of the acute respiratory distress syndrome and acute lung injury. Ann. Intern. Med. 2009, 151, 566–576. [Google Scholar] [CrossRef]
- Neto, A.S. Lung-Protective Ventilation in Intensive Care Unit and Operation Room: Tidal Volume Size, Level of Positive End-Expiratory Pressure and Driving Pressure; Faculty of Medicine, University of Amsterdam: Amsterdam, The Netherlands, 2017; Available online: https://dare.uva.nl/search?identifier=35660734-9d32-4127-8608-68207d9d5d28 (accessed on 1 April 2022).
- Walkey, A.J.; Wiener, R.S. Risk Factors for Underuse of Lung Protective Ventilation in Acute Lung Injury. Crit. Care 2012, 27, 323.e1–323.e9. [Google Scholar] [CrossRef] [Green Version]
- Checkley, W.; Brower, R.; Korpak, A.; Thompson, B.T. Effects of a clinical trial on mechanical ventilation practices in patients with acute lung injury. Am. J. Respir. Crit. Care Med. 2008, 177, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Kalhan, R.; Mikkelsen, M.; Dedhiya, P.; Christie, J.; Gaughan, C.; Lanken, P.N.; Finkel, B.; Gallop, R.; Fuchs, B.D. Underuse of lung protective ventilation: Analysis of potential factors to explain physician behavior. Crit. Care Med. 2006, 34, 300–306. [Google Scholar] [CrossRef]
- Gillan, C.J.; Novakovic, A.; Marshall, A.H.; Shyamsundar, M.; Nikolopoulos, D.S. Expediting assessments of database performance for streams of respiratory parameters. Comput. Biol. Med. 2018, 100, 186–195. [Google Scholar] [CrossRef] [Green Version]
- Herasevich, V.; Tsapenko, M.; Kojicic, M.; Ahmed, A.; Kashyap, R.; Venkata, C.; Shahjehan, K.; Thakur, S.J.; Pickering, B.W.; Zhang, J.; et al. Limiting ventilator-induced lung injury through individual electronic medical record surveillance. Crit. Care Med. 2011, 39, 34–39. [Google Scholar] [CrossRef]
- Bourdeaux, C.P.; Thomas, M.J.; Gould, T.H.; Malhotra, G.; Jarvstad, A.; Jones, T.; Gilchrist, I.D. Increasing compliance with low tidal volume ventilation in the ICU with two nudge-based interventions: Evaluation through intervention time-series analysis. BMJ Open 2016, 6, e010129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, A.H.; Novakovic, A. Analysing the performance of a real-time Healthcare 4.0 system using shared frailty time to event models. In Proceedings of the 2019 IEEE 32nd International Symposium on Computer-Based Medical Systems (CBMS), Cordoba, Spain, 5–7 June 2019. [Google Scholar]
- Austin, P.C. A Tutorial on Multilevel Survival Analysis: Methods, Models, Applications. Int. Stat. Rev. 2017, 85, 185–203. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Bustamante, A.F.; Wood, C.L.; Tran, Z.V.; Moine, P. Intraoperative ventilation: Incidence and risk factors for receiving large tidal volumes during general anesthesia. BMC Anesthesiol. 2011, 11, 22. [Google Scholar]
- Hieke, S.; Konig, C.; Engelhardt, M.; Schumacher, M. Conditional Survival: A Useful Concept to Provide Information on How Prognosis Evolves over Time. Clin. Cancer Res. 2015, 21, 1530–1536. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.-H.; Lee, H.Y.; Chow, S.-C. Statistical Methods for Conditional Survival Analysis. J. Biopharm. Stat. 2018, 28, 927–938. [Google Scholar] [CrossRef]
- Zabor, E.C.; Gonen, M.; Chapman, P.B.; Panageas, K.S. Dynamic Prognostication Using Conditional Survival Estimates. Cancer 2013, 119, 3589–3592. [Google Scholar] [CrossRef]
- Davis, F.G.; McCarthy, B.J.; Freels, S.; Kupelian, V.; Bondy, M.L. The conditional probability of survival of patients with primary malignant brain tumors. Cancer 1999, 85, 485–491. [Google Scholar] [CrossRef]
- Yuan, X.; Rai, S.N. Confidence Intervals for Survival Probabilities: A Comparison Study. Commun. Stat. Simul. Comput. 2011, 40, 978–991. [Google Scholar] [CrossRef]
- Cucchetti, A.; Piscaglia, F.; Cescon, M.; Ercolani, G.; Terzi, E.; Bolondi, L.; Zanello, M.; Pinna, A.D. Conditional Survival after Hepatic Resection for Hepatocellular Carcinoma in Cirrhotic Patients. Clin. Cancer Res. 2012, 18, 4397–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnard, B.; Kernan, W.N.; Feinstein, A.R. Indexes and boundaries for “quantitative significance” in statistical decisions. J. Clin. Epidimiol. 1990, 43, 1273–1284. [Google Scholar] [CrossRef]
- Kim, Y.; Margonis, G.A.; Prescott, J.D.; Tran, T.B.; Postlewait, L.M.; Maithel, S.K.; Wang, T.S.; Glenn, J.A.; Hatzaras, I.; Shenoy, R.; et al. Curative Surgical Resection of Adrenocortical Carcinoma: Determining Long-term Outcome Based on Conditional Disease-free Probability. Ann. Surg. 2017, 265, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, N.; Wan, F.; Abudurexiti, M.; Wang, J.; Zhu, Y.; Ye, D. Causes of Death and Conditional Survival of Renal Cell Carcinoma. Front. Oncol. 2019, 9, 591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Therneau, T.M. A Package for Survival Analysis in S. 2015. Available online: https://CRAN.R-project.org/package=survival (accessed on 1 April 2022).
- Thernau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000. [Google Scholar]
- Kang, M.; Kim, H.S.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Prognostic factors for conditional survival in patients with muscle-invasive urothelial carcinoma of the bladder treated with radical cystectomy. Sci. Rep. 2015, 5, 12171. [Google Scholar] [CrossRef] [Green Version]
- Bischof, D.A.; Kim, Y.; Dodson, R.; Jimenez, M.C.; Behman, R.; Cocieru, A.; Fisher, S.B.; Groeschl, R.T.; Squires, M.H.; Maithel, S.K.; et al. Conditional Disease-Free Survival After Surgical Resection of Gastrointestinal Stromal Tumors: A Multi-institutional Analysis of 502 Patients. JAMA Surg. 2015, 150, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Multidisciplinary Larynx Cancer Working Group; Sheu, T.; Vock, D.M.; Mohamed, A.S.R.; Gross, N.; Mulcahy, C.; Zafereo, M.; Gunn, G.B.; Garden, A.; Sevak, P.; et al. Conditional Survival Analysis of Patients with Locally Advanced Laryngeal Cancer: Construction of a Dynamic Risk Model and Clinical Nomogram. Sci. Rep. 2017, 7, 43928. [Google Scholar]
- Kang, M.; Park, J.Y.; Jeong, C.W.; Hwang, E.C.; Song, C.; Hong, S.H.; Kwak, C.; Chung, J.; Sung, H.H.; Jeon, H.G.; et al. Changeable Conditional Survival Rates and Associated Prognosticators in Patients with Metastatic Renal Cell Carcinoma Receiving First Line Targeted Therapy. J. Urol. 2018, 200, 989–995. [Google Scholar] [CrossRef]
- Liu, X.; Wu, T.; Zhu, S.Y.; Shi, M.; Su, H.; Wang, Y.; He, X.; Xu, L.-M.; Yuan, Z.-Y.; Zhang, L.-L.; et al. Risk-Dependent Conditional Survival and Failure Hazard After Radiotherapy for Early-Stage Extranodal Natural Killer/T-Cell Lymphoma. JAMA Netw. Open 2019, 2, e190194. [Google Scholar] [CrossRef] [PubMed]
- Narita, S.; Nomura, K.; Hatakeyama, S.; Takahashi, M.; Sakurai, T.; Kawamura, S.; Hoshi, S.; Ishida, M.; Kawaguchi, T.; Ishidoya, S.; et al. Changes in conditional net survival and dynamic prognostic factors in patients with newly diagnosed metastatic prostate cancer initially treated with androgen deprivation therapy. Cancer Med. 2019, 8, 6566–6577. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Cai, J.; Huang, Y.; Luo, J. Ultra-sensitive DNAzyme-based optofluidic biosensor with liquid crystal-Au nanoparticle hybrid amplification for molecular detection. Sens. Actuators B Chem. 2022, 359, 131608. [Google Scholar]
- Zahed, M.A.; Yoon, H.; Sharifuzzaman, M.; Yoon, S.H.; Kim, D.K.; Do Shin, Y.; Asaduzzaman, M.; Park, J.Y. Nanoporous Carbon-Based Wearable Hybrid Biosensing Patch for Real-Time and in Vitro Healthcare Monitoring. In Proceedings of the 2022 IEEE 35th International Conference on Micro Electro Mechanical Systems Conference (MEMS), Tokyo, Japan, 9–13 January 2022. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 60 | 120 | 180 | 240 | 300 | 360 | ||
|---|---|---|---|---|---|---|---|
| Overall (1450 alerts) | |||||||
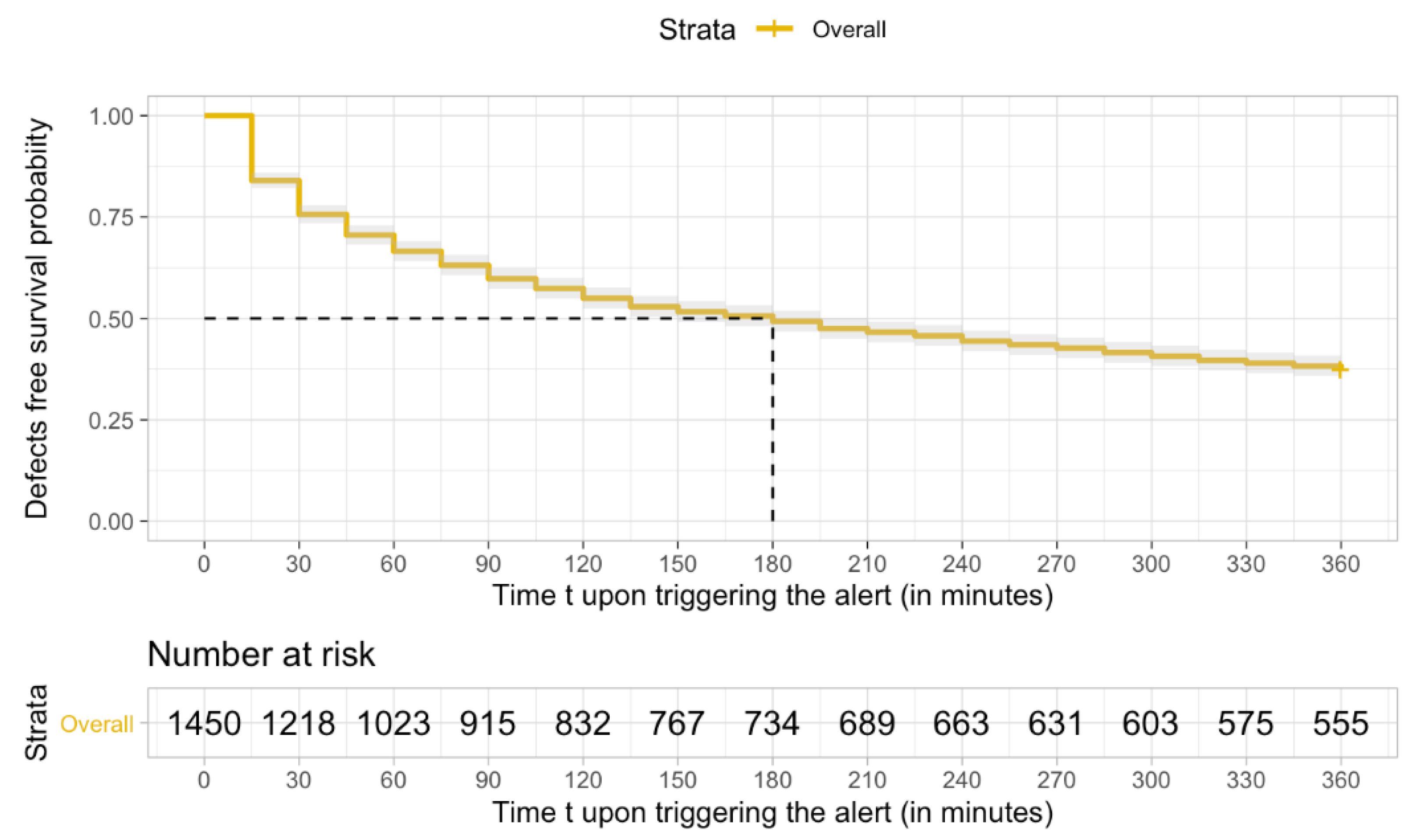
| 0 | 0.67 (0.64, 0.69) | 0.55 (0.52, 0.57) | 0.49 (0.47, 0.52) | 0.44 (0.42, 0.47) | 0.41 (0.38, 0.43) | 0.37 (0.35, 0.4) | |
| 60 | – | 0.83 (0.8, 0.85) | 0.74 (0.71, 0.77) | 0.67 (0.63, 0.7) | 0.61 (0.58, 0.64) | 0.56 (0.53, 0.59) | |
| 120 | – | – | 0.9 (0.87, 0.92) | 0.81 (0.78, 0.84) | 0.74 (0.71, 0.77) | 0.68 (0.64, 0.71) | |
| 180 | – | – | – | 0.9 (0.87, 0.92) | 0.83 (0.79, 0.85) | 0.76 (0.72, 0.79) | |
| 240 | – | – | – | – | 0.92 (0.89, 0.94) | 0.84 (0.81, 0.87) | |
| 300 | – | – | – | – | – | 0.92 (0.89, 0.94) | |
| 60 | 120 | 180 | 240 | 300 | 360 | ||
|---|---|---|---|---|---|---|---|
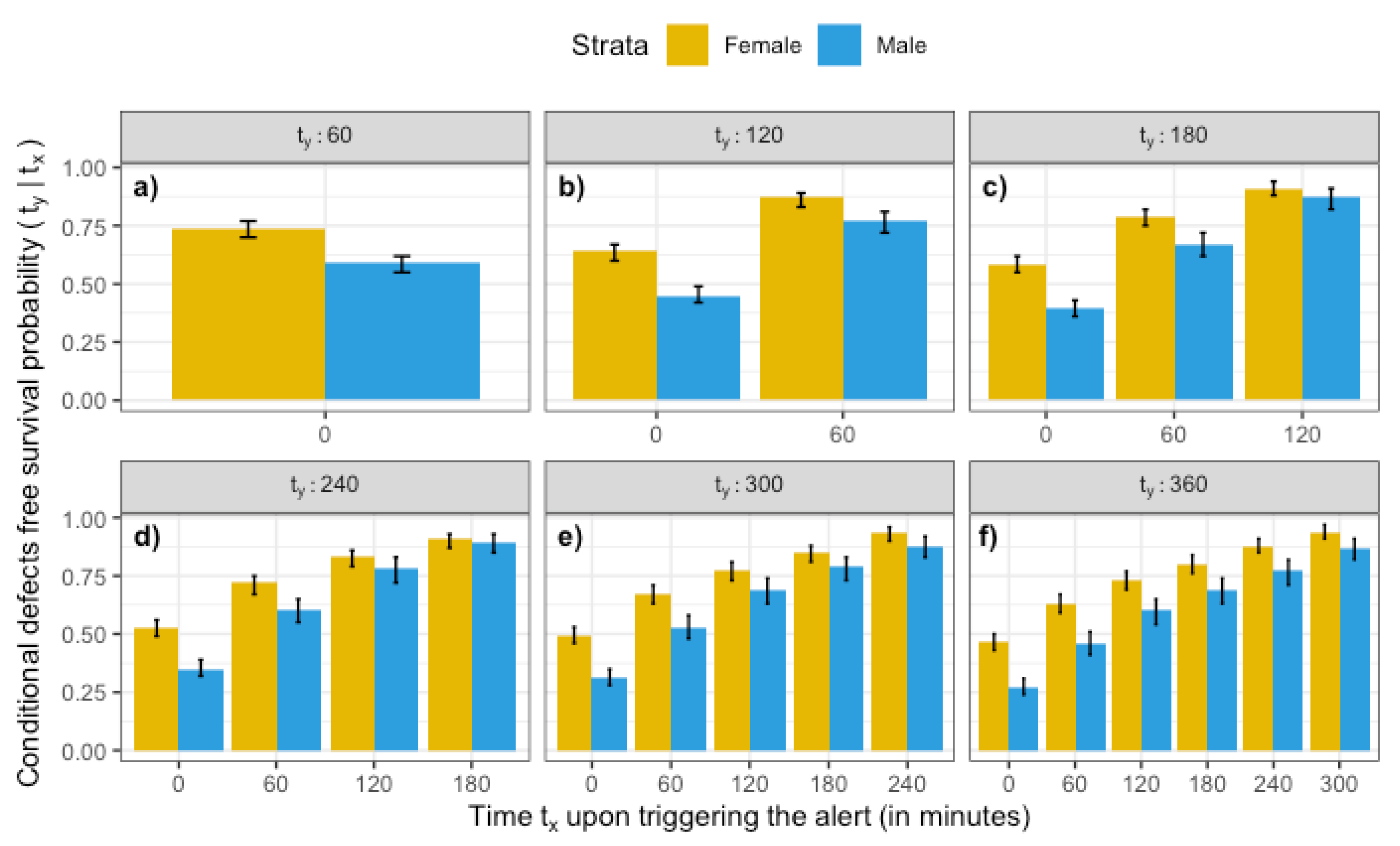
| Female (759 alerts) | |||||||
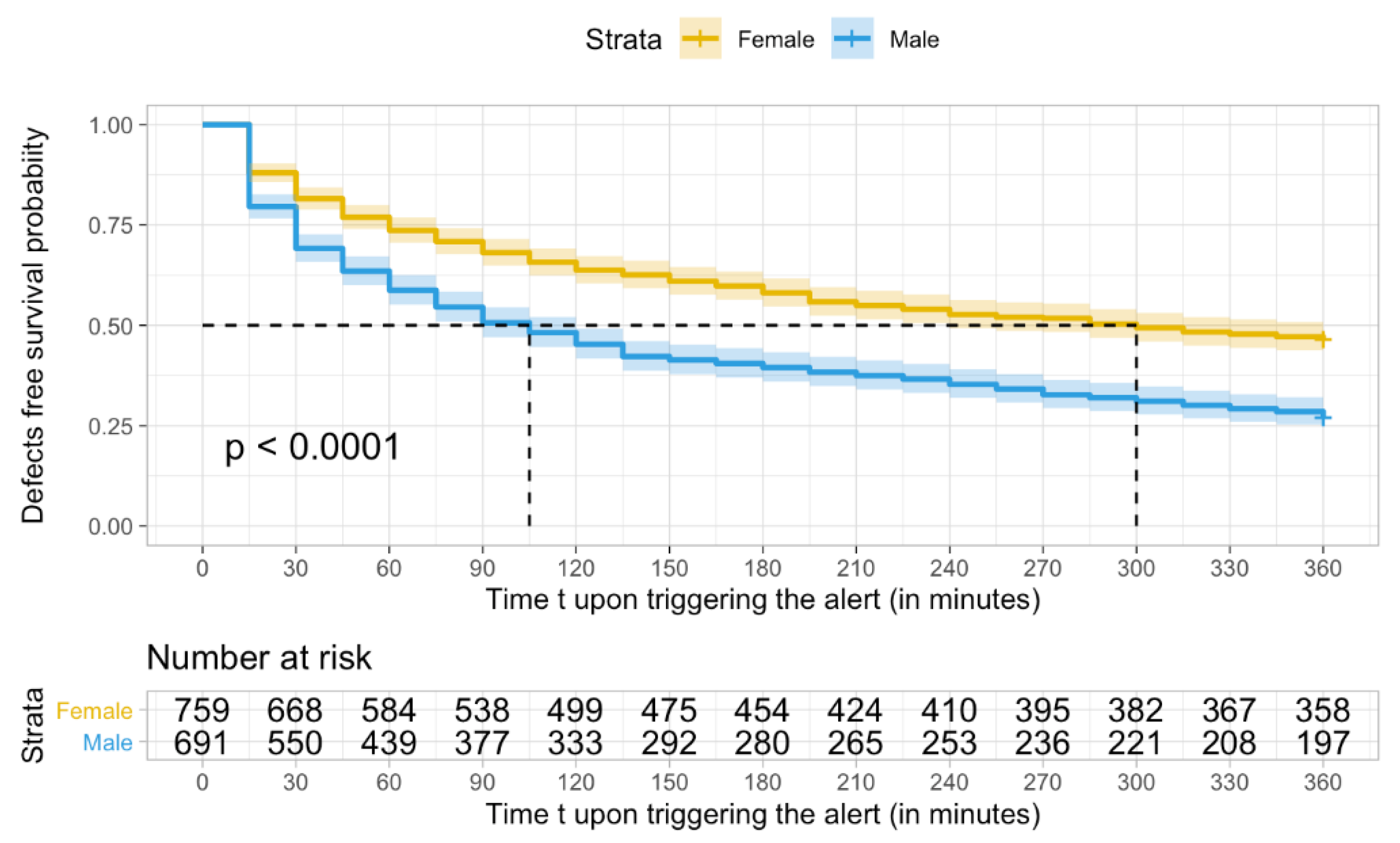
| 0 | 0.74 (0.7, 0.77) | 0.64 (0.6, 0.67) | 0.58 (0.55, 0.62) | 0.53 (0.49, 0.56) | 0.49 (0.46, 0.53) | 0.47 (0.43, 0.5) | |
| 60 | – | 0.87 (0.83, 0.89) | 0.79 (0.75, 0.82) | 0.72 (0.67, 0.75) | 0.67 (0.63, 0.71) | 0.63 (0.59, 0.67) | |
| 120 | – | – | 0.91 (0.88, 0.94) | 0.83 (0.79, 0.86) | 0.77 (0.73, 0.81) | 0.73 (0.69, 0.77) | |
| 180 | – | – | – | 0.91 (0.87, 0.93) | 0.85 (0.81, 0.88) | 0.8 (0.76, 0.84) | |
| 240 | – | – | – | – | 0.94 (0.9, 0.96) | 0.88 (0.85, 0.91) | |
| 300 | – | – | – | – | – | 0.94 (0.91, 0.97) | |
| Male (691 alerts) | |||||||
| 0 | 0.59 (0.55, 0.62) | 0.45 (0.42, 0.49) | 0.4 (0.36, 0.43) | 0.35 (0.32, 0.39) | 0.31 (0.28, 0.35) | 0.27 (0.24, 0.31) | |
| 60 | – | 0.77 (0.72, 0.81) | 0.67 (0.62, 0.72) | 0.6 (0.55, 0.65) | 0.53 (0.48, 0.58) | 0.46 (0.41, 0.51) | |
| 120 | – | – | 0.87 (0.82, 0.91) | 0.78 (0.72, 0.83) | 0.69 (0.63, 0.74) | 0.6 0(.54, 0.65) | |
| 180 | – | – | – | 0.89 (0.85, 0.93) | 0.79 (0.73, 0.83) | 0.69 (0.63, 0.74) | |
| 240 | – | – | – | – | 0.88 (0.83, 0.92) | 0.77 (0.71, 0.82) | |
| 300 | – | – | – | – | – | 0.87 (0.82, 0.91) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marshall, A.H.; Novakovic, A. Process Mining the Performance of a Real-Time Healthcare 4.0 Systems Using Conditional Survival Models. Algorithms 2022, 15, 196. https://doi.org/10.3390/a15060196
Marshall AH, Novakovic A. Process Mining the Performance of a Real-Time Healthcare 4.0 Systems Using Conditional Survival Models. Algorithms. 2022; 15(6):196. https://doi.org/10.3390/a15060196
Chicago/Turabian StyleMarshall, Adele H., and Aleksandar Novakovic. 2022. "Process Mining the Performance of a Real-Time Healthcare 4.0 Systems Using Conditional Survival Models" Algorithms 15, no. 6: 196. https://doi.org/10.3390/a15060196
APA StyleMarshall, A. H., & Novakovic, A. (2022). Process Mining the Performance of a Real-Time Healthcare 4.0 Systems Using Conditional Survival Models. Algorithms, 15(6), 196. https://doi.org/10.3390/a15060196