
Ginsenoside Absorption Rate and Extent Enhancement of Black Ginseng (CJ EnerG) over Red Ginseng in Healthy Adults

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Study Participants
2.3. Study Design
2.4. Bioanalytical Methods
2.5. Pharmacokinetics
2.6. Safety and Tolerability Assessment
2.7. Statistical Analysis
3. Results
3.1. Subjects
3.2. Validation of the Bioanalytical Method
3.3. Pharmacokinetics
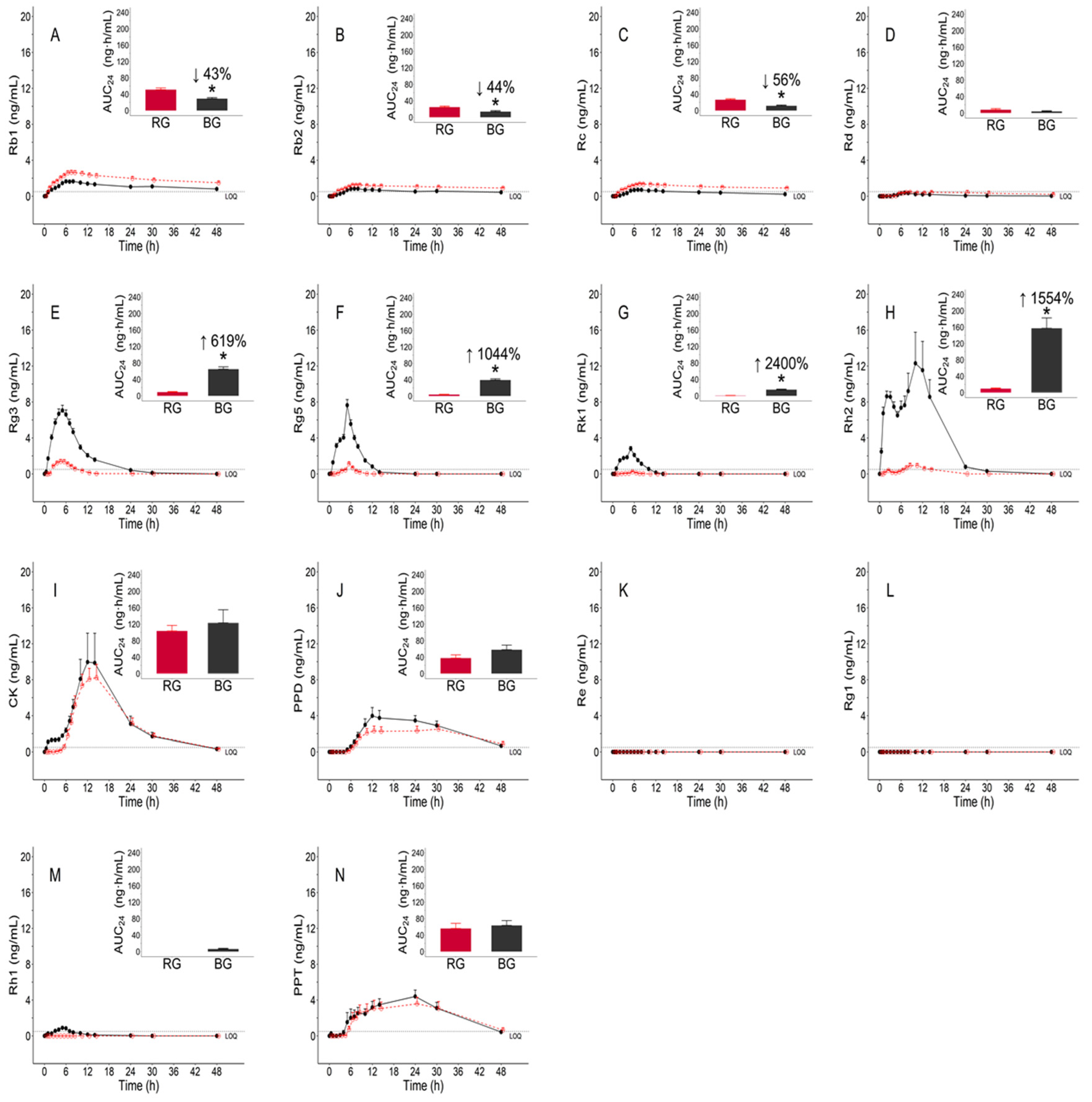
3.3.1. Pharmacokinetic Parameters of Individual Ginsenosides
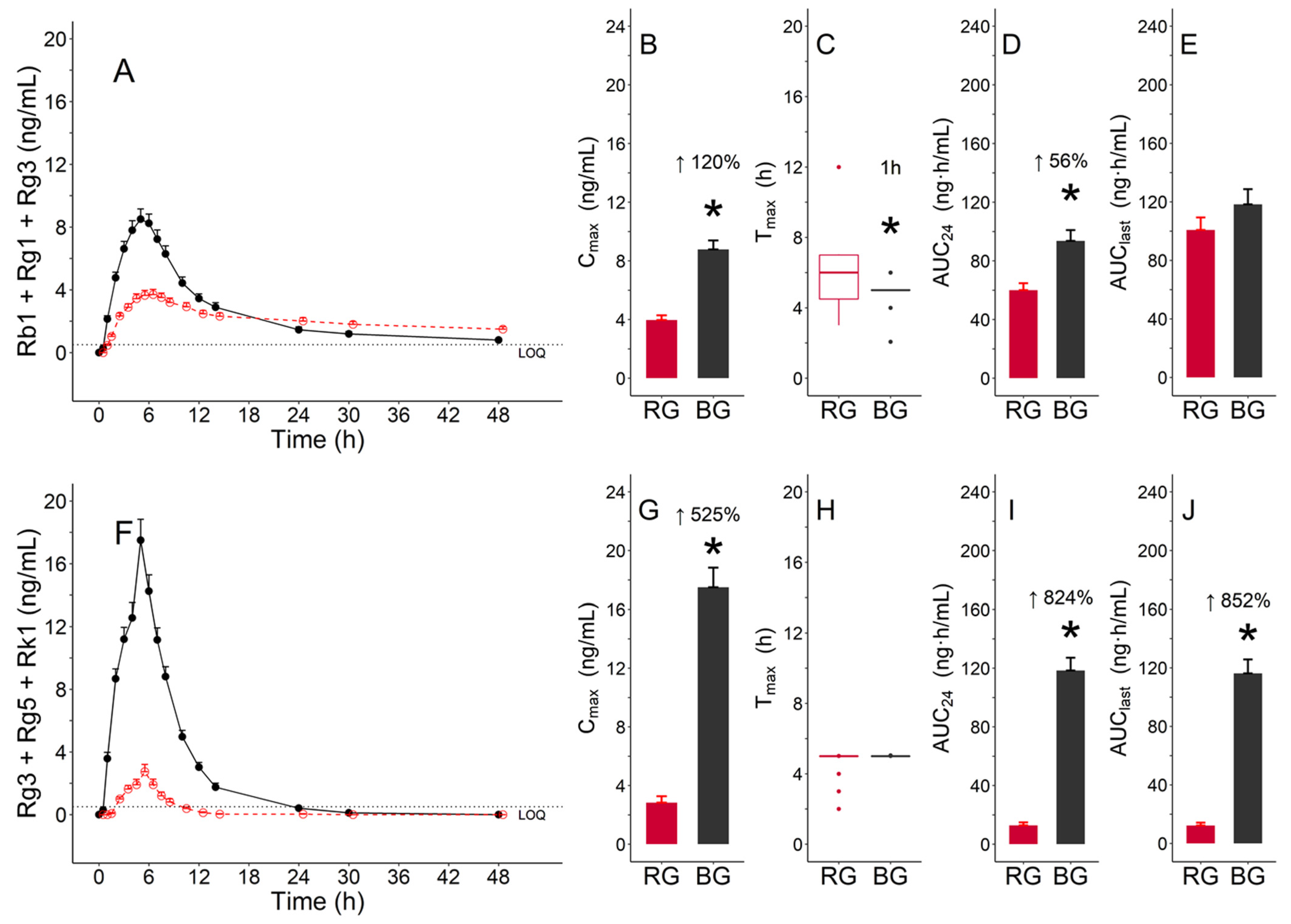
3.3.2. Pharmacokinetic Parameters of Functional Ginsenosides Group
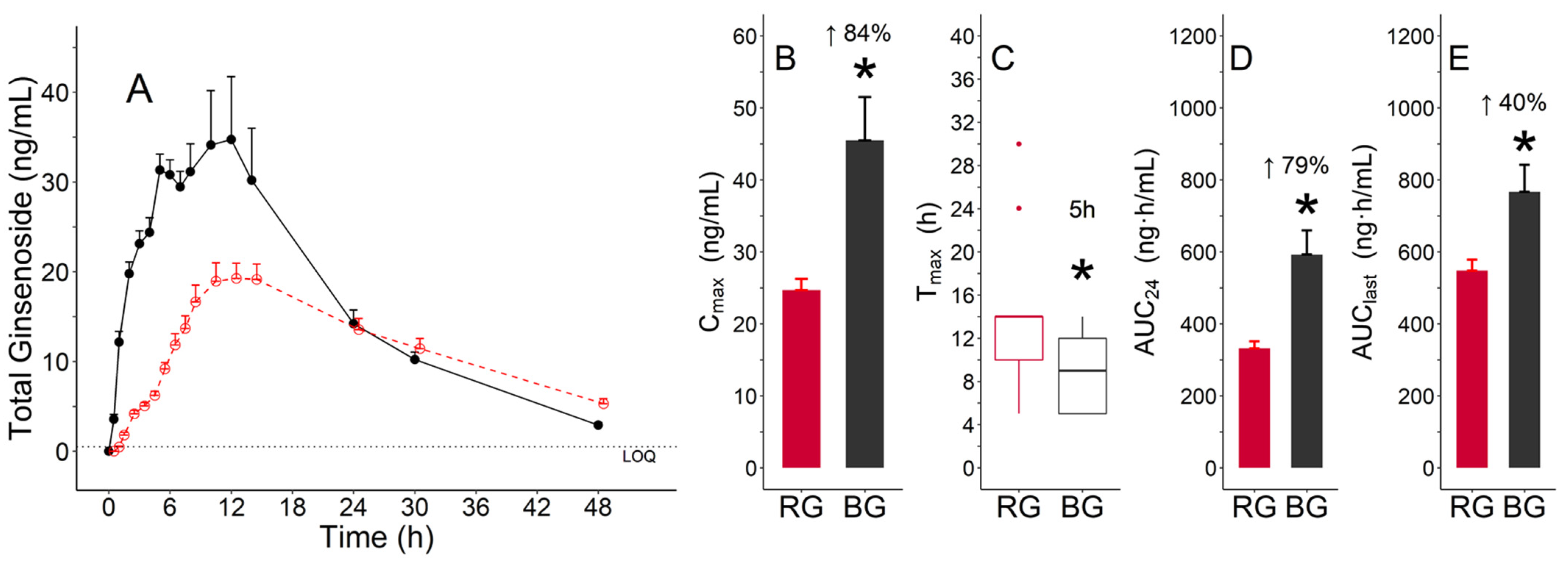
3.3.3. Pharmacokinetic Parameters of Total Ginsenosides
3.4. Safety and Tolerability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Christensen, L.P. Ginsenosides: Chemistry, biosynthesis, analysis, and potential health effects. Adv. Food Nutr. Res. 2008, 55, 1–99. [Google Scholar]
- Kang, K.S.; Kim, H.Y.; Yamabe, N.; Nagai, R.; Yokozawa, T. Protective effect of sun ginseng against diabetic renal damage. Biol. Pharm. Bull. 2006, 29, 1678–1684. [Google Scholar] [CrossRef] [Green Version]
- Qi, L.-W.; Wang, C.-Z.; Yuan, C.-S. American ginseng: Potential structure–function relationship in cancer chemoprevention. Biochem. Pharmacol. 2010, 80, 947–954. [Google Scholar] [CrossRef]
- Yun, T.-K. Panax ginseng—A non-organ-specific cancer preventive? Lancet Oncol. 2001, 2, 49–55. [Google Scholar] [CrossRef]
- Kim, D.-W.; Kim, Y.-J.; Lee, Y.-J.; Min, J.-W.; Kim, S.-Y.; Yang, D.-C. Conversion of ginsenosides by 9 repetitive steamings and dryings process of Korean ginseng root and its inhibition of BACE-1 activity. J. Physiol. Pathol. Korean Med. 2008, 22, 1557–1561. [Google Scholar]
- Chen, W.; Guo, Y.; Yang, W.; Zheng, P.; Zeng, J.; Tong, W. Protective effect of ginsenoside Rb1 on integrity of blood–brain barrier following cerebral ischemia. Exp. Brain Res. 2015, 233, 2823–2831. [Google Scholar] [CrossRef]
- Gao, X.-Q.; Yang, C.-X.; Chen, G.-J.; Wang, G.-Y.; Chen, B.; Tan, S.-K.; Liu, J.; Yuan, Q.-L. Ginsenoside Rb1 regulates the expressions of brain-derived neurotrophic factor and caspase-3 and induces neurogenesis in rats with experimental cerebral ischemia. J. Ethnopharmacol. 2010, 132, 393–399. [Google Scholar] [CrossRef]
- Salim, K.N.; McEwen, B.S.; Chao, H.M. Ginsenoside Rb1 regulates ChAT, NGF and trkA mRNA expression in the rat brain. Mol. Brain Res. 1997, 47, 177–182. [Google Scholar] [CrossRef]
- Wu, Y.; Xia, Z.-Y.; Dou, J.; Zhang, L.; Xu, J.-J.; Zhao, B.; Lei, S.; Liu, H.-M. Protective effect of ginsenoside Rb1 against myocardial ischemia/reperfusion injury in streptozotocin-induced diabetic rats. Mol. Biol. Rep. 2011, 38, 4327–4335. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Qu, Z.; Liu, Y.; Deng, H. Preliminary study on antiamnestic mechanism of ginsenoside Rg1 and Rb1. Chin. Med. J. 1990, 103, 932–938. [Google Scholar] [CrossRef]
- Zhang, Y.-J.; Zhang, X.-L.; Li, M.-H.; Iqbal, J.; Bourantas, C.V.; Li, J.-J.; Su, X.-Y.; Muramatsu, T.; Tian, N.-L.; Chen, S.-L. The Ginsenoside Rg1 Prevents Transverse Aortic Constriction–Induced Left Ventricular Hypertrophy and Cardiac Dysfunction by Inhibiting Fibrosis and Enhancing Angiogenesis. J. Cardiovasc. Pharmacol. 2013, 62, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Chai, H.; Lin, P.H.; Lumsden, A.B.; Yao, Q.; Chen, C. Ginsenoside Rb1 blocks homocysteine-induced endothelial dysfunction in porcine coronary arteries. J. Vasc. Surg. 2005, 41, 861–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Li, H.-Q.; Lu, L.; Fu, D.-L.; Liu, A.-J.; Li, J.-H.; Zheng, G.-Q. Ginsenoside Rg1 provides neuroprotection against blood brain barrier disruption and neurological injury in a rat model of cerebral ischemia/reperfusion through downregulation of aquaporin 4 expression. Phytomedicine 2014, 21, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.-H.; Kim, S.-W.; Park, S.-J.; Kim, S.; Yu, K.-M.; Kim, S.G.; Lee, S.H.; Seo, Y.-K.; Cho, N.-H.; Kang, K. Greater efficacy of black ginseng (CJ EnerG) over red ginseng against lethal influenza A virus infection. Nutrients 2019, 11, 1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.Y.; Saba, E.; Irfan, M.; Kim, M.; Yi-Le Chan, J.; Jeon, B.S.; Choi, S.K.; Rhee, M.H. The anti-inflammatory and anti-nociceptive effects of Korean black ginseng. Phytomedicine 2019, 54, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Ma, J.Y.; Sung, C.K. Chronic dietary ginseng extract administration ameliorates antioxidant and cholinergic systems in the brains of aged mice. J. Ginseng Res. 2017, 41, 615–619. [Google Scholar] [CrossRef]
- Jin, S.; Jeon, J.-H.; Lee, S.; Kang, W.Y.; Seong, S.J.; Yoon, Y.-R.; Choi, M.-K.; Song, I.-S. Detection of 13 ginsenosides (Rb1, Rb2, Rc, Rd, Re, Rf, Rg1, Rg3, Rh2, F1, Compound K, 20(S)-Protopanaxadiol, and 20(S)-Protopanaxatriol) in human plasma and application of the analytical method to human pharmacokinetic studies following two week-repeated administration of red ginseng extract. Molecules 2019, 24, 2618. [Google Scholar]
- Health Functional Food Code (No. 2020-92). MFDS. Available online: https://www.mfds.go.kr/eng/brd/m_15/view.do?seq=70011 (accessed on 23 September 2020).
- Lee, B.; Sur, B.; Park, J.; Kim, S.-H.; Kwon, S.; Yeom, M.; Shim, I.; Lee, H.; Hahm, D.-H. Ginsenoside rg3 alleviates lipopolysaccharide-induced learning and memory impairments by anti-inflammatory activity in rats. Biomol. Ther. 2013, 21, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Yan, M.-H.; Liu, Y.; Liu, Z.; Wang, Z.; Chen, C.; Zhang, J.; Sun, Y.-S. Ginsenoside Rg5 ameliorates cisplatin-induced nephrotoxicity in mice through inhibition of inflammation, oxidative stress, and apoptosis. Nutrients 2016, 8, 566. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.-N.; Xu, X.-Y.; Li, W.; Wang, Y.-M.; Liu, Y.; Wang, Z.; Wang, Y.-P. Ginsenoside Rk1 ameliorates paracetamol-induced hepatotoxicity in mice through inhibition of inflammation, oxidative stress, nitrative stress and apoptosis. J. Ginseng Res. 2019, 43, 10–19. [Google Scholar] [CrossRef]
- Kim, J.-K.; Choi, M.S.; Jeung, W.; Ra, J.; Yoo, H.H.; Kim, D.-H. Effects of gut microbiota on the pharmacokinetics of protopanaxadiol ginsenosides Rd, Rg3, F2, and compound K in healthy volunteers treated orally with red ginseng. J. Ginseng Res. 2020, 44, 611–618. [Google Scholar] [CrossRef]
- Xie, J.-T.; Mehendale, S.R.; Li, X.; Quigg, R.; Wang, X.; Wang, C.-Z.; Wu, J.A.; Aung, H.H.; Rue, P.A.; Bell, G.I. Anti-diabetic effect of ginsenoside Re in ob/ob mice. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2005, 1740, 319–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Li, Y.-F.; Han, X.-Y.; Sun, Y.-S.; Zhang, L.-X.; Liu, W.; Liu, X.-X.; Li, W.; Liu, Y.-Y. Kidney protection effect of ginsenoside re and its underlying mechanisms on cisplatin-induced kidney injury. Cell. Physiol. Biochem. 2018, 48, 2219–2229. [Google Scholar] [CrossRef]
- Zhou, X.-M.; Cao, Y.-L.; Dou, D.-Q. Protective effect of ginsenoside-Re against cerebral ischemia/reperfusion damage in rats. Biol. Pharm. Bull. 2006, 29, 2502–2505. [Google Scholar] [CrossRef] [Green Version]
- Xie, C.-L.; Li, J.-H.; Wang, W.-W.; Zheng, G.-Q.; Wang, L.-X. Neuroprotective effect of ginsenoside-Rg1 on cerebral ischemia/reperfusion injury in rats by downregulating protease-activated receptor-1 expression. Life Sci. 2015, 121, 145–151. [Google Scholar] [CrossRef]
- Quan, L.-H.; Cheng, L.-Q.; Kim, H.-B.; Kim, J.-H.; Son, N.-R.; Kim, S.-Y.; Jin, H.-O.; Yang, D.-C. Bioconversion of ginsenoside Rd into compound K by Lactobacillus pentosus DC101 isolated from Kimchi. J. Ginseng Res. 2010, 34, 288–295. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Zhu, X.-M.; Wang, Q.-J.; Zhang, D.-L.; Fang, Z.-M.; Wang, C.-Y.; Wang, Z.; Sun, B.-S.; Wu, H.; Sung, C.-K. Enzymatic preparation of 20(S, R)-protopanaxadiol by transformation of 20(S, R)-Rg3 from black ginseng. Phytochemistry 2010, 71, 1514–1520. [Google Scholar] [CrossRef]
- Hou, J.; Xue, J.; Wang, C.; Liu, L.; Zhang, D.; Wang, Z.; Li, W.; Zheng, Y.; Sung, C. Microbial transformation of ginsenoside Rg3 to ginsenoside Rh2 by Esteya vermicola CNU 120806. World J. Microbiol. Biotechnol. 2012, 28, 1807–1811. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.; Li, J.; Feng, Z.; Zhao, L.; Luo, L.; You, Z.; Li, D.; Xia, J.; Zuo, G.; Chen, D. Effect of ginsenoside Rh2 on the migratory ability of HepG2 liver carcinoma cells: Recruiting histone deacetylase and inhibiting activator protein 1 transcription factors. Mol. Med. Rep. 2014, 10, 1779–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Gao, Y.; Ma, W.; Guo, W.; Zhou, G.; Cheng, T.; Liu, Y. EGFR signaling-dependent inhibition of glioblastoma growth by ginsenoside Rh2. Tumour Biol. 2014, 35, 5593–5598. [Google Scholar] [CrossRef] [PubMed]
- Baatar, D.; Siddiqi, M.Z.; Im, W.T.; Ul Khaliq, N.; Hwang, S.G. Anti-Inflammatory Effect of Ginsenoside Rh2-Mix on Lipopolysaccharide-Stimulated RAW 264.7 Murine Macrophage Cells. J. Med. Food 2018, 21, 951–960. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ginsenosides | TRT (N 1) | PK Parameters | |||
|---|---|---|---|---|---|
| Cmax (ng/mL) | Tmax (h) | AUC24 (ng·h/mL) | AUClast (ng·h/mL) | ||
| Rb1 | RG (19) | 2.8 ± 1.0 (0.2) | 7.0 (4.0, 14.0) | 51.0 ± 18.9 (4.3) | 91.7 ± 35.4 (8.1) |
| BG (18) | 1.8 ± 0.7 (0.2) * | 7.0 (5.0, 12.0) | 29.1 ± 12.0 (2.8) * | 51.5 ± 23.4 (5.5) * | |
| Rb2 | RG (18) | 1.5 ± 0.5 (0.1) | 7.5 (5.0, 48.0) | 24.6 ± 11.5 (2.6) | 50.8 ± 21.6 (5.1) |
| BG (15) | 1.1 ± 0.4 (0.1) * | 7.0 (5.0, 12.0) | 13.7 ± 9.9 (2.3) * | 30.9 ± 17.7 (4.6) * | |
| Rc | RG (19) | 1.5 ± 0.5 (0.1) | 7.0 (6.0, 14.0) | 26.4 ± 10.1 (2.3) | 49.5 ± 20.9 (4.8) |
| BG (15) | 1.0 ± 0.3 (0.1) * | 8.0 (5.0, 12.0) | 11.6 ± 8.3 (2.0) * | 22.8 ± 15.3 (3.9) * | |
| Rd | RG (14) | 1.0 ± 1.1 (0.3) | 8.0 (2.0, 24.0) | 7.8 ± 13.0 (3.0) | 18.2 ± 37.7 (10.1) |
| BG (8) | 0.9 ± 0.4 (0.2) | 8.0 (6.0, 8.0) | 3.6 ± 7.1 (1.7) | 9.6 ± 15.7 (5.6) | |
| Rg3 | RG (19) | 1.6 ± 1.0 (0.2) | 4.0 (3.0, 5.0) | 9.0 ± 5.6 (1.3) | 8.7 ± 6.0 (1.4) |
| BG (18) | 7.3 ± 2.3 (0.5) * | 5.0 (2.1, 6.0) * | 64.7 ± 23.4 (5.5) * | 63.0 ± 27.1 (6.4) * | |
| Rg5 | RG (16) | 1.4 ± 0.6 (0.2) | 5.0 (3.0, 5.0) | 3.4 ± 2.7 (0.6) | 3.6 ± 2.5 (0.6) |
| BG (18) | 7.6 ± 2.7 (0.6) * | 5.0 (5.0, 5.1) | 38.9 ± 13.3 (3.1) * | 37.4 ± 12.0 (2.8) * | |
| Rk1 | RG (7) | 0.7 ± 0.3 (0.1) | 5.0 (2.0, 6.0) | 0.6 ± 1.3 (0.3) | 1.3 ± 1.6 (0.6) |
| BG (18) | 2.8 ± 1.0 (0.2) * | 5.0 (5.0, 5.1) | 15.0 ± 5.0 (1.2) * | 14.3 ± 5.0 (1.2) * | |
| Rh2 | RG (17) | 1.6 ± 1.1 (0.3) | 10.0 (2.0, 14.0) | 9.5 ± 7.3 (1.7) | 8.2 ± 5.6 (1.4) |
| BG (18) | 16.9 ± 12.4 (2.9) * | 10.0 (2.0, 14.0) | 157.1 ± 107.3 (25.3) * | 152.1 ± 111.8 (26.3) * | |
| CK | RG (18) | 11.7 ± 6.3 (1.5) | 12.0 (8.0, 30.0) | 103.5 ± 58.5 (13.4) | 136.2 ± 74.8 (17.6) |
| BG (18) | 11.7 ± 13.5 (3.2) | 12.0 (2.0, 24.0) | 123.0 ± 135.7 (32.0) | 147.5 ± 169.4 (39.9) | |
| PPD | RG (18) | 3.8 ± 2.3 (0.5) | 24.0 (8.0, 30.0) | 37.5 ± 33.5 (7.7) | 80.0 ± 71.9 (16.9) |
| BG (17) | 5.1 ± 3.5 (0.9) | 24.0 (12.0, 30.0) | 57.8 ± 47.6 (11.2) | 107.3 ± 74.5 (18.1) | |
| Re 2 | RG (0) | – | – | – | – |
| BG (0) | – | – | – | – | |
| Rg1 3 | RG (0) | – | – | – | – |
| BG (0) | – | – | – | – | |
| Rh1 4 | RG (0) | – | – | 0.0 ± 0.0 (0.0) | – |
| BG (16) | 1.2 ± 0.6 (0.2) | 5.0 (3.0, 10.0) | 6.2 ± 6.8 (1.6) | 6.3 ± 6.7 (1.7) | |
| PPT | RG (19) | 5.8 ± 4.4 (1.0) | 14.0 (6.0, 30.0) | 56.0 ± 54.4 (12.5) | 95.5 ± 86.9 (19.9) |
| BG (18) | 6.1 ± 4.6 (1.1) | 24.0 (5.0, 30.0) | 63.5 ± 49.6 (11.7) | 102.2 ± 76.2 (18.0) | |
| Ginsenosides | TRT (N 1) | PK Parameters | |||
|---|---|---|---|---|---|
| Cmax (ng/mL) | Tmax (h) | AUC24 (ng·h/mL) | AUClast (ng·h/mL) | ||
| Rb1 + Rg1 + Rg3 | RG (19) | 4.0 ± 1.4 (0.3) | 6.0 (3.0, 12.0) | 60.0 ± 20.9 (4.8) | 100.8 ± 37.3 (8.6) |
| BG (18) | 8.8 ± 2.6 (0.6) * | 5.0 (2.1, 6.0) * | 93.6 ± 31.2 (7.4) * | 118.2 ± 44.3 (10.4) | |
| Rg3 + Rg5 + Rk1 | RG (19) | 2.8 ± 1.9 (0.4) | 5.0 (2.0, 5.0) | 12.8 ± 8.7 (2.0) | 12.2 ± 8.6 (2.0) |
| BG (18) | 17.5 ± 5.7 (1.3) * | 5.0 (5.0, 5.1) | 118.3 ± 37.0 (8.7) * | 116.2 ± 40.1 (9.4) * | |
| Ginsenosides | TRT (N 1) | PK Parameters | |||
|---|---|---|---|---|---|
| Cmax (ng/mL) | Tmax (h) | AUC24 (ng·h/mL) | AUClast (ng·h/mL) | ||
| Total | RG (19) | 24.7 ± 6.9 (1.6) | 14.0 (5.0, 30.0) | 331.6 ± 85.3 (19.6) | 547.6 ± 134.3 (30.8) |
| BG (18) | 45.5 ± 25.4 (6.0) * | 9.0 (5.0, 14.0) * | 592.4 ± 285.9 (67.4) * | 767.0 ± 317.4 (74.8) * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, S.; Park, B.-I.; Kim, D.-h.; Lee, S.; Lee, S.-h.; Shim, W.-S.; Seo, Y.K.; Kang, K.; Lee, K.-T.; Yim, S.-V.; et al. Ginsenoside Absorption Rate and Extent Enhancement of Black Ginseng (CJ EnerG) over Red Ginseng in Healthy Adults. Pharmaceutics 2021, 13, 487. https://doi.org/10.3390/pharmaceutics13040487
Yoo S, Park B-I, Kim D-h, Lee S, Lee S-h, Shim W-S, Seo YK, Kang K, Lee K-T, Yim S-V, et al. Ginsenoside Absorption Rate and Extent Enhancement of Black Ginseng (CJ EnerG) over Red Ginseng in Healthy Adults. Pharmaceutics. 2021; 13(4):487. https://doi.org/10.3390/pharmaceutics13040487
Chicago/Turabian StyleYoo, Saebyul, Bom-I Park, Do-hyun Kim, Sooyoung Lee, Seung-hoon Lee, Wang-Seob Shim, Yong Ki Seo, Kimoon Kang, Kyung-Tae Lee, Sung-Vin Yim, and et al. 2021. "Ginsenoside Absorption Rate and Extent Enhancement of Black Ginseng (CJ EnerG) over Red Ginseng in Healthy Adults" Pharmaceutics 13, no. 4: 487. https://doi.org/10.3390/pharmaceutics13040487
APA StyleYoo, S., Park, B. -I., Kim, D. -h., Lee, S., Lee, S. -h., Shim, W. -S., Seo, Y. K., Kang, K., Lee, K. -T., Yim, S. -V., Soung, D. Y., & Kim, B. -H. (2021). Ginsenoside Absorption Rate and Extent Enhancement of Black Ginseng (CJ EnerG) over Red Ginseng in Healthy Adults. Pharmaceutics, 13(4), 487. https://doi.org/10.3390/pharmaceutics13040487