
Synthesis and In Vivo Evaluation of Insulin-Loaded Whey Beads as an Oral Peptide Delivery System

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation of Manual dWPI Beads Entrapped with Insulin
2.3. Insulin Loading and Encapsulation Efficiency in dWPI Beads
2.4. Insulin Release Studies in Simulated Buffers
2.5. Circular Dichroism
2.6. Proteolysis of Insulin in dWPI Beads
2.7. Cell-Based Bioactivity Assay for dWPI Bead-Released Insulin
2.8. Encapsulator-Generated Prototype Beads
2.9. In Situ Jejunal Instillations
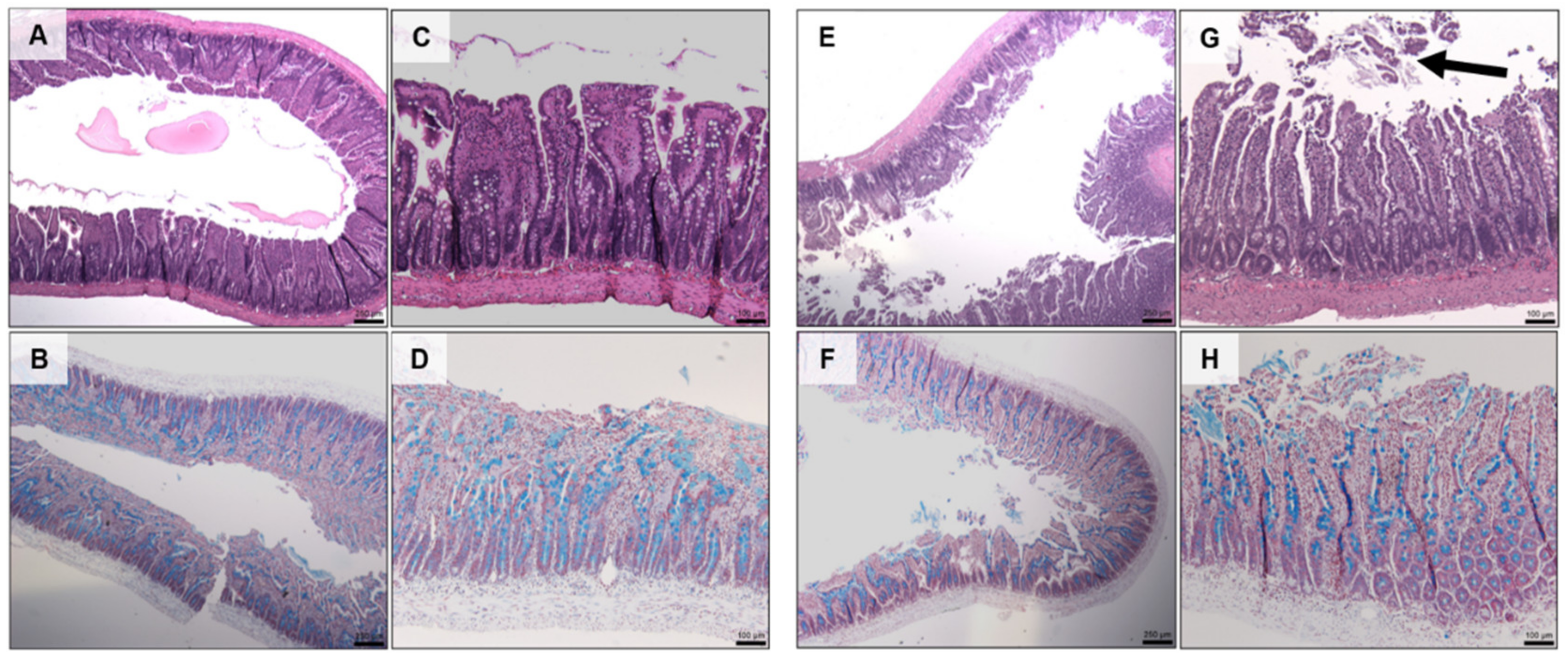
2.10. Histology
2.11. Statistical Analysis
3. Results
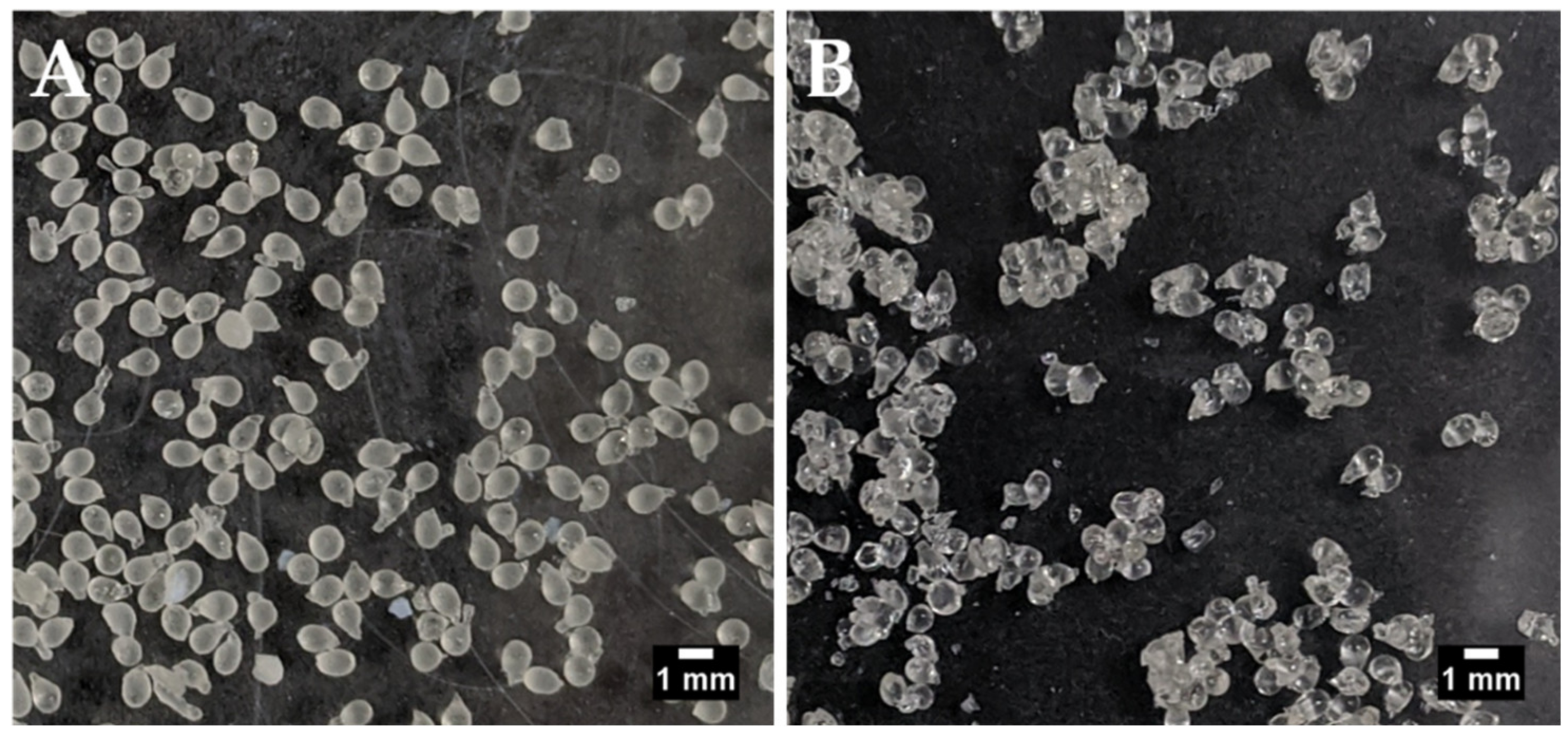
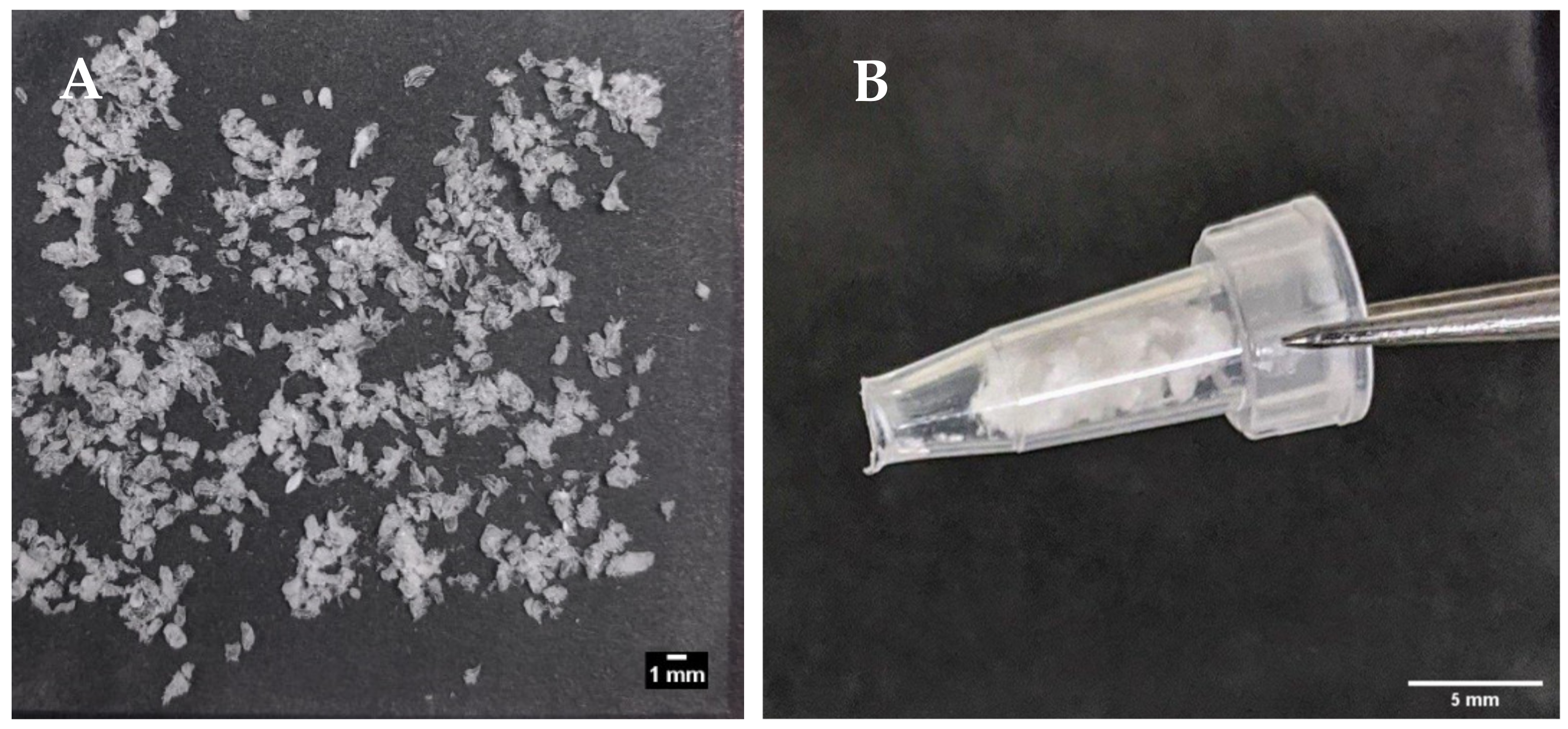
3.1. Size, Encapsulation Efficiency, and Loading of Insulin Loaded Whey Beads
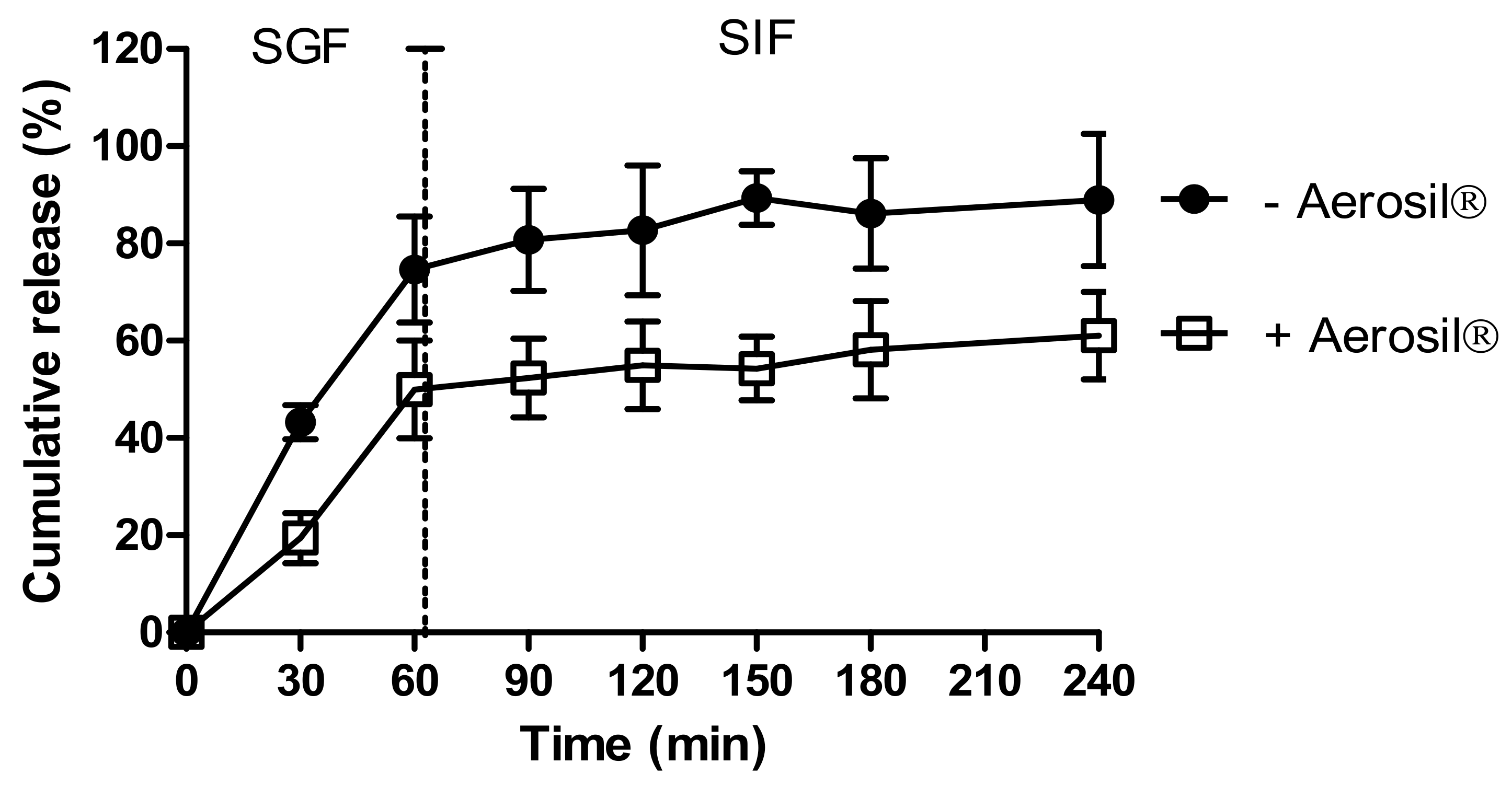
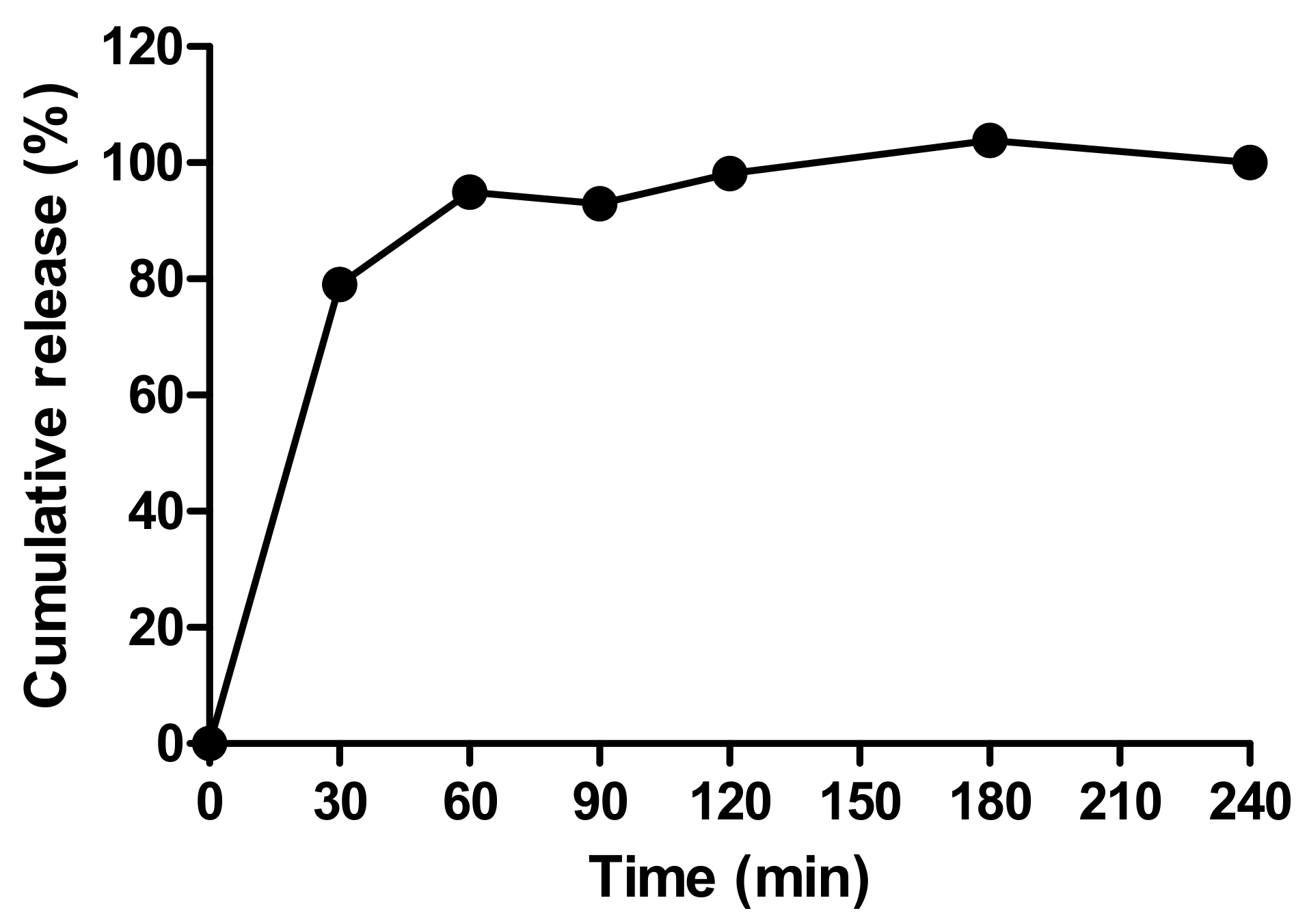
3.2. Release of Insulin in Simulated Intestinal Fluids
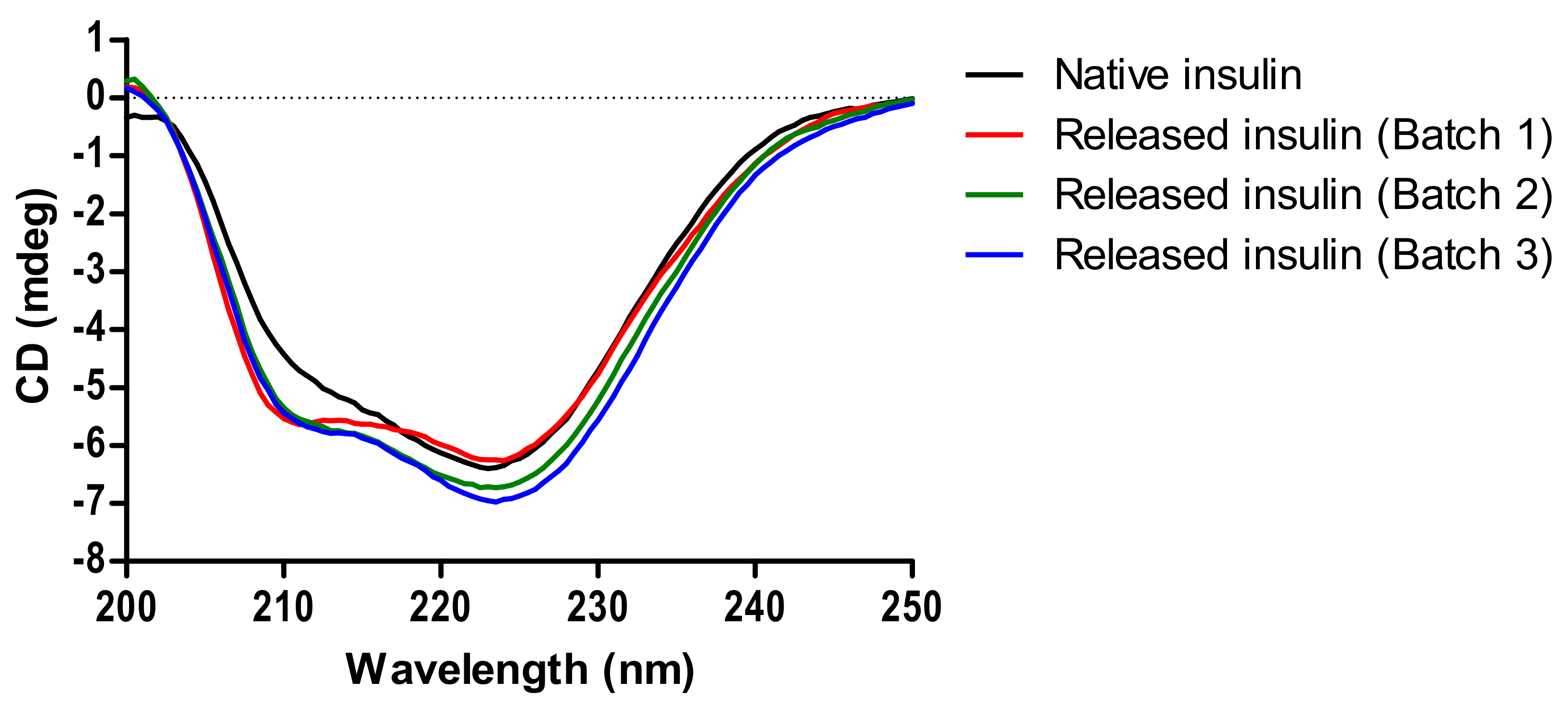
3.3. Structural Analysis of Released Insulin by CD
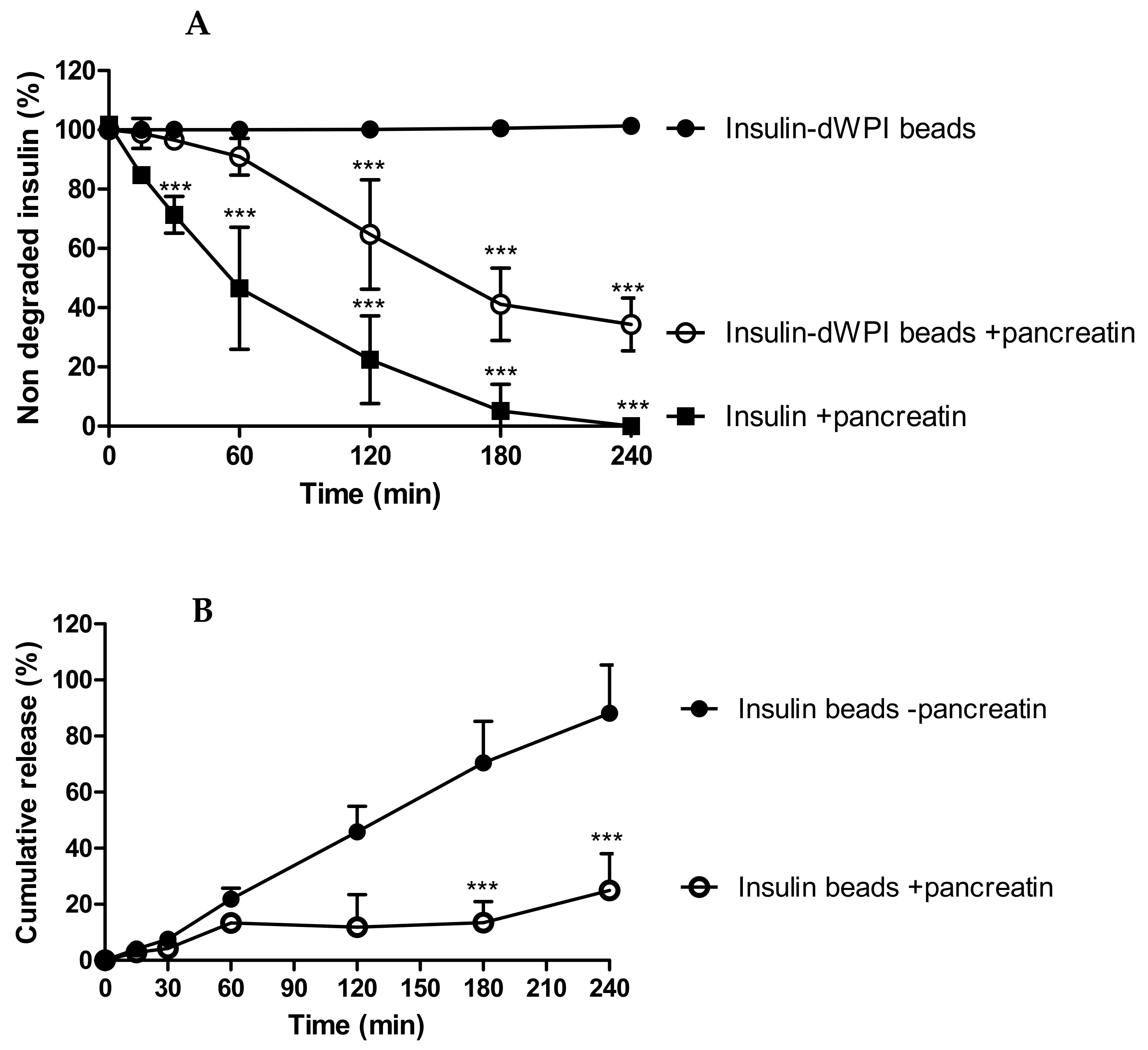
3.4. Degradation of dWPI Bead-Released Insulin by Pancreatin
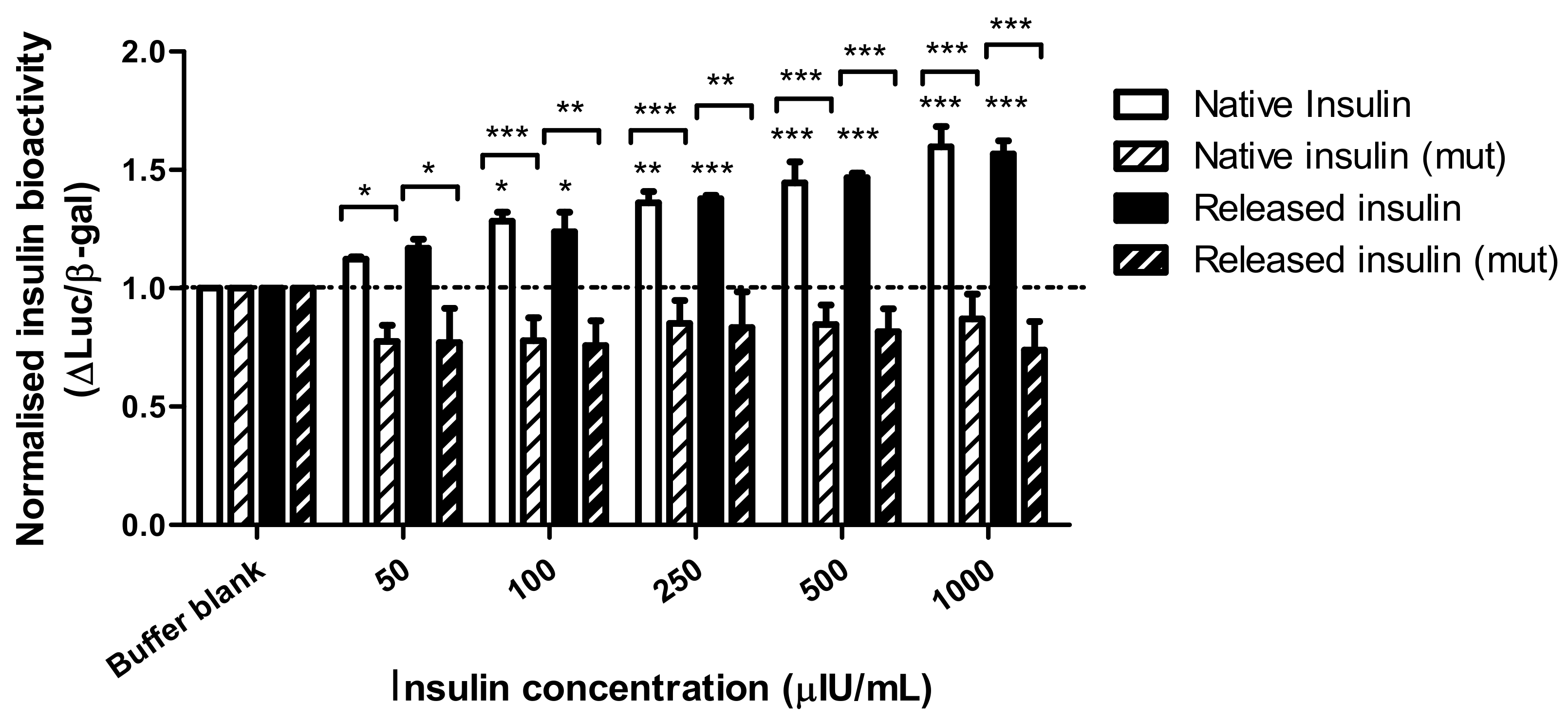
3.5. Bioactivity of dWPI-Released Insulin in Transfected HepG2 Cells Expressing Human Endogenous Insulin Receptors
3.6. Characterisation of Prototype Insulin-dWPI Beads Made by the Buchi Encapsulator
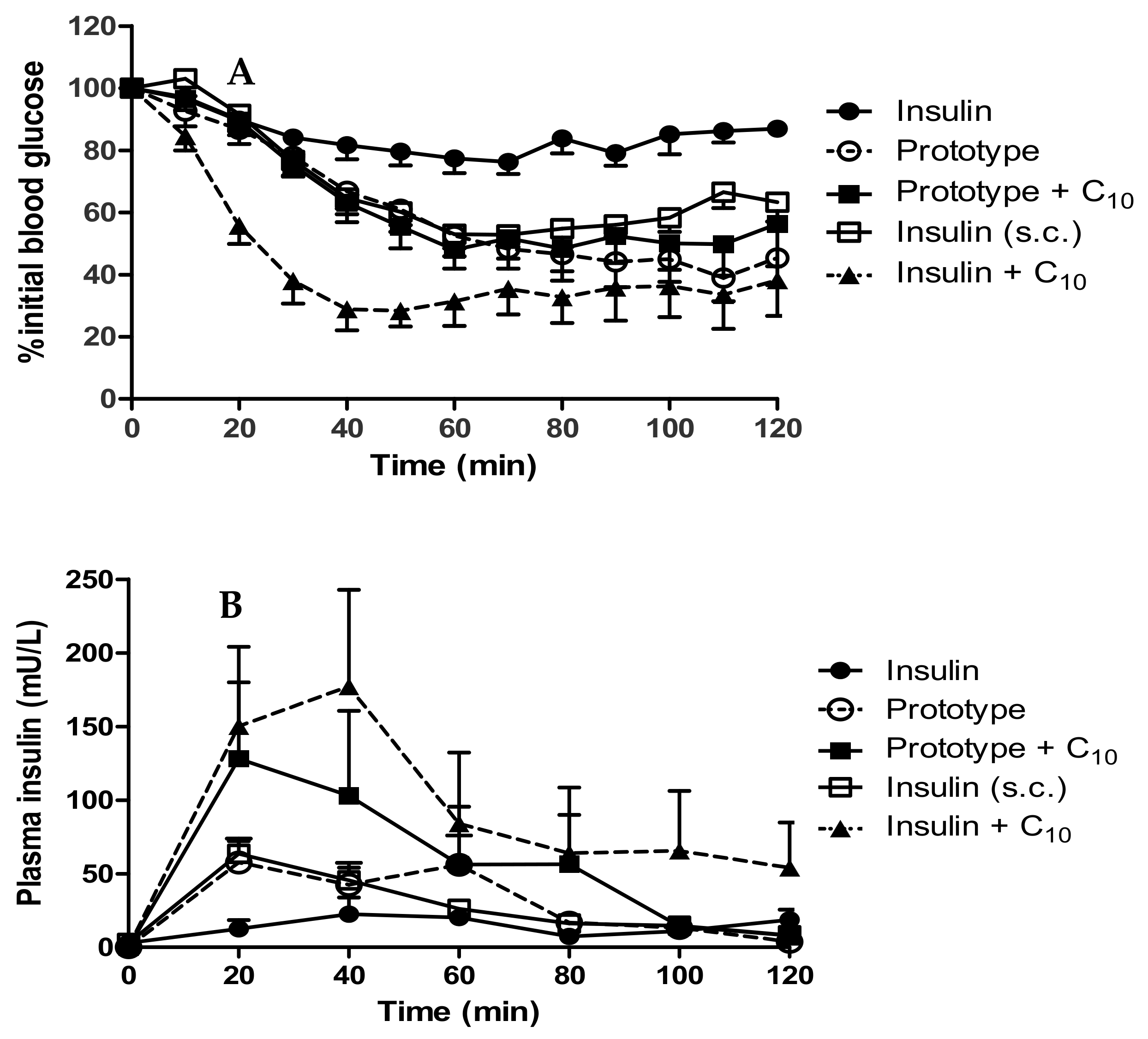
3.7. In Vivo Performance of Insulin-Loaded Prototype dWPI Beads: Rat Jejunal Instillations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brayden, D.J.; Hill, T.A.; Fairlie, D.P.; Maher, S.; Mrsny, R.J. Systemic Delivery of Peptides by the Oral Route: Formulation and Medicinal Chemistry Approaches. Adv. Drug Deliv. Rev. 2020, 157, 2–36. [Google Scholar] [CrossRef]
- Kapitza, C.; Zijlstra, E.; Heinemann, L.; Castelli, M.C.; Riley, G.; Heise, T. Oral insulin: A comparison with subcutaneous regular human insulin in patients with type 2 diabetes. Diabetes Care 2010, 33, 1288–1290. [Google Scholar] [CrossRef] [Green Version]
- Bruno, B.J.; Miller, G.D.; Lim, C.S. Basics and recent advances in peptide and protein drug delivery. Ther. Deliv. 2013, 4, 1443–1467. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, L.B.; Lau, J. The discovery and development of liraglutide and semaglutide. Front. Endocrinol. 2019, 10, 155. [Google Scholar] [CrossRef] [Green Version]
- Tuvia, S.; Atsmon, J.; Teichman, S.L.; Katz, S.; Salama, P.; Pelled, D.; Landau, I.; Karmeli, I.; Bidlingmaier, M.; Strasburger, C.J.; et al. Oral octreotide absorption in human subjects: Comparable pharmacokinetics to parenteral octreotide and effective growth hormone suppression. J. Clin. Endocrinol. Metab. 2012, 97, 2362–2369. [Google Scholar] [CrossRef] [Green Version]
- Dubey, S.K.; Parab, S.; Dabholkar, N.; Agrawal, M.; Singhvi, G.; Alexander, A.; Bapat, R.A.; Kesharwani, P. Oral peptide delivery: Challenges and the way ahead. Drug Discov. Today 2021. [Google Scholar] [CrossRef] [PubMed]
- Taverner, A.; Dondi, R.; Almansour, K.; Laurent, F.; Owens, S.E.; Eggleston, I.M.; Fotaki, N.; Mrsny, R.J. Enhanced paracellular transport of insulin can be achieved via transient induction of myosin light chain phosphorylation. J. Control. Release 2015, 210, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Shao, J.; Zaro, J.L.; Shen, W.C. Tissue barriers and novel approaches to achieve hepatoselectivity of subcutaneously-injected insulin therapeutics. Tissue Barriers 2016, 4, e1156804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamont, T.; Cousins, D.; Hillson, R.; Bischler, A.; Terblanche, M. Safer administration of insulin: Summary of a safety report from the National Patient Safety Agency. BMJ 2010, 341, c5269. [Google Scholar] [CrossRef]
- Saffran, M.; Pansky, B.; Budd, G.C.; Williams, F.E. Insulin and the gastrointestinal tract. J. Control. Release 1997, 46, 89–98. [Google Scholar] [CrossRef]
- Halberg, I.B.; Lyby, K.; Wassermann, K.; Heise, T.; Zijlstra, E.; Plum-Mörschel, L. Efficacy and safety of oral basal insulin versus subcutaneous insulin glargine in type 2 diabetes: A randomised, double-blind, phase 2 trial. Lancet Diabetes Endocrinol. 2019, 7, 179–188. [Google Scholar] [CrossRef]
- Layek, B.; Mandal, S. Natural polysaccharides for controlled delivery of oral therapeutics: A recent update. Carbohydr. Polym. 2020, 230, 115617. [Google Scholar] [CrossRef]
- Sonia, T.A.; Sharma, C.P. An overview of natural polymers for oral insulin delivery. Drug Discov. Today 2012, 17, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Hsein, H.; Garrait, G.; Mumin, M.A.; Beyssac, E.; Hoffart, V. Atomization of denatured whey proteins as a novel and simple way to improve oral drug delivery system properties. Int. J. Biol. Macromol. 2017, 105, 801–809. [Google Scholar] [CrossRef]
- Déat-Lainé, E.; Hoffart, V.; Cardot, J.M.; Subirade, M.; Beyssac, E. Development and in vitro characterization of insulin loaded whey protein and alginate microparticles. Int. J. Pharm. 2012, 439, 136–144. [Google Scholar] [CrossRef]
- Galvão, C.M.; Silva, A.F.; Custódio, M.F.; Monti, R.; Giordano, R.L. Controlled hydrolysis of cheese whey proteins using trypsin and alpha-chymotrypsin. Appl. Biochem. Biotechnol. 2001, 91–93, 761–776. [Google Scholar] [CrossRef]
- Lacroix, I.M.; Li-Chan, E.C. Isolation and characterization of peptides with dipeptidyl peptidase-IV inhibitory activity from pepsin-treated bovine whey proteins. Peptides 2014, 54, 39–48. [Google Scholar] [CrossRef]
- Déat-Lainé, E.; Hoffart, V.; Garrait, G.; Beyssac, E. Whey protein and alginate hydrogel microparticles for insulin intestinal absorption: Evaluation of permeability enhancement properties on Caco-2 cells. Int. J. Pharm. 2013, 453, 336–342. [Google Scholar] [CrossRef]
- Boddupalli, B.M.; Mohammed, Z.N.; Nath, R.A.; Banji, D. Mucoadhesive drug delivery system: An overview. J. Adv. Pharm. Technol. Res. 2010, 1, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Pharmacopeia. USP29 Reagents: Test Solutions (TS). Available online: http://ftp.uspbpep.com/v29240/usp29nf24s0_ris1s126.html (accessed on 22 March 2021).
- Sarmento, B.; Ribeiro, A.; Veiga, F.; Ferreira, D. Development and validation of a rapid reversed-phase HPLC method for the determination of insulin from nanoparticulate systems. Biomed. Chromatogr. 2006, 20, 898–903. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Huo, M.; Zhou, J.; Zou, A.; Li, W.; Yao, C.; Xie, S. DDSolver: An add-in program for modeling and comparison of drug dissolution profiles. AAPS J. 2010, 12, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Whitmore, L.; Wallace, B.A. DICHROWEB, an online server for protein secondary structure analyses from circular dichroism spectroscopic data. Nucleic Acids Res. 2004, 32, W668–W673. [Google Scholar] [CrossRef] [Green Version]
- Sreerama, N.; Woody, R.W. Estimation of protein secondary structure from circular dichroism spectra: Comparison of CONTIN, SELCON, and CDSSTR methods with an expanded reference set. Anal. Biochem. 2000, 287, 252–260. [Google Scholar] [CrossRef]
- Presas, E.; McCartney, F.; Sultan, E.; Hunger, C.; Nellen, S.; Alvarez, C.V.; Werner, U.; Bazile, D.; Brayden, D.J.; O’Driscoll, C.M. Physicochemical, pharmacokinetic and pharmacodynamic analyses of amphiphilic cyclodextrin-based nanoparticles designed to enhance intestinal delivery of insulin. J. Control. Release 2018, 286, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Santalices, I.; Vázquez-Vázquez, C.; Santander-Ortega, M.J.; Lozano, V.; Araújo, F.; Sarmento, B.; Shrestha, N.; Préat, V.; Chenlo, M.; Alvarez, C.V.; et al. A nanoemulsion/micelles mixed nanosystem for the oral administration of hydrophobically modified insulin. Drug Deliv. Transl. Res. 2021. [Google Scholar] [CrossRef]
- Dooley, K.A.; Millinder, S.; Osborne, T.F. Sterol regulation of 3-hydroxy-3-methylglutaryl-coenzyme A synthase gene through a direct interaction between sterol regulatory element binding protein and the trimeric CCAAT-binding factor/nuclear factor Y. J. Biol. Chem. 1998, 273, 1349–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.R.; Osborne, T.F.; Brown, M.S.; Goldstein, J.L.; Gil, G. Multiple sterol regulatory elements in promoter for hamster 3-hydroxy-3-methylglutaryl-coenzyme A synthase. J. Biol. Chem. 1988, 263, 18480–18487. [Google Scholar] [CrossRef]
- Harris, I.R.; Höppner, H.; Siefken, W.; Farrell, A.M.; Wittern, K.P. Regulation of HMG-CoA synthase and HMG-CoA reductase by insulin and epidermal growth factor in HaCaT keratinocytes. J. Investig. Dermatol. 2000, 114, 83–87. [Google Scholar] [CrossRef]
- Hébrard, G.; Hoffart, V.; Cardot, J.M.; Subirade, M.; Beyssac, E. Development and characterization of coated-microparticles based on whey protein/alginate using the Encapsulator device. Drug Dev. Ind. Pharm. 2013, 39, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Doherty, S.B.; Gee, V.L.; Ross, R.P.; Stanton, C.; Fitzgerald, G.F.; Brodborb, A. Development and characterisation of whey protein micro-beads as potential matrices for probiotic protection. Food Hydrocoll. 2011, 25, 1604–1617. [Google Scholar] [CrossRef]
- BÜCHI. Application Note No. 137: Encapsulation within gelatin beads. Available online: https://static1.buchi.com/sites/default/files/AN_137-2013_Production_of_gelatin_particles.pdf (accessed on 26 April 2020).
- Aguirre, T.A.S.; Aversa, V.; Rosa, M.; Guterres, S.S.; Pohlmann, A.R.; Coulter, I.; Brayden, D.J. Coated minispheres of salmon calcitonin target rat intestinal regions to achieve systemic bioavailability: Comparison between intestinal instillation and oral gavage. J. Control. Release 2016, 238, 242–252. [Google Scholar] [CrossRef]
- Sladek, S.; McCartney, F.; Eskander, M.; Dunne, D.J.; Santos-Martinez, M.J.; Benetti, F.; Tajber, L.; Brayden, D.J. An Enteric-Coated Polyelectrolyte Nanocomplex Delivers Insulin in Rat Intestinal Instillations when Combined with a Permeation Enhancer. Pharmaceutics 2020, 12, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Ji, W.; Peng, H.; Zhao, R.; Zhang, T.; Lu, Z.; Yang, J.; Liu, R.; Zhang, X. Charge-switchable zwitterionic polycarboxybetaine particle as an intestinal permeation enhancer for efficient oral insulin delivery. Theranostics 2021, 11, 4452–4466. [Google Scholar] [CrossRef]
- Wang, X.; Maher, S.; Brayden, D.J. Restoration of rat colonic epithelium after in situ intestinal instillation of the absorption promoter, sodium caprate. Ther. Deliv. 2010, 1, 75–82. [Google Scholar] [CrossRef] [PubMed]
- McCartney, F.; Rosa, M.; Brayden, D.J. Evaluation of sucrose laurate as an intestinal permeation enhancer for macromolecules: Ex vivo and in vivo studies. Pharmaceutics 2019, 11, 565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Huo, M.; Zhou, J.; Xie, S. PKSolver: An add-in program for pharmacokinetic and pharmacodynamic data analysis in Microsoft Excel. Comput. Methods Programs Biomed. 2010, 99, 306–314. [Google Scholar] [CrossRef]
- McCartney, F.; Jannin, V.; Chevrier, S.; Boulghobra, H.; Hristov, D.R.; Ritter, N.; Miolane, C.; Chavant, Y.; Demarne, F.; Brayden, D.J. Labrasol® is an efficacious intestinal permeation enhancer across rat intestine: Ex vivo and in vivo rat studies. J. Control. Release 2019, 310, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Supramaniam, J.; Adnan, R.; Mohd Kaus, N.H.; Bushra, R. Magnetic nanocellulose alginate hydrogel beads as potential drug delivery system. Int. J. Biol. Macromol. 2018, 118, 640–648. [Google Scholar] [CrossRef]
- Amaral, M.; Martins, A.S.; Catarino, J.; Faísca, P.; Kumar, P.; Pinto, J.F.; Pinto, R.; Correia, I.; Ascensão, L.; Afonso, R.A.; et al. How can biomolecules improve mucoadhesion of oral insulin? A comprehensive insight using ex vivo, in silico, and in vivo models. Biomolecules 2020, 10, 675. [Google Scholar] [CrossRef]
- Bruschi, M.L. Mathematical models of drug release. In Strategies to Modify the Drug Release from Pharmaceutical Systems; Woodhead Publishing: Cambridge, UK, 2015; pp. 63–84. [Google Scholar]
- Juère, E.; Caillard, R.; Marko, D.; Del Favero, G.; Kleitz, F. Smart protein-based formulation of dendritic mesoporous silica nanoparticles: Toward oral delivery of insulin. Chemistry 2020, 26, 5195–5199. [Google Scholar] [CrossRef]
- Swinnen, S.G.; Hoekstra, J.B.; DeVries, J.H. Insulin therapy for type 2 diabetes. Diabetes Care 2009, 32 (Suppl. 2), S253–S259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarmento, B.; Ribeiro, A.; Veiga, F.; Sampaio, P.; Neufeld, R.; Ferreira, D. Alginate/chitosan nanoparticles are effective for oral insulin delivery. Pharm. Res. 2007, 24, 2198–2206. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, P.; Hoong Leong, K.; Nyamathulla, S.; Onuki, Y.; Takayama, K.; Yong Chung, L. Chitosan complexed carboxymethylated iota-carrageenan oral insulin particles: Stability, permeability and in vivo evaluation. Mater. Today Commun. 2019, 20, 100557. [Google Scholar] [CrossRef]
- Tuvia, S.; Pelled, D.; Marom, K.; Salama, P.; Levin-Arama, M.; Karmeli, I.; Idelson, G.H.; Landau, I.; Mamluk, R. A novel suspension formulation enhances intestinal absorption of macromolecules via transient and reversible transport mechanisms. Pharm. Res. 2014, 31, 2010–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melmed, S.; Polonsky, K.S.; Larsen, P.R.; Kronenberg, H.M. Williams Textbook of Endocrinology, 12th ed.; Elsevier Health Sciences: Philadelphia, PA, USA, 2011. [Google Scholar]
- Fonte, P.; Soares, S.; Costa, A.; Andrade, J.C.; Seabra, V.; Reis, S.; Sarmento, B. Effect of cryoprotectants on the porosity and stability of insulin-loaded PLGA nanoparticles after freeze-drying. Biomatter 2012, 2, 329–339. [Google Scholar] [CrossRef] [Green Version]
- Doherty, S.B.; Auty, M.A.; Stanton, C.; Ross, R.P.; Fitzgerald, G.F.; Brodkorb, A. Application of whey protein micro-bead coatings for enhanced strength and probiotic protection during fruit juice storage and gastric incubation. J. Microencapsul. 2012, 29, 713–728. [Google Scholar] [CrossRef] [PubMed]
- Hristov, D.; McCartney, F.; Beirne, J.; Mahon, E.; Reid, S.; Bhattacharjee, S.; Penarier, G.; Werner, U.; Bazile, D.; Brayden, D.J. Silica-coated nanoparticles with a core of zinc, L-arginine, and a peptide designed for oral delivery. ACS Appl. Mater. Interfaces 2020, 12, 1257–1269. [Google Scholar] [CrossRef]
- Maher, S.; Geoghegan, C.; Brayden, D.J. Intestinal permeation enhancers to improve oral bioavailability of macromolecules: Reasons for low efficacy in humans. Expert Opin. Drug Deliv. 2021, 18, 273–300. [Google Scholar] [CrossRef] [PubMed]
- Berg, S.; Krause, J.; Björkbom, A.; Walter, K.; Harun, S.; Granfeldt, A.; Janzén, D.; Nunes, S.F.; Antonsson, M.; Van Zuydam, N.; et al. In vitro and in vivo evaluation of 3D printed capsules with pressure triggered release mechanism for oral peptide delivery. J. Pharm. Sci. 2021, 110, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Thanou, M.; Verhoef, J.C.; Junginger, H.E. Chitosan and its derivatives as intestinal absorption enhancers. Adv. Drug Deliv. Rev. 2001, 50 (Suppl. 1), S91–S101. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Shelf Temp (°C) | Ramp Rate (°C) | Hold Time (min) | Vacuum (mbar) | |
|---|---|---|---|---|
| Loading | 5 | 0.5 | 30 | ~700 |
| Freezing | −40 | 0.5 | 300 | ~700 |
| Primary drying | −30 | 0.3 | 2800 | 0.13 |
| Secondary drying | 25 | 0.3 | 240 | 0.13 |
| Storage | 5 | NA | NA | 800 |
| Air-Dried Beads | Diameter (mm) | EE (%) | Loading (%) | Loading (µg/mg Beads) |
|---|---|---|---|---|
| + Aerosil® | 1.49 ± 0.27 *** | 61.42 ± 11.01 | 2.46 ± 0.34 | 24.65 ± 3.38 |
| − Aerosil® | 1.09 ± 0.13 | 72.59 ± 21.26 | 3.22 ± 0.40 | 32.78 ± 4.84 |
| Helix 1 | Helix 2 | Strand 1 | Strand 2 | Turns | Unordered | |
|---|---|---|---|---|---|---|
| Native insulin | 0.01 | 0.05 | 0.24 | 0.12 | 0.23 | 0.33 |
| Released insulin (Batch 1) | 0.03 | 0.09 | 0.17 | 0.11 | 0.26 | 0.33 |
| Released insulin (Batch 2) | 0.03 | 0.09 | 0.17 | 0.11 | 0.26 | 0.34 |
| Released insulin (Batch 3) | 0.03 | 0.09 | 0.16 | 0.11 | 0.27 | 0.34 |
| Diameter (mm) | EE (%) | Loading (%) | Final Loading (µg/mg) | Beads (mg) per Rat | |
|---|---|---|---|---|---|
| Prototype beads | 1.66 ± 0.89 | 42.02 | 2.77 | 27.71 | 17.53 |
| Tmax (min) | Cmax (mU/L) | AUC (mU/L.min) | % PA | % F | |
|---|---|---|---|---|---|
| Insulin (s.c.) | 23.3 ± 8.2 | 64.9 ± 22.7 | 3356 ± 995 | - | - |
| Beads | 36.7 ± 19.7 | 87.4 ± 38.8 | 3761 ± 1429 | 2.4 | 2.2 |
| Beads + C10 | 25.0 ± 10.0 | 128.9 ± 105.4 | 7239 ± 6675 | 2.3 | 4.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heade, J.; McCartney, F.; Chenlo, M.; Marro, O.M.; Severic, M.; Kent, R.; Bleiel, S.B.; Alvarez, C.V.; Griffin, B.T.; Brayden, D.J. Synthesis and In Vivo Evaluation of Insulin-Loaded Whey Beads as an Oral Peptide Delivery System. Pharmaceutics 2021, 13, 656. https://doi.org/10.3390/pharmaceutics13050656
Heade J, McCartney F, Chenlo M, Marro OM, Severic M, Kent R, Bleiel SB, Alvarez CV, Griffin BT, Brayden DJ. Synthesis and In Vivo Evaluation of Insulin-Loaded Whey Beads as an Oral Peptide Delivery System. Pharmaceutics. 2021; 13(5):656. https://doi.org/10.3390/pharmaceutics13050656
Chicago/Turabian StyleHeade, Joanne, Fiona McCartney, Miguel Chenlo, Olga Moreno Marro, Maja Severic, Robert Kent, Sinead B. Bleiel, Clara V. Alvarez, Brendan T. Griffin, and David J. Brayden. 2021. "Synthesis and In Vivo Evaluation of Insulin-Loaded Whey Beads as an Oral Peptide Delivery System" Pharmaceutics 13, no. 5: 656. https://doi.org/10.3390/pharmaceutics13050656
APA StyleHeade, J., McCartney, F., Chenlo, M., Marro, O. M., Severic, M., Kent, R., Bleiel, S. B., Alvarez, C. V., Griffin, B. T., & Brayden, D. J. (2021). Synthesis and In Vivo Evaluation of Insulin-Loaded Whey Beads as an Oral Peptide Delivery System. Pharmaceutics, 13(5), 656. https://doi.org/10.3390/pharmaceutics13050656