3. Materials and Methods
The study on childhood clinical manifestations was conducted by retrospectively analyzing data from 402 medical records of children hospitalized with stroke in the Neurology Departments of the Institute of Mother and Child PHMI (IMSP IMC) and the Clinical Hospital No. 1 PHMI (IMSP SCM) from 2010 to 2016. Additionally, prospective data from 108 children with stroke collected from 2017 to 2020 were included. A comprehensive analysis of clinical manifestations from both retrospective and prospective data was performed to obtain reliable statistical results. The analysis aimed to evaluate symptoms indicative of ischemic stroke in children of different ages using a logistic regression analysis, chosen to determine the relationship between triggering symptoms and stroke and establish algorithms for timely recognition and prediction of stroke.
This study employed a prognostic cohort design to estimate the incidence of pediatric stroke and assess its prognostic outcomes. The sample size was calculated based on the estimated incidence rate of pediatric stroke (p = 0.0075) and the desired confidence level and margin of error. With adjustments for design effect and non-response rate, a representative sample of 53 children with IS was included in the study. The research was conducted in consecutive stages, with the first stage comprising the full descriptive study, focusing on analyzing incidence, morbidity, and mortality rates, as well as the distribution of IS cases by various factors. The second stage was a prognostic cohort study, which aimed to assess the incidence of pediatric stroke and its prognostic outcomes.
The following types of studies were conducted:
Full descriptive study—to analyze the incidence, prevalence, disability, and mortality rates in children who experienced acute stroke between 2010 and February 2020
Prognostic cohort study:
p is the incidence of pediatric stroke, estimated by the statistical frequency of IS in children and newborns in the population 2–13/100,000; it is on average p = 0.0075;
Z = 1.96 for the 95.0% confidence interval;
e = 0.03 is the accepted error;
n = 0.0075 × 0.9925 (1.96/0.03)2 = 31.74; n × design effect (1.5) = 47.6 and with a 10.0% non-response rate, so a representative sample size has to include 53 children with IS.
The scientific research was carried out consecutively in several stages.
Stage I included the full descriptive study (2010–2020). Data were assessed by the IBM SPSS Statistics 26 program. This study involved a comprehensive examination of the evolutionary aspects and structure of neonatal and pediatric ischemic stroke (IS) in the Republic of Moldova from 2010 to 2020. It included retrospective and prospective observational analytical studies on incidence, morbidity, and mortality, conducted at the Pediatric Neurology Clinic of the Department of Pediatrics of the PI USMF Nicolae Testemițanu, along with relevant sections within IMSP IMC and IMSP SCM No. 1. The analysis covered the distribution of IS cases across different regions of the Republic of Moldova, as well as by age and gender. Furthermore, the study analyzed the profile of determinants involved in initiating IS in the pediatric population of the Republic of Moldova, categorized by age category. The estimation of cases diagnosed with neonatal IS and pediatric IS from 2010 to 2020 (totaling 510 children) was conducted, considering evolving clinical and paraclinical manifestations.
In stage II, the prognostic study was conducted in two directions: (1) on pregnant women at risk of giving birth to children with IS, involving 153 pregnant women, and (2) on a group of children who suffered acute IS, totaling 108 children.
The first study aimed to analyze the results of examinations of pregnant women using both non-invasive (fetal ultrasonography and biochemical screening: double/triple test) and invasive (amniocentesis with fetal karyotype study) prenatal diagnosis methods. These examinations were performed at the Center for Reproductive Health and Medical Genetics under the National Program for the Evaluation of Pregnant Women and Prophylaxis of Hereditary Pathologies. The results from 153 pregnant women who underwent medico-genetic counseling were evaluated to prevent and predict cerebral pathology in children.
Additionally, within the prospective study, children who suffered acute neonatal IS (NIS) or acute pediatric IS (PIS) between 2017 and 2020 (108 children) were identified. This study allowed for the highlighting and specification of the clinical–paraclinical manifestations of NIS and PIS based on the determinants involved (perinatal and postnatal) and the age of the patient. A detailed analysis of prenatal factors associated with the risk of NIS was conducted, estimating the importance of the medical-genetic consultation in such cases. Furthermore, clinical symptoms characteristic of the studied age were elucidated through neurological examination, utilizing the PedNIHSS scale to assess the severity of CNS involvement in IS.
In stage III, an assessment of the prognosis of neurological complications in patients with stroke was conducted. This involved assessing the relationship between determinants involved in stroke, the age of the child, clinical features at the stage of confirming the diagnosis, and the risk of occurrence using mathematical analysis methods for neurological complications. Predictive methods were proposed for the prevention of IS risk and neurological complications in children. Statistical processing of the obtained data was carried out by researching correlations and conducting a multivariate analysis of the causes involved in the development of IS, considering clinical and imaging factors depending on the child’s age to calculate the risk of neurological complications.
Stage IV included the development of algorithms for managing women/families at risk of giving birth to a child with IS and algorithms for the diagnosis and management of newborns and children with IS. Additionally, the National Clinical Protocol for cerebral vascular accidents in children was developed, aiming at prophylaxis, early diagnosis, and definitive treatment of stroke in pediatric patients, for healthcare professionals and the population of the Republic of Moldova.
In the context of the study, the following criteria for inclusion/exclusion of patients served as conceptual and methodological benchmarks:
Criteria for including patients in the study:
Children diagnosed with acute ischemic stroke of various types.
Newborn infants aged between 0 and 28 days.
Children aged between 28 days and 18 years.
Pregnant women.
Availability of informed consent from parents or guardians.
Exclusion criteria from the study:
Children diagnosed with hemorrhagic stroke.
Children diagnosed with venous sinus thrombosis.
Children older than 18 years.
Children with acute craniocerebral trauma.
Premature infants.
Lack of informed consent from parents or guardians.
The research was made possible by the project “Evaluation of incidence, prevalence, risk factors, research of clinical, neuroimaging, neurophysiological, and neurotrophic remedial aspects of cerebrovascular accidents in children” within the state program “Systemogenesis of risk factors, optimization of the medical assistance service, evaluation sustainable and mathematical modeling of Stroke”, considering the cost and methodological difficulties (exceptionally used for scientific purposes) of the method. The project was conducted in the Department of Pediatrics of SUMP “Nicolae Testemițanu”.
Patients underwent examinations in departments specializing in neurological care, the resuscitation department, and neonatal neurology. A periodic observation of patients was conducted as necessary, depending on established diagnoses and the child’s age. Data were recorded in a questionnaire which included information on risk factors, determinants, clinical outcomes following the Amiel-Tison test (for newborns and children up to 3 months), and the pedNIHSS scale (for children over 3 months). Additional examinations such as CT and MRI of the brain, as well as EEG, were utilized to assess functional and structural changes in the brain. These investigations were conducted in inpatient settings. EEGs were performed based on existing indications, and imaging examinations were conducted in 108 children with acute neonatal or pediatric stroke in the prospective study group. The results of these additional investigations facilitated the confirmation of acute stroke diagnosis in children, the assessment of the dimensions of the cerebral ischemic focus, and the evaluation of the disease prognosis.
The participants included in the study, namely, the parents of children with IS, had to complete the Informed Agreement prior to the study. Confidentiality and protection of personal data were ensured by coding all the names and any personal data of the participants, before transferring data into Excel tables. Prior to conducting the study, it was approved by the favorable opinion of the ethics committee no. 69, dated 21 March 2017.
4. Results
The results of the descriptive statistics characterize both studied cohorts, including the retrospectively and the prospectively analyzed patients, as follows: (1) a retrospective analysis of 402 medical records of newborn children (291 children, 57.1%; 95% CI [54.91–59.29]) and those aged between 28 days and 18 years (111 children, 21.8%; 95% CI [19.97–23.63]), diagnosed with neonatal or pediatric ischemic stroke between 2010 and 2016 in the neurology departments of IMSP IMC and IMSP SCM No. 1; and (2) a prospective study from 2017 to 2020 within the same medical institutions, with a sample of 108 children aged 0 to 18 years, distributed by age categories: newborn—71 (65.7%; 95% CI [61.13–70.27]), children aged between 28 days and 18 years (meeting pediatric ischemic stroke criteria)—37 (28.7%; 95% CI [24.35–33.05]), all diagnosed with acute ischemic stroke. To analyze epidemiological aspects, clinical manifestations, and neurological outcomes in both retrospective and prospective studies, data from 510 medical records of childhood acute stroke cases were examined, distributed by age categories: newborn—362 (71%, 95% CI [68.99–73.01]), child—148 (29%, 95% CI [26.99–31.01]). Imaging, neurofunctional, and immunological manifestations were analyzed based on results obtained from the 108 patients with ischemic stroke in the prospective study.
The study of the clinical manifestations of IS in children across different age groups is crucial in this field. IS cases were predominantly diagnosed in newborns, with 362 cases (71%, 95% CI 68.99–73.01), while 148 cases (29%, 95% CI 26.99–31.01) occurred after 28 days of birth. Among newborns with IS, 242 (66.9%, 95% CI 64.43–69.37) were boys and 120 (33.1%, 95% CI 30.63–35.57) were girls.
Perinatal IS is defined in the specialized literature as an acute neurological syndrome of vascular origin, occurring between 20 weeks of gestation and 28 days after birth, confirmed by neuroimaging or neuropathological studies, and leading to neurological outcomes. Clinical manifestations in this group of children are less specific, with seizures, apnea, and impaired consciousness being the most common. In the pediatric population, perinatal IS accounts for 25% of IS cases and 43% of cavernous sinus thrombosis cases.
The analysis of IS clinical manifestations revealed differences compared to other age groups, characterized by several generalized symptoms (refer to
Table 1), associated with age-specific nervous system development.
Table 1 illustrates that 88.7% of newborns with ischemic stroke experienced convulsive seizures, with 65.7% exhibiting focal manifestations. The most prevalent clinical symptoms were apnea attacks, impaired consciousness, and movement disorders, while tremors, pathologic irritability, and converging strabismus were less frequent. However, it is important to include pathologic irritability in the algorithm for decision-making, as it represents an alarming sign. To interpret that, a brief difference to physiologic irritability is emphasized: Physiological irritability typically increases in the early weeks of life, peaks around 6–8 weeks of age, and generally improves by 3–4 months of age. In contrast, pathological irritability is characterized by excessive and relentless crying, which may lead to hypoxia and even epileptic seizures. This is a significant risk factor for abusive head trauma (previously known as shaken baby syndrome) and may indicate intense pain [
7]. Some infants also displayed additional manifestations such as rotatory nystagmus (6.07%) and leg clonus (5%). Consequently, newborns present clinical signs reminiscent of various central nervous system disorders, necessitating a thorough differential diagnosis. These events, documented in the neonatal period, are closely linked to cognitive and/or motor outcomes in childhood, often resulting in varying degrees of disability. The logistic regression analysis revealed a significant association between clinical symptoms and the child’s age. Specifically, epileptic seizures (
p < 0.001; RR = 5.118), impaired consciousness (
p = 0.006; RR = 2.909), generalized movement disorders (
p = 0.004; RR = 3.963), and apnea attacks (
p = 0.002; RR = 2.861) were identified as the most significant suggestive symptoms for diagnosing ischemic strokes in newborns.
The clinical presentation of childhood stroke varies depending on factors such as age, developmental characteristics of the central nervous system, affected artery, and the underlying cause of the disease. To account for these variations, the clinical manifestations of IS were evaluated in 148 children aged between 28 days and 18 years. They were categorized according to the stages of child development: infants (28 days–1 year), young children (1–3 years), preschoolers (4 years–6 years), schoolchildren (7–12 years), and adolescents (13–18 years), with grouping based on similarities of IS clinical symptoms to those observed in adults (
Figure 1).
Children aged between 28 days and 1 year old presented one-sided body weakness (p < 0.001; OR = 4.324), one-hand preferential use (p = 0.004; RR = 8.588), focal epileptic seizures (p = 0.006; RR = 3.377), and impaired consciousness (p = 0.003; RR = 1.143).
Children aged between 1 and 3 years old presented one-sided body weakness (p = 0.003; RR = 3.438), focal movement disorder (p = 0.002; RR = 1.178); focal epileptic seizures (p < 0.001; RR = 3.348), speech disorders (p = 0.004; RR = 4.163), psychomotor agitation (p = 0.003; RR = 1.114), and impaired consciousness (p = 0.001; RR = 1.043).
Children older than 3 years old presented hemiparesis (p = 0.004; RR = 1.153), headaches (p = 0.001; RR = 3.159), sensory disturbances (p = 0.003; RR = 3.156), psychomotor agitation (p = 0.002; RR = 2.341), and focal epileptic seizures (p < 0.001; RR = 4.365).
Following the analysis of ischemic stroke (IS) symptoms in children older than 28 days, it was found that the clinical presentation correlated with the children’s early age. The symptoms of stroke in infants (28 days–1 year) are often described as subtle focal neurological deficits that may go unnoticed by parents and doctors, such as reduced one-sided body strength, preferential use of one hand, fist clenching or leg clonus, psychomotor agitation, mainly focal epileptic seizures, as well as respiratory and consciousness disorders in severe cases. The clinical symptoms in young children (from 1 to 3 years old) are characterized by slight focal neurological deficits such as hemiparesis, focal movement disorders, and one-sided body weakness. Motor deficits often manifest on one side of the body, more commonly on the right, followed by injury to the left cerebral hemisphere. Other predominant symptoms include focal epileptic seizures, impaired consciousness, psychomotor agitation, and less commonly, coordination disorders, tremor, nystagmus, impaired eyesight, and vomiting. Children over three years of age may present the following clinical manifestations: focal neurological deficit, commonly followed by hemiparesis, less often by hemiplegia, focal epileptic seizures, mental disorders, headaches, and agitation. Less common symptoms observed are ataxia, nystagmus, dizziness, hemianopia, and speech disorder.
Based on the child’s age, disease onset, clinical symptoms, and imaging findings, neurological examination results suggested significant logistic regression outcomes. Moreover, the data analysis, modeling the relationship between a series of independent variables and a dichotomous dependent variable, identified the most important suggestive symptoms for diagnosing IS, depending on the child’s age.
Therefore, mathematical calculations on clinical IS symptoms in children of different ages are crucial for confirming the disease and initiating early treatment.
Table 2 illustrates the clinical manifestations of stroke according to age.
Further studies are required to confirm the diagnosis of stroke. Imaging findings, including brain CT scans, often do not reveal the presence of brain injury, largely depending on the timing of the examination. MRI scanning of the brain allows an assessment of the pathological focus topography and volume. During the study, it was observed that in newborns, the anterior cerebral artery and the middle cerebral artery were primarily affected, accounting for 228 cases (63.0%; 95% CI 60.46–65.54), along with the left cerebral hemisphere in 245 cases (67.7%; 95% CI 65.24–70.16). Multifocal brain injuries were identified in one-third of the children, totaling 119 cases (32.9%; 95% CI 30.43–35.37).
Throughout the study, a wide range of outcomes was observed among patients in the acute phase of the disease, reflecting varying degrees of severity from mild to severe symptoms, often resulting in severe neuro-psychomotor impairment (
Table 3).
Of the 108 children examined, 82 (75.9%; 95% CI [71.79–80.01]) presented motor deficits, 45 (41.7%; 95% CI [36.96–46.44]) had convulsions, and 19 (17.6%; 95% CI [13.94–21.26]) experienced impaired consciousness. Additionally, among these children, 87 (80.6%; 95% CI [76.79–84.41]) had a unilateral stroke, and 77 (71.3%; 95% CI [66.95–75.65]) showed signs of middle cerebral artery injuries. The degree of neurological manifestations was assessed using the Amiel-Tison and Gosselin summary tables (classified as shown in
Table 3) and the PedNIHSS scale. The mean value of the PedNIHSS scale was 7.8 points, with the scale ranging from 0 to 17 points. The statistical results of the calculated tests (χ
2 = 13.923, df = 4, and
p < 0.01) were significant. The majority of children with IS exhibited a mild to moderate IS severity, with 89 cases (82.4%; 95% CI [78.74–86.06]) falling within this range. The results obtained from the assessment of the Amiel-Tison, Gosselin, and PedNIHSS scale confirmed the clinical neurological manifestations, enabling the recognition of mild and moderate forms of IS in most patients.
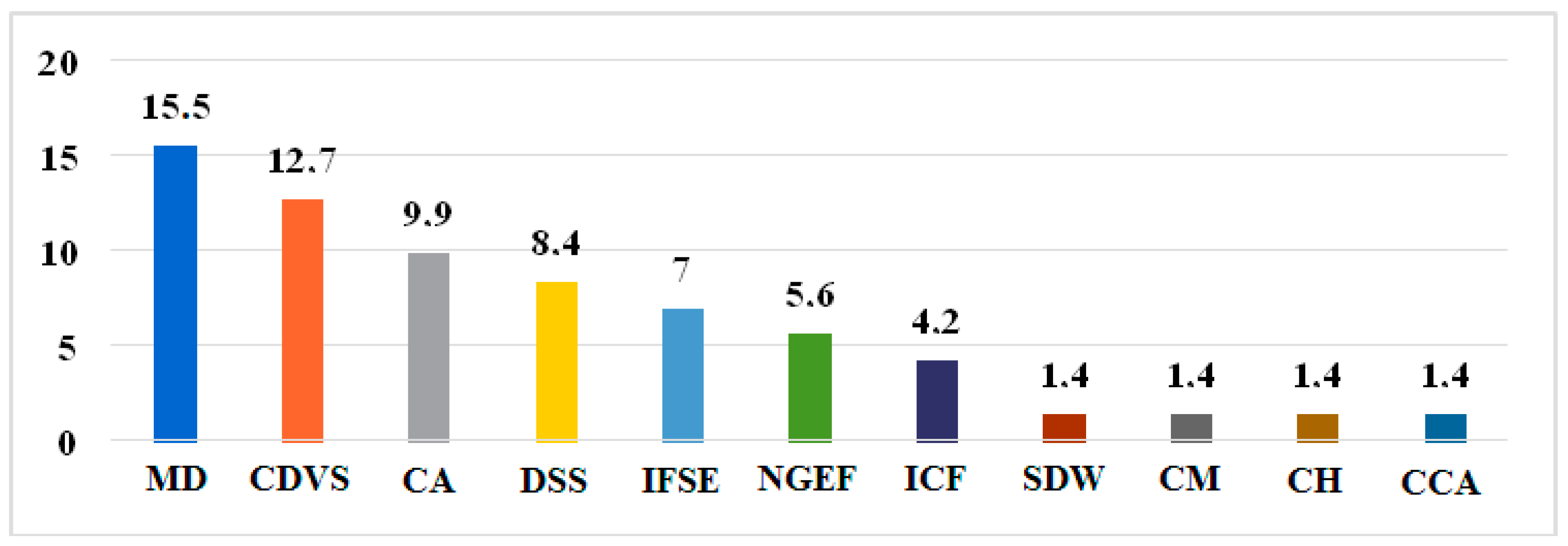
Children presenting with sudden onset of general neurologic symptoms should undergo an immediate neurological examination to identify the following neurological symptoms: focal neurological symptoms, seizures associated with neurological symptoms, visual or speech disorders, mental disorders, impaired coordination or ataxia, headaches, and signs of intracranial tension. Urgent neuroimaging studies are essential in such cases, as these symptoms have a high significance as predictors for IS. Regarding the imaging aspects of IS, in addition to cerebral hypodensities observed through CT examination in neonates, other cerebral changes were also identified. These included myelination deficiency (
n = 11; 15.5%; 95% CI [11.21–19.79]), congenital dilatation of the ventricular system (
n = 9; 12.7%; 95% CI [8.75–16.65]), cortical atrophy with various localizations (
n = 7; 9.9%; 95% CI [6.36–13.44]), dilatation of the subarachnoid spaces (
n = 6; 8.5%; 95% CI [5.2–11.8]), nonspecific glioependymal foci (
n = 4; 5.6%; 95% CI [2.86–8.32]), intracerebral foci with subcortical extension (
n = 5; 7.0%; 95% CI [3.96–10.04]), intracerebral cystic formations
(n = 3; 4.2%; 95% CI [1.81–6.59]), and anomalies of brain development, among others (see
Figure 2).
Next, the imaging changes detected during cerebral MRI examination are presented, depending on the size of the ischemic focus. In newborns, the initial imaging examination was performed, in most cases, within the first week, during the onset of disease symptoms (
Table 4).
The cerebral CT examination was not sufficient to establish the diagnosis, but it was helpful to clear concerns regarding the presence of a hemorrhagic stroke, tumor process, etc., and a brain MRI evaluation followed. This evaluation was performed in all 37 children (34.3%; 95% CI [29.73–38.87]) with suspected IS during the acute period of the disease. In all examined cases, ischemic lesions of various sizes were detected, characterized by a hypointense signal in T1 and a hyperintense signal in T2 (
Table 5). Medium-sized ischemic lesions predominated in 46% of cases, while small or large lesions were observed in a smaller number of cases (24.3% and 29.7%, respectively).
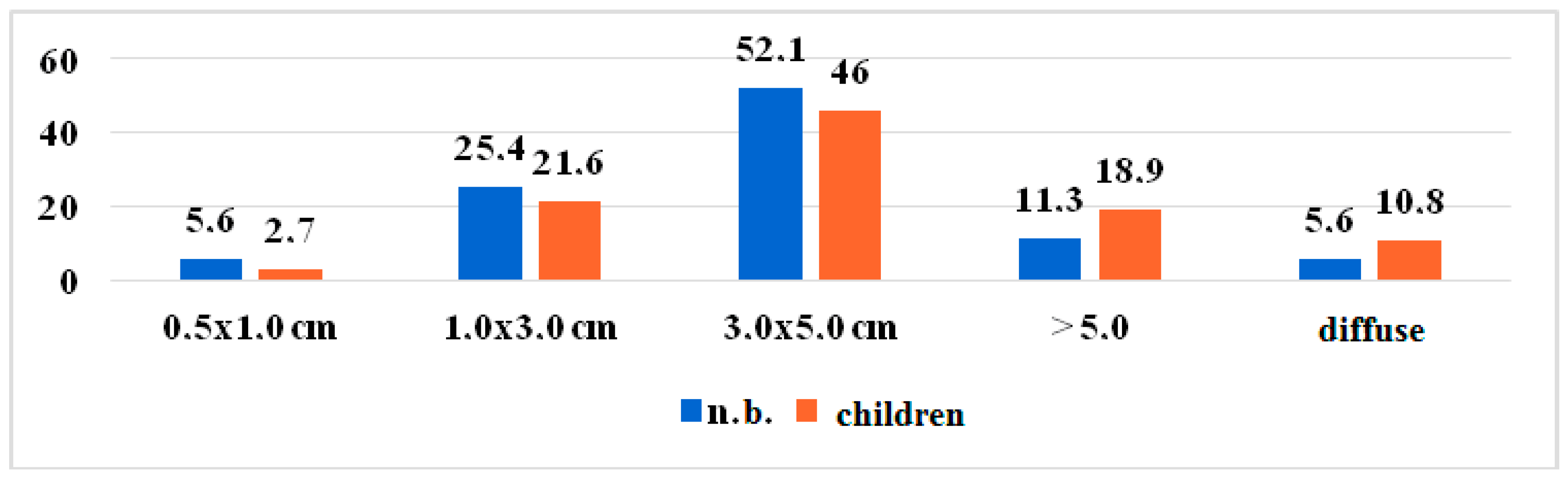
The distribution of ischemic foci according to size in the total study group, within the prospective study, is depicted in
Figure 3. It is observed that medium-sized ischemic lesions were the most frequent type detected, with a slight predominance in the infant group. However, large-sized foci prevailed in the group of children older than 28 days, particularly in infants and those of young age. This trend was influenced by the characteristic etiologies associated with these age groups, often determined by infectious causes.
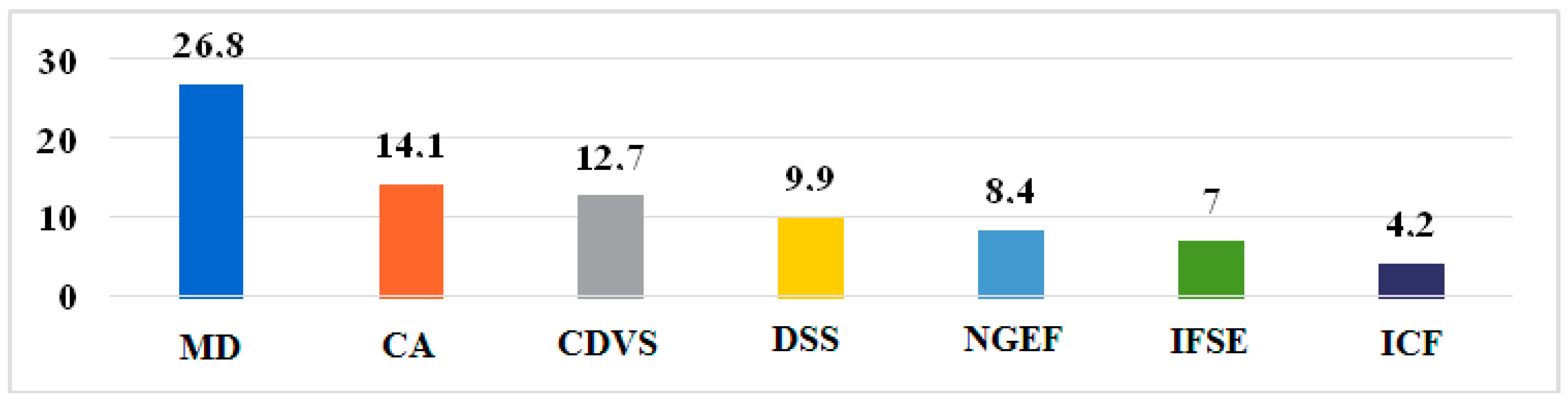
In the cerebral MRI examination, in addition to the ischemic foci, other types of changes were also detected in some children, which possibly constituted a cause of IS or worsened the evolution of this disease. Among such changes were myelination deficiency (
n = 19; 26.8%; 95% CI [21.55–32.05]), congenital dilatation of the ventricular system (
n = 9; 12.7%; 95% CI [8.75–16.65]), cortical atrophy with various locations and degrees
(n = 10; 14.1%; 95% CI [9.97–18.23]), dilatation of the subarachnoid spaces (
n = 7; 9.9%; 95% CI [6.36–13.44]), nonspecific glioependymal foci (
n = 6; 8.5%; 95% CI [5.2–11.8]), nonspecific intracerebral foci with subcortical extension (
n = 5; 7.0%; 95% CI [3.96–10.04]), intracerebral cystic formations (
n = 3; 4.2%; 95% CI [1.81–6.59]), etc. (
Figure 4).
Such changes, in some cases combined, were mainly detected in the group of infants and young children. In some children, besides ischemic foci, other types of changes were observed, which might have been present before the stroke or contributed to its onset. These included: myelination deficiency
(n = 5; 13.5%; 95% CI [7.88–19.12]), ventricular system dilatation (
n = 9; 24.3%; 95% CI [17.25–31.35]), cortical atrophy of varying degrees and locations (
n = 6; 16.2%; 95% CI [10.14–22.26]), subarachnoid space dilatation (
n = 5; 13.5%; 95% CI [7.88–19.12]), nonspecific glioependymal foci of various sizes (
n = 7; 18.9%; 95% CI [12.46–25.34]), nonspecific intracerebral foci with subcortical extension (
n = 2; 5.4%; 95% CI [1.68–9.12]), intracerebral cystic formations (
n = 3; 8.1%; 95% CI [3.61–12.59]), and other anomalies of brain development (
Figure 5). These changes, sometimes occurring together, were predominantly observed in infants and young children.
According to the results of MRI in children and newborns, the most frequent additional stroke-associated cerebral MRI changes in children were dilatation of the ventricular system and nonspecific glioependymal foci (
Figure 6). Comparing with newborns, the results of MRI showed that the most common additional stroke-associated cerebral changes in newborns are represented by myelination deficiency, on first place and on the second place by the cortical atrophy (
Figure 6).
Below are some developmental anomalies of the brain found in children with IS, such as a developmental anomaly of the ventricular system (
n = 3; 8.1%; 95% CI [3.61–12.59]), hypogenesis of the corpus callosum (
n = 2; 5.4%; 95% CI [1.68–9.12]), hypogenesis of the cerebellar vermis, retrocerebellar cyst, Arnold Chiari malformation, and hypogenesis of the cerebellar hemispheres, each one case (2.7%; 95% CI [0.03–5.37]). Thus, brain developmental abnormalities detected in children with stroke were present in nine (
n = 9; 24.3%; 95% CI [17.25–31.35]) cases (
Figure 7).
Brain MRI results associated with the age of the child and the topographic location of the ischemic focus were analyzed (
Figure 8).
Brain MRI was performed in the acute period of the stroke and at six months after the disease in all children included in the prospective study group. In contrast to CT, MRI images were much more informative and allowed for the assessment of the dimensions of the pathological focus at a distance compared to the acute period of the disease. It was found that the ischemic changes in the brain tissue detected during the acute period evolved into gliotic foci or cysts of various sizes, with a statistically significant difference being attested in that case (
Table 6).
Evolution towards normality was found only in the case of very small ischemic foci (3.7%). Additionally, a slight reduction in medium-sized ischemic foci was observed in 17 (31.5%) cases, possibly due to tissue recovery from the ischemic penumbra. Large lesions underwent cystic transformation. Angio-CT and angio-MRI were applied in exceptional cases to eight children with suspected vascular malformations (
Figure 9).
5. Discussion
IS in children is specified as a major neurological emergency, being a primary cause of morbidity and mortality. In the neonatal period, one in 2500–4000 live-born children presents with a stroke, and in children over one month old, 1.2–8 per 100,000 [
7]. The data of the given study showed the following distribution: A 24.5% decrease in the primary disability indicator was observed in 2020 (2.1 cases per 100,000 children) compared to 2016 (2.8/100,000). The highest values were recorded in 2017 and 2018 (3.7/100,000), and the trends for the repeated disability indicator were similar. Cases certified in 2020 (11.6/100,000 children) were 23.9% less than in 2016 (15.3/100,000), with the highest level recorded in 2017 (16.9/100,000).
Clinical manifestations of IS in children, unlike those in adults, are varied depending on age, and are often obscure, with a variable clinical polymorphism. Also, IS can occur during pregnancy or immediately after birth, without significant symptoms. The mortality rate from pediatric stroke is between 5% and 10%. More than half of survivors have long-term neurological sequelae, and 10–20% suffer from stroke recurrences [
7,
9]. These arguments condition the creation of emergency care and rehabilitation centers for pediatric stroke patients, a multidisciplinary approach, highly specialized evaluation and treatment, with significant input from the health care system, families, and the community.
According to the WHO classification, stroke can be of several types: transient stroke (TS), which represents ischemia in a localized area of the brain, with motor deficit up to 24 h (from a few minutes to a few hours), without neurological sequelae; involutive stroke, characterized by acute cerebral ischemia with motor deficit for more than 24 h, with its complete involution for 21 days; lacunar stroke—a type of stroke in which blood flow is blocked in a group of very small arteries inside the brain, mainly those that supply blood to deep areas of the brain. In these types of infarctions, cerebral ischemic lesions range from 2 to 20 mm in diameter; IS in evolution is characterized by a slow-progressive evolution, from a few hours to a few days. Clinical symptoms persist for more than three weeks and motor deficit evolves/regresses in about 30 days. In progressive evolution, it can evolve towards established IS—this is a consequence of the neuronal destruction in the damaged vascular territory, which will manifest itself clinically with an installed motor deficit [
10]. Each type of stroke requires its specific approach to diagnostics and treatment. For that reason, the study design of this research work included only one type of stroke, ischemic stroke.
According to several researchers [
11] ischemic stroke is defined when a focal neurological deficit occurs that lasts more than 24 h, with neuroimaging evidence of cerebral infarction. In the case of a neurological deficit that recovers before 24 h and there are no neuroradiological changes, the event is called a transient ischemic attack. If the clinical manifestations last less than 24 h, but there are neuroradiological signs of infarction, it is considered an IS [
11]. According to the authors G. Jeong et al., stroke in children is defined as a sudden focal infarction of brain tissue, diagnosed by neuroimaging or at autopsy, which may lead to arterial stroke or venous infarction. An IS occurs when there is a sudden occlusion of one or more cerebral arteries. In children, arterial ischemic stroke is the most common subtype, accounting for just over half of all cerebrovascular accidents [
12]. Some authors mention in their papers [
13] that IS in children can present with subtle symptoms, especially among newborns and small children. According to researchers, the clinical manifestations and risk factors of IS in children are different from those of adults; therefore, the disease can be considered an independent nosological entity [
13,
14]. To address the issue of uncertain clinical symptoms of IS in children and newborns, a significant aspect of the study involved evaluating the clinical signs of IS in that population. Consequently, all signs exhibited by patients were considered potential diagnostic and prognostic features and were statistically analyzed. The most relevant signs, which demonstrated a significant association with IS, were then incorporated into the algorithms. The following standardized measures served as the basis for characterizing all clinical signs assessed in the study. Stroke symptoms in early childhood are usually nonspecific, and in older children, they often manifest as focal neurological deficits, such as acute hemiplegia. The neurological examination should highlight the most subtle symptoms suggestive of a stroke, including monitoring of vital parameters, identifying neurological damage and suggesting the presumptive diagnosis and brain topography involved. As a rule, some systemic diseases that increase the risk of stroke must be excluded. The suggestive symptoms for damage to a cerebral vascular territory are the following: (1) internal carotid artery—hemiparesis, aphasia, and hemianopsia; (2) anterior cerebral artery—hemiparesis, especially in the lower limbs; (3) middle cerebral artery—hemiparesis of the upper limbs, hemianopsia, and aphasia; (4) posterior cerebral artery—hemiparesis, hemianopsia, ataxia, and dizziness; (5) basilar artery—difficulty breathing, sensory or balance disturbances, ataxia, nystagmus, opisthotonus, tremors, and vomiting; (6) cerebellar artery—sensory deficit, headache, fever, vomiting, and cerebellar signs [
6]. The clinical manifestation of IS in children varies depending on the age, the involved artery and the cause [
3]. Focal symptoms, especially hemiplegia, are most frequently present in hemorrhagic stroke and vary according to different authors. The clinical presentation of IS is diverse, and common IS symptoms such as altered consciousness, convulsions, etc., may be encountered. The diagnosis of pediatric ischemic stroke is based on the recognition of clinical manifestations depending on the age and the cerebral vascular system involved.
The statistical analysis in this study revealed distinct clinical symptom patterns as the most relevant for IS in children of different age groups:
Children aged between 28 days and 1 year old presented one-sided body weakness, one-hand preferential use, focal epileptic seizures, and impaired consciousness. These symptoms were significant indicators of ischemic stroke in that age group.
Children aged between 1 and 3 years old exhibited one-sided body weakness, focal movement disorder, focal epileptic seizures, speech disorders, psychomotor agitation, and impaired consciousness. These symptoms were more pronounced compared to infants, indicating a clearer clinical picture.
Children older than 3 years old demonstrated hemiparesis, headaches, sensory disturbances, psychomotor agitation, and focal epileptic seizures. These symptoms were more akin to those observed in adults, highlighting a closer resemblance in clinical presentation.
The most common disabilities found in children older than 3 years, who had suffered a stroke were motor disability—74.9%, including hemiparesis—63.7%, tetraparesis—25.8%, tetraplegia—10.4%, epilepsy—28%, disorders of speech—17.8%, cognitive and behavioral problems—53.9%.
IS represents a clinical syndrome with rapid evolution, manifested by the global or focal disturbance of cerebral function, lasting more than 24 h or leading to death without any obvious nonvascular reason [
7]. The importance of developing algorithms to reduce decision-making time is obvious. A clear correlation between the clinical and imaging aspects of ischemic stroke is evident, as it is a clinical syndrome characterized by a neurological deficit related to the perfusion territory of a cerebral artery and neuroradiological evidence of an ischemic lesion” [
7]. For that obvious reason, in the recently developed algorithms, the paraclinical signs were also included. The diagnosis of IS in children is often delayed because signs and symptoms can be subtle and nonspecific, and thus treatment is often delayed and limited.
Several authors mention that even the definitive causes in the majority of pediatric, especially neonatal, strokes have not been established, and large case–control studies are needed to understand the early clinical manifestations and pathogenesis if treatment outcomes are to be improved [
6]. The authors DeLaroche A.M. and Sivaswamy L. consider that IS in children are some of the most frequent complications of hypoxia and ischemia in the first week of life [
2]. Lee J et al. describe how those complications following perinatal stroke vary according to the type of accident and that some children may have a normal neurological outcome, while others develop cerebral palsy (CP) (58%), language (25%), and behavioral disorders (22%). In other cases, motor symptoms can be observed later after birth [
14]. The authors of another study consider that in children, unlike young children or adolescents, there are no clinical signs suggestive of a presumptive diagnosis of arterial IS, and the recognition of the condition is based on imaging data [
3]. Authors Lai M.C. and Yan S.N. found that among children with perinatal stroke, the specific radiological findings and the lack of symptoms in newborns were associated with a high risk of CP [
15], especially the hemiparetic forms. Taking into consideration the above-mentioned problem of unspecific imaging signs, a delayed or lack of indication for imaging lengthens the diagnostic and treatment time. Thus, the important applicative value of this study is that some clinical and paraclinical signs that were not previously considered pathognomonic for ischemic stroke in newborns and children have now been included in the new algorithms of national protocols as direct and urgent signs for MRI and CT and for appropriate treatment. In the past, these signs were not indications for CT and MRI, leading to delayed diagnosis and treatment, resulting in long-lasting complications and consequences in children. According to the study, only CT and MRI can confirm the diagnosis of stroke, so it is crucial to recognize these signs for timely intervention. These new paraclinical signs, included in the algorithm, belong to the clinical presentation of ischemic stroke (IS) in children and vary depending on their age. Younger children tend to have more subtle and nonspecific symptoms, which are often initially attributed to other causes. This can lead to a delay in diagnosing IS and result in further complications. The study results suggest that imaging should be considered for all children, even those with minimal suspicion of IS. In fact, in all cases where there was minimal suspicion of stroke, IS was diagnosed using CT and MRI. Identifying the minimal but relevant clinical signs for IS based on the age of the children can serve as the right indications for CT and MRI. The mathematical analysis yielded the following results: (1) newborns: epileptic seizures, disturbance of consciousness, generalized motor disorders, and apnea attacks; (2) infants: decreased strength in one half of the body, preferential use of one hand, focal epileptic seizures, and impaired consciousness; (3) young children: decreased strength in one side of the body, focal movement impairment, focal epileptic seizures, speech disorder, and disorder of consciousness; (4) children older than three years: weakness on one side of the body, headache, sensory disturbances, and psychomotor agitation, and focal epileptic seizures.
IS in both the middle cerebral artery system and the posterior cerebral artery system may manifest as seizures of one half of the body, whereas stroke in the middle cerebral artery system may manifest as seizures of the hand and face only. Seizures isolated to one leg can be found in neonatal IS with localization in the anterior cerebral artery system, and those isolated to the upper extremities are characteristic of the involvement of the posterior part of the middle cerebral artery. Authors Gelfand A.A. and Glass H.C. mention that in cases of an involvement of the middle cerebral artery, atypical convulsions are observed (hiccupping, eye blinking, gaze fixation, chewing, sucking, vertical nystagmus, and thumb adduction) [
16], such convulsions being rarely isolated. Apnea attacks or cyanotic attacks, probably of an epileptic nature, have been reported. Strokes, regardless of age of onset, can be hemorrhagic (subarachnoid or intraparenchymal) or ischemic. The type of stroke varies depending on the age of the patient and the etiology, which is different in the child than in the adult. More than 70 potential risk factors for stroke in children and adults are described. Often, however, ischemia is the result of nonatherosclerotic vasculopathy, cardiac embolisms, or coagulability disorders. In children, stroke can occur as a result of congenital heart diseases, acquired heart diseases, infectious or inflammatory diseases, vascular disorders, hematological diseases, cerebrovascular malformations, or brain trauma; however, for a third of strokes, the etiology remains undetermined [
17,
18].
The incidence of ischemic stroke (IS) in children is increasing due to the advancement of imaging techniques for diagnosing the disease. Imaging studies help in identifying the type and location of IS, as well as in making a differential diagnosis. According to the data from a specific study, medium-sized ischemic areas are more common in neonates (52.1%) compared to pediatric patients (46%), while larger areas are predominant in the pediatric group (29.7%), especially in infants and young children. The middle cerebral artery (51.0%) and the anterior cerebral artery (40.7%) are the main arteries involved in the ischemic process across all age groups, with a higher prevalence in neonates and infants. The posterior cerebral artery (8.3%) is more frequently involved in older children (16.7%). The left hemisphere is more commonly affected (72.2%) compared to the right (27.8%), and a diffuse distribution of the pathological focus was found in 27.8% of cases, with a higher prevalence in infants (38.5%) and newborns (32.4%). These findings align with existing literature data. The study’s strength lies in its correlation of clinical signs relevant to IS prognosis with paraclinical results. Strong correlations were found between imaging and clinical data (rxy = 0.983), which facilitated the development of a clinical-etiological classification of IS in children based on age. This formed the basis for the algorithm development and its inclusion in protocols. These newly developed algorithms led to the standardization of imaging protocols in pediatric centers for stroke patients. An international study of clinical and imaging analyses of symptomatic IS summarized various clinical presentations, risk factors, types of investigations, treatments, and early outcomes in IS. The most important clinical symptoms reported were seizures (72%) and nonfocal neurological signs (63%) [
19]. However, some studies mention that about 40% of children do not show specific symptoms in the neonatal period; they are recognized later, with the appearance of motor disorders, developmental delays, cognitive impairment, or seizures [
20]. Notably, pediatric IS (PIS) leads to significant morbidity and mortality. Of all cases, approximately 10–25% will be fatal, up to 25% of patients will have a recurrence, and up to 66% will have persistent neurological deficits or develop epilepsy, learning problems, or developmental problems. Up to one-third of children who have had a stroke have a history of recent events compatible with transient stroke. Neurological impairment during childhood will have a major impact on the quality of life of the child and the family, but also on the economic and emotional costs of society [
21]. Early recognition of PIS requires emergency neurological consultation and hospitalization to provide coherent etiological/pathogenetic diagnostic and treatment management and improve outcomes.
The diagnosis of PIS is based on the recognition of symptoms according to age and the vessel involved. Signs of stroke in early childhood are usually nonspecific, and in older children, focal neurological deficits are often noted, such as acute hemiplegia. The neurological examination should highlight the most subtle symptoms of a possible stroke, including monitoring of vital parameters, identifying neurological damage, and assuming the presumptive diagnosis and topography of the involved vessel. As a rule, some systemic diseases that increase the risk of IS must be excluded. Neuroimaging is crucial in defining the diagnosis, other tests being necessary depending on the clinical picture. Thus, PIS is better recognized among practitioners as a clinically significant entity [
22]. It is known that the diagnosis of stroke in children can often be delayed, and sometimes missed due to mild and nonspecific clinical symptoms and since they are initially related to other causes than stroke. The suggestive stroke symptoms characteristic of a certain age category may improve diagnosis in 66–99.7% of cases [
23] if using the mathematical calculations proposed for the prevalence of certain symptoms of the disease. In this context, the results of the study reveal that children with sudden onset of the following clinical symptoms are at high risk of developing IS: focal neurological symptoms, seizures, accompanied by neurological symptoms, visual or speech disorders, mental disorders, impaired coordination or ataxia, headaches, and signs of intracranial tension. For that reason, these clinical signs have to be regarded as predictors of IS, and the patients should undergo an immediate neurological examination for the detection of IS. At the same time, urgent neuroimaging studies are required. Children with suspected ischemic stroke should undergo MRI, as a method of early diagnosis. If an urgent MRI examination is not possible, a brain CT scan should be considered as an alternative, especially in adolescents [
24]. Brain MRI or brain CT scanning should be performed in children with suspected hemorrhagic stroke [
25]. Based on the symptoms that had a significant relationship with the following stroke event, the data-driven statistical analysis makes it possible for the first time to establish algorithms that enable a clinical plan for fast, time-saving recognition of the stroke diagnosis; thus, it allows the choice of the best, time-dependent treatment options of stroke events in newborns and children of different age groups. Logistic regression was used to derive the algorithms for decision-making regarding stroke diagnosis and its early treatment, to decrease life-long morbidity and mortality of children. Based on the results of this study, algorithms for timely newborn stroke recognition were elaborated. Furthermore, it is planned that to adopt these newly elaborated algorithms and train a fuzzy classifier-based diagnostic model using these algorithms for developing machine learning algorithms for decision-making regarding prompt, time-saving stroke recognition. This is an important step towards a new generation of algorithm formation based on machine learning techniques [
18]. The advantage of such an approach to diagnosis and prediction, especially in neurology, when a time-dependent recognition of trigger symptoms is critical, is described in the literature [
14,
15,
16,
17,
23,
24]. In the study conducted by Shkilniak L. et al., relevant results in prognostic modeling in pathological conditions regarding edema of soft tissue with the implementation of vessels and blood clotting abnormalities, realized via a fuzzy classifier, were shown [
26]. From the literature data, it can be assumed that the fuzzy classifier is an appropriate method for the future conversion of the developed algorithms into automatized algorithms. The basics for its realization will be implemented based on the fundamental principles of neural network circuits, regarding their potential possibilities for application in biosciences and medicine [
27]. It is known that machine learning algorithms have to be trained with high-quality data [
18]. The clinical algorithms developed in this study for valid, timely IS detection are therefore promising results for further training the fuzzy classifier with this validated and high-quality data, which is planned as the next step of the study.
Clinical impact of the developed algorithms
In the current research, the solved scientific problem consists in the elucidation of the evolutionary clinical–paraclinical peculiarities of IS in children, which will improve the early diagnosis of the disease and the prophylaxis of neurological disorders in the future. The diagnosis and treatment of strokes can be optimized by applying the diagnostic and therapeutic algorithms elaborated in this study. They involve a combination of clinical, neuroimaging, neurofunctional assessment methods, and laboratory tests. Implementing these algorithms in clinical settings will help recognize and prevent childhood strokes, reduce treatment delays for ischemic stroke, and provide real-time decision support. These algorithms include clinical and paraclinical signs that were not previously considered for stroke diagnosis but are now included in newly developed national protocols as pathognomonic signs. They are now considered urgent signs for MRI and CT to facilitate real-time decision support. Analyzing the risk factors for ischemic stroke has also allowed for the development of an algorithm to identify and manage newborns and children at risk for this disease, along with recommendations for its prevention in children.
The generalizability of the results to various populations and healthcare settings
The study involved evaluating children and newborns from across the country based on specific criteria and signs that were identified in advance as potential predictors and diagnostic signs of ischemic stroke. The findings of the study can be applied to the general population of Moldova, particularly to children and newborns with ischemic stroke. Additionally, these findings can be useful in various healthcare settings, as three distinct algorithms have been developed for specialized medical care, preclinical medical assistance, and management of relatives’ behavior.
Future outlook
Furthermore, the developed algorithms will also be included in training machine learning algorithms, as it was shown in a series of studies that the training of machine learning algorithms using neuroimaging findings with a certain aim revealed promising results [
15,
16,
17,
28].
The presented algorithms will allow specialists in the field to timely diagnose stroke in children and to correctly apply their diagnostic and treatment methods. Therefore, a logistic regression was applied to recognize which symptoms were related to the triggering and prediction of stroke. Further machine learning methods will have to prove how well these correlations work in automatic algorithms. However, this study is an important tool to develop further machine learning tools for clinical and paraclinical symptom-based recognition and prediction of IS.
The need for external validation is important, however, to obtain additional data, and it must be carried out in future studies.
Similar studies are also required for children with hemorrhagic stroke; thus, in the future, we will also investigate the relevant diagnostic and predictive signs for timely hemorrhagic stroke recognition.
The results of the study convinced the Medical Society of the Republic of Moldova of the importance of early diagnosis of IS not only in adults but also in children. Until recently it was considered that IS was only a condition in adults; we demonstrated through concrete studies that the number of children with IS in the Republic of Moldova was high, and these studies can also be replicated in other countries of the world. It may be necessary to join some international IS research studies.
Limitations of the study and potential bias
Parents provided information about the clinical and anamnestic data because newborns and children were unable to express verbally their symptoms and the circumstances when the signs appeared. We were reliant on the reports of the relatives, which may lead to some missing data and paraclinical information. The retrospective analysis may also be biased due to the quality of the data collection from the parents being reflected in the documentation, which depended on the subjective human factor. Another limitation is that the study design only focused on newborns and children with ischemic stroke, not hemorrhagic stroke, so the study results are limited to ischemic stroke. Therefore, any conclusions about the broader population should be limited to what can be supported by the sample studied.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}