
The Road to Better Management in Resistant Hypertension—Diagnostic and Therapeutic Insights

 ,
,
Abstract
:1. Introduction
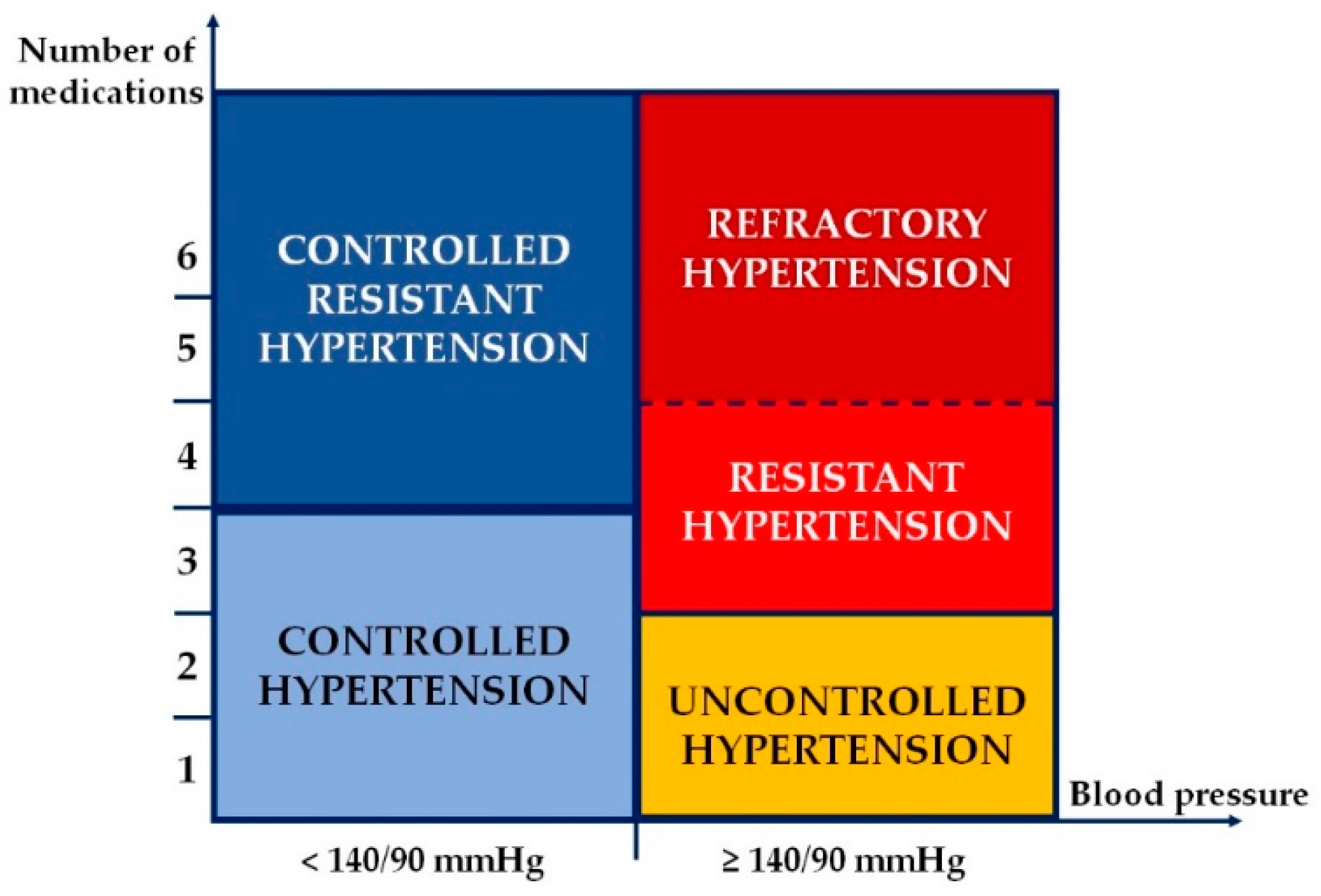
2. Resistant Hypertension-Associated Phenotypes
3. Pathophysiology of Resistant Hypertension
3.1. Role of the Renin-Angiotensin-Aldosterone System
3.2. Role of the Sympathetic Nervous System
3.3. Role of Genetics
4. Diagnostic Approach of Resistant Hypertension
4.1. Confirm Treatment Resistance
- White-coat uncontrolled HTN—in patients with office BP above goal, but out-of-office BP measured by ABPM or HBPM are below target values;
- Masked uncontrolled HTN—in patients with adequate office BP control, but with elevated out-of-office BP measured by either ABPM or HBPM;
- Sustained uncontrolled HTN—in patients whose BP values are elevated at both office and out-of-office measurements.
- Uncontrolled R-HTN—in patients with office BP ≥ 140/90 mmHg and/or 24-h ambulatory BP ≥ 130/80 mmHg, taking three or more antihypertensive medications of different classes, including a diuretic, and usually a long-acting calcium channel blocker and a blocker of the renin-angiotensin system blocker at maximal or maximally tolerated doses;
- Controlled R-HTN—in patients with office BP < 140/90 mmHg and/or 24-h ambulatory BP < 130/80 mmHg, taking at least four antihypertensive medications of different classes.
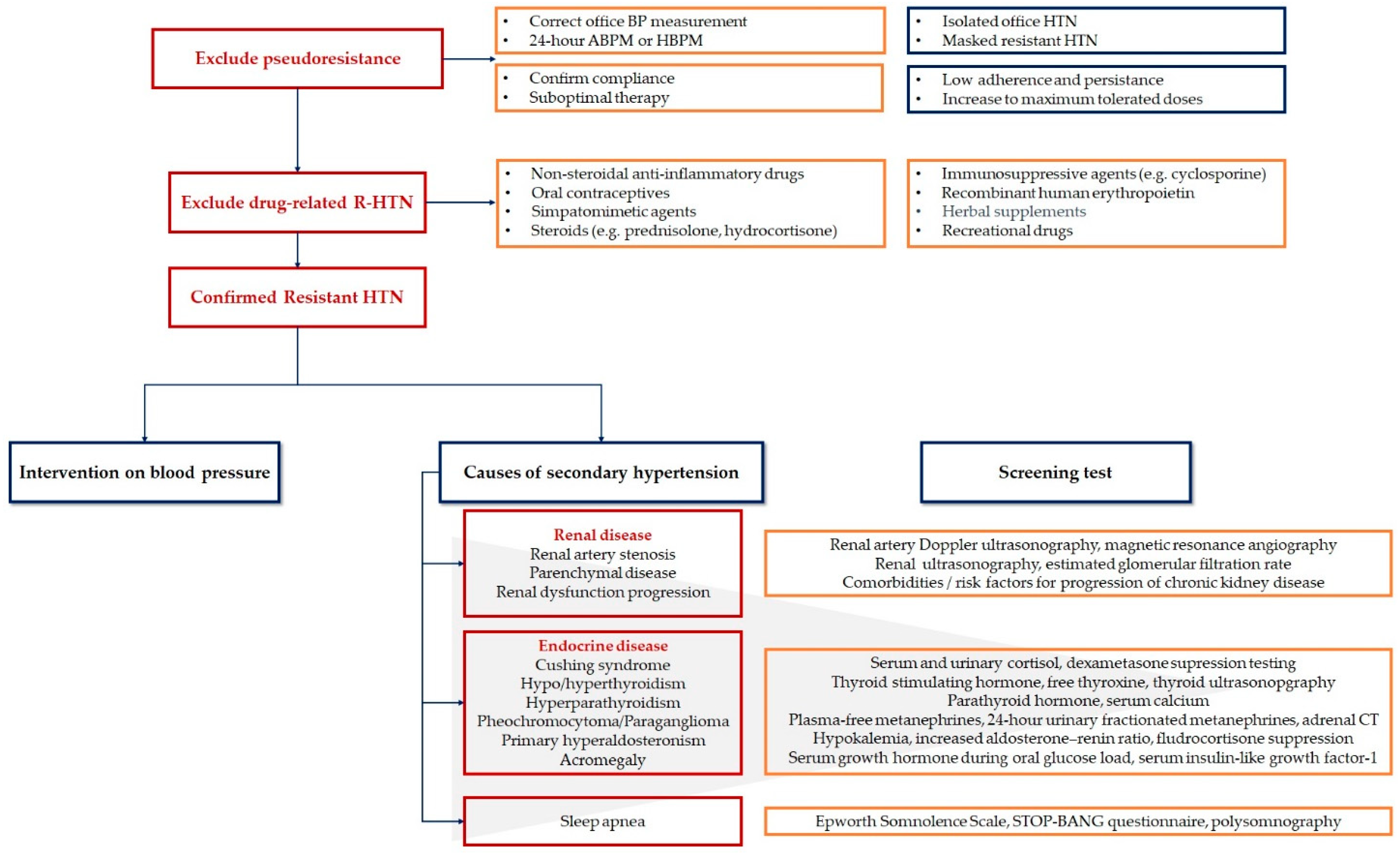
4.2. Exclude Pseudoresistance
4.3. Exclude Drug-Related Resistant Hypertension
4.4. Exclude Secondary Causes of Hypertension
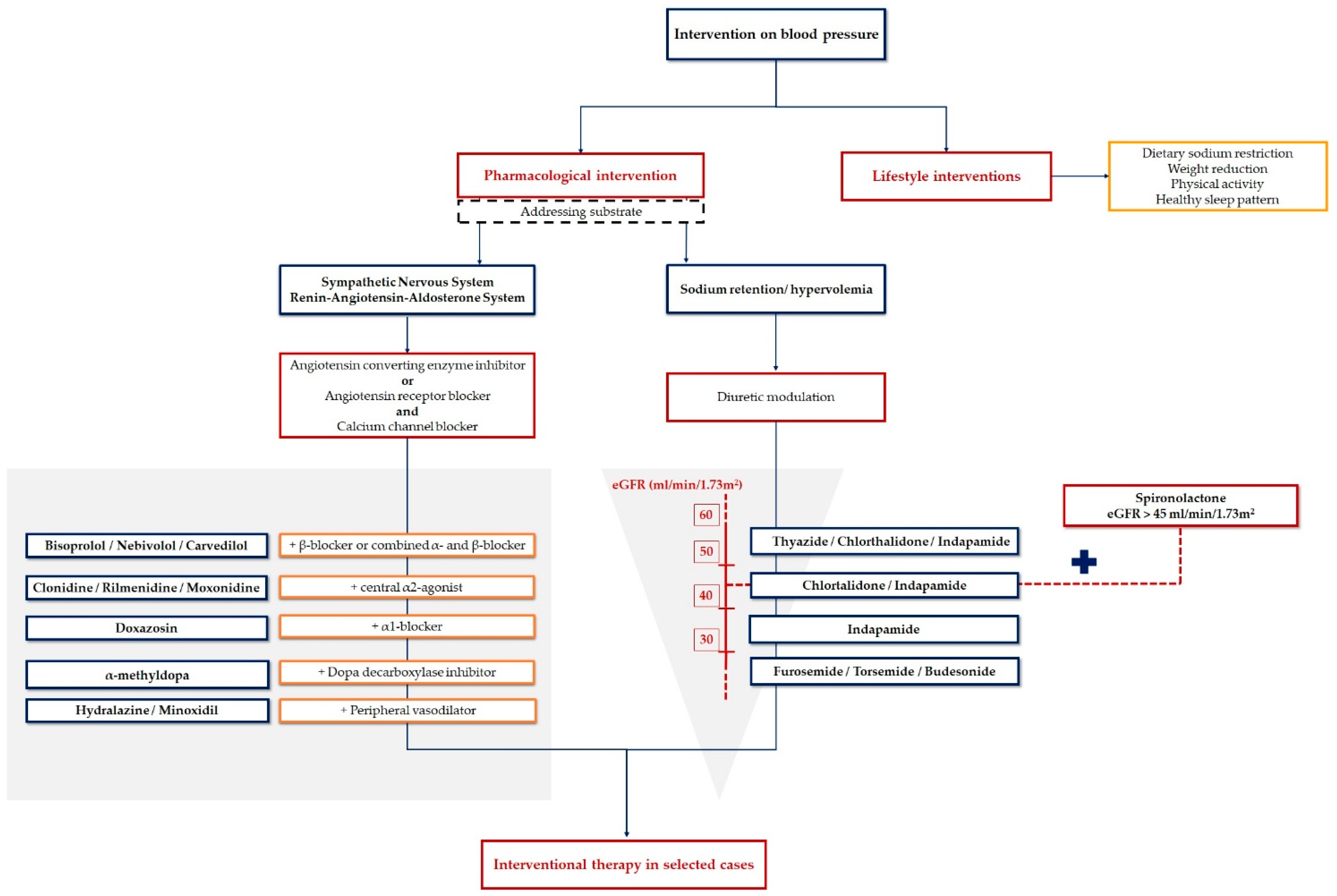
5. Therapeutic Approach of Resistant Hypertension
5.1. Nonpharmacological Strategies
5.1.1. Weight Reduction
5.1.2. Dietary Sodium Restriction
5.1.3. The DASH Diet
5.1.4. Physical Activity
5.1.5. Other Risk Factors
5.1.6. Psychological Counseling
5.2. Pharmacological Strategies
5.2.1. Optimizing the Three-Drug Regimen
5.2.2. Optimizing the Diuretic Treatment
5.2.3. Adding a Mineralocorticoid Receptor Antagonist
5.2.4. Adding a β-Blocker or a Combined α- and β-Blocker
5.2.5. Adding an α1-Blocker or a Peripheral Vasodilator
5.3. Device-Based Therapy
5.3.1. Renal Sympathetic Denervation
5.3.2. Carotid Baroreceptor Activation Therapy
5.3.3. Central Arteriovenous Anastomosis
6. Looking into the Future
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- NCD Risk Factor Collaboration. Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [Green Version]
- Chow, C.K.; Teo, K.K.; Rangarajan, S.; Islam, S.; Gupta, R.; Avezum, A.; Bahonar, A.; Chifamba, J.; Dagenais, G.; Diaz, R.; et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 2013, 310, 959–968. [Google Scholar] [CrossRef] [Green Version]
- Frieden, T.R.; Jaffe, M.G. Saving 100 million lives by improving global treatment of hypertension and reducing cardiovascular disease risk factors. J. Clin. Hypertens. 2018, 20, 208–211. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESH/ESC Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; De Palma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar]
- Armario, P.; Calhoun, D.A.; Oliveras, A.; Blanch, P.; Vinyoles, E.; Banegas, J.R.; Gorostidi, M.; Segura, J.; Ruilope, L.M.; Dudenbostel, T.; et al. Prevalence and clinical characteristics of refractory hypertension. J. Am. Heart Assoc. 2017, 6, e007365. [Google Scholar] [CrossRef] [Green Version]
- Calhoun, D.A.; Booth, J.N.; Oparil, S.; Irvin, M.R.; Shimbo, D.; Lackland, D.T.; Howard, G.; Safford, M.M.; Muntner, P. Refractory hypertension: Determination of prevalence, risk factors, and comorbidities in a large, population-based cohort. Hypertens. Dallas Tex. 1979 2014, 63, 451–458. [Google Scholar] [CrossRef] [Green Version]
- Banegas, J.R.; Ruilope, L.M.; de la Sierra, A.; de la Cruz, J.J.; Gorostidi, M.; Segura, J.; Martell, N.; Garcia-Puig, J.; Deanfield, J.; Williams, B. High prevalence of masked uncontrolled hypertension in people with treated hypertension. Eur. Heart J. 2014, 35, 3304–3312. [Google Scholar] [CrossRef] [Green Version]
- Banegas, J.R.; Ruilope, L.M.; de la Sierra, A.; Vinyoles, E.; Gorostidi, M.; de la Cruz, J.J.; Ruiz-Hurtado, G.; Segura, J.; Rodriguez-Artalejo, F.; Williams, B. Relationship between clinic and ambulatory blood-pressure measurements and mortality. N. Engl. J. Med. 2018, 378, 1509–1520. [Google Scholar] [CrossRef]
- Capelli, I.; Gasperoni, L.; Ruggeri, M.; Donati, G.; Baraldi, O.; Sorrenti, G.; Caletti, M.T.; Aiello, V.; Cianciolo, G.; La Manna, G. New mineralocorticoid receptor antagonists: Update on their use in chronic kidney disease and heart failure. J. Nephrol. 2020, 33, 37–48. [Google Scholar] [CrossRef]
- McCurley, A.; Jaffe, I.Z. Mineralocorticoid receptors in vascular function and disease. Mol. Cell Endocrinol. 2012, 350, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Jaffe, I.Z.; Mendelsohn, M.E. Angiotensin II and aldosterone regulate gene transcription via functional mineralocortocoid receptors in human coronary artery smooth muscle cells. Circ. Res. 2005, 96, 643–650. [Google Scholar] [CrossRef] [Green Version]
- Sowers, J.R.; Whaley-Connell, A.; Epstein, M. Narrative review: The emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann. Intern. Med. 2009, 150, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, L.A.; Moscato, T.S.; Pisanti, N.; Marotta, T.; Krogh, V.; Capone, D.; Mancini, M. Is the sympathetic nervous system altered in children with familial history of arterial hypertension? Cardiology 1988, 75, 200–205. [Google Scholar] [CrossRef]
- Mancia, G.; Grassi, G. The Autonomic Nervous System and Hypertension. Circ. Res. 2014, 114, 1804–1814. [Google Scholar] [CrossRef] [Green Version]
- Grassi, G.; Mark, A.; Esler, M. The sympathetic nervous system alterations in human hypertension. Circ. Res. 2015, 116, 976–990. [Google Scholar] [CrossRef] [Green Version]
- Heagerty, A.M.; Withers, S.B.; Izzard, A.S.; Greenstein, A.S.; Aghamohammadzadeh, R. Small artery structure and function in hypertension. In Manual of Hypertension of the European Society of Hypertension, 2nd ed.; Mancia, G., Grassi, G., Redon, J., Eds.; CRC Press: London, UK, 2014; pp. 203–210. [Google Scholar]
- Seravalle, G.; Volpe, M.; Ganz, F.; Magni, L.; Brambilla, G.; Dell’Oro, R.; Bombelli, M.; Mancia, G.; Grassi, G. Neuroadrenergic profile in patients with resistant hypertension. J. Hypertens. 2011, 29, e141. [Google Scholar]
- Ehret, G.B.; Munroe, P.B.; Rice, K.M.; Bochud, M.; Johnson, A.D.; Chasman, D.I.; Smith, A.M.; Tobin, M.D.; Verwoert, G.C.; Hwang, S.J.; et al. Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk. Nature 2011, 478, 103–109. [Google Scholar]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, R.; Zanchetti, A.; Bohm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension. Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar]
- Carey, R.M.; Calhoun, D.A.; Bakris, G.L.; Brook, R.D.; Daugherty, S.L.; Dennison-Himmelfarb, C.R.; Egan, B.M.; Flack, J.M.; Gidding, S.S.; Judd, E.; et al. Resistant Hypertension: Detection, Evaluation, and Management. A Scientific Statement From the American Heart Association. Hypertension 2018, 72, e53–e90. [Google Scholar] [CrossRef]
- Durand, H.; Hayes, P.; Morrissey, E.C.; Newell, J.; Casey, M.; Murphy, A.W.; Molloy, G.J. Medication adherence among patients with apparent treatment-resistant hypertension: Systematic review and meta-analysis. J. Hypertens. 2017, 35, 2346–2357. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.P.; Taylor, S.D. Factors affecting medication adherence in hypertensive patients. Ann. Pharmacother. 2002, 36, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Khan, H.; Heydon, E.; Shroufi, A.; Fahimi, A.; Moore, C.; Stricker, B.; Mendis, S.; Hofman, A.; Mant, J.; et al. Adherence to cardiovascular therapy: A meta-analysis of prevalence and clinical consequences. Eur. Heart J. 2013, 34, 2940–2948. [Google Scholar] [CrossRef] [Green Version]
- Culig, J.; Leppée, M. From Morisky to Hill-Bone; Self-Reports Scales for Measuring Adherence to Medication. Coll. Antropol. 2014, 38, 55–62. [Google Scholar]
- Hartman, L.; Lems, W.F.L.; Boers, M. Outcome measures for adherence data from a medication event monitoring system: A literature review. J. Clin. Pharm. Ther. 2019, 44, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Hiu, Y.K. “Globesity” Epidemic. Ann. Obes. Disord. 2016, 1, 1007. [Google Scholar]
- Vague, J. The degree of masculine differentiation of obesities: A factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. Am. J. Clin. Nutr. 1956, 4, 20–34. [Google Scholar] [CrossRef]
- Doll, S.; Paccaud, F.; Bovet, P.; Burnier, M.; Wietlisbach, V. Body mass index, abdominal adiposity and blood pressure: Consistency of their association across developing and developed countries. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Egan, B.M.; Zhao, Y.; Axon, R.N.; Brzezinski, W.A.; Ferdinand, K.C. Uncontrolled and apparent treatment resistant hypertension in the United States, 1988–2008. Circulation 2011, 124, 1046–1058. [Google Scholar] [CrossRef] [Green Version]
- Aucott, L.; Poobalan, A.; Smith, W.C.; Avenell, A.; Jung, R.; Broom, J. Effects of weight loss in overweight/obese individuals and long-term hypertension outcomes: A systematic review. Hypertension 2005, 45, 1035–1041. [Google Scholar] [CrossRef] [Green Version]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [Green Version]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. DASH-Sodium Collaborative Research Group. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Comelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar]
- Lopes, S.; Mesquita-Bastos, J.; Alves, A.J.; Ribeiro, F. Exercise as a tool for hypertension and resistant hypertension management: Current insights. Integr. Blood Press. Control. 2018, 11, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Mena-Martin, F.J.; Martin-Escudero, J.C.; Simal-Blanco, F.; Carretero-Ares, J.L.; Arzua-Mouronte, D.; Herreros-Fernandez, V. Health-related quality of life of subjects with known and unknown hypertension: Results from the population-based Hortega study. J. Hypertens. 2003, 21, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Chen, D.; Yang, Y.; Zheng, Y.; Hui, R. Depression increases the risk of hypertension incidence: A meta-analysis of prospective cohort studies. J. Hypertens. 2012, 30, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Gilsanz, P.; Walter, S.; Tchetgen, E.J.T.; Patton, K.K.; Moon, J.R.; Capistrant, B.D.; Marden, J.R.; Kubzansky, L.D.; Kawachi, I.; Glymour, M.M. Changes in Depressive Symptoms and Incidence of First Stroke Among Middle-Aged and Older US Adults. J. Am. Heart Assoc. 2015, 4, e001923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.K.; Arshad, S.; Poulter, N.R. Compliance, safety, and effectiveness of fixed-dose combinations of antihypertensive agents: A meta-analysis. Hypertension 2010, 55, 399–407. [Google Scholar] [CrossRef] [Green Version]
- Roush, G.C.; Ernst, M.E.; Kostis, J.B.; Tandon, S.; Sica, D.A. Head-to-Head Comparisons of Hydrochlorothiazide with Indapamide and Chlorthalidone. Hypertension 2015, 65, 1041–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorsch, M.P.; Gillespie, B.W.; Erickson, S.R.; Bleske, B.E.; Weder, A.B. Chlorthalidone reduces cardiovascular events compared with hydrochlorothiazide: A retrospective cohort analysis. Hypertension 2011, 57, 689–694. [Google Scholar] [CrossRef]
- Ernst, M.E.; Neaton, J.D.; Grimm, R.H.; Collins, G.; Thomas, W.; Soliman, E.Z.; Prineas, R.J.; Multiple Risk Factor Intervention Trial Research Group. Long-term effects of chlorthalidone versus hydrochlorothiazide on electrocardiographic left ventricular hypertrophy in the multiple risk factor intervention trial. Hypertension 2011, 58, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Malha, L.; Mann, S.J. Loop Diuretics in the Treatment of Hypertension. Curr. Hypertens. Rep. 2016, 18, 27. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; MacDonald, T.M.; Morant, S.; Webb, D.J.; Sever, P.; McInnes, G.; Ford, I.; Cruickshank, J.K.; Caulfield, M.J.; Salsbury, J.; et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): A randomised, double-blind, crossover trial. Lancet 2015, 386, 2059–2068. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, R.; Rossignol, P.; Romero, A.; Garza, D.; Mayo, M.R.; Warren, S.; Ma, J.; White, W.B.; Williams, B. Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease (AMBER): A phase 2, randomised, double-blind, placebo-controlled trial. Lancet 2019, 394, 1540–1550. [Google Scholar] [CrossRef]
- Williams, B.; MacDonald, T.M.; Morant, S.V.; Webb, D.J.; Sever, P.; McInnes, G.T.; Ford, I.; Cruickshank, J.K.; Caulfield, M.J.; Padmanabhan, S.; et al. Endocrine and haemodynamic changes in resistant hypertension, and blood pressure responses to spironolactone or amiloride: The PATHWAY-2 mechanisms substudies. Lancet Diabetes Endocrinol. 2018, 6, 464–475. [Google Scholar] [CrossRef] [Green Version]
- Warnock, D.G.; Kusche-Vihrog, K.; Tarjus, A.; Sheng, S.; Oberleithner, H.; Kleyman, T.R.; Jaisser, F. Blood pressure and amiloride-sensitive sodium channels in vascular and renal cells. Nat. Rev. Nephrol. 2014, 10, 146–157. [Google Scholar] [CrossRef] [Green Version]
- Manolis, A.A.; Manolis, T.A.; Melita, H.; Manolis, A.S. Eplerenone Versus Spironolactone in Resistant Hypertension: An Efficacy and/or Cost or Just a Men’s Issue? Curr. Hypertens. Rep. 2019, 21, 22. [Google Scholar] [CrossRef]
- Fujimura, A.; Ebihara, A.; Ohashi, K.; Shiga, T.; Kumagai, Y.; Nakashima, H.; Kotegawa, T. Comparison of the pharmacokinetics, pharmacodynamics, and safety of oral (Catapres) and transdermal (M-5041T) clonidine in healthy subjects. J. Clin. Pharmacol. 1994, 34, 260–265. [Google Scholar] [CrossRef]
- Krieger, E.M.; Drage, L.F.; Giorgi, D.M.A.; Pereira, A.C.; Barreto-Filho, J.A.S.; Nogueira, A.R.; Mill, J.G.; Lotufo, P.A.; Amodeo, C.; Batista, M.C.; et al. Spironolactone versus clonidine as a fourth-drug therapy for resistant hypertension: The ReHOT randomized study (Resistant Hypertension Optimal Treatment). Hypertension 2018, 71, 681–690. [Google Scholar] [CrossRef]
- Opie, L.H. Calcium Channel Blockers. In Drugs for the Heart, 8th ed.; Opie, L.H., Gersh, B., Eds.; Saunders: Philadelphia, PA, USA, 2013; pp. 72–93. [Google Scholar]
- Opie, L.H.; Krum, H.; Victor, R.G.; Kaplan, N.M. Antihypertensive Therapies. In Drugs for the Heart, 8th ed.; Opie, L.H., Gersh, B., Eds.; Saunders: Philadelphia, PA, USA, 2013; pp. 224–271. [Google Scholar]
- Sica, D.A. Minoxidil: An underused vasodilator for resistant or severe hypertension. J. Clin. Hypertens. 2004, 6, 283–287. [Google Scholar] [CrossRef] [Green Version]
- Krum, H.; Schlaich, M.; Whitbourn, R.; Sobotka, P.A.; Sadowski, J.; Bartus, K.; Kapelak, B.; Walton, A.; Sievert, H.; Thambar, S.; et al. Catheter-based renal sympathetic denervation for resistant hypertension: A multicentre safety and proof-of-principle cohort study. Lancet 2009, 373, 1275–1281. [Google Scholar] [CrossRef]
- Esler, M.D.; Krum, H.; Sobotka, P.A.; Schlaich, M.P.; Schmieder, R.E.; Böhm, M. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): A randomized controlled trial. Lancet 2010, 376, 1903–1909. [Google Scholar] [PubMed]
- Bhatt, D.L.; Kandzari, D.E.; O’Neill, W.W.; D’Agostino, R.; Flack, J.M.; Katzen, B.T.; Leon, M.B.; Liu, M.; Mauri, L.; Negoita, M.; et al. A controlled trial of renal denervation for resistant hypertension. N. Engl. J. Med. 2014, 370, 1393–1401. [Google Scholar] [CrossRef] [Green Version]
- Azizi, M.; Sapoval, M.; Gosse, P.; Monge, M.; Bobrie, G.; Delsart, P.; Midulla, M.; Mounier-Véhier, C.; Courand, P.Y.; Lantelme, P.; et al. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN): A multicentre, open-label, randomised controlled trial. Lancet 2015, 385, 1957–1965. [Google Scholar] [CrossRef]
- Townsend, R.R.; Mahfoud, F.; Kandzari, D.E.; Kario, K.; Pocock, S.; Weber, M.A.; Ewen, S.; Tsioufis, K.; Tousoulis, D.; Sharp, A.S.P.; et al. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): A randomised, sham-controlled, proof-of-concept trial. Lancet 2017, 390, 2160–2170. [Google Scholar] [CrossRef]
- Mabin, T.; Sapoval, M.; Cabane, V.; Stemmett, J.; Iyer, M. First experience with endovascular ultrasound renal denervation for the treatment of resistant hypertension. EuroIntervention 2012, 8, 57–61. [Google Scholar] [CrossRef]
- Bisognano, J.D.; Bakris, G.; Nadim, M.K.; Sanchez, L.; Kroon, A.A.; Schafer, J.; de Leeuw, P.W.; Sica, D.A. Baroreflex activation therapy lowers blood pressure in patients with resistant hypertension: Results from the double-blind, randomized, placebo-controlled rheos pivotal trial. J. Am. Coll. Cardiol. 2011, 58, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Faul, J.; Schoors, D.; Brouwers, S.; Scott, B.; Jerrentrup, A.; Galvin, J.; Luitjens, S.; Dolan, E. Creation of an iliac arteriovenous shunt lowers blood pressure in chronic obstructive pulmonary disease patients with hypertension. J. Vasc. Surg. 2014, 59, 1078–1083. [Google Scholar] [CrossRef] [Green Version]
- Kostis, J.B.; Packer, M.; Black, H.R.; Schmieder, R.; Henry, D.; Levy, E. Omapatrilat and enalapril in patients with hypertension: The Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am. J. Hypertens. 2004, 17, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.M.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Geng, Q.; Yan, R.; Wang, Z.; Hou, F. Effects of LCZ696 (Sacubitril/Valsartan) on Blood Pressure in Patients with Hypertension: A Meta-Analysis of Randomized Controlled Trials. Cardiology 2020, 145, 589–598. [Google Scholar] [CrossRef]
- Pitt, B.; Kober, L.; Ponikowski, P.; Gheorghiade, M.; Filippatos, G.; Krum, H.; Nowack, C.; Kolkhof, P.; Kim, S.Y.; Zannad, F. Safety and tolerability of the novel non-steroidal mineralocorticoid receptor antagonist BAY 94-8862 in patients with chronic heart failure and mild or moderate chronic kidney disease: A randomized, double-blind trial. Eur. Heart J. 2013, 34, 2453–2463. [Google Scholar] [CrossRef] [PubMed]
- Lattenist, L.; Lechner, S.M.; Messaoudi, S.; Le Mercier, A.; El Moghrabi, S.; Prince, S.; Bobadilla, N.A.; Kolkhof, P.; Jaisser, F.; Barrera-Chimal, J. Nonsteroidal mineralocorticoid receptor antagonist finerenone protects against acute kidney injury mediated chronic kidney disease: Role of oxidative stress. Hypertension 2017, 69, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Marc, Y.; Llorens-Cortes, C. The role of the brain renin-angiotensin system in hypertension: Implications for new treatment. Prog. Neurobiol. 2011, 95, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Keck, M.; Hmazzou, R.; Llorens-Cortes, C. Orally active aminopeptidase a inhibitor prodrugs: Current state and future directions. Curr. Hypertens. Rep. 2019, 21, 50. [Google Scholar] [CrossRef]
- Marc, Y.; Gao, J.; Balavoine, F.; Michaud, A.; Roques, B.P.; Llorens-Cortes, C. Central antihypertensive effects of orally active aminopeptidase A inhibitors in spontaneously hypertensive rats. Hypertension 2012, 60, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Marc, Y.; Hmazzou, R.; Balavoine, F.; Flahault, A.; Llorens-Cortes, C. Central antihypertensive effects of chronic treatment with RB150: An orally active aminopeptidase A inhibitor in deoxycorticosterone acetate-salt rats. J. Hypertens. 2018, 36, 641–650. [Google Scholar] [CrossRef]
- Ferdinand, K.C.; Balavoine, F.; Besse, B.; Black, H.R.; Desbrandes, S.; Dittrich, H.C.; Nesbitt, S.D. Efficacy and safety of firibastat, a first-inclass brain aminopeptidase a inhibitor, in hypertensive overweight patients of multiple ethnic origins. A phase 2, open-label, multicenter, dose-titrating study. Circulation 2019, 140, 138–146. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bădilă, E.; Japie, C.; Weiss, E.; Balahura, A.-M.; Bartoș, D.; Scafa Udriște, A. The Road to Better Management in Resistant Hypertension—Diagnostic and Therapeutic Insights. Pharmaceutics 2021, 13, 714. https://doi.org/10.3390/pharmaceutics13050714
Bădilă E, Japie C, Weiss E, Balahura A-M, Bartoș D, Scafa Udriște A. The Road to Better Management in Resistant Hypertension—Diagnostic and Therapeutic Insights. Pharmaceutics. 2021; 13(5):714. https://doi.org/10.3390/pharmaceutics13050714
Chicago/Turabian StyleBădilă, Elisabeta, Cristina Japie, Emma Weiss, Ana-Maria Balahura, Daniela Bartoș, and Alexandru Scafa Udriște. 2021. "The Road to Better Management in Resistant Hypertension—Diagnostic and Therapeutic Insights" Pharmaceutics 13, no. 5: 714. https://doi.org/10.3390/pharmaceutics13050714
APA StyleBădilă, E., Japie, C., Weiss, E., Balahura, A. -M., Bartoș, D., & Scafa Udriște, A. (2021). The Road to Better Management in Resistant Hypertension—Diagnostic and Therapeutic Insights. Pharmaceutics, 13(5), 714. https://doi.org/10.3390/pharmaceutics13050714