
Chitosan–Platelet-Rich Plasma Implants Improve Rotator Cuff Repair in a Large Animal Model: Pivotal Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of the Freeze-Dried Chitosan Formulation
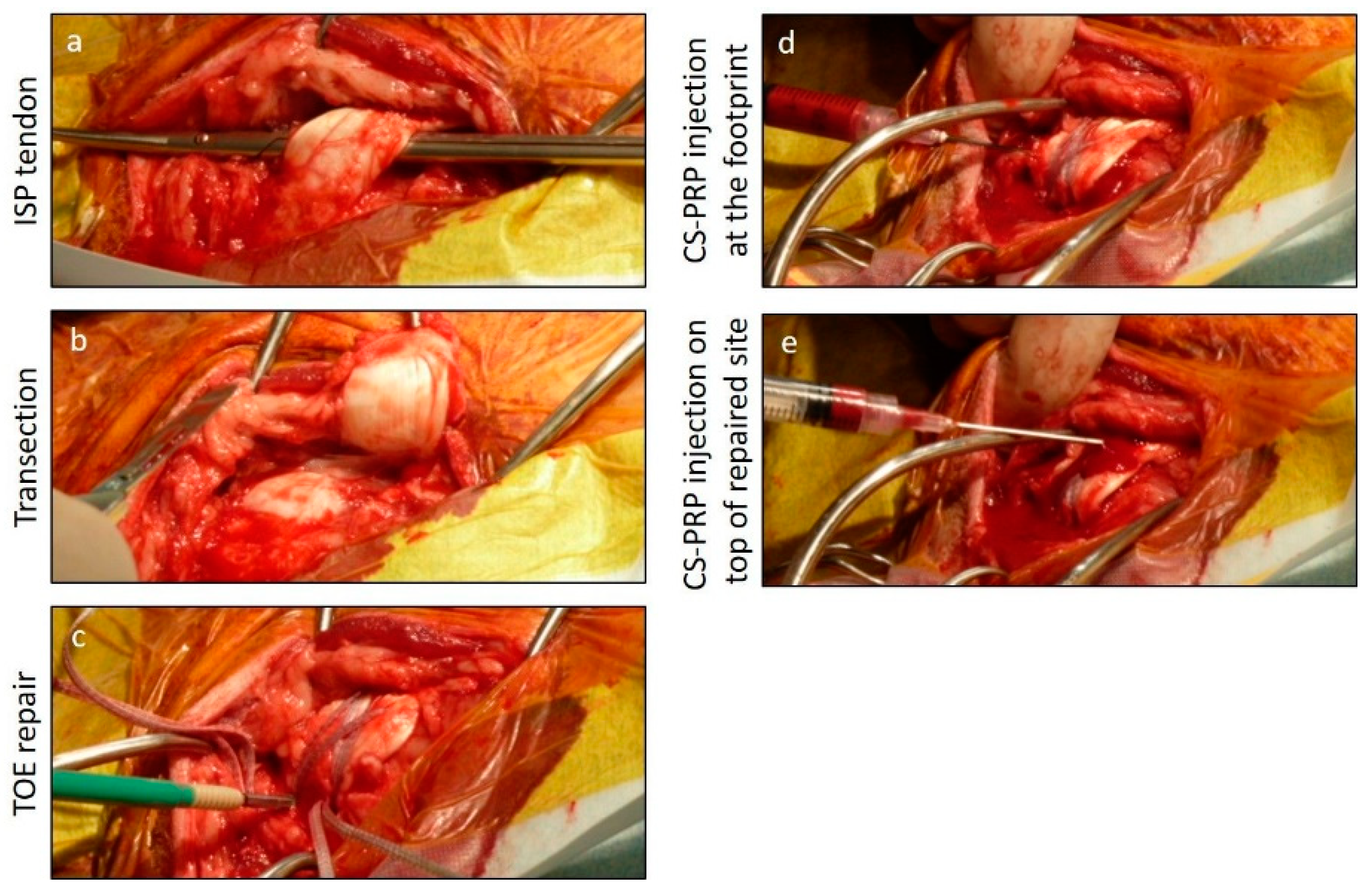
2.2. Rotator Cuff Tear Model and Study Design
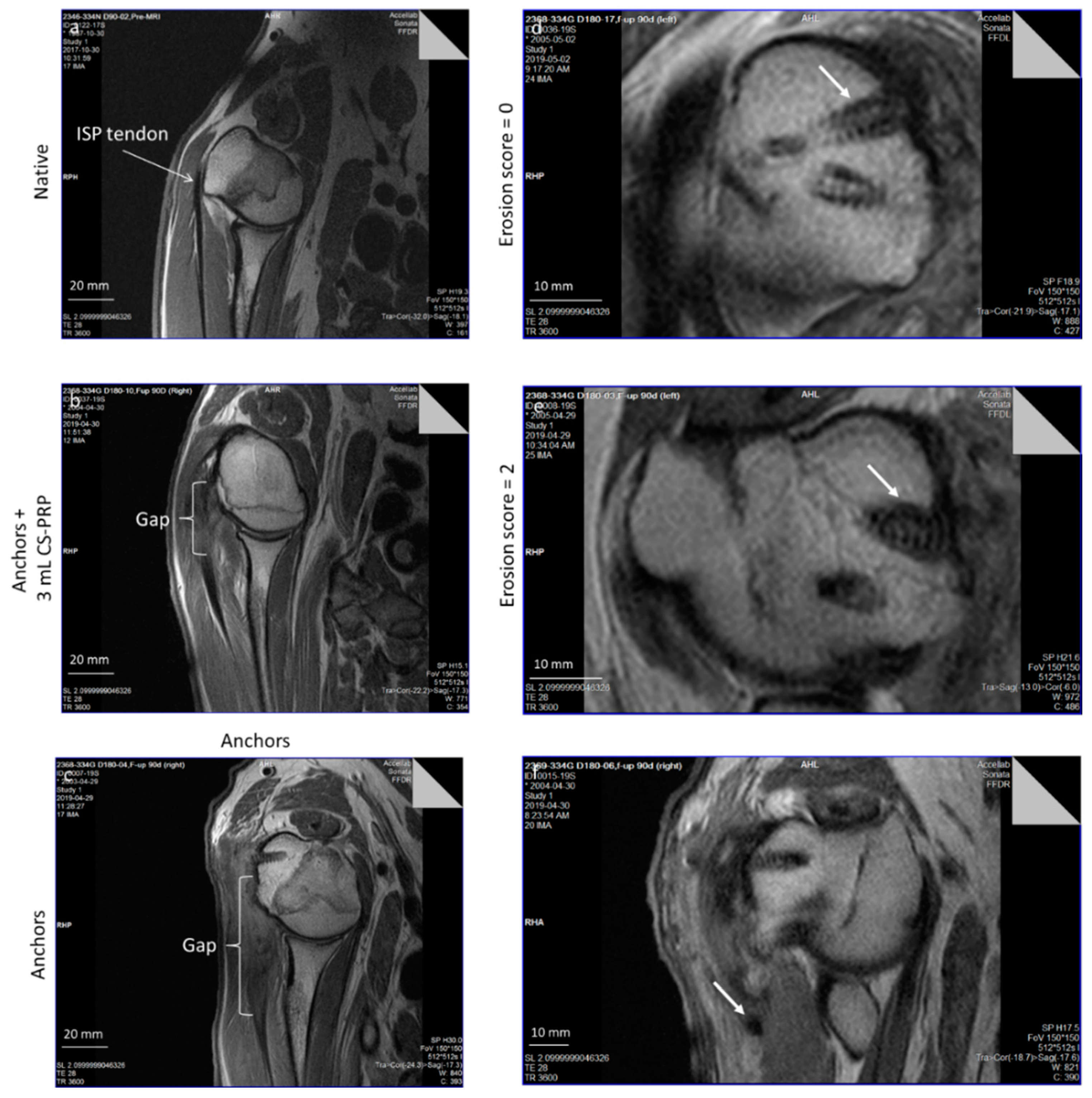
2.3. Magnetic Resonance Imaging (Mri) Imaging and Scoring
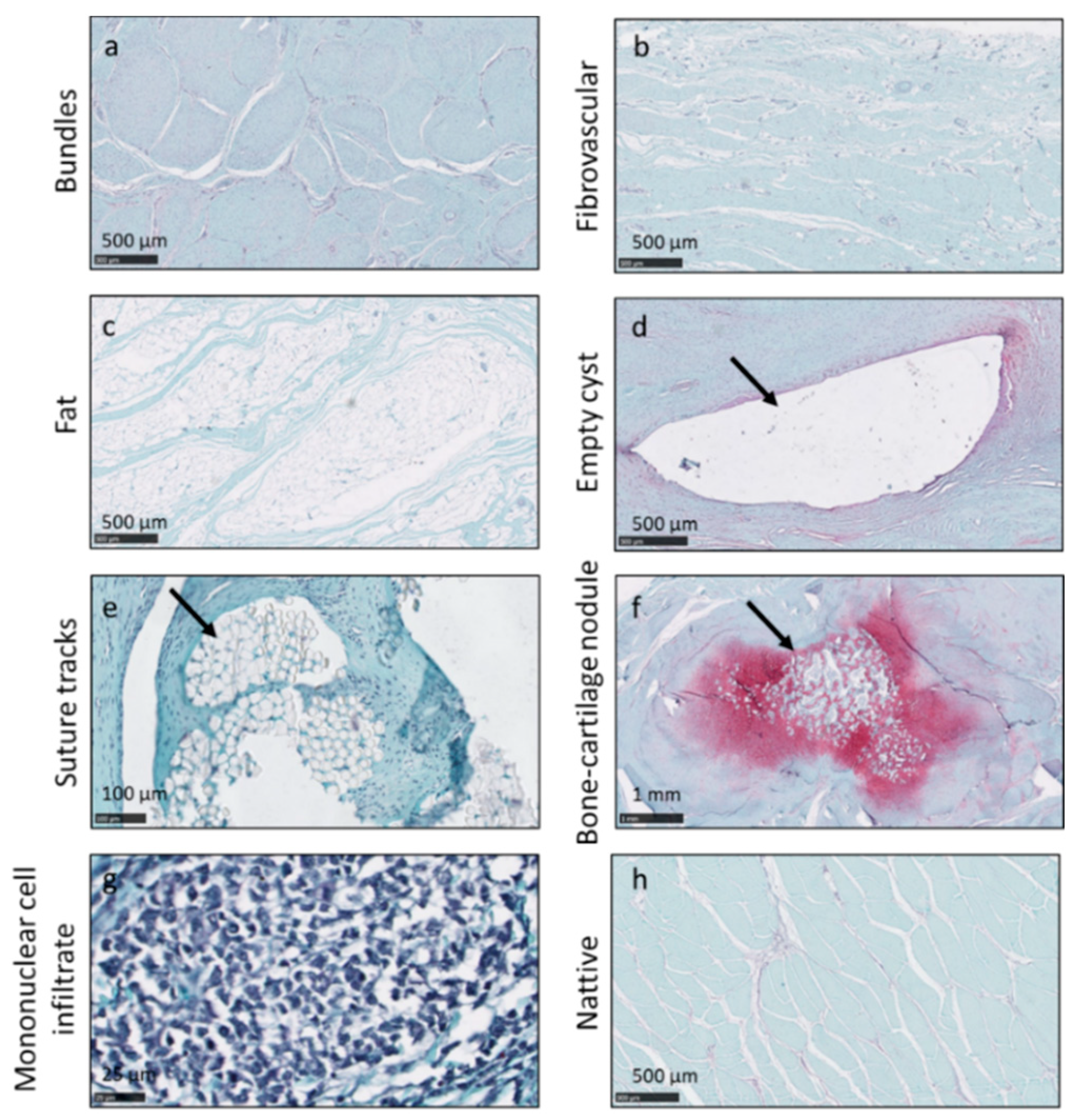
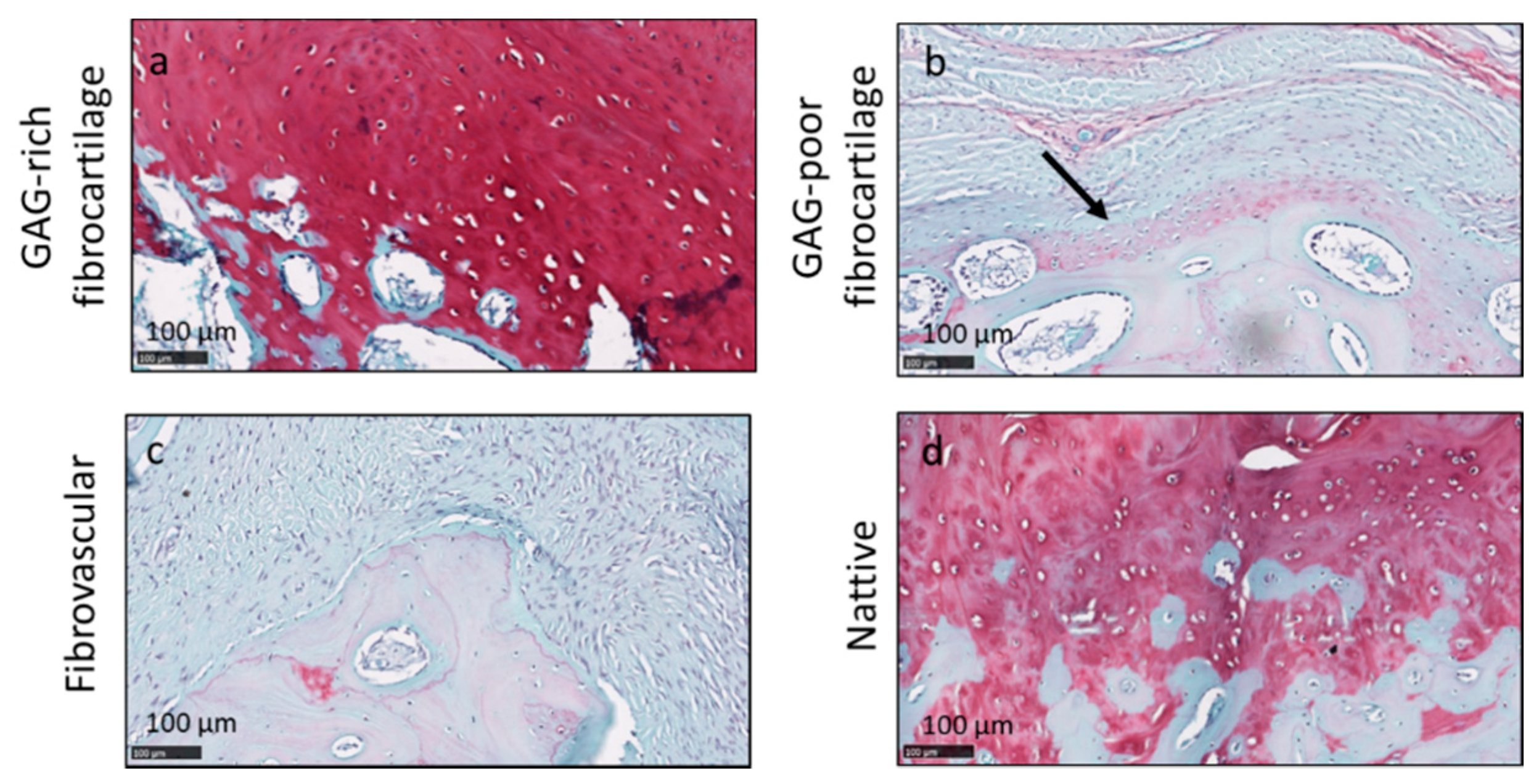
2.4. Histological Processing and Scoring
2.5. Additional Outcome Measures Collected
2.6. Statistical Analysis
3. Results
3.1. Chitosan–PRP Implants Decreased Tendon Gap at 3 Months Post-Operative
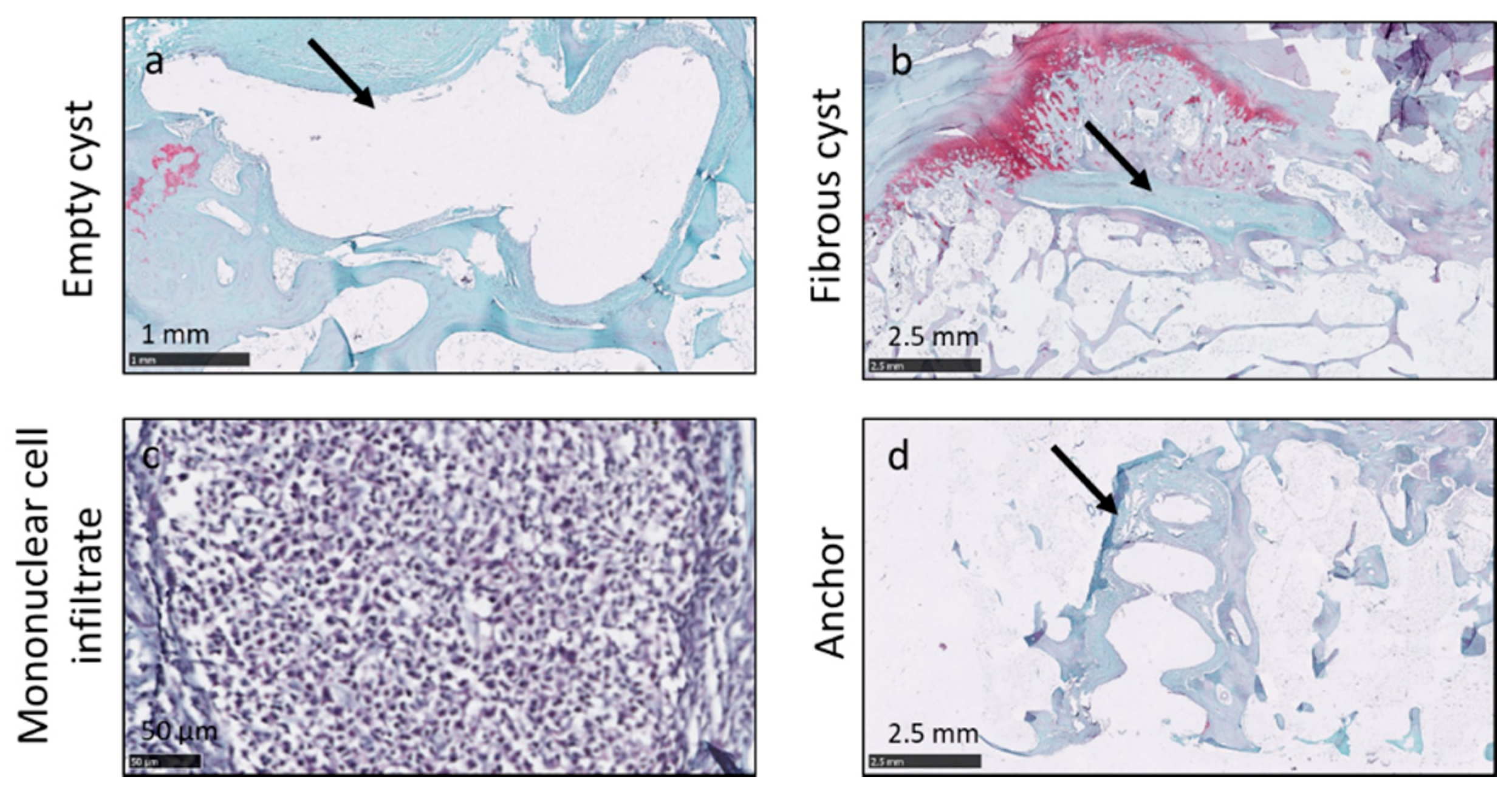
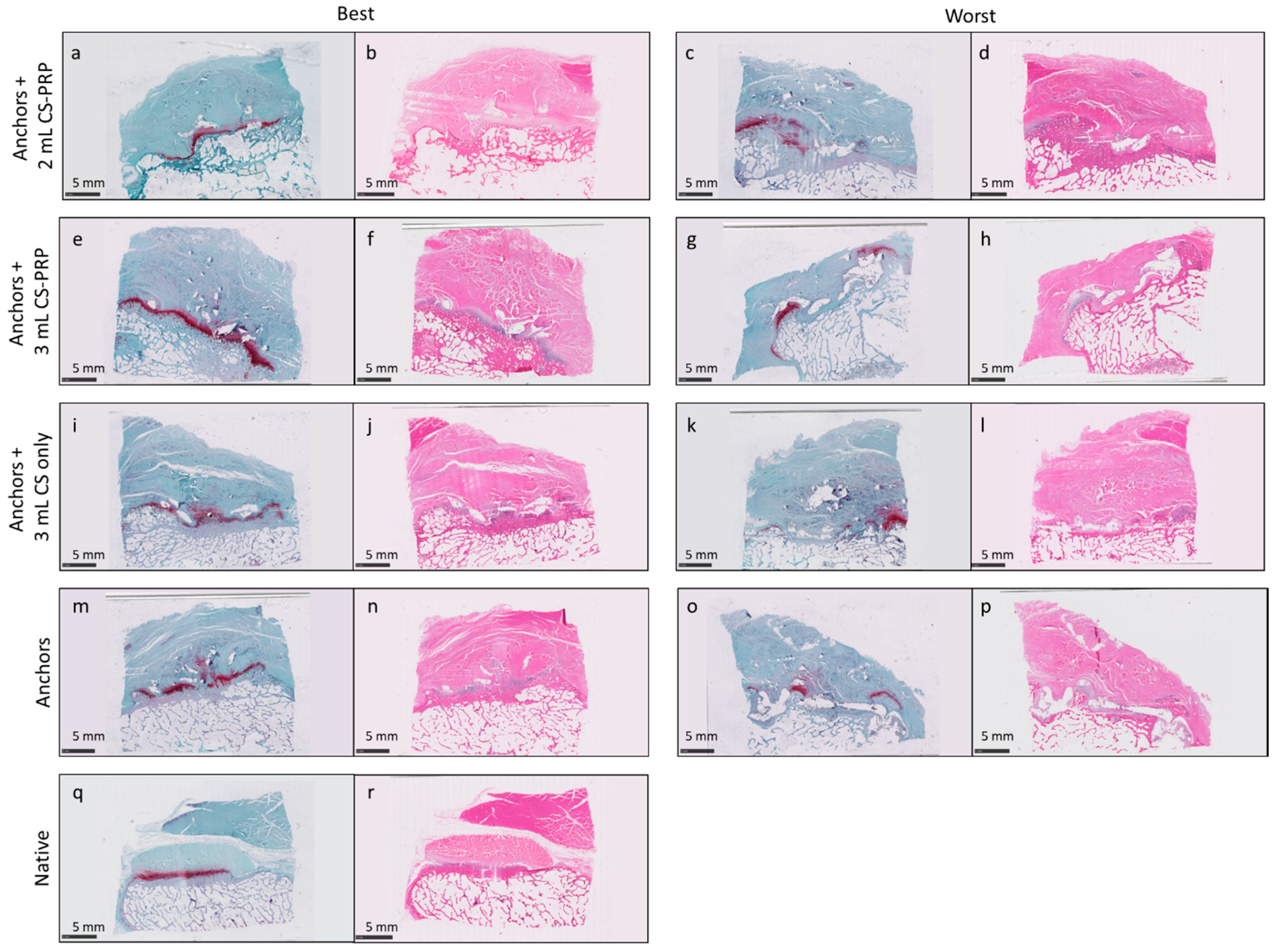
3.2. Chitosan–PRP Implants Improved Some Histopathological Features at 6 Months
3.3. No Treatment-Specific Effects on All Standard Safety Outcome Measures Were Detected
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamamoto, A.; Takagishi, K.; Osawa, T.; Yanagawa, T.; Nakajima, D.; Shitara, H.; Kobayashi, T. Prevalence and risk factors of a rotator cuff tear in the general population. J. Shoulder Elb. Surg. 2010, 19, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, H.; Yamamoto, N.; Abe, H.; Fukuda, M.; Seki, N.; Kikuchi, K.; Kijima, H.; Itoi, E. Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. J. Orthop. 2013, 10, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.L.; Briggs, L.; Murrell, G.A. Intraoperative determinants of rotator cuff repair integrity: An analysis of 500 consecutive repairs. Am. J. Sports Med. 2012, 40, 2771–2776. [Google Scholar] [CrossRef]
- Khazam, M.; Sager, B.; Box, H.N.; Wallace, S.B. The effect of age on risk of retear after rotator cuf repair: A systematic review and meta-analysis. JSES Int. 2020, 4, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Pandey, V.; Bandi, A.; Madi, S.; Agarwal, L.; Acharya, K.K.; Maddukuri, S.; Sambhaji, C.; Willems, W.J. Does application of moderately concentrated platelet-rich plasma improve clinical and structural outcome after arthroscopic repair of medium-sized to large rotator cuff tear? A randomized controlled trial. J. Shoulder Elb. Surg. 2016, 25, 1312–1322. [Google Scholar] [CrossRef]
- Snow, M.; Hussain, F.; Pagkalos, J.; Kowalski, T.; Green, M.; Massoud, S.; James, S. The effect of delayed injection of leukocyte-rich platelet-rich plasma following rotator cuff repair on patient function: A randomized double-blind controlled trial. Medicine 2020, 36, 648–657. [Google Scholar] [CrossRef]
- Bergeson, A.G.; Tashjian, R.Z.; Greis, P.E.; Crim, J.; Stoddard, G.J.; Burks, R.T. Effects of platelet-rich fibrin matrix on repair integrity of at-risk rotator cuff tears. Am. J. Sports Med. 2012, 40, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Chao, F.C.; Shepro, D.; Tullis, J.L.; Belamarich, F.A.; Curby, W.A. Similarities between platelet contraction and cellular motility during mitosis: Role of platelet microtubules in clot retraction. J. Cell Sci. 1976, 20, 569–588. [Google Scholar] [CrossRef]
- Cohen, I.; Gerrard, J.M.; White, J.G. Ultrastructure of clots during isometric contraction. J. Cell Biol. 1982, 93, 775–787. [Google Scholar] [CrossRef]
- Deprés-Tremblay, G.; Chevrier, A.; Tran-Khanh, N.; Nelea, M.; Buschmann, M.D. Chitosan inhibits platelet-mediated clot retraction, increases platelet-derived growth factor release, and increases residence time and bioactivity of platelet-rich plasma in vivo. Biomed. Mater. 2017, 13, 015005. [Google Scholar] [CrossRef]
- Chevrier, A.; Darras, V.; Picard, G.; Nelea, M.; Veilleux, D.; Lavertu, M.; Hoemann, C.D.; Buschmann, M.D. Injectable chitosan-platelet-rich plasma (PRP) implants to promote tissue regeneration: In vitro properties, in vivo residence, degradation, cell recruitment and vascularization. J. Tissue Eng. Regen. Med. 2018, 12, 217–228. [Google Scholar] [CrossRef]
- Ghazi Zadeh, L.; Chevrier, A.; Lamontagne, M.; Buschmann, M.D.; Hoemann, C.D.; Lavertu, M. Multiple platelet-rich plasma preparations can solubilize freeze-dried chitosan formulations to form injectable implants for orthopedic indications. Bio-Med. Mater. Eng. 2019, 30, 349–364. [Google Scholar] [CrossRef]
- Rezaei, F.S.; Sharifianjazi, F.; Esmaeilkhanian, A.; Salehi, E. Chitosan films and scaffolds for regenerative medicine applications: A review. Carbohydr. Polym. 2021, 273, 118631. [Google Scholar] [CrossRef]
- Shen, S.; Chen, X. Marine polysaccharides for wound dressings application: An overview. Pharmaceutics 2021, 13, 1666. [Google Scholar] [CrossRef] [PubMed]
- Shive, M.S.; Stanish, W.D.; McCormack, R.G.; Forriol, F.; Mohtadi, N.; Pelet, S.; Desnoyers, J.; Méthot, S.; Vehik, K.; Restrepo, A. BST-CarGel® Treatment Maintains Cartilage Repair Superiority over Microfracture at 5 Years in a Multicenter Randomized Controlled Trial. Cartilage 2015, 6, 62–72. [Google Scholar] [CrossRef]
- Melamed, E.; Beutel, B.G.; Robinson, D. Enhancement of acute tendon repair using chitosan matrix. Am. J. Oorthop. 2015, 44, 212–216. [Google Scholar]
- Deprés-Tremblay, G.; Chevrier, A.; Snow, M.; Rodeo, S.; Buschmann, M.D. Freeze-dried chitosan-platelet-rich plasma implants improve supraspinatus tendon attachment in a transosseous rotator cuff repair model in the rabbit. J. Biomed. Appl. 2019, 33, 792–807. [Google Scholar] [CrossRef]
- Deprés-Tremblay, G.; Chevrier, A.; Hurtig, M.B.; Snow, M.; Rodeo, S.; Buschmann, M.D. Freeze-dried chitosan-platelet-rich plasma implants for rotator cuff tear repair: Pilot ovine studies. ACS Biomater. Sci. Eng. 2018, 4, 3737–3746. [Google Scholar] [CrossRef] [PubMed]
- Chevrier, A.; Hurtig, M.B.; Lacasse, F.-X.; Lavertu, M.; Potter, H.; Pownder, S.; Rodeo, S.; Buschmann, M.D. Freeze-dried chitosan solubilised in platelet-rich plasma in a sheep model of rotator cuff repair. In Proceedings of the Orthopaedic Research Society, Austin, TX, USA, 10 April 2019. [Google Scholar]
- Kim, J.; Seo, B.S. How to calculate sample size and why. Clin. Orthop. Surg. 2013, 5, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Rodeo, S.A.; Potter, H.G.; Kawamura, S.; Turner, A.S.; Kim, H.J.; Atkinson, B.L. Biologic augmentation of rotator cuff tendon-healing with use of a mixture of osteoinductive growth factors. J. Bone Jt. Surg. 2007, 89, 2485–2497. [Google Scholar] [CrossRef]
- Provencher, M.T.; Kercher, J.S.; Galatz, L.M.; Elattrache, N.S.; Frank, R.M.; Cole, B.J. Evolution of rotator cuff repair techniques: Are our patients really benefiting? Instr. Course Lect. 2011, 60, 123–136. [Google Scholar]
- Derwin, K.A.; Baker, A.R.; Iannotti, J.P.; McCarron, J.A. Preclinical Models for Translating Regenerative Medicine Therapies for Rotator Cuff Repair. Tissue Eng. Part B Rev. 2010, 16, 21–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edelstein, L.; Thomas, S.J.; Soslowsky, L.J. Rotator Cuff Tears: What have we learned from animal models? J. Musculoskelet. Neuronal Interact. 2011, 11, 150–162. [Google Scholar]
- Turner, A.S. Experiences with sheep surgery: Strengths and as an animal model for shoulder shortcomings. J. Shoulder Elb. Surg. 2007, 16, 158S–163S. [Google Scholar] [CrossRef] [PubMed]
- Thomopoulos, S.; Parks, W.C.; Rifkin, D.B.; Derwin, K.A. Mechanisms of tendon injury and repair. J. Orthop. Res. 2015, 33, 832–839. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, I.; Green, K.L.; Smart, J.D.; Smistad, G.; Karlsen, J. Bioadhesion of hydrated chitosans: An in vitro and in vivo study. Int. J. Pharm. 1996, 145, 231–240. [Google Scholar] [CrossRef]
- Hoemann, C.D.; Chen, G.; Marchand, C.; Tran-Khanh, N.; Thibault, M.; Chevrier, A.; Sun, J.; Shive, M.S.; Fernandes, M.J.G.; Poubelle, P.E.; et al. Scaffold-Guided Subchondral Bone Repair Implication of Neutrophils and Alternatively Activated Arginase-1 + Macrophages. Am. J. Sports Med. 2010, 38, 1845–1856. [Google Scholar] [CrossRef]
- Abraham, A.C.; Shah, S.A.; Thomopoulos, S. Targeting Inflammation in Rotator Cuff Tendon Degeneration and Repair. Tech. Shoulder Elb. Surg. 2017, 18, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Sunwoo, J.Y.; Eliasberg, C.D. The role of the macrophage in tendinopathy and tendon healing. J. Orthop. Res. 2020, 38, 1666–1675. [Google Scholar] [CrossRef]
- Chow, J.C.; Gu, Y. Material reaction to suture anchor. Arthroscopy 2004, 20, 314–316. [Google Scholar] [CrossRef]
- Nusselt, T.; Freche, S.; Klinger, H.M.; Baums, M.H. Intraosseous foreign body granuloma in rotator cuff repair with bioabsorbable suture anchor. Arch. Orthop. Trauma Surg. 2010, 130, 1037–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, M.S.; Smith, R.D.J.; Nagra, N.; Wheway, K.; Watkins, B.; Snelling, S.; Dakin, S.G.; Carr, A.J. Rotator cuff repair with biological graft augmentation causes adverse tissue outcomes. Acta Orthop. 2020, 91, 782–788. [Google Scholar] [CrossRef]
- Gerber, C.; Meyer, D.C.; Schneeberger, A.G.; Hoppeler, H.; Von Rechenberg, B. Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: An experimental study in sheep. J. Bone Jt. Surg. 2004, 86A, 1973–1982. [Google Scholar] [CrossRef] [PubMed]
- Gerber, C.; Meyer, D.C.; Frey, E.; von Rechenberg, B.; Hoppeler, H.; Frigg, R.; Jost, B.; Zumstein, M.A. Neer Award 2007: Reversion of structural muscle changes caused by chronic rotator cuff tears using continuous musculotendinous traction. An experimental study in sheep. J. Shoulder Elb. Surg. 2009, 18, 163–171. [Google Scholar] [CrossRef]
- Gerber, C.; Meyer, D.C.; Flueck, M.; Benn, M.C.; von Rechenberg, B.; Wieser, K. Anabolic Steroids Reduce Muscle Degeneration Associated with Rotator Cuff Tendon Release in Sheep. Am. J. Sports Med. 2015, 43, 2393–2400. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Treatment | Dosage of Chitosan (mg) | Vehicle Used | Number of Animals | Time Point/Outcome Measure |
|---|---|---|---|---|---|
| 1 | Anchors + 2 mL CS-PRP | 20 | PRP | 12 | Baseline (Clinical pathology) 3 months (Clinical pathology + MRI) 6 months (Clinical pathology, MRI, Histopathology) |
| 2 | Anchors + 3 mL CS-PRP | 30 | PRP | 12 | |
| 3 | Anchors + 3 mL CS-water (Chitosan safety group) | 30 | Sterile water | 12 | |
| 4 | Anchors (Standard-of-care controls) | 0 | NA | 12 |
| Parameter Measured | Unit/Grade |
|---|---|
| Tendon gap 1 | mm |
| Tendon thickness 2 | mm |
| Tissue volume 3 | cc |
| Presence of bursitis | None = 0; Mild = 1; Moderate = 2; Severe = 3 |
| Synovial reaction | None = 0; Mild = 1; Moderate = 2; Severe = 3 |
| Heterotopic bone formation | None = 0; Mild = 1; Moderate = 2; Severe = 3 |
| Erosion of bone along the anchors | None = 0; At aperture only = 0.5; Along the entire anchor = 1 Note that each of 4 anchors were scored separately and then a sum was calculated Minimum score is 0 and maximum score is 4 |
| Cellularity | Score | Tenocytes | Score |
| None | 0 | Marked/Normal tenocyte cellularity | 0 |
| Minimal | 1 | Moderate (slight decrease tenocyte cellularity) | 1 |
| Mild | 2 | Mild | 2 |
| Moderate | 3 | Minimal | 3 |
| Marked | 4 | None | 4 |
| Vascularity | Score | Glycosaminoglycan Expression | Score |
| None | 0 | None | 0 |
| Minimal | 1 | Minimal | 1 |
| Mild | 2 | Mild | 2 |
| Moderate | 3 | Moderate | 3 |
| Marked | 4 | Marked | 4 |
| Inflammatory Cells in Tendon Tissue | Score | Structural Organization | Score |
| None (None observed and/or occasional isolated mononuclear cells) | 0 | Native tendon | 0 |
| Minimal (Few inflammatory cells) | 1 | Repair tissue mostly organized in bundles | 1 |
| Mild (More abundant inflammatory cells and/or locally extensive infiltration) | 2 | Repair tissue mostly aligned but not in bundles | 2 |
| Moderate (Larger locally extensive and/or more widespread inflammatory cell infiltration) | 3 | Repair tissue completely disorganized, but areas of tendon material can be identified | 3 |
| Marked (Dense inflammatory cell infiltration obscuring local architecture) | 4 | Complete loss of tendon architecture (minimal or no recognizable tendon material) | 4 |
| Structural Appearance of the Enthesis | Score |
| Native insertion with tidemark throughout | 0 |
| Insertion has continuity with bone ingrowth and fibrocartilage and tidemark partially present | 1 |
| Insertion has continuity with bone ingrowth and fibrocartilage cells but no tidemark | 2 |
| Insertion has continuity with fibrous tissue | 3 |
| Insertion has continuity with fat | 4 |
| No continuity | 5 |
| Glycosaminoglycans (GAG) at Insertion Site | Score |
| No change/typical appearance and/or subjective quantity of GAG staining | 0 |
| Slight (some GAG staining but faint), decreased compared to typical insertion site | 1 |
| None (complete absence of GAG staining) | 2 |
| Bone Remodeling at Insertion Site | Score |
| None | 0 |
| Minimal | 1 |
| Mild | 2 |
| Moderate | 3 |
| Marked | 4 |
| Pan-Enthesis Remodeling/Healing | Score |
| No healing of enthesis site (i.e., complete absence of tendon reattachment) | 0 |
| Partial healing of enthesis site (absence of fibrocartilage and/or nearly complete replacement by fibrous enthesis) with disorganized tendon bundles | 1 |
| Complete healing of enthesis site with moderate remodeling (remodeling characterized by the presence of: variable thickness of fibrocartilage layer and/or bone remodeling and/or large nodular regions of fibrocartilage) with mostly organized tendon bundles and some fibrocartilage present | 2 |
| Complete healing of enthesis site with mild remodeling (variable thickness of fibrocartilage layer and/or bone remodeling and/or large nodular regions of fibrocartilage) with mostly organized tendon bundles and organized fibrocartilage present along most of the enthesis site | 3 |
| Complete healing of enthesis site with a smaller degree of remodeling (variable thickness of fibrocartilage layer and/or bone remodeling and/or large nodular regions of fibrocartilage) with well-organized tendon bundles associated with organized fibrocartilage mostly present along enthesis site | 4 |
| Complete healing of enthesis site with well-organized repair tissue; appears very similar/identical to native enthesis; recapitulates native anatomy | 5 |
| Length of Insertion Site Present | Score |
| No insertion site evidence on slide | 0 |
| Approximately <25% length of tissue on slide | 1 |
| Approximately 26–50% length of tissue on slide | 2 |
| Approximately 51–75% length of tissue on slide | 3 |
| Approximately >76% length of tissue on slide | 4 |
| Quality/Consistency of Glycosaminoglycan (GAG) Staining of Cartilage/Fibrocartilage | Score |
| Absence of GAG staining (no red color with Safranin-O) | 0 |
| Minimal GAG staining (decreased staining intensity) | 1 |
| Mild level of GAG staining (slightly decreased staining intensity) | 2 |
| Typical level of GAG staining +/− minimal staining of fibrous bundles associated with fibrocartilage | 3 |
| Excessive widespread GAG staining | 4 |
| Body Weight Scoring Stall Side | Score |
| Emaciated | 1 |
| Thin | 2 |
| Normal | 3 |
| Overweight | 4 |
| Severely overweight | 5 |
| Lameness Scoring Done Stall Side | Score |
| Normal | 0 |
| Marginal intermittent lameness | 1 |
| Consistent mild lameness | 2 |
| Consistent moderate lameness | 3 |
| Consistent moderate lameness where the leg is used intermittently | 4 |
| Non weight bearing | 5 |
| Pain Scoring Is Done Stall Side | Score |
| Normal | 0 |
| Separation from group, quiet-alert-responsive, slightly increased respiratory rate | 1 |
| Separation from group, quiet-alert-responsive, slow to rise, reduced appetite, reduced rumen motility, increased respiratory rate | 2 |
| Separation from group, reluctant to rise when approached, no appetite, dull, teeth | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chevrier, A.; Hurtig, M.B.; Lavertu, M. Chitosan–Platelet-Rich Plasma Implants Improve Rotator Cuff Repair in a Large Animal Model: Pivotal Study. Pharmaceutics 2021, 13, 1955. https://doi.org/10.3390/pharmaceutics13111955
Chevrier A, Hurtig MB, Lavertu M. Chitosan–Platelet-Rich Plasma Implants Improve Rotator Cuff Repair in a Large Animal Model: Pivotal Study. Pharmaceutics. 2021; 13(11):1955. https://doi.org/10.3390/pharmaceutics13111955
Chicago/Turabian StyleChevrier, Anik, Mark B. Hurtig, and Marc Lavertu. 2021. "Chitosan–Platelet-Rich Plasma Implants Improve Rotator Cuff Repair in a Large Animal Model: Pivotal Study" Pharmaceutics 13, no. 11: 1955. https://doi.org/10.3390/pharmaceutics13111955
APA StyleChevrier, A., Hurtig, M. B., & Lavertu, M. (2021). Chitosan–Platelet-Rich Plasma Implants Improve Rotator Cuff Repair in a Large Animal Model: Pivotal Study. Pharmaceutics, 13(11), 1955. https://doi.org/10.3390/pharmaceutics13111955