1. Introduction
Over the past fifty years, major public health concern for cancer diseases has been rising, especially for lung cancer, which is the most common cancer diagnosed in the world, contributing to 37% of the leading causes of cancer-related death worldwide from total deaths in 2018 [
1]. There are two main categories of lung cancer—non-small cell lung carcinoma (NSCLC), which makes up 85% of cases, while small-cell lung carcinoma (SCLC) amounts to 15% of cases among all lung cancer cases [
2]. A significant factor that leads to lung cancer is cigarette smoking. However, increasing lung cancer cases among non-smokers are quite alarming nowadays [
3].
Different stages of lung cancer with different treatments are the primary reason for the low survival rate of cancer patients. Likewise, in other cancer cases, detection and confirmation usually can only be made at stage four (IV) [
4]. The current treatments used for lung cancer are surgery, chemotherapy, and radiation therapy depending on the stage and overall performance of cancer cells. For the advanced stage of lung cancer, chemotherapy is the first-line treatment, where most of the treatments are available as intravenous (IV) formulations into systematic circulation [
5]. Cancer chemotherapeutic drugs are usually used to destroy cancer cells by preventing the cancer cell from growing, dividing, and producing more cells. Conventionally, a patient who undergoes chemotherapy will be given a single or multi-drug at a time—for example, either Cis or Gem alone or a combination of both drugs. It was found that the combination of drugs improved the survival rate among cancer patients compared to single drug usage [
6]. This has shown that the optimum dosage of the combination of drugs can be efficient in increasing the survival rate of the lung cancer patient as well as help minimize side effects such as vomiting, sore throat, chest congestion, and nausea [
7].
Generally, Gem and Cis are administered at a higher dosage of 1.250 and 0.075 g/m
2 per cycle, respectively, which will lead to higher toxicity [
8]. Cancer chemotherapeutic drugs that are administered orally are always limited due to the first-pass metabolism, where the drug concentration is usually reduced as it passes through the gastrointestinal tract, before the drug can access the systematic circulation [
9]. Multi-drug resistance (MDR) in lung cancer stem-like cells (CSC) becomes a limitation to the combination of cancer therapy even though the dual drug has the potential to improve cancer treatment by reducing the drug dosage which leads to less side effects [
10]. The suitability of the liposomal Gem-HCl formulation in dry powder form, developed by Gandhi et al. [
11], was confirmed for lung cancer through in vitro aerosol delivery with deposition of formulation around the trachea and upper portion of the lung. As studied by Levet et al. [
12], a dry powder form of Cis also showed deposition of formulation in the deeper lung with controlled-release of Cis at high doses. Thus, a more efficient carrier for this combination of drugs should be developed to improve the delivery of both drugs to the lung (targeted site).
The demand for nanocarriers for drug administration in medical applications, especially in chemotherapy treatment, has increased as drug development is advancing. Nanocarriers are believed to have great potential in the delivery of single or multiple drugs (at low-dosage drug) to tissue tumors by overcoming biological barriers and can reach the tiniest area in the body due to their small particle size. Furthermore, most of the nanocarrier systems increase the effectiveness of chemotherapy and minimize side effects by enhancing the deposition of the drug at the tumor based on their stability and permeability [
13]. Nanocarriers provide a larger surface area, have the potential to increase solubility, improve the controlled release of the drug, and enhance the bioavailability in the delivery of chemotherapy drugs to the targeted tumor area. There are a few nanocarriers currently being used as targeting drug delivery systems, such as micelles, dendrimers, nanoparticles, liposomes, and niosomes [
14].
Among these nanocarriers, liposomes and niosomes have great potential in multiple drug delivery. Niosomes are formed of bilayer spherical vesicles, which consist of nonionic surfactants and cholesterol in an aqueous medium [
15], while liposomes are bilayer vesicles made by phospholipids enclosing an aqueous medium [
16]. Both have efficiency in encapsulating hydrophilic and hydrophobic drugs at the aqueous layer and the lipid bilayer, respectively. However, liposomes are less suitable because of their instability due to oxidation or hydrolysis of phospholipids, they need special storage conditions in a dark area sealed with nitrogen, and the materials used to produce liposomes are expensive [
17]. Nonionic surfactants are commonly used in the preparation of niosomes due to their high degree of compatibility with other ingredients. As membrane additives to the bilayer composition of niosomes, cholesterol enhances the stability and reduces the leakage of vesicles, which will increase the entrapment efficiency of the drug [
18]. Niosomes are chemically stable, have high compatibility with biological systems, and low toxicity because of their nonionic nature [
19].
Therefore, it is not surprising that niosomes (as nanocarrier) are currently being used to deliver drugs such as (i) 5-Fluorouracil, increasing drug penetration in skin cancer treatment; (ii) tamoxifen citrate, providing higher cytotoxicity against breast cancer cells; and (iii) curcumin, giving more significant apoptotic effect towards ovarian cancer cells [
20]. However, there is no study which has been conducted on dual drug usage (Cis and Gem) to treat lung cancer via aerosolization. Thus, this research aims to prepare and optimize a niosome formulation intended for aerosol delivery containing Gem and Cis using Mixture Experimental Design (MED). The physicochemical characterization, aerosol output, and stability of the optimized niosome formulation were investigated. The in vitro drug release and cytotoxicity study towards lung cancer (A549) cell lines were also evaluated.
2. Materials and Methods
2.1. Materials
Gem and Cis were purchased from AK Scientific (Ahern Avenue, Union City, CA, USA). Sorbitan monostearate (Span 60) and polyoxyethylene sorbitan tristearate (Tween 65) were purchased from Fluka (Loughborough, UK). Sodium dodecyl sulfate (SDS), sodium chloride (NaCl), and acetone were purchased from Merck (Darmstadt, Germany). Cholesterol, phosphate buffered saline (PBS, pH 7.4), and simulated lung fluid (SLF, pH 7.4 and 6.7) were supplied by R & M Chemical (Selangor, Malaysia). Glycerol was purchased from Fisher Scientific (Loughborough, UK). Deionized water was from a Milli-Q filtration system, EMD Millipore (Billerica, MA, USA).
2.2. Drug Solubility Study
A combination of drug Gem and Cis (0.10% w/w) with ratio 1:1 was added into 5.00 g of NaCl solution (0.90% w/v in deionized water). The mixture was stirred in a water bath at 1000 rpm, 27 °C for 15 min using the water bath technique on a magnetic stirrer (MS-H280-Pro, Scilogex LC, Rocky Hill, CT, USA) until all the Gem and Cis were dissolved and a clear NaCl solution was observed. Another 0.10% w/w of Gem and Cis was added into the previous NaCl solution until a clear solution was formed. The step of Gem and Cis addition (0.10% w/w) was repeated until a non-clear and precipitation of the drug in NaCl solution was observed. The total percentage of the combination of Gem and Cis that successfully dissolved in the clear NaCl with no precipitation signs after centrifuging using a centrifuge (EBA 200, Hettich, GmbH & Co., KG, Tuttlingen, Germany) at 4000 rpm for 15 min was recorded as the highest amount of gemcitabine and cisplatin that can be dissolved in NaCl solution.
2.3. Preparation of Niosome Formulation
NGC was prepared according to the heating method described by Basiri et al. [
21] with some modifications. For the lipid phase, a combination of surfactants (Tween 65: Span 60 with a ratio of 1:2) was mixed using a magnetic stirrer at 800 rpm, 120 °C for 5 min in an amber glass Schott bottle. Cholesterol was added into the mixture and further homogenized for 30 min. SDS was then added into the mixture, and then, continuously heated at 120 °C for 30 min. Glycerol solution (3%
w/
w in PBS pH 7.4) was added into the mixture dropwise and then, continuously heated at 60 °C for 45 min. The final mixture was sonicated using a bath sonicator (Powersonic 405, Hwashin Technology, Seoul, Korea) at 27 °C for 15 min.
For the aqueous phase, Gem and Cis were mixed in a NaCl solution (0.90% w/v), which had been sonicated at 27 °C for 15 min. Then, the mixture was stirred for 15 min using a magnetic stirrer at 1000 rpm. The mixture was added into the lipid phase and continuously homogenized by a magnetic stirrer at 1000 rpm, 60 °C for 60 min. Finally, the sample was sonicated using a probe sonicator (Vibra Cells, Sonics, Newtown, CT, USA) for 30 s “on” and 5 s “off” for four cycles.
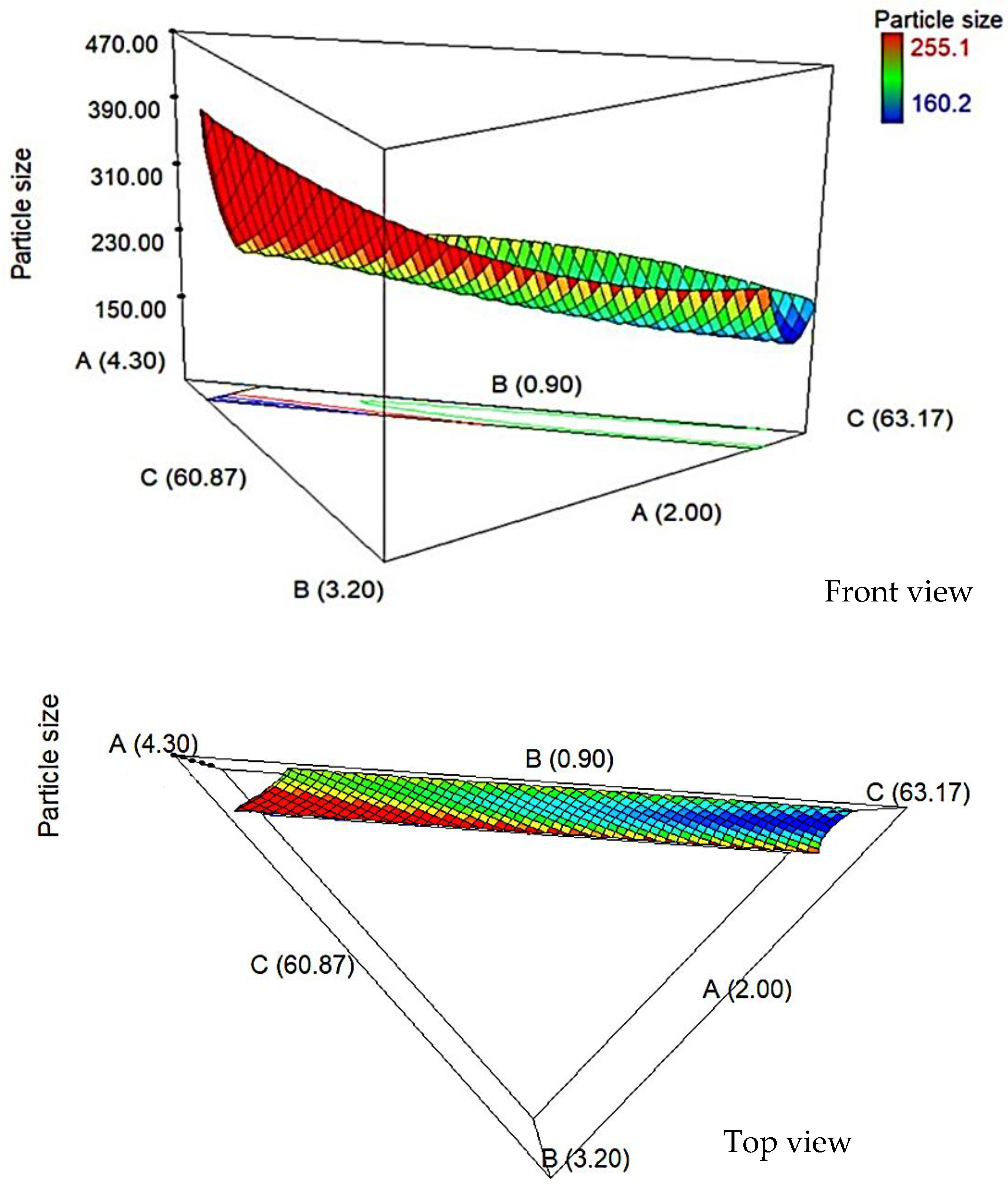
2.4. Optimization of the Niosome Formulation
2.4.1. Experimental Design
The niosome formulation was optimized using the D-optimal mixture design according to the method used by Arbain et al. [
22]. The results were statistically analyzed using Design-Expert, Version 7.0 (Stat-Ease Inc., Minneapolis, MN, USA, 2005) and Statistica, Version 12 (Statsoft Inc., Tulsa, OK, USA, 2013). In this preliminary study, the lower and the higher limits of the independent variables were determined by the software. The minimum and maximum proportions of these components are listed in
Table 1, while Cis (0.05%
w/
w), Gem (0.05%
w/
w), NaCl solution (33.33%
w/
w), and SDS (0.50%
w/
w) were kept constant. The independent variables were utilized to investigate the effect of percentage of surfactant, cholesterol, and glycerol solution on a response variable (particle size) of niosome formulation. The three-dimensional surface graphs were plotted to show the effect of independent variables on the response variable. The optimal compositions for niosome formulation with minimum response variables were chosen.
2.4.2. Statistical Analysis
Analysis of variance (ANOVA) and R2 (coefficient of determination) were carried out to investigate the significant differences among the independent variables. In order to obtain the final model with a very high correlation, Prob > F value must be significant (<0.05) and the value of R2 must be higher than 0.9. A non-significant lack of fit and desirable adequate precision greater than 4.00 indicated that the model could be used to navigate the space.
2.4.3. Verification of Models
The optimum composition was selected from the designed model by the D-optimal mixture design that gives a minimum particle size. Several random formulations were prepared according to the range variables to validate the obtained models and compare the actual and predicted values using Equation (1):
2.5. Physicochemical Characterization
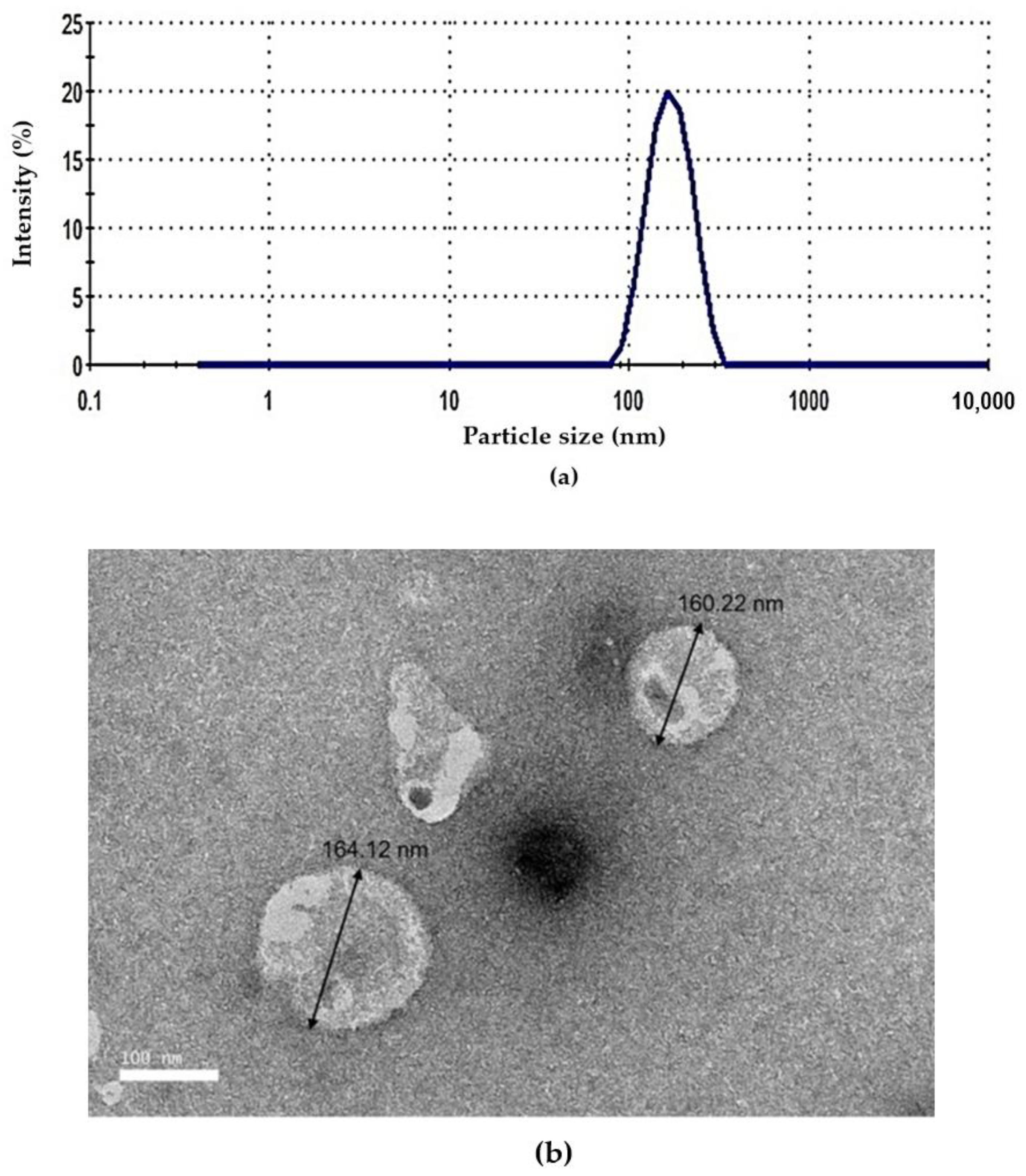
2.5.1. Particle Size, Polydispersity Index (PDI) and Zeta Potential Measurement
Particle size, polydispersity index, and zeta potential were measured using the Dynamic Light Scattering (DLS) technique which scattered at the angle of 173° and temperature of 25 °C. This process was carried out using the Malvern Nano ZS90 (Malvern Instrument, Malvern, UK). Niosome formulation was diluted with PBS (1:100) and injected into the sample cell. The measurement was repeated in triplicate. The calculation of zeta potential was performed based on the measurement of the electrophoretic mobility of dispersed particles in a charged field.
2.5.2. pH Measurement
The pH of the niosome formulation was measured using a Delta 320 pH meter (Mettler-Toledo, Schwerzenbach, Switzerland) at room temperature. The pH meter was calibrated with pH standard buffer solutions before measurements. The average value of pH from the three readings was calculated.
2.5.3. Surface Tension Measurement
The surface tension of niosome formulation was determined using a KSV Sigma 702 tension meter (Biolin Scientific, Espoo, Finland) by a ring method. Before measuring, the platinum ring was cleaned with acetone and washed thoroughly with deionized water, then burnt red using the Bunsen burner. The Du Noüy ring method was applied. Therefore, calibration with the deionized water must be taken at 72 mN/m. The ring was submerged in the sample and then, slowly lifted out of the liquid. The average of the surface tension values was calculated (n = 3).
2.6. Drug Entrapment Efficiency Measurement
The entrapment efficiency (EE %) can be determined using centrifugation of 1 mL of the formulation at 21,000 rpm for 1 h. The supernatant and the sediment were separated and then, diluted to 25 mL with SLF pH 7.4, filtered using a PTFE syringe filter (0.22 μm pore size, Membrane Solutions, Auburn, WA, USA), and then, measured using a UV–vis spectrophotometer (Beckman, DU 530, Fullerton, CA, USA). The percentage of drug entrapment in niosomes was calculated using Equation (2).
2.7. Morphology
Transmission Electron Microscopy (TEM) was performed to investigate the morphology of niosome by placing a drop of niosome suspension onto carbon-coated copper grids (400-mesh pores). Niosome formulation was diluted with PBS, pH 7.4 (1:100). The sample was then negatively stained with 1% uranyl acetate for 10 min at room temperature. After the excess liquid was drained off with a filter paper, the grid containing niosome samples was observed by a Hitachi H-7100 Transmission Electron Microscope (Tokyo, Japan).
2.8. Aerosol Output
The aerosol output of the optimized niosome was evaluated according to the method used by [
23]. A total of 3.0 mL of optimized niosome was loaded in the medication compartment of an OMRON MicroAIR nebulizer (NE-U22V1, Kyoto, Japan) and was commenced to dryness on continuous mode. Aerosol output was calculated before and after nebulization (Equation (3)).
where W
initial was the weight of liquid present in the nebulizer before nebulization and W
final was the weight of liquid remaining after nebulization.
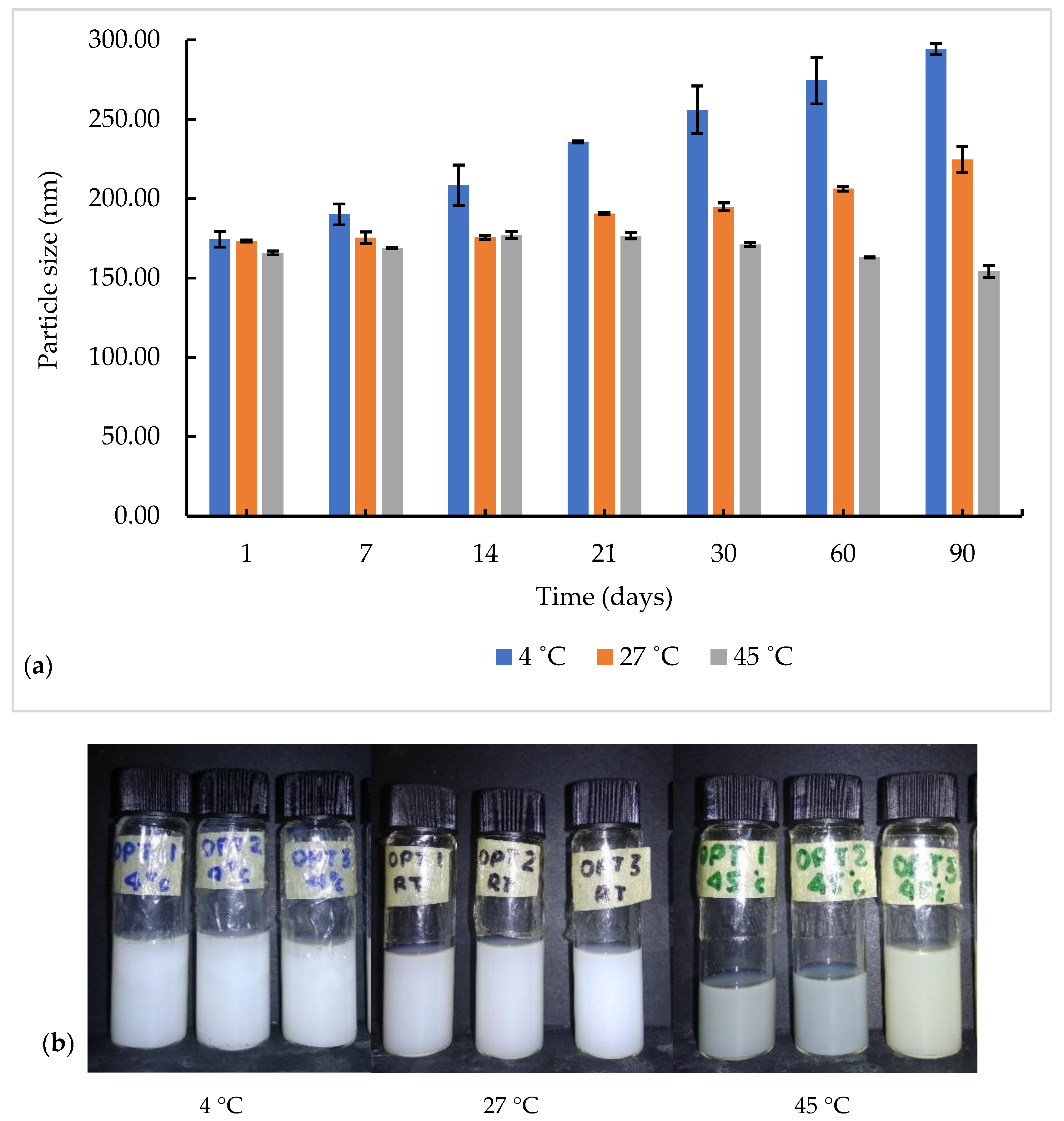
2.9. Stability Study
The optimized niosome formulation underwent a centrifugation test at 4000 rpm for 15 min. The sample was divided into three test tubes and kept at different storage temperatures (4, 27, and 45 °C) for 90 days. The physical appearance (no phase separation and no change in color), changes in particle size, and PDI with time were observed. The graphs of the particle size as a function of time at different temperatures were plotted.
2.10. In Vitro Drug Release Study
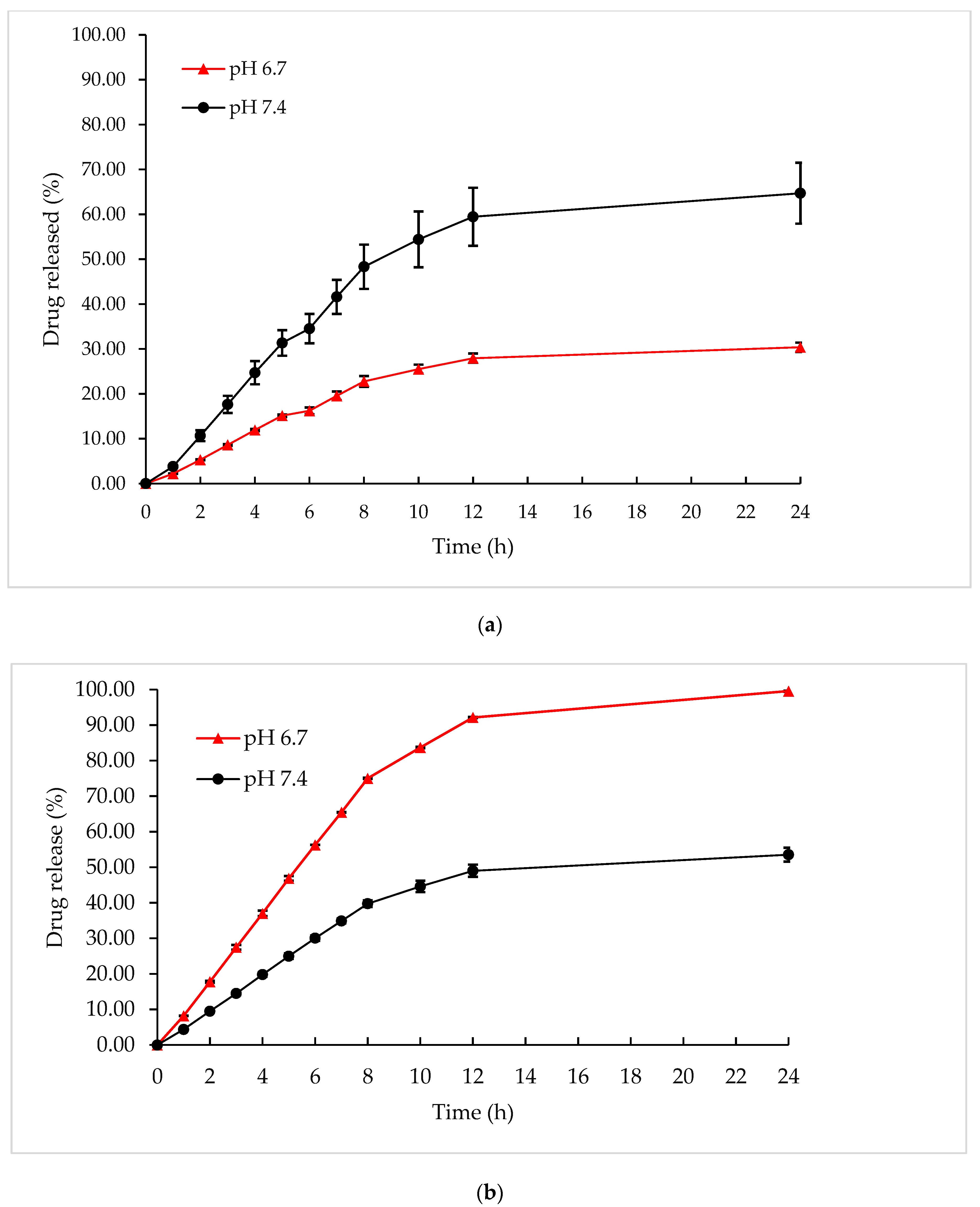
The diffusion of formulations was studied using the dialysis bag diffusion technique. Cellulose membranes were soaked overnight in the release medium. Then, 6.50 mL (M°Cis = 3.75 mg, M°Gem = 3.75 mg) of optimized niosome formulation was placed into the dialysis bag. Both ends of the bag were tied and then carefully immersed in a beaker containing a simulated lung fluid at pH 7.4, which mimicked the normal lung’s pH condition. The elution medium was stirred using a magnetic bar at 100 rpm. One milliliter of the receptor medium was withdrawn at different time intervals (typically at 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, and 24 h) and then, replaced with the same volume of fresh media to maintain the sink conditions. These procedures were repeated with simulated lung fluid pH 6.7, which mimicked the pH condition of lung cancer. All experiments were carried out in triplicate.
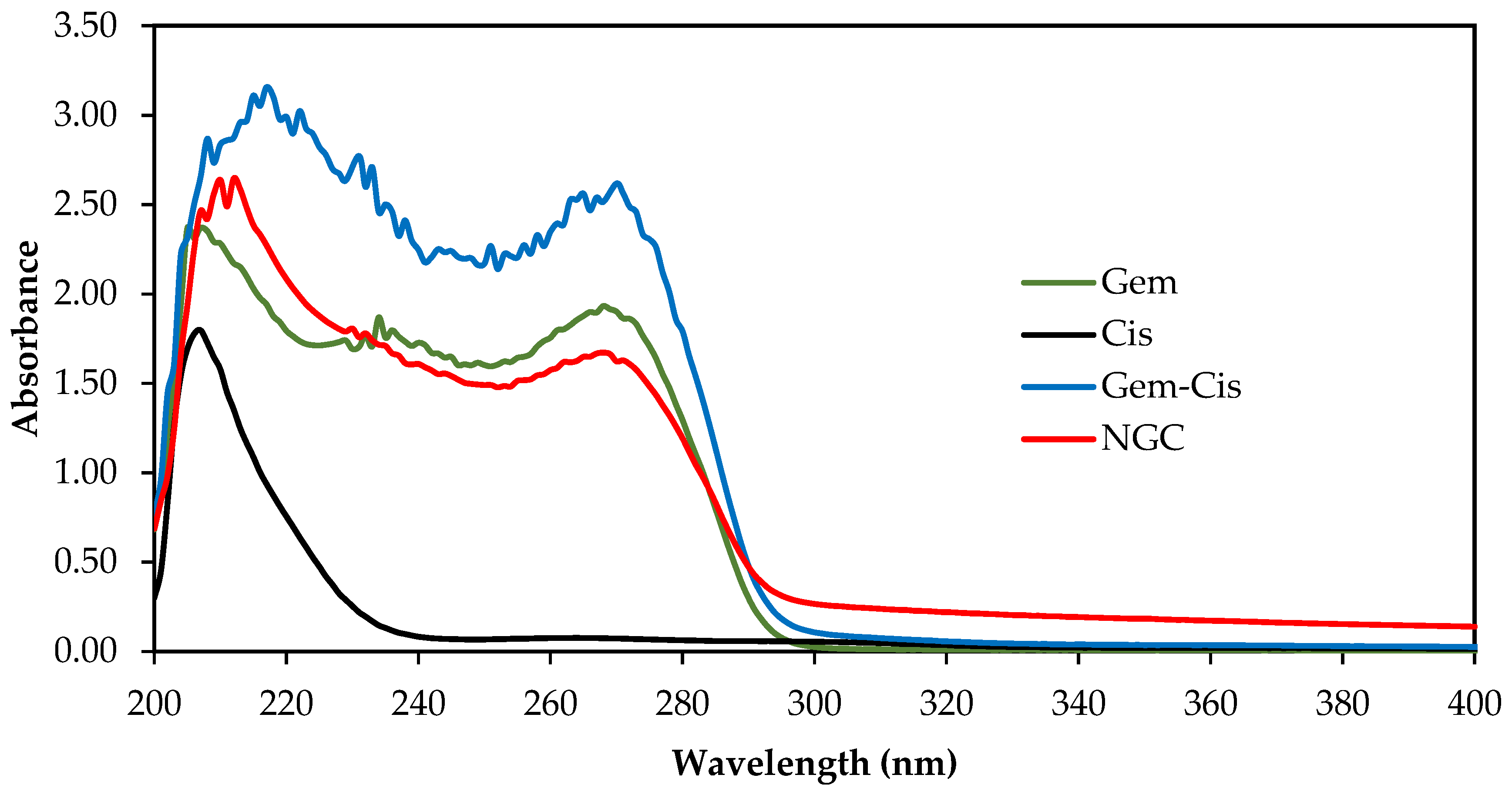
These samples were analyzed using a UV–vis spectrophotometer (Beckman, DU 530, Switzerland) at ʎ
max 207 nm for Cis and ʎ
max 268 nm for Gem to determine the amount of both drugs released. The calibration curves for Cis and Gem in simulated lung fluid at pH 7.4 and in simulated lung fluid at pH 6.7 were plotted separately to determine cumulative percentage of Cis and Gem released. The amount of drug released from NGC was calculated using the following equation:
where M
d is the concentration of Cis or Gem in the supernatant measured spectrophotometrically at λmax of Cis or Gem, V is the volume of the release media, and M°
d is the amount of Cis or Gem loading.
Kinetic Release Measurement
The following mathematical models were used to evaluate the kinetics and mechanism of drug release from optimized niosome formulation: zero-order (cumulative amount of drug release versus time, Equation (5)), first-order (log the cumulative amount of drug remaining versus time, Equation (6)), Higuchi (cumulative percentage of drug release versus square root of time, Equation (7)), Hixson–Crowell (cube root cumulative amount of drug remaining versus time, Equation (8)), and Korsmeyer–Peppas (log cumulative percentage of drug release versus log time, Equation (9)). The model that best fit the drug release data was selected based on the correlation coefficient (
R2) value obtained from the plotted graph in various models. The model that gave the highest value was considered as the best fit for release data.
where
is the initial amount of drug in dissolution media, M
t the amount of drug released in time,
,
,
,
are the release rate constants,
the fraction of drug release over time, n is the release exponent, and t is the time.
2.11. In Vitro Cytotoxicity Study on Normal Lung (MRC5) and Lung Cancer (A549) Cell Lines
MTT assay (3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide) on normal lung (MRC5) and lung cancer (A549) cell lines were used to determine the cytotoxicity of the optimized NGC. A concentration of 2 × 10
3 cells/mL was prepared and plated (100 µL/well) onto 96-well plates. The samples were diluted onto each well with identified concentrations 100.000, 50.000, 25.000, 12.500, 6.250, 3.125, and 1.560 μg/mL, and then, were further incubated for 72 h. MTT solution was added to each cell and continued for incubation in the incubator for 3 h. After solubilization of the purple formazan crystals using DMSO was completed, the Optical Density (OD) of the samples was measured using an ELISA reader at a wavelength of 570 nm. Cytotoxicity was recorded as the drug concentration causing 50% growth inhibition of the cells (IC
50 value) using Equation (10), given below:
After determination of the percentage of cell viability was completed, graphs of the percentage of cell viability against their respective concentrations were plotted. This experiment was repeated using a blank niosome formulation (without drugs).
Statistical Analysis
By using Statistical Analysis System (SAS) software version 4.3 (SPSS Inc., Chicago, IL, USA, 2013), the statistical analysis of variance (ANOVA) of the experiment was determined using two tests, which were a Type I t-test (least significant different, LSD) and Duncan’s Multiple Range Test. A p-value of less than 0.05 was considered significant. All experiments were carried out in triplicate. The mean values with standard deviation (SD) were represented as an error bar.
4. Conclusions
The results of this study demonstrated that the optimized NGC formulation was successfully formulated using a heating method with good stability and homogeneity against phase separation at different temperatures during 90 days of storage. This formulation has appropriate values in controlled drug release, is safe, and exhibits cell growth inhibition against A549 lung cancer cells. These studies suggested that the optimized NGC formulation has the potential to be used for cancer treatment with good entrapment efficiency and aerosol output. However, this should be further confirmed by performing cascade impactor analysis, which reported their benefits to correlate with the deposited drug into the lungs through inhalation.
A synergistic effect between Gem and Cis has been demonstrated in NSCLC, and their response rates are as high as 54%, as reported in the literature. On top of that, the synergistic effect between Gem and Cis in an optimized NGC formulation can be an interesting study to see the changes in their response rates against NSCLC. The unique mechanisms of action of Gem and Cis and their favorable toxicity profile make these drugs interesting prospects for combination chemotherapy.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}