Effect of Tiotropium Soft Mist Inhalers on Dynamic Changes in Lung Mechanics of Patients with Chronic Obstructive Pulmonary Disease Receiving Mechanical Ventilation: A Prospective Pilot Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Protocol and Lung Mechanics Measurement
2.3. Statistical Analysis
3. Results
3.1. Patients’ Clinical and Demographic Characteristics
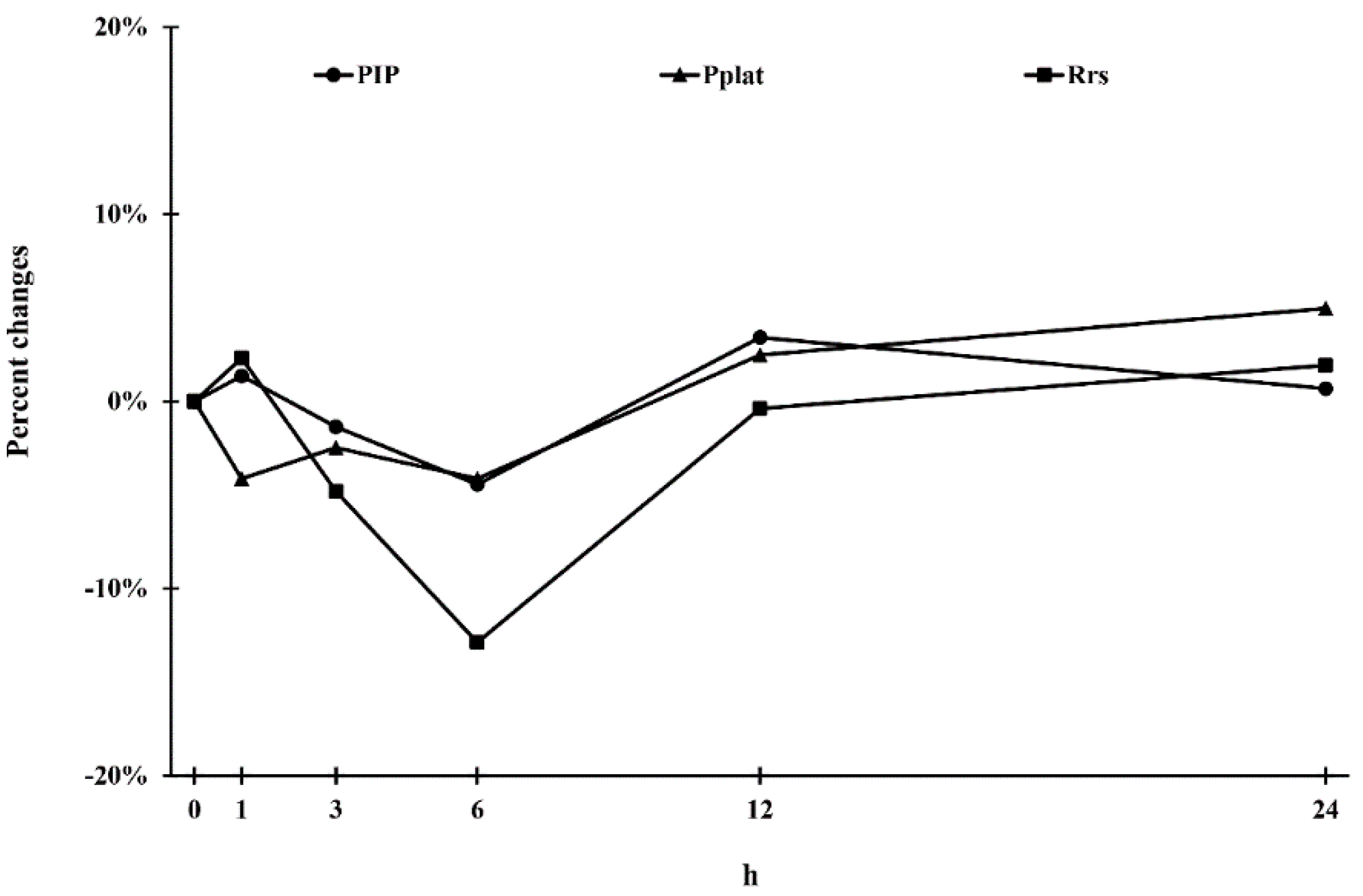
3.2. Lung Mechanics at Different Time Points
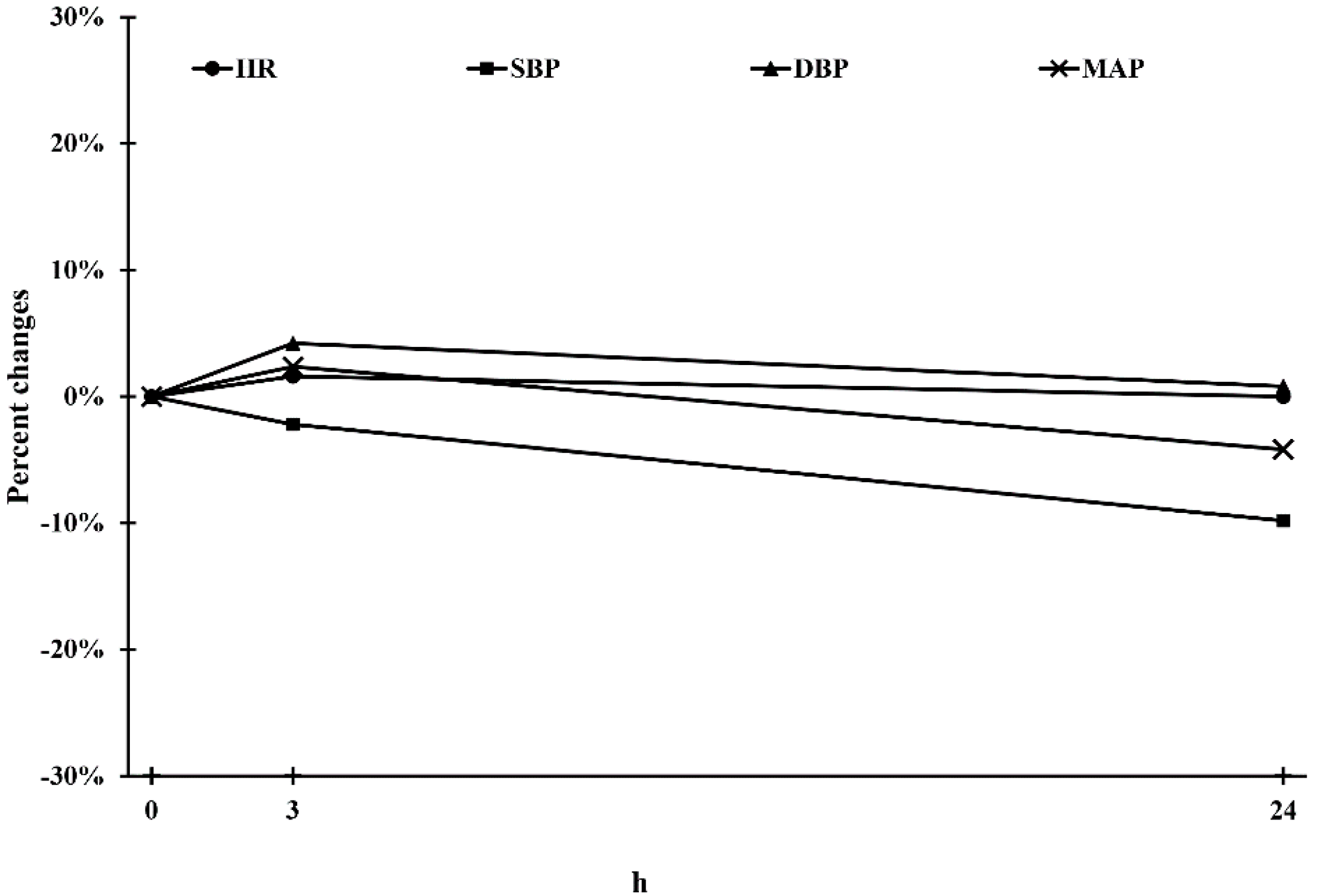
3.3. Physiological Parameters at Different Time Points
3.4. Blood Gas Parameters and PaO2/FiO2 at Different Time Points
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Quaderi, S.A.; Hurst, J.R. The unmet global burden of COPD. Glob. Health Epidemiol. Genom. 2018, 3, e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celli, B.R.; Wedzicha, J.A. Update on Clinical Aspects of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2019, 381, 1257–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flattet, Y.; Garin, N.; Serratrice, J.; Perrier, A.; Stirnemann, J.; Carballo, S. Determining prognosis in acute exacerbation of COPD. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 467–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maccari, J.G.; Teixeira, C.; Gazzana, M.B.; Savi, A.; Dexheimer-Neto, F.L.; Knorst, M.M. Inhalation therapy in mechanical ventilation. J. Bras. Pneumol. 2015, 41, 467–472. [Google Scholar] [CrossRef] [Green Version]
- Guerin, C.; Fassier, T.; Bayle, F.; Lemasson, S.; Richard, J.C. Inhaled bronchodilator administration during mechanical ventilation: How to optimize it, and for which clinical benefit? J. Aerosol. Med. Pulm. Drug Deliv. 2008, 21, 85–96. [Google Scholar] [CrossRef]
- Duarte, A.G. Inhaled bronchodilator administration during mechanical ventilation. Respir. Care 2004, 49, 623–634. [Google Scholar]
- Malliotakis, P.; Linardakis, M.; Gavriilidis, G.; Georgopoulos, D. Duration of salmeterol-induced bronchodilation in mechanically ventilated chronic obstructive pulmonary disease patients: A prospective clinical study. Crit. Care 2008, 12, R140. [Google Scholar] [CrossRef] [Green Version]
- Calverley, P.M.A.; Anzueto, A.R.; Carter, K.; Gronke, L.; Hallmann, C.; Jenkins, C.; Wedzicha, J.; Rabe, K.F. Tiotropium and olodaterol in the prevention of chronic obstructive pulmonary disease exacerbations (DYNAGITO): A double-blind, randomised, parallel-group, active-controlled trial. Lancet Respir. Med. 2018, 6, 337–344. [Google Scholar] [CrossRef]
- Tamura, G. Comparison of the aerosol velocity of two Respimat((R)) soft mist inhalers and two pressurized metered-dose inhalers for short-acting muscarinic antagonists. Respir. Investig. 2017, 55, 287–288. [Google Scholar] [CrossRef]
- Tamura, G. Comparison of the aerosol velocity of Respimat(R) soft mist inhaler and seven pressurized metered dose inhalers. Allergol. Int. 2015, 64, 390–392. [Google Scholar] [CrossRef] [Green Version]
- Neumeier, A.; Keith, R. Clinical Guideline Highlights for the Hospitalist: The GOLD and NICE Guidelines for the Management of COPD. J. Hosp. Med. 2020, 15, e1–e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD science committee report 2019. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef] [PubMed]
- van Noord, J.A.; Cornelissen, P.J.; Aumann, J.L.; Platz, J.; Mueller, A.; Fogarty, C. The efficacy of tiotropium administered via Respimat Soft Mist Inhaler or HandiHaler in COPD patients. Respir. Med. 2009, 103, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, R.; Moghtader, S.; Ayyala, U.; Bandi, V.; Sharafkhaneh, A. Update on management of stable chronic obstructive pulmonary disease. J. Thorac. Dis. 2019, 11, S1800–S1809. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease-2020 Report. 2020. Available online: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf (accessed on 5 April 2020).
- Ke, W.R.; Wang, W.J.; Lin, T.H.; Wu, C.L.; Huang, S.H.; Wu, H.D.; Chen, C.C. In Vitro Evaluation of Aerosol Performance and Delivery Efficiency During Mechanical Ventilation Between Soft Mist Inhaler and Pressurized Metered-Dose Inhaler. Respir. Care 2020, 65, 1001–1010. [Google Scholar] [CrossRef]
- Fang, T.P.; Chen, Y.J.; Yang, T.M.; Wang, S.H.; Hung, M.S.; Chiu, S.H.; Li, H.H.; Fink, J.B.; Lin, H.L. Optimal Connection for Tiotropium SMI Delivery through Mechanical Ventilation: An In Vitro Study. Pharmaceutics 2020, 12, 291. [Google Scholar] [CrossRef] [Green Version]
- Toumpanakis, D.; Loverdos, K.; Tzouda, V.; Vassilakopoulou, V.; Litsiou, E.; Magkou, C.; Karavana, V.; Pieper, M.; Vassilakopoulos, T. Tiotropium bromide exerts anti-inflammatory effects during resistive breathing, an experimental model of severe airway obstruction. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2207–2220. [Google Scholar] [CrossRef] [Green Version]
- Dalby, R.; Spallek, M.; Voshaar, T. A review of the development of Respimat Soft Mist Inhaler. Int. J. Pharm. 2004, 283, 1–9. [Google Scholar] [CrossRef]
- Dellweg, D.; Wachtel, H.; Hohn, E.; Pieper, M.P.; Barchfeld, T.; Kohler, D.; Glaab, T. In vitro validation of a Respimat(R) adapter for delivery of inhaled bronchodilators during mechanical ventilation. J. Aerosol Med. Pulm. Drug Deliv. 2011, 24, 285–292. [Google Scholar] [CrossRef]
- Suggett, J.; Nagel, M. Assessment of a Ventilator Circuit Adapter to Be Used in Conjunction with the Respimat Soft Mist Inhaler (SMI); Institute of Occupational Medicine and Industrial Hygiene, College of Public Health, National Taiwan University: Taipei, Taiwan, 2017. [Google Scholar]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Chen, W.C.; Chen, H.H.; Chiang, C.H.; Lee, Y.C.; Yang, K.Y. Effect of salmeterol/fluticasone combination on the dynamic changes of lung mechanics in mechanically ventilated COPD patients: A prospective pilot study. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guglielminotti, J.; Desmonts, J.M.; Dureuil, B. Effects of tracheal suctioning on respiratory resistances in mechanically ventilated patients. Chest 1998, 113, 1335–1338. [Google Scholar] [CrossRef] [PubMed]
- Henderson, W.R.; Sheel, A.W. Pulmonary mechanics during mechanical ventilation. Respir. Physiol. Neurobiol. 2012, 180, 162–172. [Google Scholar] [CrossRef]
- Storme, L.; Riou, Y.; Leclerc, F.; Kacet, N.; Dubos, J.P.; Gremillet, C.; Rousseau, S.; Lequien, P. Respiratory mechanics in mechanically ventilated newborns: A comparison between passive inflation and occlusion methods. Pediatr. Pulmonol. 1992, 12, 203–212. [Google Scholar] [CrossRef]
- FDA. RespiConnect* Adapter 11250194040. 2020. Available online: https://fda.report/GUDID/62860112501020 (accessed on 5 April 2020).
- Dhand, R. Inhalation therapy with metered-dose inhalers and dry powder inhalers in mechanically ventilated patients. Respir. Care 2005, 50, 1331–1334; discussion 1344–1345. [Google Scholar]
- Dhand, R.; Tobin, M.J. Bronchodilator delivery with metered-dose inhalers in mechanically-ventilated patients. Eur. Respir. J. 1996, 9, 585–595. [Google Scholar] [CrossRef] [Green Version]
- Malliotakis, P.; Mouloudi, E.; Prinianakis, G.; Kondili, E.; Georgopoulos, D. Influence of respiratory efforts on b2-agonist induced bronchodilation in mechanically ventilated COPD patients: A prospective clinical study. Respir. Med. 2007, 101, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Hindle, M.; Kaviratna, A.; Huynh, B.K.; Delvadia, R.R.; Sandell, D.; Byron, P.R. In Vitro Tests for Aerosol Deposition. VI: Realistic Testing with Different Mouth-Throat Models and In Vitro-In Vivo Correlations for a Dry Powder Inhaler, Metered Dose Inhaler, and Soft Mist Inhaler. J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 358–371. [Google Scholar] [CrossRef]
- Cazzola, M.; Noschese, P.; De Michele, F.; D’Amato, G.; Matera, M.G. Effect of formoterol/budesonide combination on arterial blood gases in patients with acute exacerbation of COPD. Respir. Med. 2006, 100, 212–217. [Google Scholar] [CrossRef] [Green Version]
- Knudson, R.J. Constantine HP. An effect of isoproterenol on ventilation-perfusion in asthmatic versus normal subjects. J. Appl. Physiol. 1967, 22, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Khoukaz, G.; Gross, N.J. Effects of salmeterol on arterial blood gases in patients with stable chronic obstructive pulmonary disease. Comparison with albuterol and ipratropium. Am. J. Respir. Crit. Care Med. 1999, 160, 1028–1030. [Google Scholar] [CrossRef] [PubMed]
- Ando, F.; Ruggeri, P.; Girbino, G.; Cazzola, M. Tiotropium and salmeterol/fluticasone combination do not cause oxygen desaturation in COPD. Respir. Med. 2008, 102, 815–818. [Google Scholar] [CrossRef] [PubMed]
- Santus, P.; Centanni, S.; Morelli, N.; Di Marco, F.; Verga, M.; Cazzola, M. Tiotropium is less likely to induce oxygen desaturation in stable COPD patients compared to long-acting beta2-agonists. Respir. Med. 2007, 101, 1798–1803. [Google Scholar] [CrossRef] [PubMed]
- Bouloukaki, I.; Tzanakis, N.; Mermigkis, C.; Giannadaki, K.; Moniaki, V.; Mauroudi, E.; Michelakis, S.; Schiza, S.E. Tiotropium Respimat Soft Mist Inhaler versus HandiHaler to improve sleeping oxygen saturation and sleep quality in COPD. Sleep Breath. 2016, 20, 605–612. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Calverley, P.M.; Lee, A.; Edwards, J.C. Long-acting inhaled anticholinergic therapy improves sleeping oxygen saturation in COPD. Eur. Respir. J. 2004, 23, 825–831. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Median | IQR |
|---|---|---|
| Age | 77.00 | (67–83) |
| Gender (n, %) Male | 9 | (81.8%) |
| GOLD (n, %) | ||
| 1–2 (FEV1 ≧ 50%) | 5 | (45.5%) |
| 3–4 (FEV1 < 50%) | 6 | (54.5%) |
| Group (n, %) | ||
| B | 4 | (36.4%) |
| D | 7 | (63.6%) |
| Comorbidities (n, %) | ||
| Cardiovascular disease | 6 | (42.9%) |
| Diabetes Mellitus | 3 | (21.4%) |
| Chronic liver disease | 1 | (7.1%) |
| Chronic renal disease | 1 | (7.1%) |
| Chronic neurogenic disease | 2 | (14.3%) |
| SOFA score | 5.0 | (4–8) |
| APACHE-Ⅱ score | 21.0 | (17.5–25.0) |
| Pulmonary Function test | ||
| FEV1 (L) | 1.13 | (0.71–1.55) |
| FEV1(%) | 43 | (28–75) |
| FEV1/FVC (%) | 54 | (44–70) |
| Vital signs (at baseline) | ||
| HR (beats/min) | 74 | (57–103) |
| MAP (mmHg) | 76 | (61–84) |
| Arterial blood gas (at baseline) | ||
| PH | 7.45 | (7.38–7.46) |
| PaO2 | 74.4 | (70–82.6) |
| HCO3− | 27.4 | (22.8–30.6) |
| PaCO2 | 37.9 | (31.8–52.3) |
| PaO2/FiO2 | 191.0 | (175–221) |
| Parameters | Zero | 1st h | 3rd h | 6th h | 12th h | 24th h | p |
|---|---|---|---|---|---|---|---|
| PIP | 24.0 (18–36) | 24.0 (19–39) | 26.0 (20–30) | 22.0 (18–32) | 27.0 (19–35) | 25.0 (21–33) | 0.775 |
| Pplat | 15.50 (13–17) | 14.0 (13–16) | 15.0 (14–15.8) | 15.0 (13.3–15.8) | 15.0 (14–16.8) | 15.5 (14.3–17.5) | 0.680 |
| Pmean | 9.00 (9–11) | 9.0 (8–10) | 9.0 (8–10) | 9.0 (7–11) | 9.0 (8–11) | 9.0 (9–11) | 0.864 |
| PEEP | 5.00 (4.25–5) | 5.0 (4.25–5) | 5.0 (5–5) | 5.0 (5–5) | 5.0 (4.25–5) | 5.0 (4.25–5) | 0.940 |
| RR | 16.00 (14–18) | 15.0 (14–18) | 16.0 (14–18) | 14.0 (14–20) | 15.0 (14–16) | 14.0 (14–15) | 0.132 |
| MVi | 7.65 (6.88–8.05) | 6.85 (5.7–7.93) | 7.3 (6–8.7) | 6.65 (5.85–8.45) | 7.1 (5.9–8.28) | 7.65 (6.25–7.98) | 0.069 |
| MVe | 7.70 (7–8.4) | 7.40 (5.7–8.6) | 7.6 (6.1–9) | 7.0 (6.1–9.1) | 7.4 (6.2–8.2) | 7.6 (6.2–7.9) | 0.247 |
| VTi | 472.0 (445–505) | 470.0 (445–498) | 471.0 (446–503) | 468.0 (446–498) | 474.0 (445–518) | 477.0 (446–545) | 0.150 |
| VTe | 467.0 (432–516) | 475.0 (432–477) | 463.0 (405–474) | 469.0 (422–497) | 483.0 (452–506) | 466.0 (433–554) | 0.172 |
| Rrs | 18.0 (11.5–31.5) | 22.0 (14–28.2) | 23.0 (14–24) | 19.0 (13.5–22.3) | 22.0 (16–24.8) | 21.0 (16.5–26) | 0.356 |
| Parameters | Zero Time | 3rd h | 24th h | p Value | p Value | ||
|---|---|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | Zero vs. 3rd h | Zero vs. 24th h | 3rd h vs. 24th h | ||
| Physiology parameters | |||||||
| HR | 74.0 (57–103) | 82.0 (64–97) | 75.0 (61–92) | 0.850 | |||
| MAP | 76.0 (61–84) | 72.0 (62–88) | 66.0 (61–74) | 0.643 | |||
| Blood gas parameters | |||||||
| PH | 7.45 (70–82.6) | 7.42 (7.39–7.47) | 7.44 (7.4–7.47) | 0.746 | |||
| PaO2 | 74.4 (31.8–52.3) | 80.8 (71.1–99.9) | 84.8 (81–107.2) | 0.078 | |||
| PaCO2 | 37.9 (22.8–30.6) | 40.0 (35–54.4) | 40.8 (32.7–44.5) | 0.850 | |||
| HCO3- | 27.4 (22.8–30.6) | 26.6 (23.4–30.6) | 26.7 (21.1–34.9) | 0.423 | |||
| BEB | 2.1 (−2.15–6.93) | 1.6 (−1.88–6.73) | 3.7 (0.8–7.95) | 0.301 | |||
| FiO2 | 0.4 (0.4–0.4) | 0.4 (0.3–0.4) | 0.4 (0.3–0.4) | 0.050 | |||
| PaO2/FiO2 | 191.0 (175–221) | 221.75 (202–292) | 246.7 (211.25–324) | 0.012 * | 0.407 | 0.009 ** | 0.407 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, P.-K.; Wei, Y.-F.; Sheu, C.-C.; Wang, C.-Y.; Hsu, C.-K.; Chen, C.-M.; Chen, W.-C.; Yang, K.-Y. Effect of Tiotropium Soft Mist Inhalers on Dynamic Changes in Lung Mechanics of Patients with Chronic Obstructive Pulmonary Disease Receiving Mechanical Ventilation: A Prospective Pilot Study. Pharmaceutics 2021, 13, 51. https://doi.org/10.3390/pharmaceutics13010051
Fu P-K, Wei Y-F, Sheu C-C, Wang C-Y, Hsu C-K, Chen C-M, Chen W-C, Yang K-Y. Effect of Tiotropium Soft Mist Inhalers on Dynamic Changes in Lung Mechanics of Patients with Chronic Obstructive Pulmonary Disease Receiving Mechanical Ventilation: A Prospective Pilot Study. Pharmaceutics. 2021; 13(1):51. https://doi.org/10.3390/pharmaceutics13010051
Chicago/Turabian StyleFu, Pin-Kuei, Yu-Feng Wei, Chau-Chyun Sheu, Chen-Yu Wang, Chi-Kuei Hsu, Chia-Min Chen, Wei-Chih Chen, and Kuang-Yao Yang. 2021. "Effect of Tiotropium Soft Mist Inhalers on Dynamic Changes in Lung Mechanics of Patients with Chronic Obstructive Pulmonary Disease Receiving Mechanical Ventilation: A Prospective Pilot Study" Pharmaceutics 13, no. 1: 51. https://doi.org/10.3390/pharmaceutics13010051
APA StyleFu, P. -K., Wei, Y. -F., Sheu, C. -C., Wang, C. -Y., Hsu, C. -K., Chen, C. -M., Chen, W. -C., & Yang, K. -Y. (2021). Effect of Tiotropium Soft Mist Inhalers on Dynamic Changes in Lung Mechanics of Patients with Chronic Obstructive Pulmonary Disease Receiving Mechanical Ventilation: A Prospective Pilot Study. Pharmaceutics, 13(1), 51. https://doi.org/10.3390/pharmaceutics13010051