
Design of a Lower Limb Exoskeleton: Robust Control, Simulation and Experimental Results

 , ,
, , 
Abstract
:1. Introduction
- Passive rehabilitation: does not involve movement by the patient themself.
- Active rehabilitation: involves the participation of the patient, who is the one performing the movement.
- Sprains of Grade 1. They cause little ligament injury. Despite the fact that it has been considerably stretched, it could still aid in preserving the stability of the knee joint.
- Sprains of Grade 2. The ligament is stretched to the point of becoming loose. This is frequently referred to as a partial ligament tear.
- Sprains of Grade 3. This is a total ligament tear. The knee joint is unstable because the ligament has been split in half.
2. Motion Analysis for Acl Injury Rehabilitation
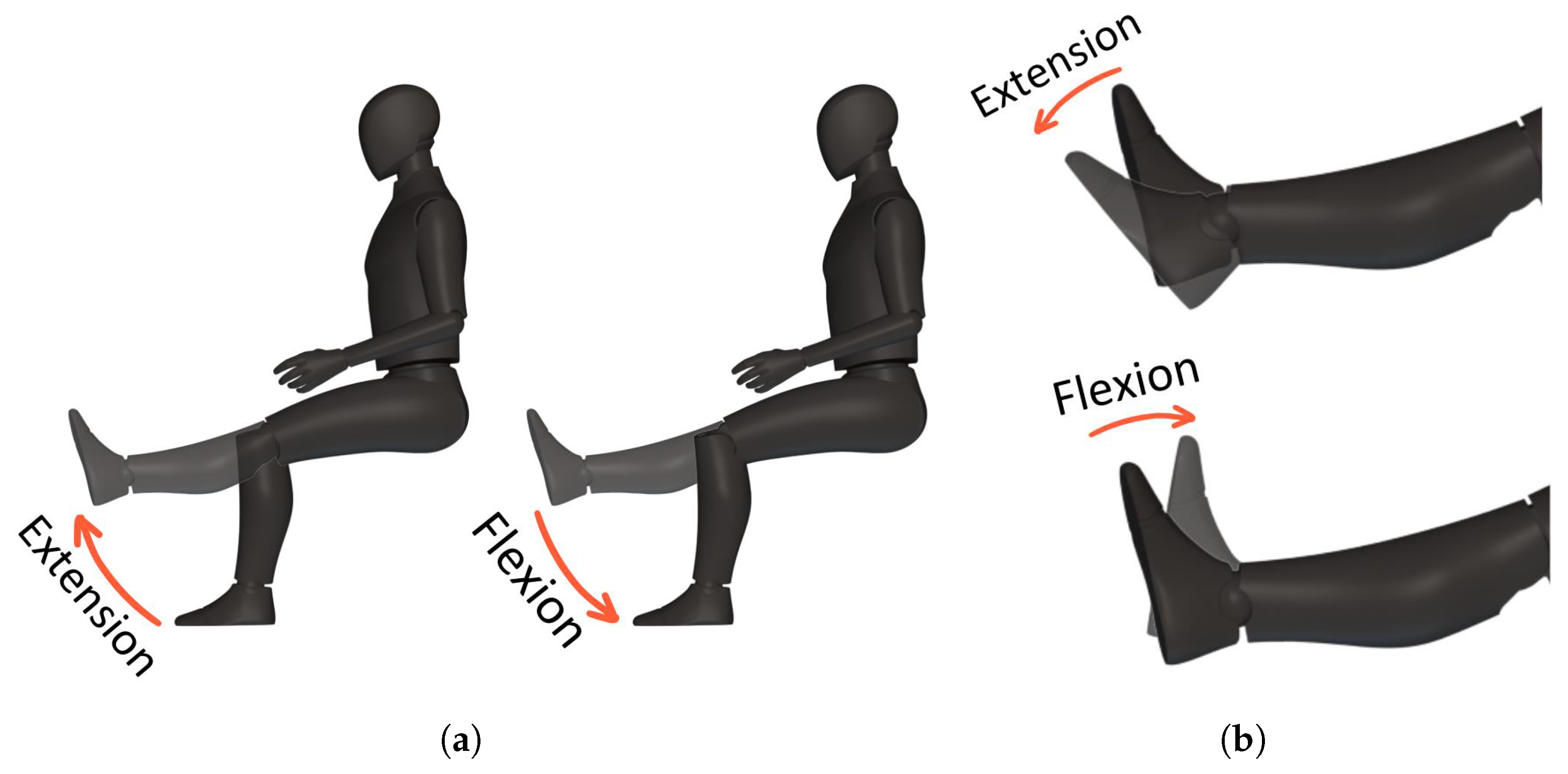
2.1. Motion Required by the Prototype
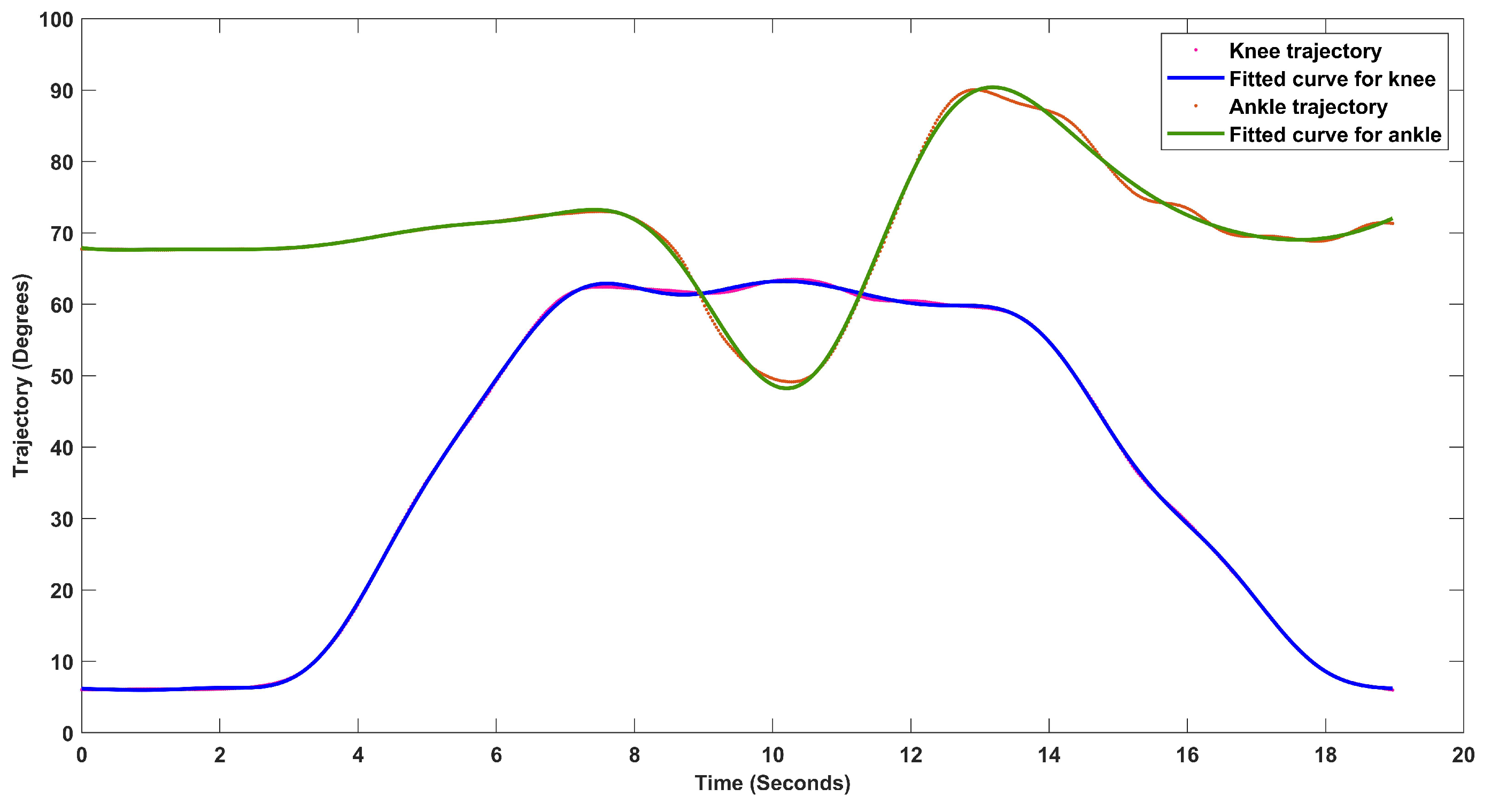
2.2. Development of Trajectories of Motion
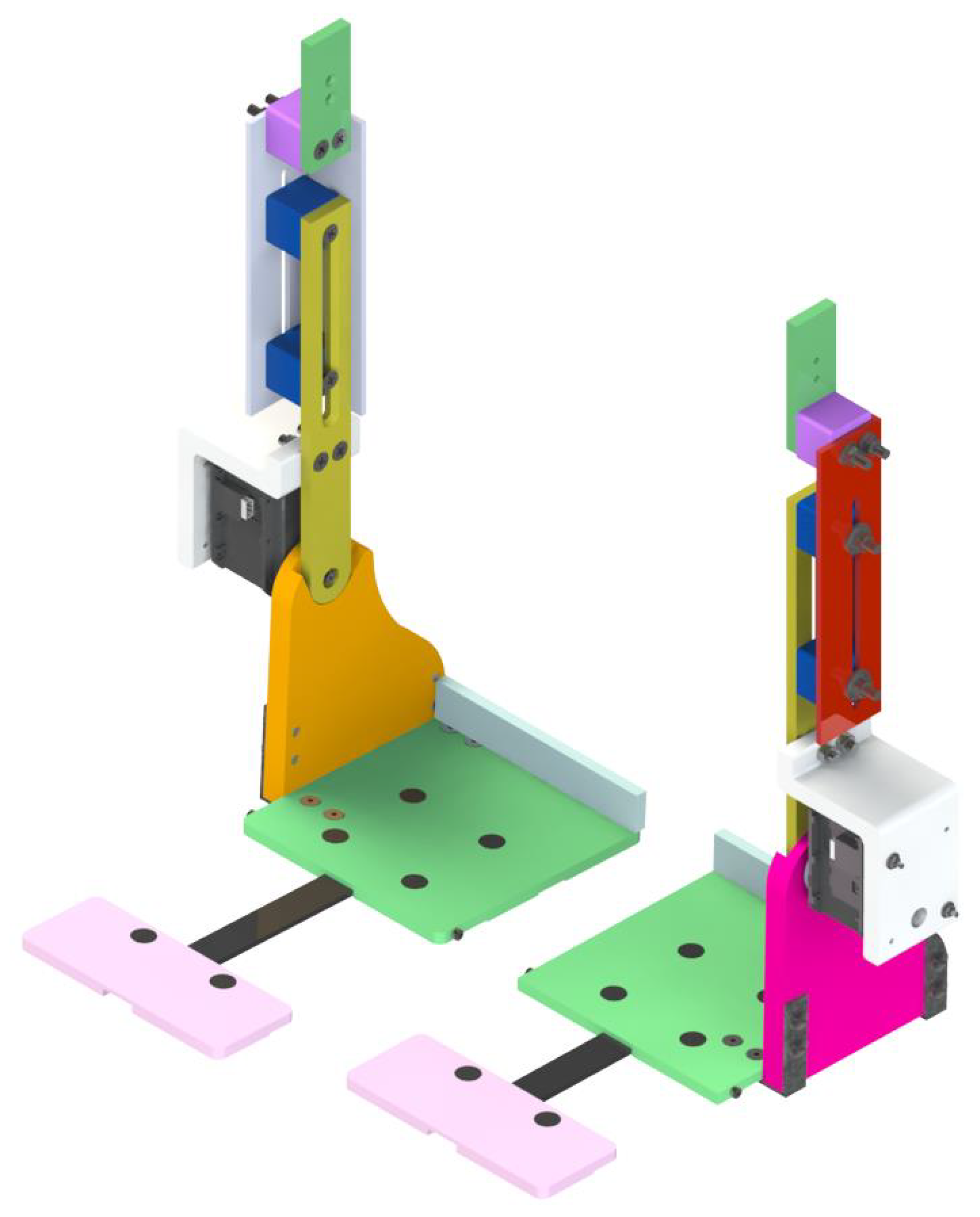
3. Mechanical Design of the Prototype
- Adjust the sizes to the Latin American population;
- Compact structure;
- Passive rehabilitation;
- Add mechanical stops to prevent hyperextension of the joints;
- The design must be ergonomic and easy to place.
3.1. Ankle Joint Prototype
3.1.1. Stress Analysis
3.1.2. Selection of the Motors
- The axes of the actuators are aligned with the axes of the joints.
- The wearer does not apply muscular force.
3.2. Exoskeleton for Acl Injury Rehabilitation
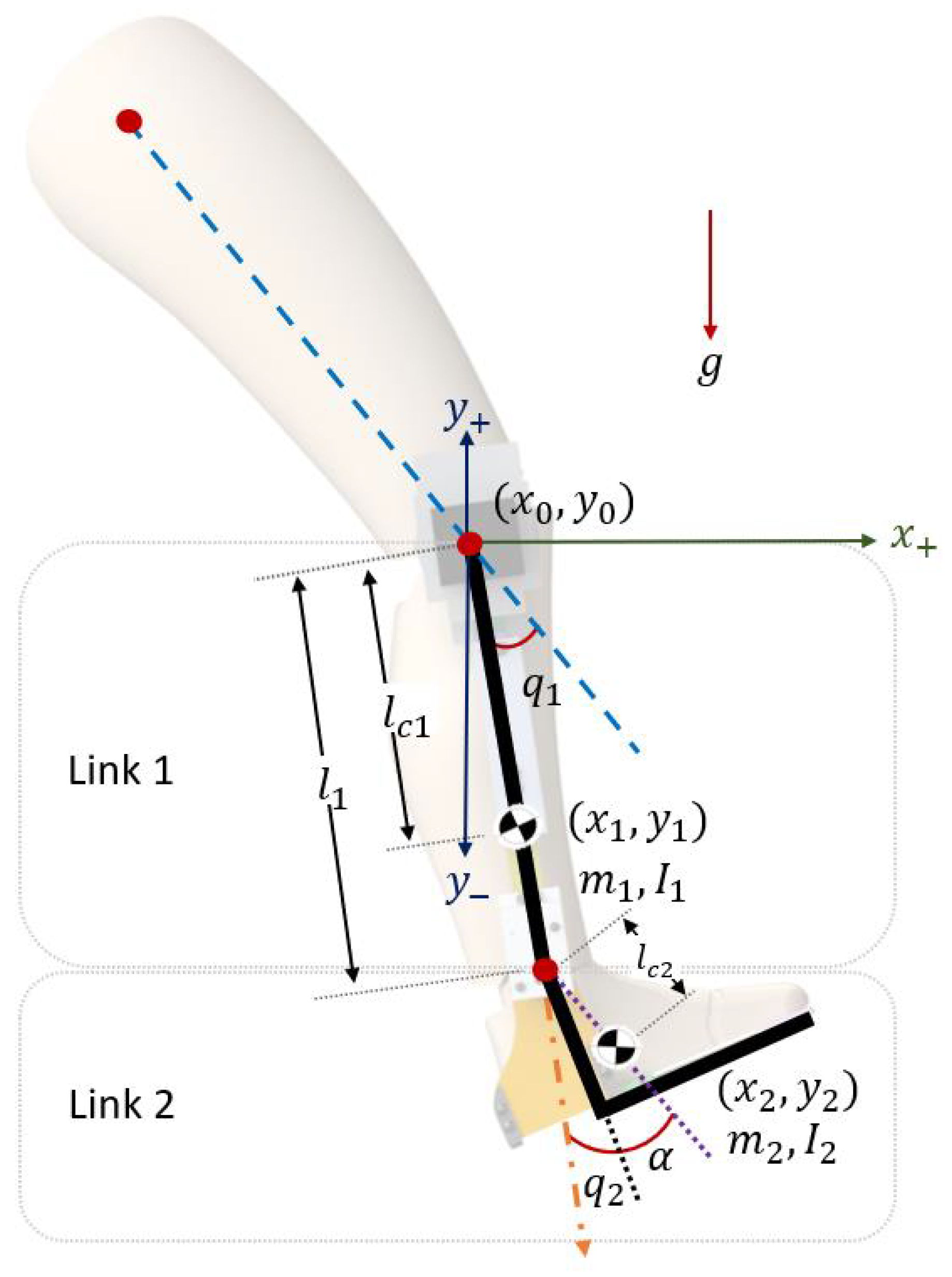
4. Mathematical Model
Dynamic Model
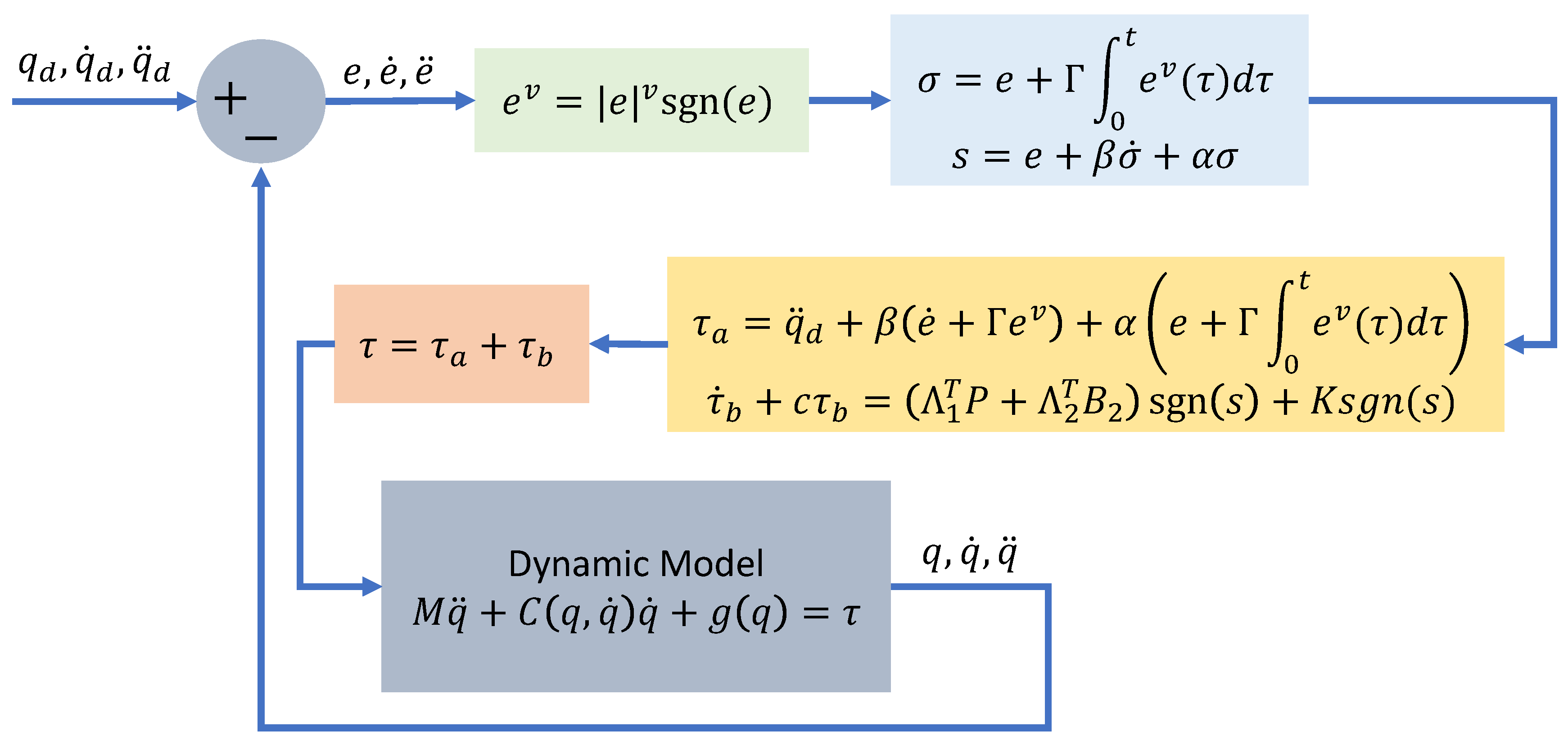
5. Control Algorithm
5.1. Control Algorithm
5.2. Stability Analysis
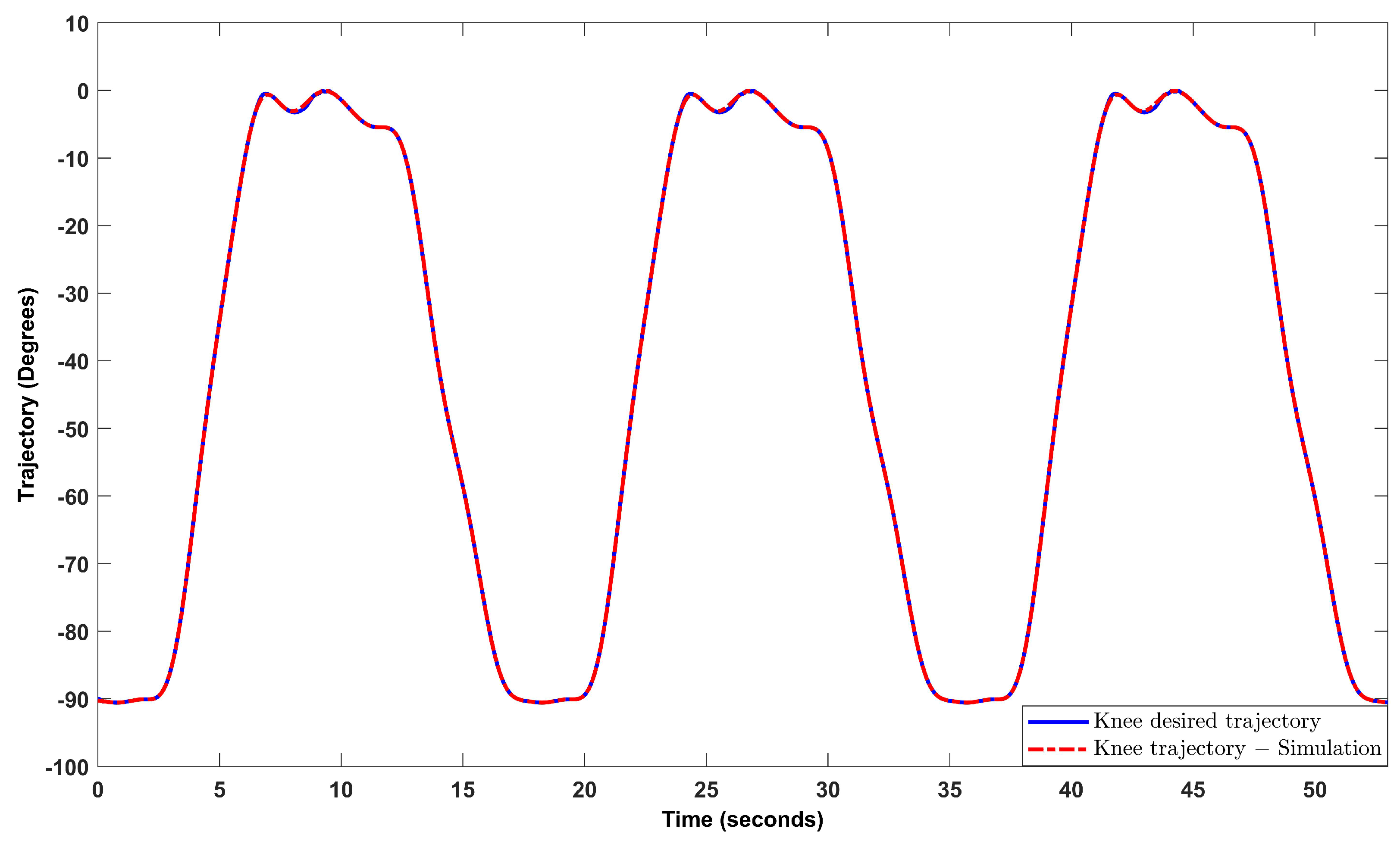
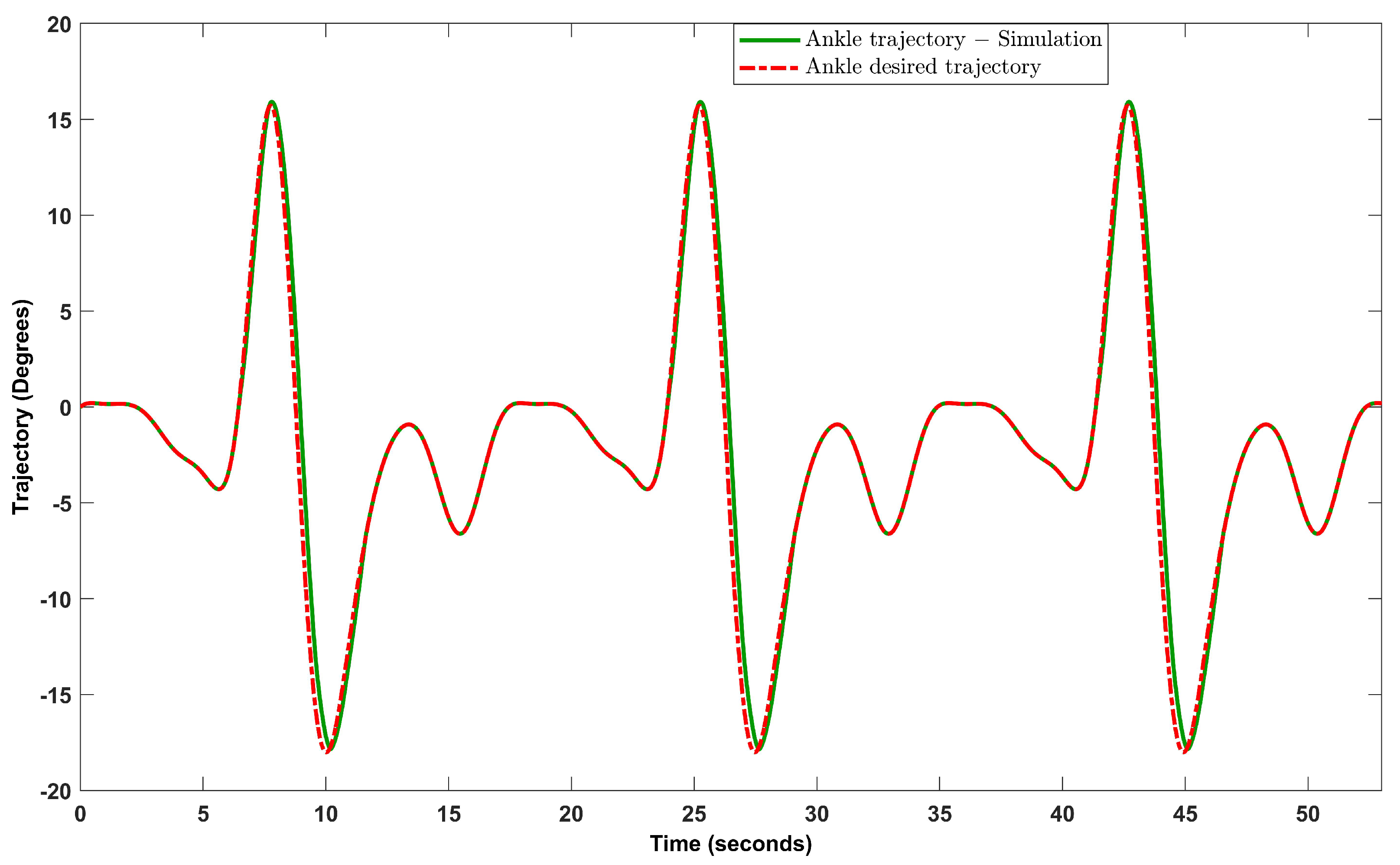
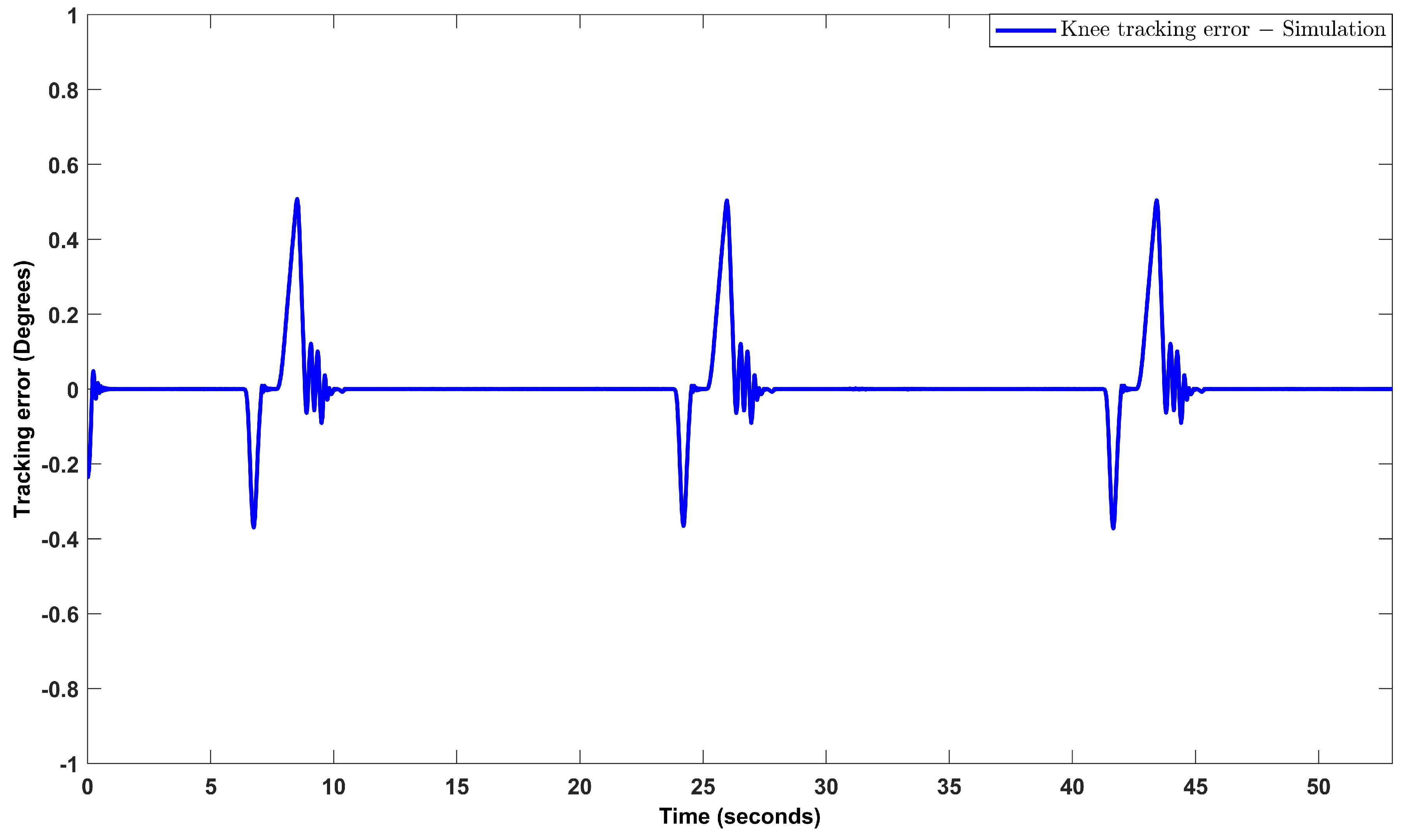
6. Results
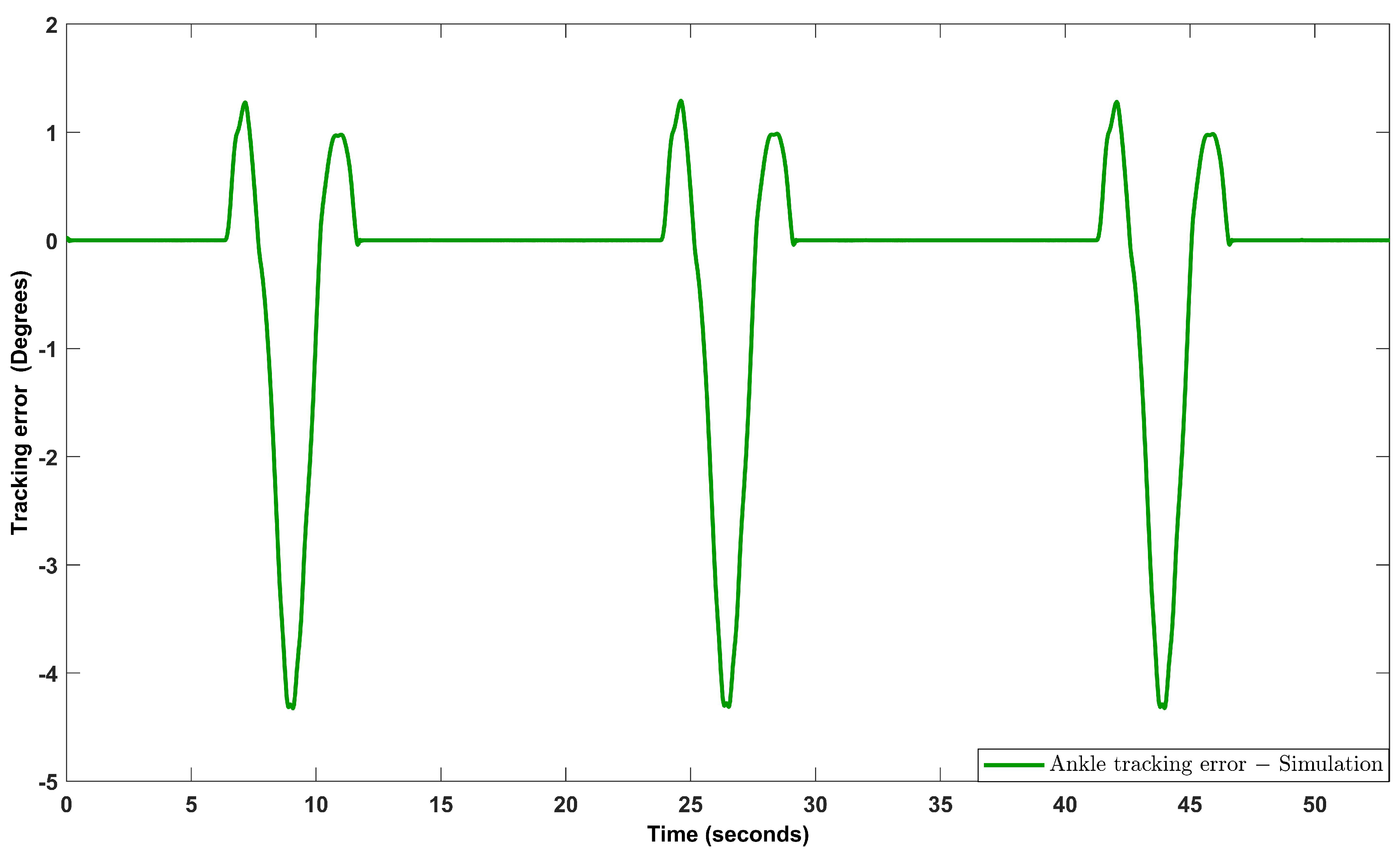
6.1. Numerical Results
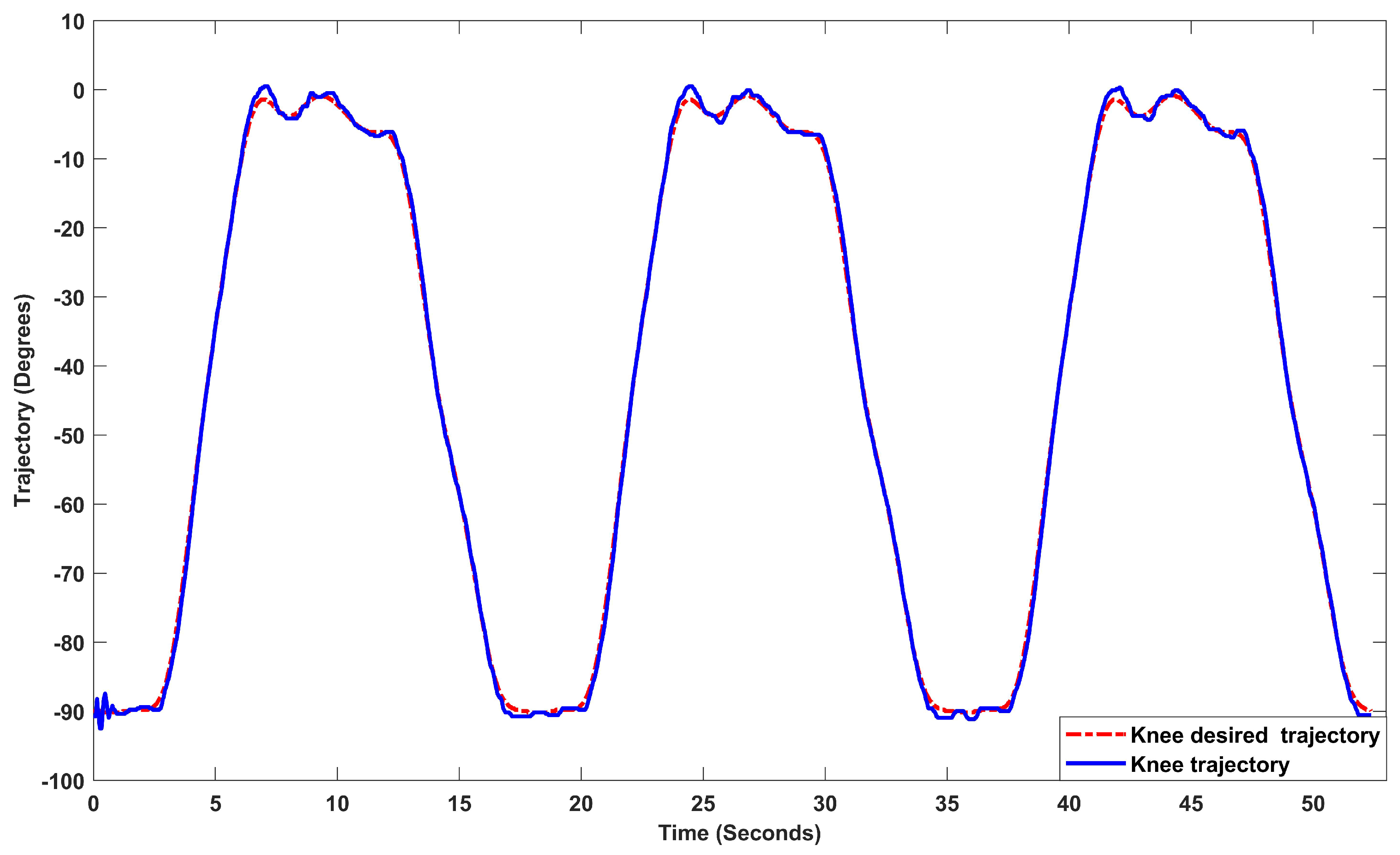
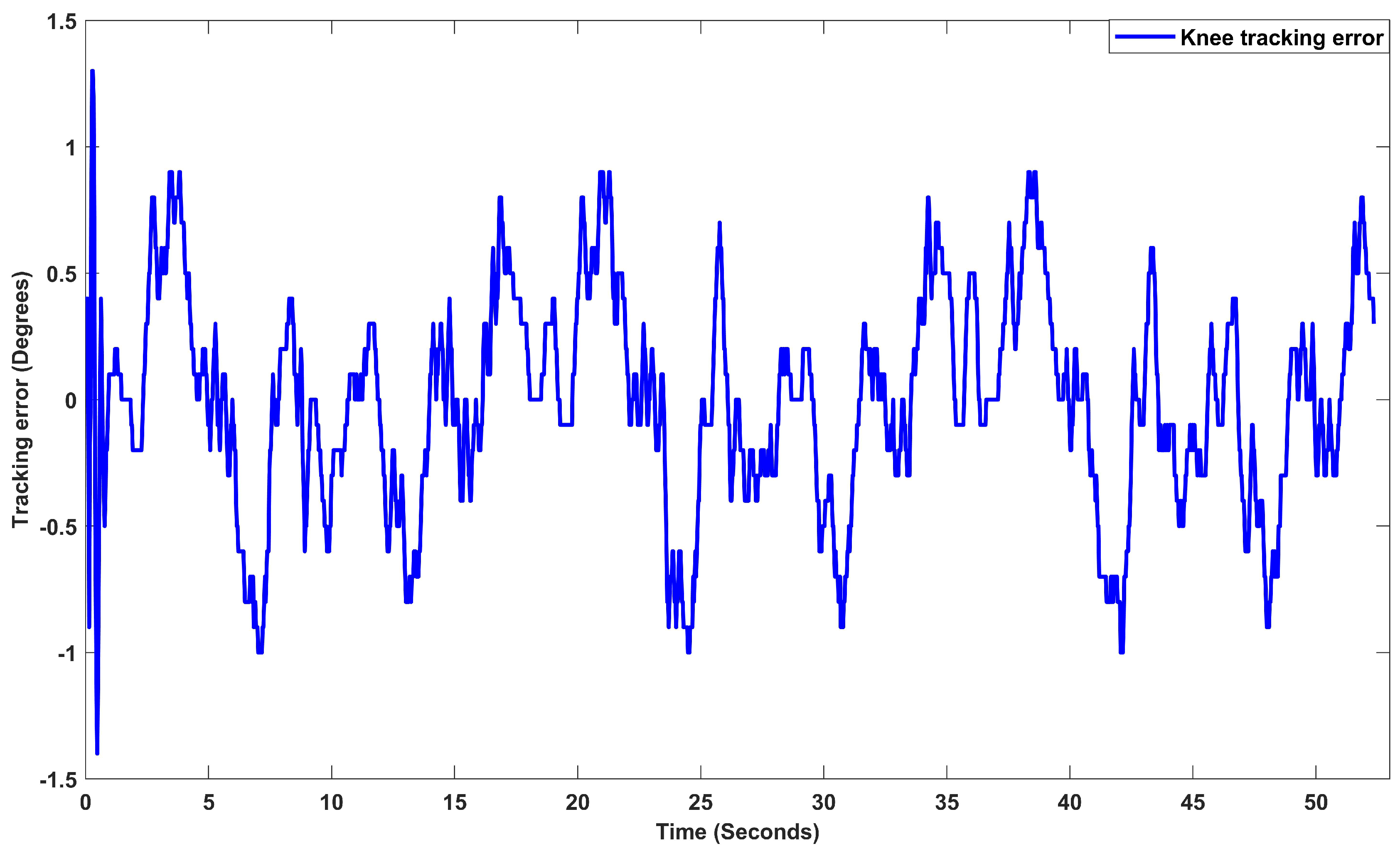
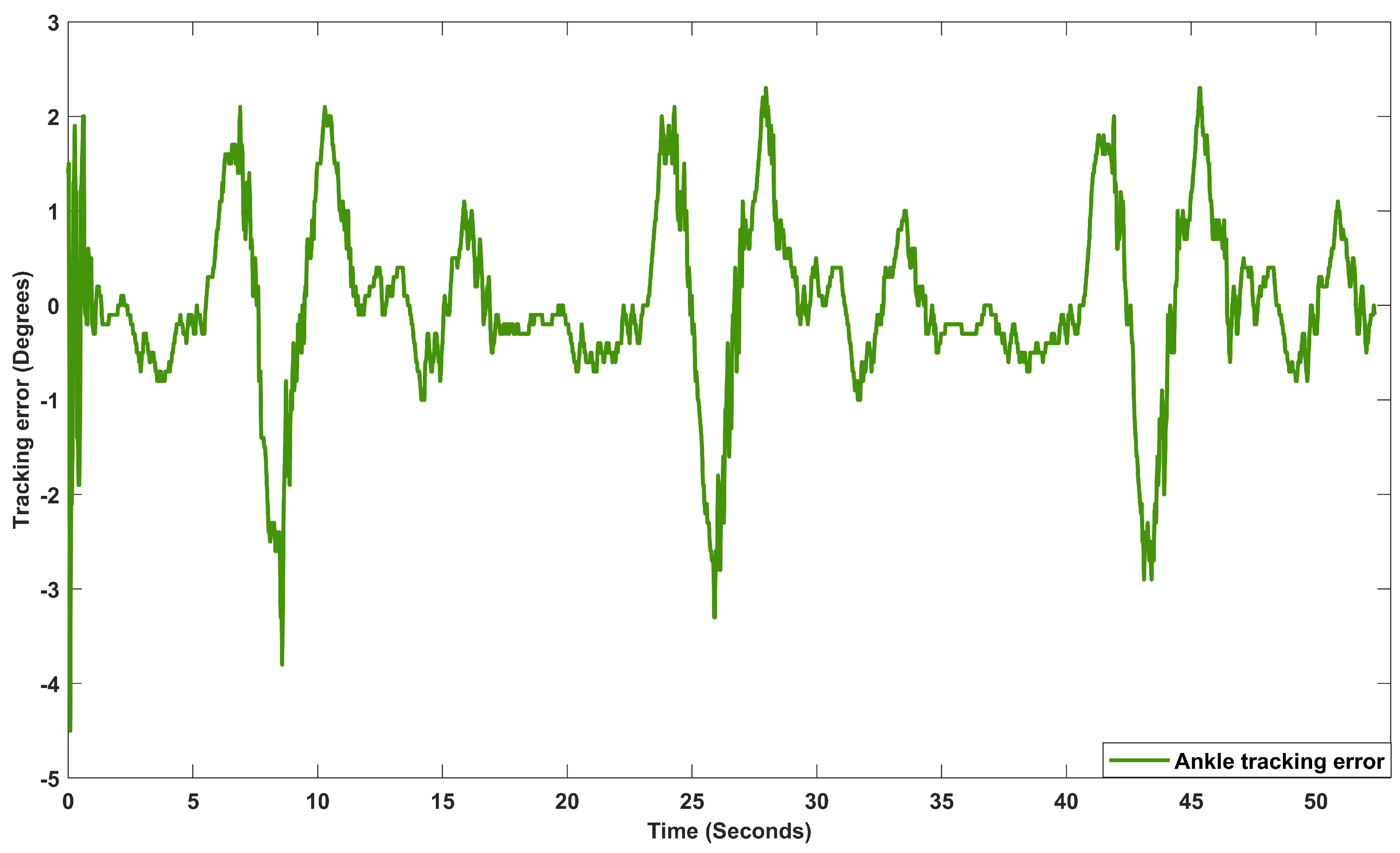
6.2. Experimental Results
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larwa, J.; Stoy, C.; Chafetz, R.S.; Boniello, M.; Franklin, C. Stiff Landings, Core Stability, and Dynamic Knee Valgus: A Systematic Review on Documented Anterior Cruciate Ligament Ruptures in Male and Female Athletes. Int. J. Environ. Res. Public Health 2021, 18, 3826. [Google Scholar] [CrossRef] [PubMed]
- D’Isanto, T.; D’Elia, F.; Esposito, G.; Altavilla, G.; Raiola, G. Examining the Effects of Mirror Therapy on Psychological Readiness and Perception of Pain in ACL-Injured Female Football Players. J. Funct. Morphol. Kinesiol. 2022, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Zhen, T.; Yan, L.Y.P. Walking Gait Phase Detection Based on Acceleration Signals Using LSTM-DNN Algorithm. Algorithms 2019, 12, 253. [Google Scholar] [CrossRef]
- Tarnacka, B.; Korczyński, B.; Frasuńska, J. Impact of Robotic-Assisted Gait Training in Subacute Spinal Cord Injury Patients on Outcome Measure. Diagnostics 2023, 13, 1966. [Google Scholar] [CrossRef] [PubMed]
- Sarajchi, M.; Sirlantzis, K. Design and Control of a Single-Leg Exoskeleton with Gravity Compensation for Children with Unilateral Cerebral Palsy. Sensors 2023, 23, 6103. [Google Scholar] [CrossRef] [PubMed]
- Tamantini, C.; Cordella, F.; Lauretti, C.; Di Luzio, F.S.; Campagnola, B.; Cricenti, L.; Bravi, M.; Bressi, F.; Draicchio, F.; Sterzi, S.; et al. Tailoring upper-limb robot-aided orthopedic rehabilitation on patients’ psychophysiological state. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 3297–3306. [Google Scholar] [CrossRef] [PubMed]
- Pezeshki, L.; Sadeghian, H.; Keshmiri, M.; Chen, X.; Haddadin, S. Cooperative Assist-as-Needed Control for Robotic Rehabilitation: A Two-Player Game Approach. IEEE Robot. Autom. Lett. 2023, 8, 2852–2859. [Google Scholar] [CrossRef]
- Goo, A.C.; Wiebrecht, J.J.; Wajda, D.A.; Sawicki, J.T. Human Factors Assessment of a Novel Pediatric Lower-Limb Exoskeleton. Robotics 2023, 12, 26. [Google Scholar] [CrossRef]
- Rosales-Luengas, Y.; Espinosa-Espejel, K.I.; Lopéz-Gutiérrez, R.; Salazar, S.; Lozano, R. Lower Limb Exoskeleton for Rehabilitation with Flexible Joints and Movement Routines Commanded by Electromyography and Baropodometry Sensors. Sensors 2023, 23, 5252. [Google Scholar] [CrossRef] [PubMed]
- Huo, W.; Mohammed, S.; Moreno, J.C.; Amirat, Y. Lower limb wearable robots for assistance and rehabilitation: A state of the art. IEEE Syst. J. 2014, 10, 1068–1081. [Google Scholar] [CrossRef]
- Lee, H.; Ferguson, P.W.; Rosen, J. Lower limb exoskeleton systems—Overview. In Wearable Robotics; Academic Press: Cambridge, MA, USA, 2020; pp. 207–229. [Google Scholar]
- Su, Q.; Pei, Z.; Tang, Z.; Liang, Q. Design and Analysis of a Lower Limb Loadbearing Exoskeleton. Actuators 2022, 11, 285. [Google Scholar] [CrossRef]
- Pană, C.F.; Popescu, D.; Rădulescu, V.M. Patent Review of Lower Limb Rehabilitation Robotic Systems by Sensors and Actuation Systems Used. Sensors 2023, 23, 6237. [Google Scholar] [CrossRef] [PubMed]
- Young, A.J.; Ferris, D.P. State of the Art and Future Directions for Lower Limb Robotic Exoskeletons. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Olguin-Roque, J.; Salazar, S.; González-Hernandez, I.; Lozano, R. A Robust Fixed-Time Sliding Mode Control for Quadrotor UAV. Algorithms 2023, 16, 229. [Google Scholar] [CrossRef]
- Saim, A.; Haoping, W.; Tian, Y. Adaptive Fractional High-order Terminal Sliding Mode Control for Nonlinear Robotic Manipulator under Alternating Loads. Asian J. Control. 2021, 23, 1900–1910. [Google Scholar] [CrossRef]
- Hernández, J.H.; Cruz, S.S.; López-Gutiérrez, R.; González-Mendoza, A.; Lozano, R. Robust nonsingular fast terminal sliding-mode control for Sit-to-Stand task using a mobile lower limb exoskeleton. Control. Eng. Pract. 2020, 101, 104496. [Google Scholar] [CrossRef]
- Siegler, S.; Chen, J.; Schneck, C. The three-dimensional kinematics and flexibility characteristics of the human ankle and subtalar joints—Part I: Kinematics. J. Biomech. Eng. 1988, 110, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Roach, K.E.; Miles, T.P. Normal hip and knee active range of motion: The relationship to age. Phys. Ther. 1991, 71, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Tsoi, Y.H.; Xie, S.Q. Design and control of a parallel robot for ankle rehabilitation. Int. J. Intell. Syst. Technol. Appl. 2010, 8, 100–113. [Google Scholar] [CrossRef]
- Zhihong, M.; O’day, M.; Yu, X. A robust adaptive terminal sliding mode control for rigid robotic manipulators. J. Intell. Robot. Syst. 1999, 24, 23–41. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ROM of the Human | ROM of the Robot | |||
|---|---|---|---|---|
| Joint | Minimum Angle | Maximum Angle | Minimum Angle | Maximum Angle |
| Knee | ||||
| Ankle | ||||
| Dimension | Maximum | Minimum |
|---|---|---|
| Length of the calf | 40 cm | 48 cm |
| Length of the foot | 17 cm | 27 cm |
| Parameter | Variable | Value |
|---|---|---|
| Mass of the link 1 | kg | |
| Mass of Link 2 | kg | |
| Center of mass of Link 1 | m | |
| Center of mass of Link 2 | m | |
| Length of Link 1 | m | |
| Inertia of Link 1 | kg · m | |
| Inertia of Link 2 | kg · m | |
| Alpha |
| Parameter | Variable | Value |
|---|---|---|
| Alpha | ||
| Beta | 20 | |
| Gamma | diag | |
| v | v | |
| K | k | diag |
| c | c | |
| P | p | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salcido, E.A.A.; Centeno-Barreda, D.; Rosales, Y.; Lopéz-Gutiérrez, R.; Salazar, S.; Lozano, R. Design of a Lower Limb Exoskeleton: Robust Control, Simulation and Experimental Results. Algorithms 2023, 16, 449. https://doi.org/10.3390/a16090449
Salcido EAA, Centeno-Barreda D, Rosales Y, Lopéz-Gutiérrez R, Salazar S, Lozano R. Design of a Lower Limb Exoskeleton: Robust Control, Simulation and Experimental Results. Algorithms. 2023; 16(9):449. https://doi.org/10.3390/a16090449
Chicago/Turabian StyleSalcido, E. Anyuli Alvarez, Daniel Centeno-Barreda, Yukio Rosales, Ricardo Lopéz-Gutiérrez, Sergio Salazar, and Rogelio Lozano. 2023. "Design of a Lower Limb Exoskeleton: Robust Control, Simulation and Experimental Results" Algorithms 16, no. 9: 449. https://doi.org/10.3390/a16090449
APA StyleSalcido, E. A. A., Centeno-Barreda, D., Rosales, Y., Lopéz-Gutiérrez, R., Salazar, S., & Lozano, R. (2023). Design of a Lower Limb Exoskeleton: Robust Control, Simulation and Experimental Results. Algorithms, 16(9), 449. https://doi.org/10.3390/a16090449