1. Introduction
Providing effective pain management is a clinical imperative for every patient undergoing surgery. Infiltration of local anesthetics (LAs) into the surgery site is one aspect of the multimodal approach to pre- and postsurgical analgesia. However, the duration of action of LA is limited, lasting only a few hours, and patients may experience breakthrough pain before they are able to take or tolerate oral analgesics, necessitating the use of strong parenteral analgesics (frequently opioids) in the immediate postsurgical period.
Another limitation of the clinical application of LAs is their systemic toxicity, including cardiac and neurological toxicity. The occurrence of life-threatening adverse events related to local anesthetic systemic toxicity has been increasing in recent years [
1], highlighting the critical need for long-acting local anesthetics that extend the anesthetic effect while limiting the dose administered to patients, and thus risks associated with their use as well as the need for additional opioids. The cardiotoxic and neurotoxic effects of LAs have been known for some time [
2,
3] and are dose dependent, but the severity of the phenomenon is different for each LA. The more potent local anesthetics (such as etidocaine and bupivacaine) are for example more cardiotoxic than lidocaine. Liposomal formulations can protect from such negative secondary effects. For instance, encapsulating doxorubicin in PEGylated liposomes significantly reduced the risks of cardiotoxicity associated with the use of free doxorubicin [
4,
5]. We previously described a formulation of large multivesicular liposomes for the local slow release of bupivacaine [
6,
7]. Encapsulating bupivacaine into large multivesicular vesicles with a very large trapped aqueous volume, combined with the transmembrane ammonium ion gradient-driven bupivacaine loading, offers several benefits over the free drug. These advantages include higher drug-to-lipid ratio [
8,
9], a significantly slower release rate [
7], producing a much longer duration of anesthesia [
9,
10] and lower plasmatic C
max [
6], resulting in lower systemic toxicity. However, the neurological toxicity of this formulation has not been previously addressed.
The local neurotoxic effects of different LAs have been evaluated in in vitro studies [
11,
12] and it was shown that all local anesthetics are neurotoxic in a dose-dependent (or concentration-dependent) manner [
13] and that clinical levels of the drugs are enough to cause nerve injury [
14]. In addition, the duration of exposure to LA also increases the extent of nerve damage [
11,
13], and the neurotoxicity of LA can be caused by the active drug itself or its additive. Epinephrin is often used together with LA to increase nerve block duration via its vasoconstrictive effect, but the vasoconstriction and resulting decrease in blood flow contribute to prolonging the contact of the nerve with concentrated LA, which may induce damage to the nerve and surrounding tissue [
15,
16]. In addition, the risk of mechanical damage to the nerve with a needle further increases the risk of neurotoxicity; intrafascicular injection of LA can expose nerves to high concentrations of local anesthetics and increase the associated neurotoxic effects [
17].
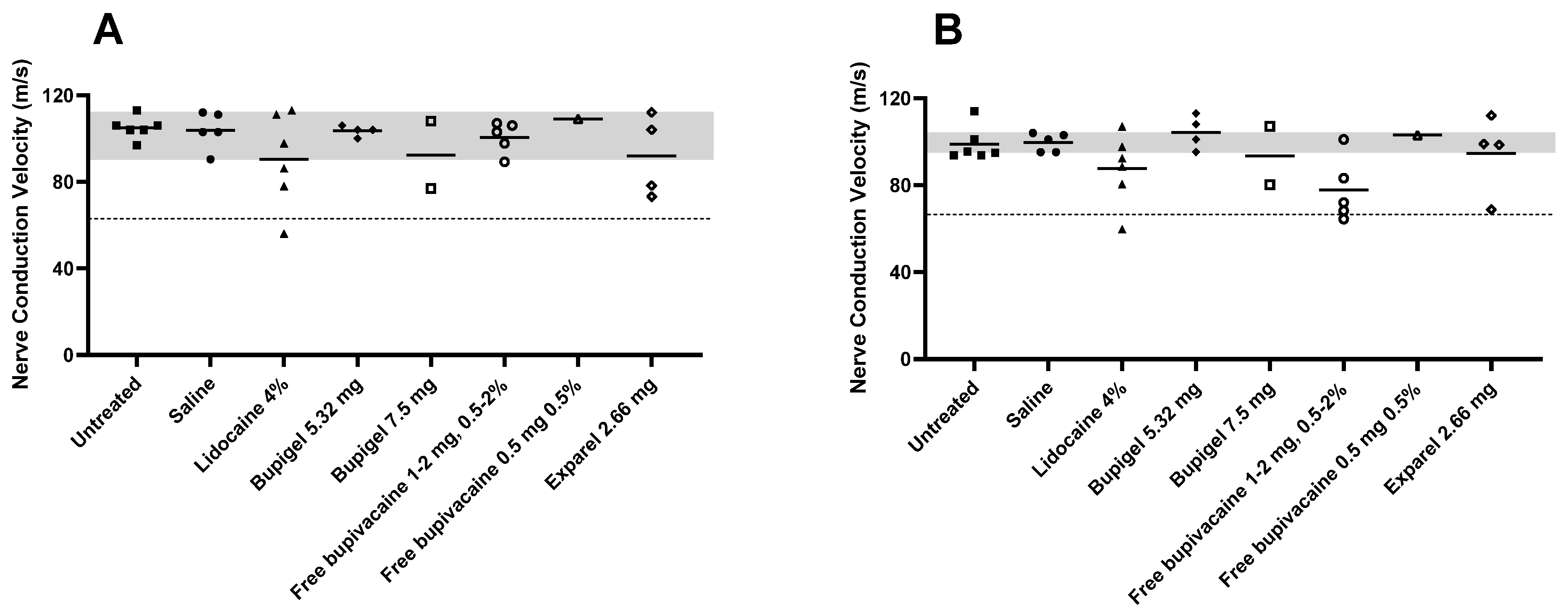
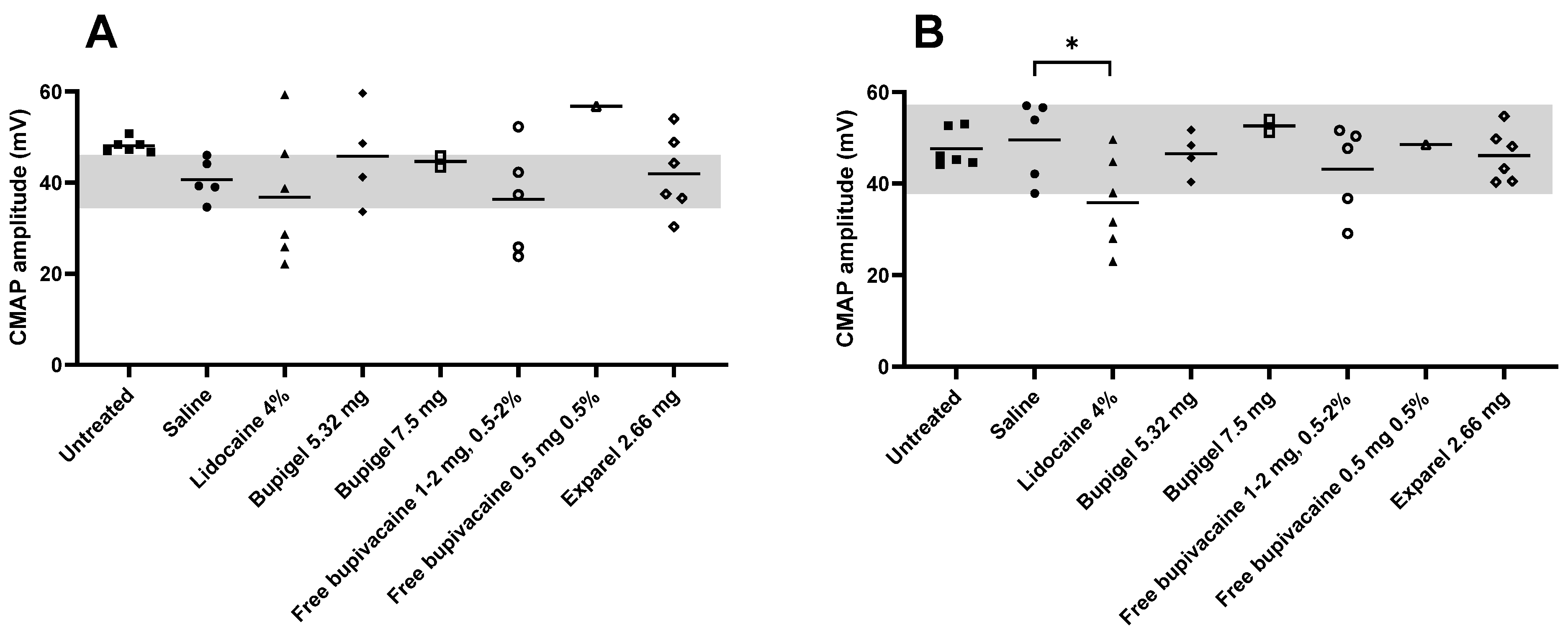
The objective of this study was to assess neurotoxicity resulting from a long residence time of a local anesthetic in proximity to the sciatic nerve in rabbits. To achieve this goal, we performed a functional neurological test on the sciatic nerve of rabbits following administration of different formulations in this area. Measurements included quantification of nerve conduction velocity (NCV), compound muscle action potentials (CMAPs) amplitude and area, and detection of sural sensory nerve action potentials (SNAPs).
2. Materials and Methods
2.1. Materials
For the preparation of the liposomal bupivacaine formulation (Bupigel), HSPC (hydrogenated soybean phosphatidylcholine) and cholesterol were purchased from Lipoid GmbH (Ludwigshafen, Germany). The HSPC used in this study is a mixture of two phosphatidylcholines (PCs) containing mostly distearoyl PC (DSPC) mixed with smaller amounts of 1-palmitoyl-2-stearoyl phosphatidylcholine (PSPC). The small batch-to-batch variations in the PSPC/DSPC mole % ratio range from 28/72 to 34/66 and the phase transition temperature (Tm) varied accordingly from 53.04 to 51.07 °C (see Supplementary Table S2 of [
18]). The drug product bupivacaine HCl was purchased from MOEHS (Barcelona, Spain) as a powder. For the “free bupivacaine” formulations tested (see
Section 2.6. Perineurial Administration Procedure), bupivacaine HCl 5 mg/mL was purchased from Kamada Ltd., Israel and diluted at the desired concentration in ultrapure water. Exparel
® (liposomal bupivacaine) was purchased from Pacira Pharmaceuticals (Parsipanny, NJ, USA) and lidocaine HCl (Xylocaine, App Pharmaceuticals, Schaumburg, IL, USA) was purchased as powder and dissolved in ultrapure water at 40 mg/mL (4%). Sterile saline for injection was purchased from Teva (Jerusalem, Israel).
2.2. Preparation of Bupigel
Multilamellar vesicles (MLVs) were prepared as described previously [
7]. Briefly, cholesterol and HSPC were dissolved in ethanol at a weight ratio of 4:6. The lipids were then hydrated by adding this ethanolic lipid solution to 250 mM ammonium sulfate. Following incubation for 1 h at 65 °C, the MLVs were submitted to 10 freeze–thaw cycles (2 and 5 min, respectively, in liquid nitrogen and hot water) to increase the trapped aqueous volume of the liposomes. This procedure creates large multivesicular vesicles (LMVVs) [
7,
9]. A transmembrane ammonium gradient, the driving force for the active remote loading of bupivacaine into LMVVs, was created by replacing the external ammonium sulfate aqueous phase by 0.9% NaCl (saline) with 10 consecutive cycles of centrifugations and suspension of the precipitate with sterile saline. This step also allowed the complete removal of the ethanol that was in the external medium (as was confirmed by osmolality measurements of the external medium that gave results similar to saline osmolality, i.e., 287 ± 2 mOsm/kg). Osmolality was measured with a Model 1332 osmometer (Advanced Instruments, Norwood, MA, USA). Remote active loading of bupivacaine was performed by adding the LMVVs to 5.75% (weight) bupivacaine HCl solution to form Bupisomes. The free (non- encapsulated) drug was then removed from the external medium by centrifugation and replacement of the upper phase by sterile saline. The Bupisomes were then mixed at 1:1 volume ratio with alginate 1% and dropped into a solution of calcium chloride 1.54% to form Bupigel [
7].
Identical Bupisomes were embedded in other hydrogel-forming agents in addition to alginate 1% to compare their respective bupivacaine release profile (in vitro studies only): Polyvinylpyrrolidone 20% (Kollidon® 25), Poloxamer (Pluronic® F-68), hyaluronic acid 0.5% and alginate 0.3% mixed with CaCl2 in stoichiometric ratio.
2.3. Characterization of the Bupisomes and Bupigel
The phospholipid content of Bupisomes was measured by a modified Bartlett procedure as described earlier [
19,
20]. The bupivacaine content of the formulation (free and encapsulated) was quantified using a Hewlett-Packard series 1100 high-performance liquid chromatography (HPLC) with UV detection. The samples were injected into a 150 × 4.6 mm column (Luna, Phenomenex OOF-4252-EO). A mobile phase of acetonitrile:phosphate buffer 25 mM pH 6.8 (70:30) was used, and absorption was measured at a wavelength of 200 nm. The retention time of the bupivacaine was approximately 5.5 min. The lipid content and encapsulated bupivacaine concentration were used to calculate the drug to lipid ratio. The Bupisomes size was determined using a laser diffraction particle size analyzer (Beckman Coulter LS 13 320). The trapped LMVV aqueous volume of 17.4 mL/mmole HSPC was determined from the intraliposome ammonium concentration [
21]. A more detailed physicochemical characterization of Bupigel is described in Table 3 of [
7].
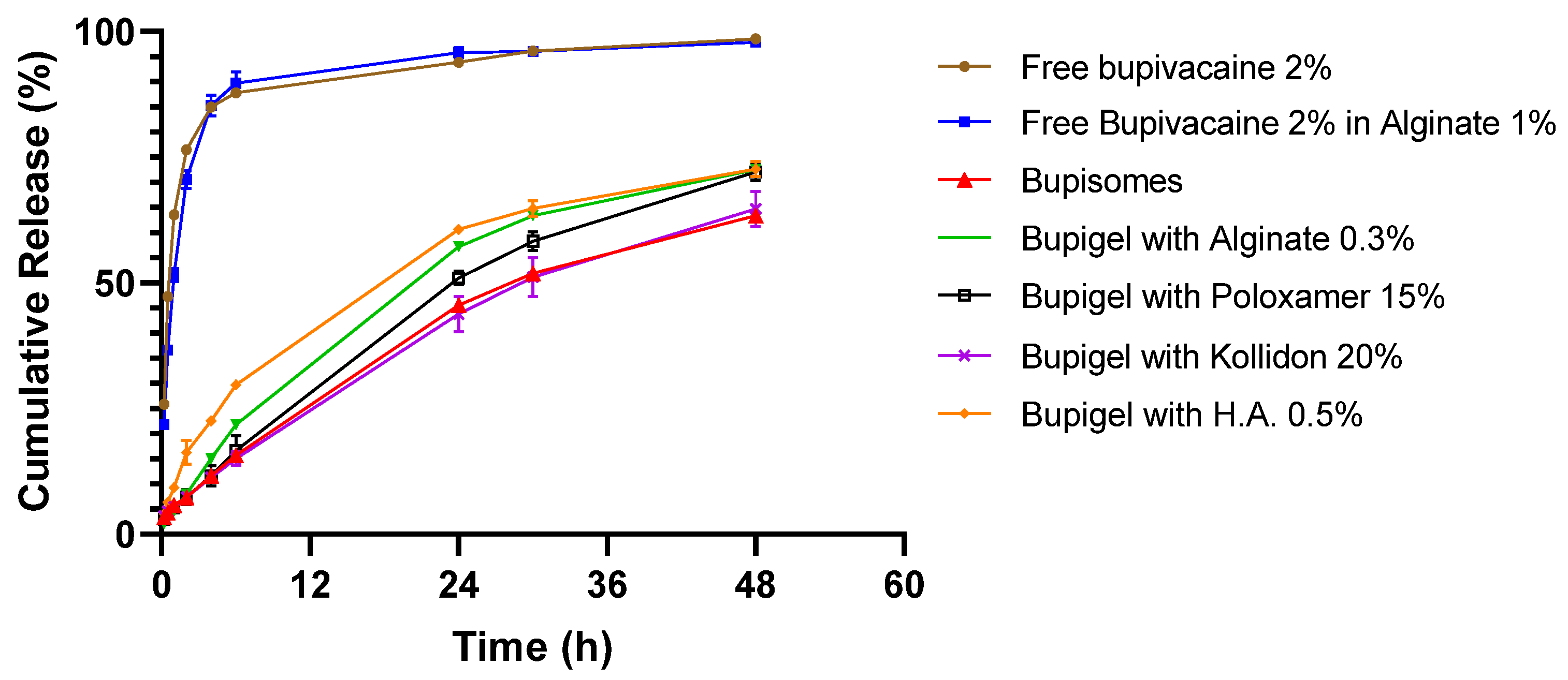
2.4. “Dissolution” Test for Bupivacaine Release from Bupigel
Bupivacaine release from Bupigel was measured using a standard Apparatus type 2 pharmaceutical dissolution tester Vision G2 Classic 6 (Hanson, Chatsworth, CA, USA) in a dissolution-like approach. The apparatus was equipped with an in-house-designed enhancer cell containing 0.5 g of the sample with a 0.2 µm membrane that allowed only for the low molecular weight molecules to cross without any barrier to the upper compartment containing the desired dissolution buffer (in our case, filtered saline 0.9%). This modified instrument allows close simulation of subcutaneous depot injection. The release tests were performed over 48 h at 37 °C. The concentration of the released drug was quantified in samples (0.5 g) collected from the upper compartment in duplicates at different time points using the same HPLC protocol as described in the section “Characterization of the Bupisomes and Bupigel” above.
2.5. Animals
Twenty-three male New Zealand White (NZW) rabbits (strain HsdOkd:NZW, Envigo, Denver, PA, USA) weighing 2.8–3.8 kg at the beginning of the study were allowed to acclimate in the animal facility for at least one week before the study. The rabbits were housed by pairs in 12/12 h light/dark period and allowed free access to water and standard chow (Teklad global rabbit diet) with supplement of fresh hay every 3 days. All in vivo experiments were approved by the Animal Ethical Care Committee of the Hebrew University of Jerusalem, Israel (ethics approval MD-12-13079-3).
2.6. Perineurial Administration Procedure
On the day of the nerve block, each rabbit was weighed and anesthetized with an intramuscular (IM) injection of ketamine/xylazine (150/15 mg/kg). They were then maintained under anesthesia by inhalation of isoflurane 2–4% (according to need) until the end of the procedure and kept warm with an electric heating pad. The skin of the rabbit was shaved from the buttock to the knee on both legs. The rabbits were administered antibiotics (cefamezin 30 mg/kg, intramuscular) before surgery (prophylactic) and the 2 following days. They were also injected with a systemic painkiller (carprofen 7.5 mg/kg, subcutaneous, SC) before the beginning of the procedure and for 3 additional days. All IM and SC injections were performed as far as possible from the sciatic nerve in order not to interfere with the experimental measurements.
For perineurial administration, muscles along the planes of fascia between the hamstring muscles were carefully separated in order to expose the sciatic nerve. Each tested formulation (detailed below) was then administered dropwise directly onto the exposed sciatic nerve (in mid-thigh), then the fascia and skin were closed with absorbable suture (Vicryl 3/0). After the procedure rabbits were monitored until they fully awoke and recovered from the surgery.
The formulations were tested as follows (n being the number of legs injected): saline (200 or 400 µL, n = 5) was used as a negative control, while lidocaine 4% (4 mg in 100 µL, n = 6) was used as a positive control for nerve damage. Bupigel was tested at 2 doses (5.32 mg and 7.5 mg in 250–400 µL according to the concentration of the formulation, n = 4 and n = 2, respectively) and compared to free bupivacaine (0.5 to 2 mg, 0.5–2% in a volume of 50–200 µL, n = 6, one leg per dose/concentration tested) and to Exparel® (2.66 mg in 200 µL, n = 4). In addition, nerve conduction studies (NCSs) were conducted on naïve rabbits (n = 6 legs tested) before perineurial administration, in order to compare values of non-injected nerves to saline administration.
2.7. Clinical Follow-up of the Animals
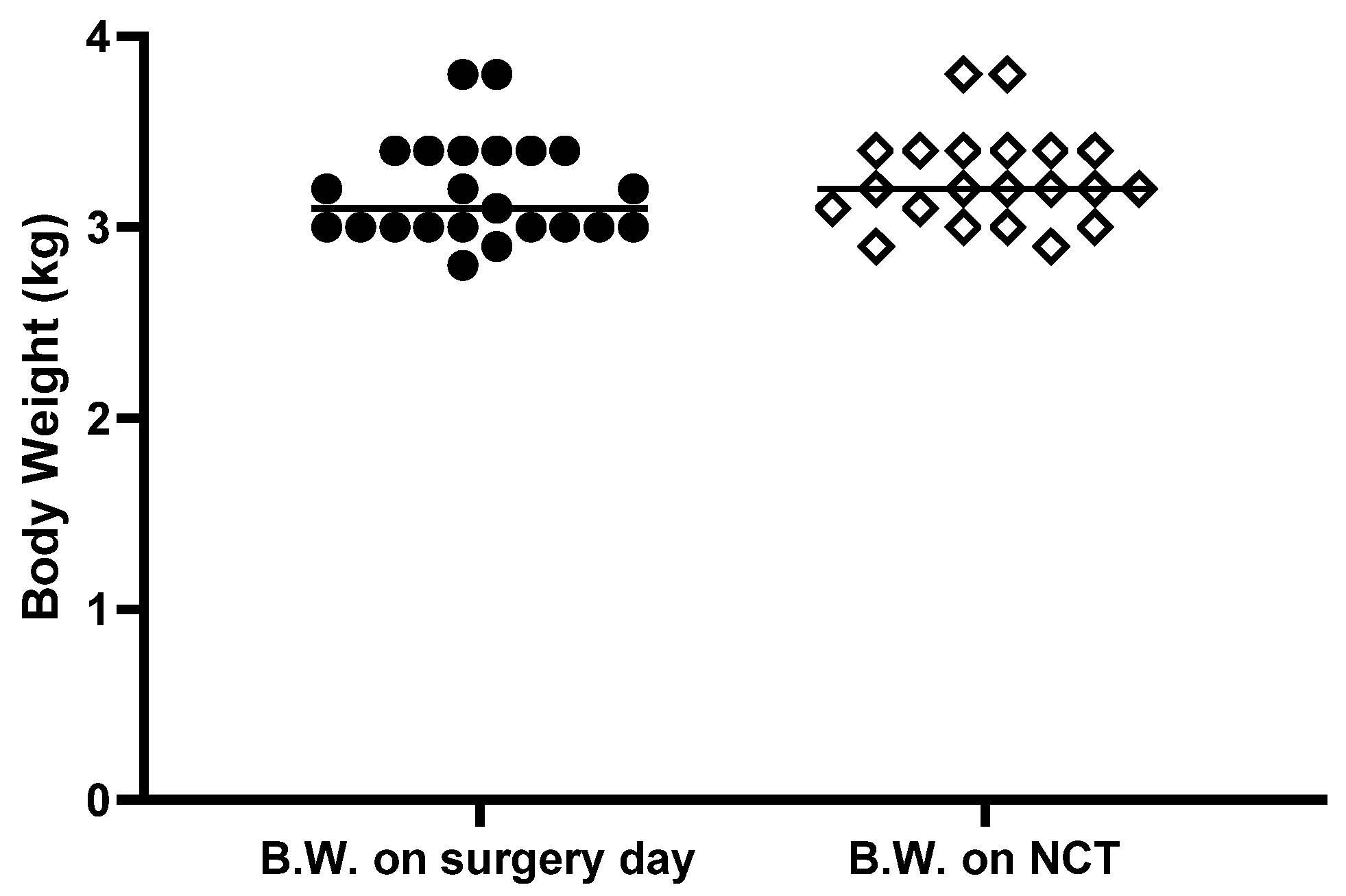
The animals underwent clinical inspection prior to and throughout the study. The rabbits were weighed on the day of perineurial administration and following the surgery, for 3 consecutive days. The incision site was inspected for signs of infection, opening of the sutures or signs of pain. Until the completion of the study, side cage observation was performed daily, but rabbits were weighed only before perineurial administration and NCS in order to decrease stress caused to the animals and especially to minimize risk of hematoma due to leg trauma.
2.8. Nerve Conduction Study (NCS)
Two weeks after perineurial drug administration, the rabbits underwent NCSs. For this test, each rabbit was anesthetized with an intramuscular injection of ketamine/xylazine (150/15 mg/kg) in the paraspinous muscle, along the vertebral column (not in the legs in order to avoid the sciatic nerve) and injected with carprofen 5 mg/kg before the beginning of the procedure.
Sciatic-tibial and sciatic-peroneal motor NCSs were tested in both hind limbs, adapted from previously described methods [
22,
23,
24,
25,
26]. A Dantec Keypoint
® Net version 2.11, Natus Medical Incorporated, Skovlunde, Denmark, EMG (electromyography) system was used set at sensitivity 2 mv/div., sweep speed 1 ms/div., HFF 5 KHz, and LFF 10Hz for nerve stimulation and data acquisition. The anesthetized rabbit was placed on a heating pad in a temperature-controlled room in the lateral decubitus position. Rectal temperature was recorded with a thermistor probe and maintained between 38–40 °C (normal values). Thigh skin temperature was monitored using an infrared thermometer (Extech instruments). Fur was shaved on the skin surface and recording 10 mm gold-plated EEG cup electrodes were affixed to the skin in a belly-tendon montage using Ten20 Paste as conductive adhesive and strapped with adhesive tape. A pick-up (G1) cup electrode was placed over the
gastrocnemius muscle mid-belly for the sciatic-tibial nerve. For sciatic-peroneal nerve, G1 was placed over the
tibialis anterior muscle at a point along a line 40 percent of the distance measured from
patella mid-point to lateral ankle. A reference electrode (G2) was placed over the anterior ankle midway between the medial and lateral
malleolus (peroneal) and
Calcaneus tendon (tibial). Stimulation was by subdermal disposable sensory needle electrodes (SNEs) (Natus
® Alpine bioMed, 28G, 15mm × 0.35 mm) with stimulating cathode (negative pole) and anode 1.5 cm apart. Distal stimulation ≥2.5 cm below the injection site was performed for peroneal nerve at the fibular head level through the upper fibers of the lateral head of
gastrocnemius muscle, and tibial nerve in the posterior thigh just above the popliteal crease in the midline. Proximal stimulation was at sciatic notch level (≥2.5 cm above injection site). A disposable monopolar needle (Medtronic
®, 26G 37 mm × 0.4 mm) was placed subcutaneously between stimulator cathode and active pick-up (G1) electrode for grounding. Maximal CMAP amplitudes were obtained both proximally and distally by stepwise increment in stimulation intensity, and without artefacts (currents: 15–80 mA, duration: 0.1–0.2 ms). Supramaximal CMAP amplitude was acquired by further increase in stimulation intensity, without further increase in CMAP size. Measurements obtained were: peak-to-peak CMAP amplitudes (supramaximal), compound muscle action potential area under the negative peak, CMAP duration from onset of the initial negative peak to return to baseline of the final negative peak, and compound muscle action potential latencies measured from stimulus artefact to initial onset of the wave, both proximally and distally. Nerve conduction velocity (NCV) was calculated by dividing the distance by the difference between proximal and distal latencies. Distances were measured by a vinyl inelastic tape measure (Dantec™, Natus
® Neurology) along the path of the sciatic-tibial and sciatic-peroneal nerves, between the cathodes of sciatic-notch and distal stimulation sites.
Sural sensory studies were tested from the foot by a method adapted from [
23]. The rabbit was placed in the lateral decubitus position with test-side up and fur shaved to skin from distal posterior leg to lateral foot. Stimulation was performed using SNEs as described above placed ~3 cm proximal to the lateral
malleolus in a groove anterior to
Calcaneus tendon, cathode-anode 1.5 cm apart. Active pick-up (G1) was from a subdermal SNE inserted in the lateral edge of the foot, 0.5 cm distal to a line perpendicular to lateral edge of foot connecting with lateral
malleolus above. Reference (G2) SNE was placed 4 cm distal to G1 along the lateral edge of the foot. A ground (monopolar needle electrode) was inserted subcutaneously in the lateral heel. A train of 20–40 SNAPs were averaged, and best of 2 trials taken with filters same as for motor, sweep 2 ms/division and sensitivity 10–20 μV/division. Sural SNAP (sensory nerve action potential) peak latency and amplitude were measured.
Needle EMG studies were conducted using the above Dantec Keypoint® EMG system with sensitivity 0.1 mv/div., sweep speed 20 ms/div., HFF 5 KHz, and LFF 10 Hz. A disposable concentric needle EMG electrode (0.30 × 25 mm, 30G; Dantec, Alpine Biomed ApS, Skovlunde, Denmark) was inserted into gastrocnemius and tibialis anterior muscles of both hind limbs to assess for active denervation: fibrillation potentials, positive sharp waves, and other abnormal spontaneous activity. Motor unit action potential analysis was limited due to anesthesia. At the end of the NCS/EMG test, rabbits were sacrificed and sciatic nerves collected and fixed in formalin 4% for histological studies.
2.9. Statistical Analysis
All values are expressed as the mean ± standard deviation (SD) unless otherwise stated. Mann–Whitney test was performed using IBM SPSS 25 to compare the saline and Bupigel (5.32 mg) groups, and p < 0.05 was the threshold set for statistical significance.
4. Discussion
Our study shows that neurotoxic effects of local anesthetics can be measured by NCS, a functional test performed two weeks after local injection. Electrodiagnostic testing (nerve conduction and needle EMG) allows for a non-invasive and detailed characterization of a neuropathy. It is highly sensitive for defining the pattern and degree of nerve involvement and can provide insight into the underlying pathophysiology, defining a neuropathy as either axonal or demyelinating, and gives an idea of the severity of the damage. However, because it is so sensitive, the results are affected by anything between the electrodes and the nerve, such as peripheral edema resulting from trauma [
29]. Rabbits are very sensitive to stress and therefore they tend to run and kick if they feel aggressed, for example in the presence of an aggressive cage mate, and any blow or bite to the region tested (from the thigh to the ankle) may cause edema that can disturb the NCS readings. For this reason, great care must be taken in the handling and housing of the rabbits. Contacts between the animals and caretaker should be maintained to a minimum, and male rabbits should be housed individually if they show signs of aggressiveness to avoid local trauma [
30]. In addition, drugs other than the tested formulations that require intramuscular injection (such as painkillers, antibiotics, or drugs used to induce anesthesia) should not be administered close to the tested area because any pressure caused by the volume of injection in the nearby muscles can modify nerve conduction. The effect on the NCS is obviously more important if the formulation is targeting the nerve. This was observed when the induction of anesthesia in rabbits was performed by an intramuscular injection of ketamine and xylazine in the femoral biceps without any other procedure. The injection of the local anesthetic in muscles close to the tested area caused very severe partial conduction block in both sciatic-tibial and sciatic-peroneal motor fibers, with motor NCV slowing and moderately severe secondary axonal damage (ongoing/active denervation). In addition, sural sensory studies were absent (data not shown). For this reason, the cocktail of anesthesia inducers was injected as far as possible from the sciatic nerve, in the dorsal area, for the rest of the study. In addition, a study [
31] showed that the use of ketamine and xylazine as anesthetic agents caused a decrease in motor NCV values in mice (while sensory NCV values remained unchanged) compared to animals anesthetized with isoflurane. In our study, the rabbits received a dose of ketamine and xylazine to induce the anesthesia while the procedure itself (perineurial administration and NCS) was performed under isoflurane anesthesia. Nevertheless, the NCV decrease observed in mice was reported to be consistent within experimental groups and across multiple experiments [
31], therefore it should not be of concern in this study. Another effect observed by the same group following ketamine and xylazine anesthesia in mice is a decrease in core and surface temperature (measured in hind limbs) compared to mice anesthetized with isoflurane. It is widely known that temperature affects diverse parameters of NCS [
32,
33,
34,
35], and for this reason the rabbits’ temperatures were maintained constant during the procedure with a heating pad. In addition, NCS requires the animals to be under general anesthesia, thus restricting needle EMG motor unit action potential analysis and volition/recruitment. However, performing the NCS on the sciatic nerve is an advantage because of the large perineurial space, allowing the administration of relatively large volumes of formulations without causing pressure on the nerve. For this reason, the lower tibial CMAP amplitude observed in saline-injected legs compared to naïve (untreated) is unlikely due to mechanical compression of the nerve by the volume of saline injected but rather could be caused by irritation caused by saline touching the nerve and triggering vasomotor responses. The effect of saline has been studied in epineurial injections [
36,
37] and has been shown to cause nerve damage. Despite the use of saline-injected legs as control, there has been no NCS comparison in naïve animals compared to perineurial injection of saline to the best of our knowledge.
The interval between the perineurial injection and the NCS (2 weeks) was chosen considering several parameters. The first parameter is the rate of drug release determined by dissolution kinetics (
Figure 1) and from plasma PK studies in humans [
6] where the long half-life of Bupisome injected SC was found to be 294 ± 860 min compared to 131 ± 58 min for free bupivacaine 0.5%. The second parameter is having the NCS 14 days after the perineurial injection, giving sufficient time to detect any electrophysiological evidence of nerve damage. The third point to take into consideration is that the NCS should be performed after the resorption of post-operative inflammation (one week after perineurial administration, the inflammation in the legs was still impairing NCS measurements, data not shown). The fourth and final parameter is the presence of local anesthetic near the sciatic nerve that will, by nature, slow nerve impulses and therefore affect the NCS. Thus, sufficient time should be given to allow for complete wash-out of the tested formulations. In adults, the terminal half-life of bupivacaine is 2.7 h [
38]. Therefore, 2 weeks (the interval between the administration of local anesthetic and the nerve conduction study), is sufficient for complete wash-out of all tested formulations, and the variations in the different parameters of NCS measured are due to nerve damage and not to the direct effect of the local anesthetic on the nerves.
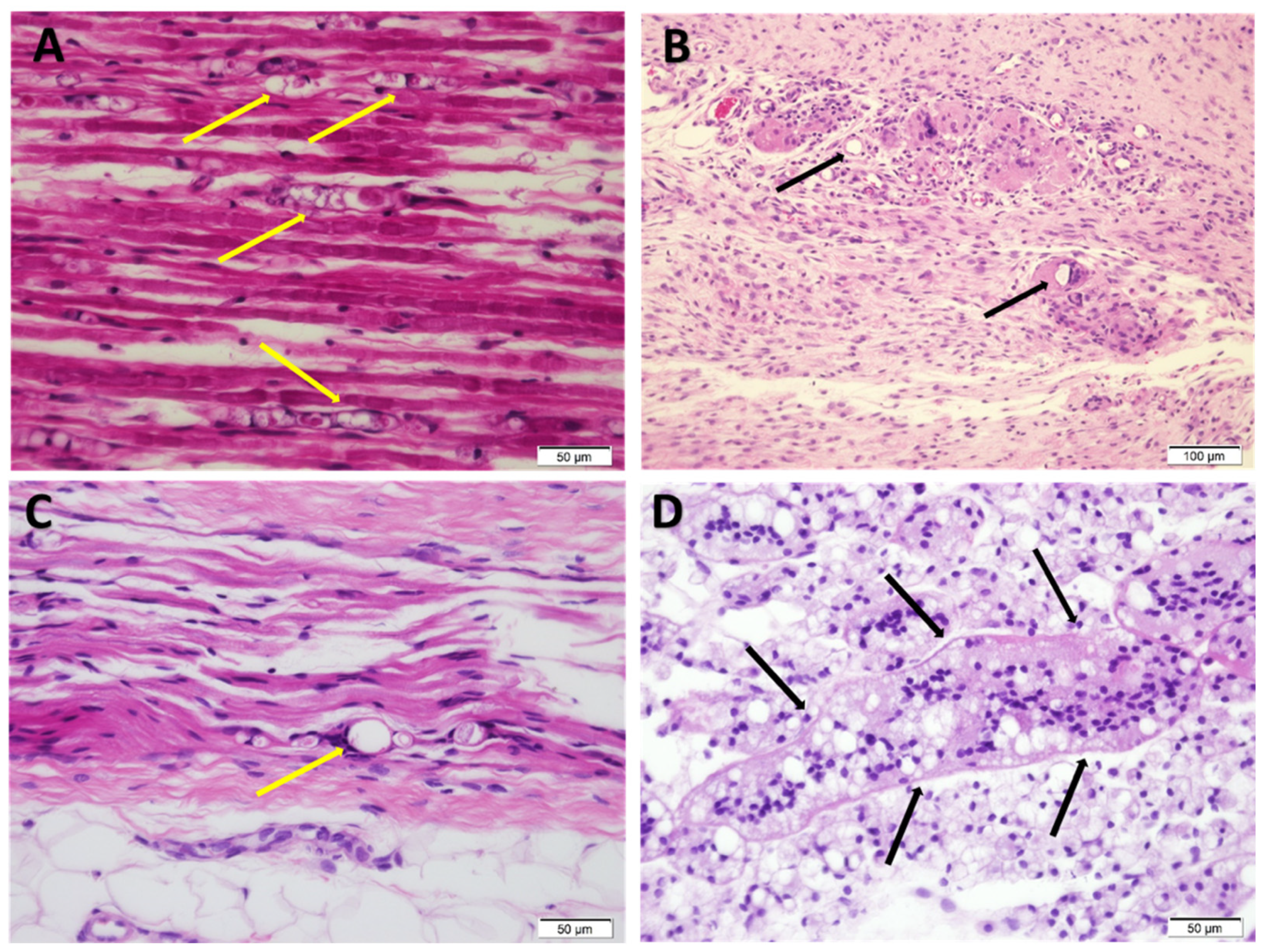
A study [
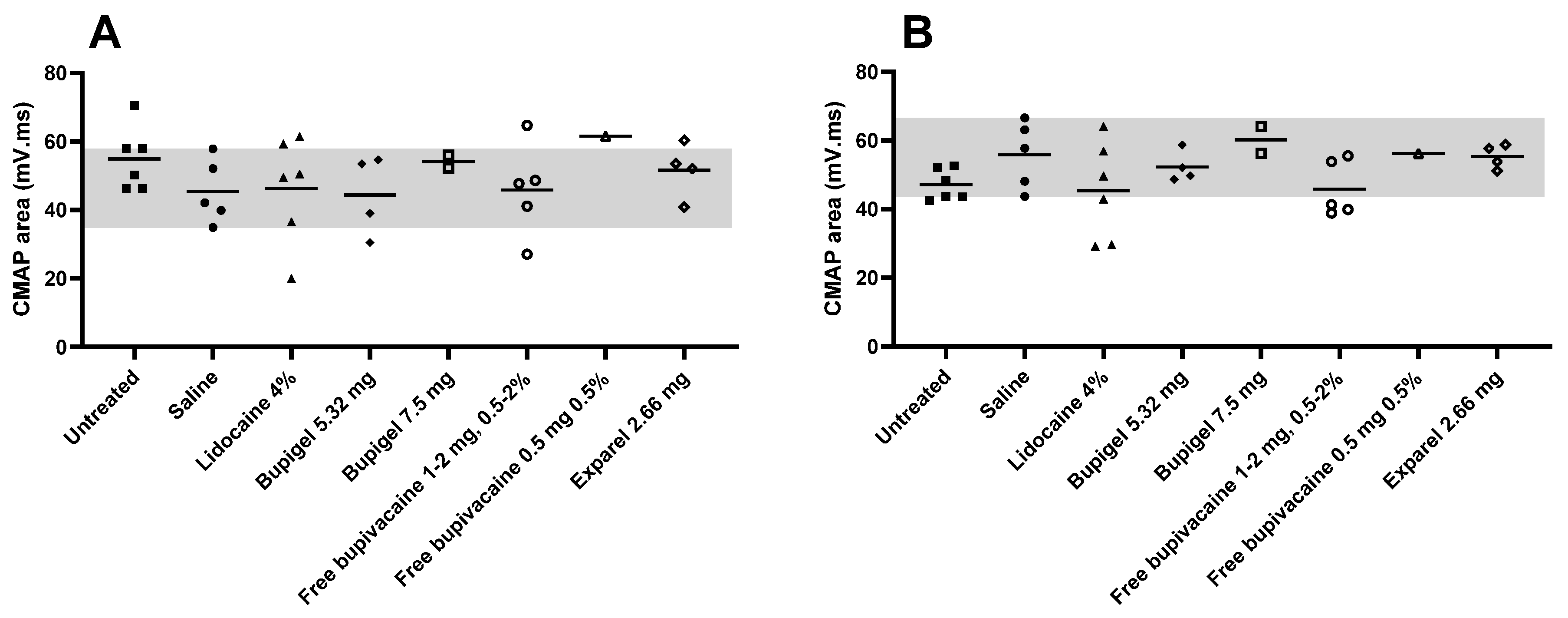
39] assessing the neurotoxicity of a liquid formulation of liposomal bupivacaine after perineural administration in pigs showed that even using electron microscopy, there was no detectable sign of neurotoxicity caused by the formulation. Signs of inflammatory response were detected, as expected after a surgical procedure. Similarly, in our study, microscopic examination did not reveal signs of nerve injury besides mild signs of inflammation that are most probably residues of post-operative inflammation. In addition, this effect was only observed in sciatic tibial CMAP amplitude but not in the peroneal fibers, nor in CMAP area or nerve velocity. Similarly, no effect of saline could be detected by active denervation on needle EMG, suggesting any possible axonal damage was only mild and limited to tibial fibers.
In our study the positive control for nerve damage (lidocaine 4 mg at 4%) proved to cause nerve damage in four rabbits out of five. The nerve damage in the rabbits affected was mostly mild motor demyelination and three rabbits out of four had axonal damage in the sensory fibers (absent sural sensory SNAP). One of the limbs injected with lidocaine had a mild partial conduction block, indicating the presence of mild focal motor myelin damage.
In order to find the smallest dose (and concentration) of free bupivacaine that would not cause neurotoxicity we tried several combinations: 2 mg at 2% or 1%, 1 mg at 2%, 1% and 0.5%, and finally 0.5 mg at 0.5%. Among all these combinations, only the smallest dose (0.5 mg at 0.5%) did not cause damage to the nerve. The limbs injected with doses of free bupivacaine between 1–2 mg (concentration ranging from 0.5% to 2%) showed varying degrees of nerve damage, from mild non-specific NCV slowing in axonal range (less than 30% below LLN, 64.4 to 72 m/s), to mild demyelinative damage shown by 30–40% slowing below LLN and mild partial conduction block. In addition, there was sensory fiber damage in all cases (5/5), but no motor axonal damage with this preparation.
The limbs injected with a dose of free bupivacaine as small as 1 mg showed signs of neurotoxicity with mild motor myelin damage and absent sensory potentials. However, we demonstrated in this study than none of the limbs injected with a dose more than 5-times higher of liposomal bupivacaine showed any signs of nerve damage. The limbs injected with 5.32 mg of bupivacaine encapsulated in Bupigel had NCV values that were within the normal range and distal CMAP amplitudes very similar to the limbs injected with saline. There were no signs of motor axonal or sensory fiber damage in the Bupigel-injected limbs at this dose. Increasing the liposomal bupivacaine dose to 7.5 mg resulted in mild motor myelin damage and absent sural SNAPs. This dose is apparently above the toxic threshold for our liposomal formulation. Interestingly, Exparel® administration caused signs of motor myelin and sensory fibers damage at half of the Bupigel dose that was found innocuous. The high standard deviation related to the low number of animals in each group and high variations between individuals did not allow us to draw definitive conclusions regarding the effect of the formulations compared to saline (except in one parameter). Nevertheless, there was an obvious trend showing a toxic effect in several nerves, including clear signs of demyelinative damage in lidocaine-injected legs, showing the relevance of such a test for the detection of neurotoxicity.
One of the major limitations of LAs is their short duration of action. The duration of anesthesia is in part influenced by the residence time of the LA in close proximity to the neural fibers, and for this reason vasopressors are added to many LA formulations. Their effect, constricting neighboring vasculature, delays the absorption of the LA to the systemic circulation and therefore extends the effect of the anesthesia [
40]. The use of our formulation, consisting of large multivesicular liposomes with high trapped aqueous volume which are embedded in hydrogel, overcomes the need for vasopressors in order to keep the LA at the action site. The viscosity of various hydrogel-forming polymers including hyaluronic acid or alginate hydrogels, ensures good injectability and is high enough to mechanically keep the formulation at the injection site where the bupivacaine is slowly released [
7]. We previously showed that the slow release offered by liposomal formulation protects from the cardiotoxic effect of free bupivacaine [
6]. In this study we demonstrated in addition that Bupigel formulation is innocuous at the tested dose with regard to local toxicity to the sciatic nerve, as shown by the nerve conduction study performed that allowed us to administer a dose more than 5-times higher than the non-liposomal bupivacaine without any sign of local nerve damage. In addition, performing a functional test for the detection of neurotoxicity allowed us to detect neural damage that could not always be observed by traditional histological observations.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}