
Translational Studies on the Potential of a VEGF Nanoparticle-Loaded Hyaluronic Acid Hydrogel

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
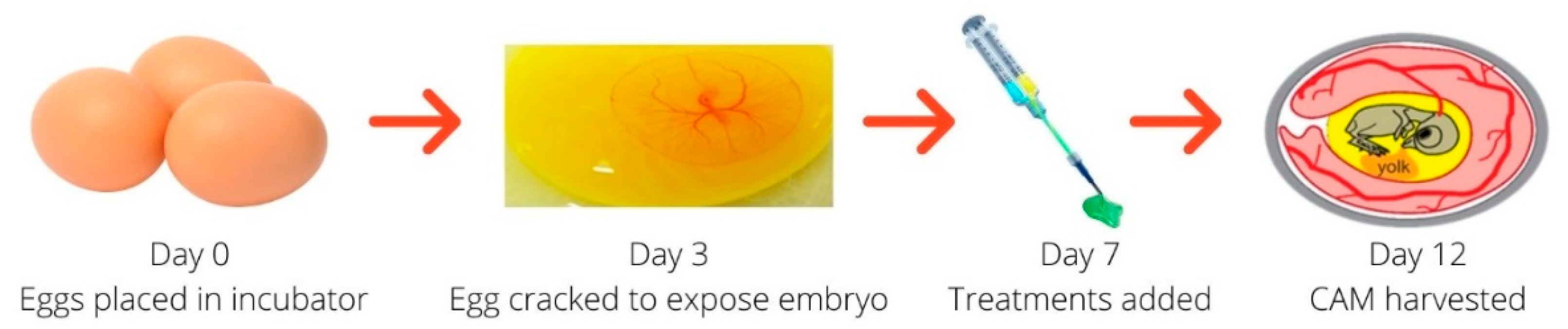
2.2. Biocompatibility and Bioactivity of Nano-VEGF-HA-TA in an In Vivo CAM Model
2.2.1. Incubation of Eggs for CAM Study
2.2.2. Addition of Treatments to the CAM Membrane
2.2.3. Investigation of Angiogenesis Induced on the CAM Model
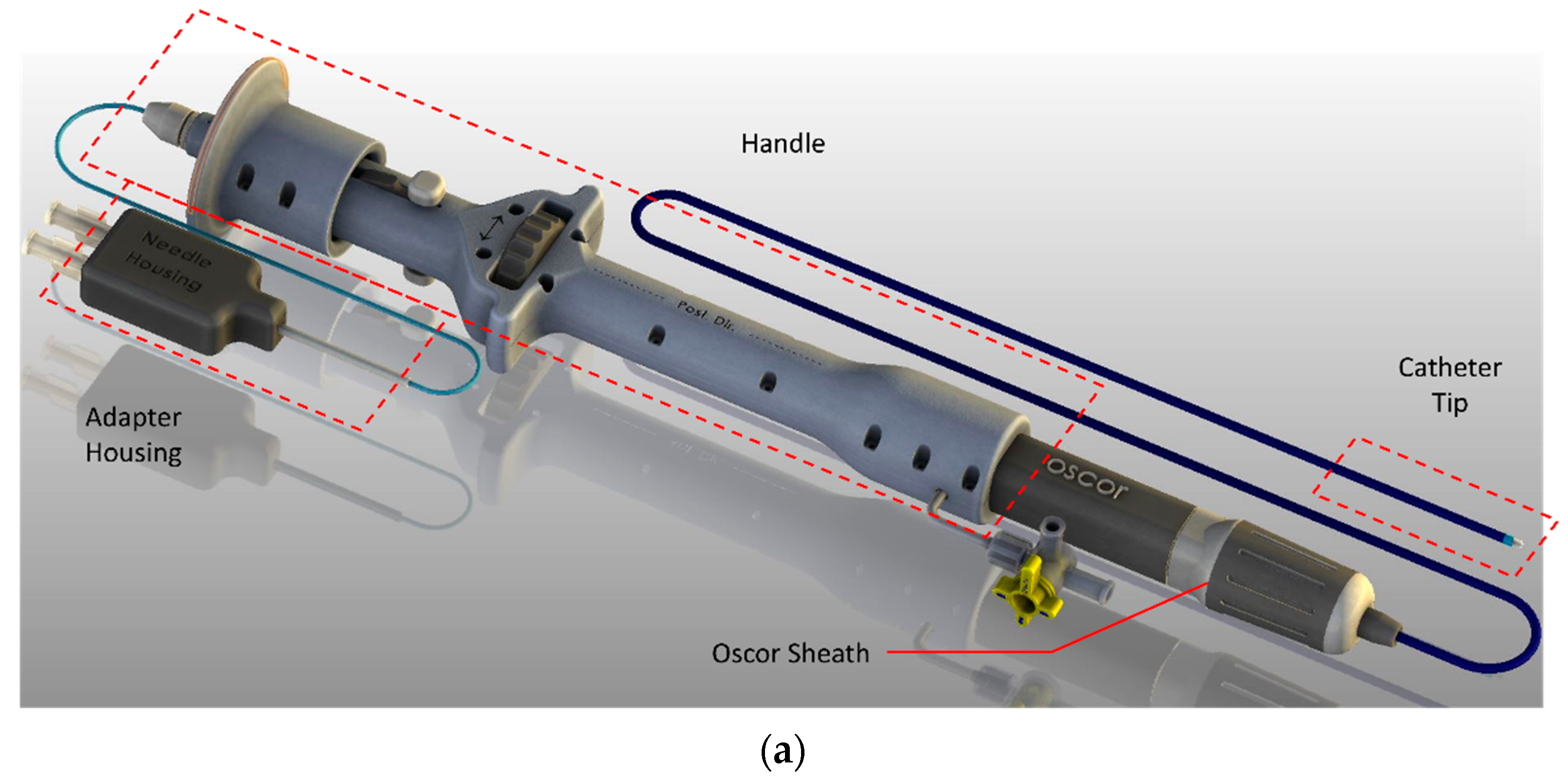
2.3. Injection of Nano-VEGF-HA-TA through a Prototype AMCath Catheter
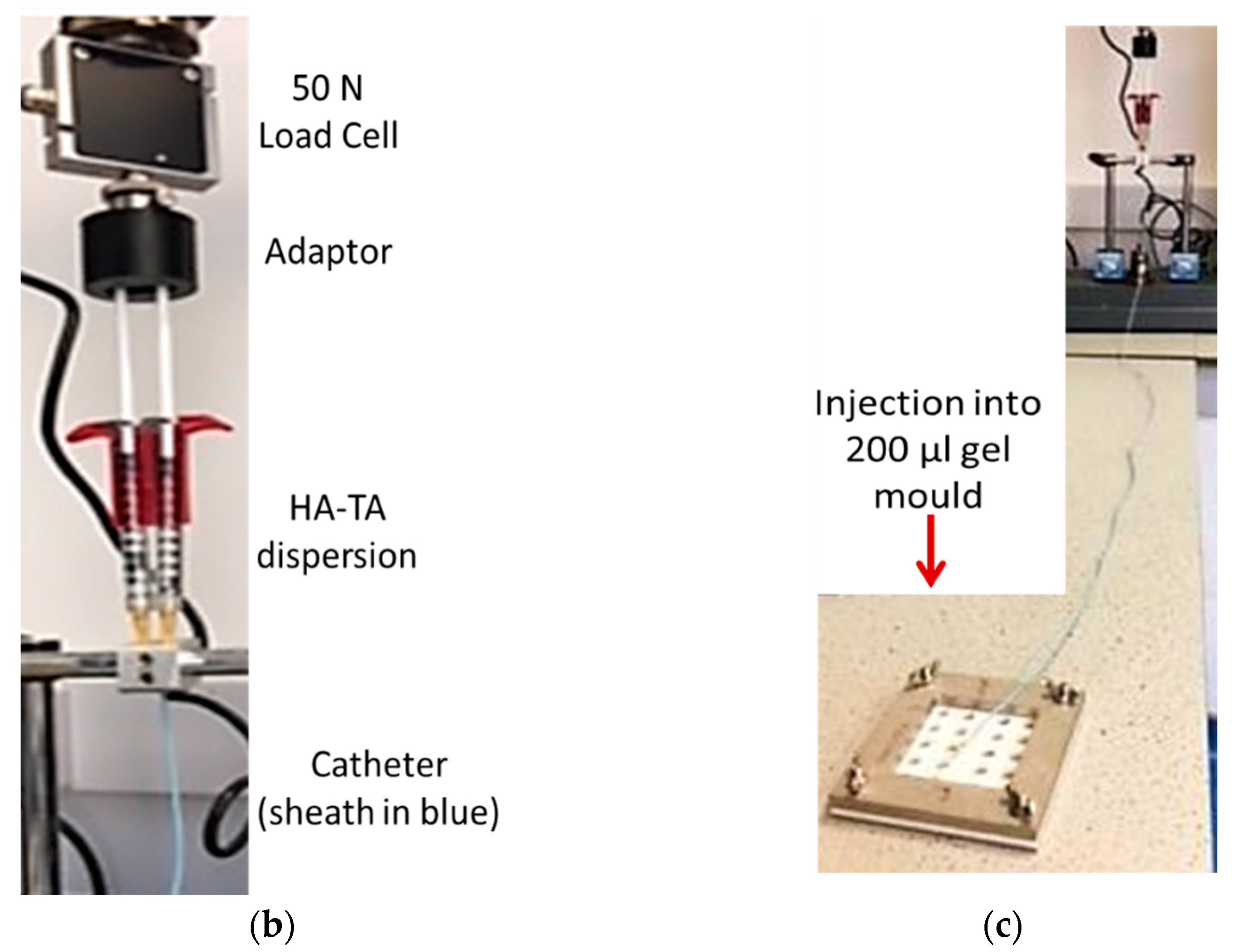
2.4. Injection of Nano-VEGF-HA-TA through the AMCath Catheter with an Automated Injection System
2.4.1. Mechanical Testing and VEGF Release of Catheter-Injected Nano-VEGF-HA-TA
2.4.2. VEGF Release from Catheter-Injected Nano-VEGF-HA-TA
2.4.3. Biocompatibility and Bioactivity of Released VEGF
Biocompatibility
Bioactivity—Matrigel® Assay
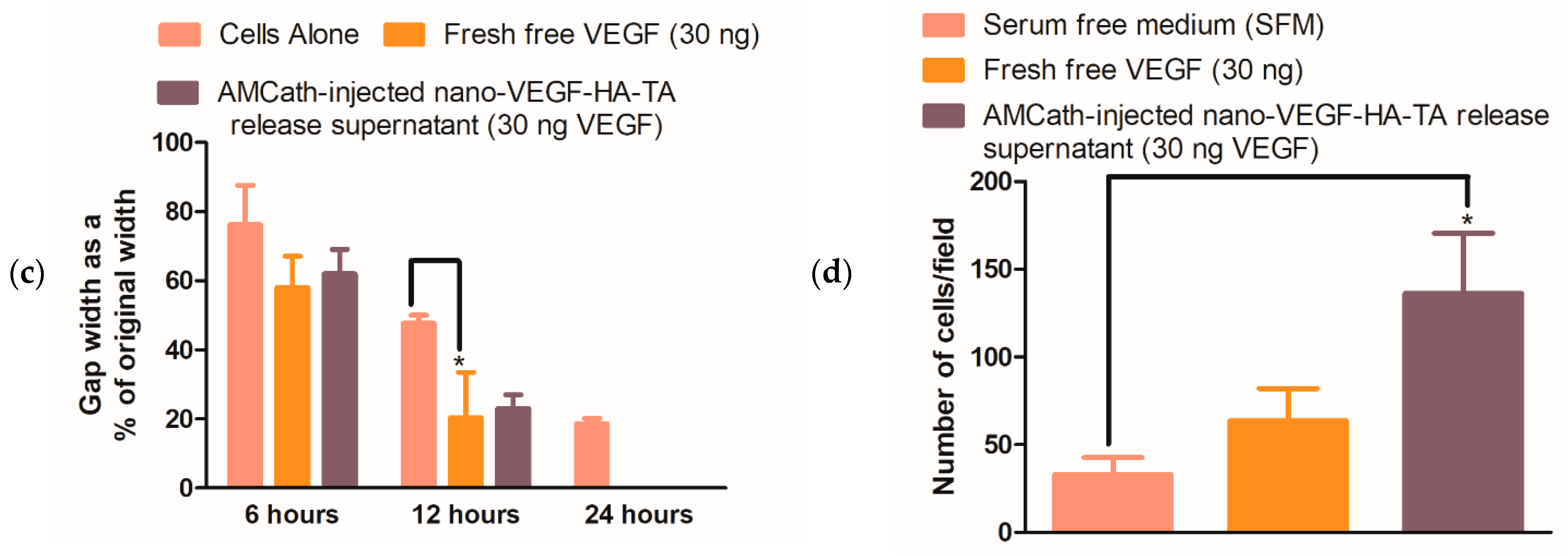
Bioactivity—Scratch Assay
Bioactivity—Transwell® Migration
2.5. Statistical Analysis
3. Results
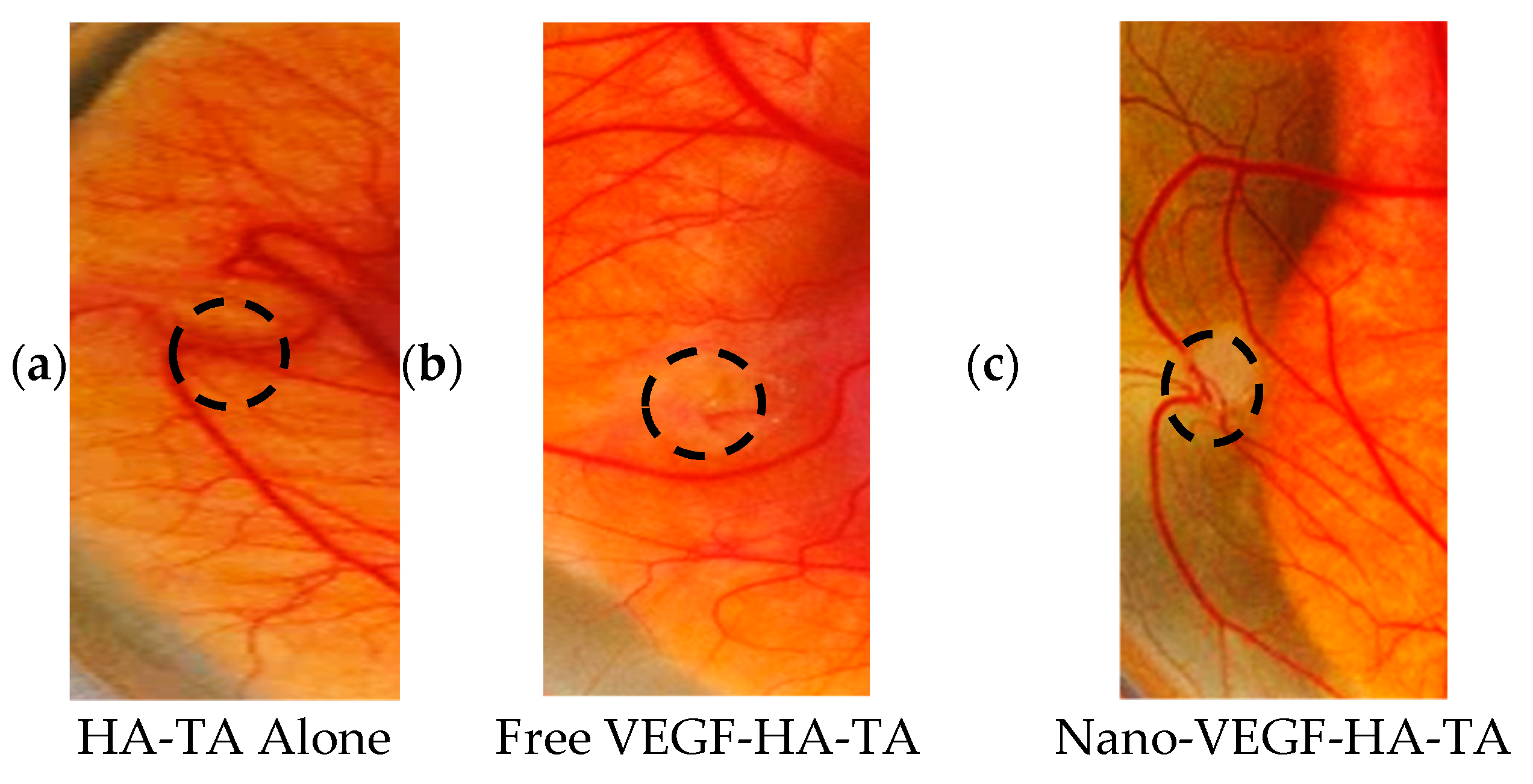
3.1. In Vivo Testing of Nano-VEGF-HA-TA Hydrogels in a CAM Model
3.1.1. Clinical Observation of Chick Embryos
3.1.2. Integrity of CAM Vasculature Post-Treatment
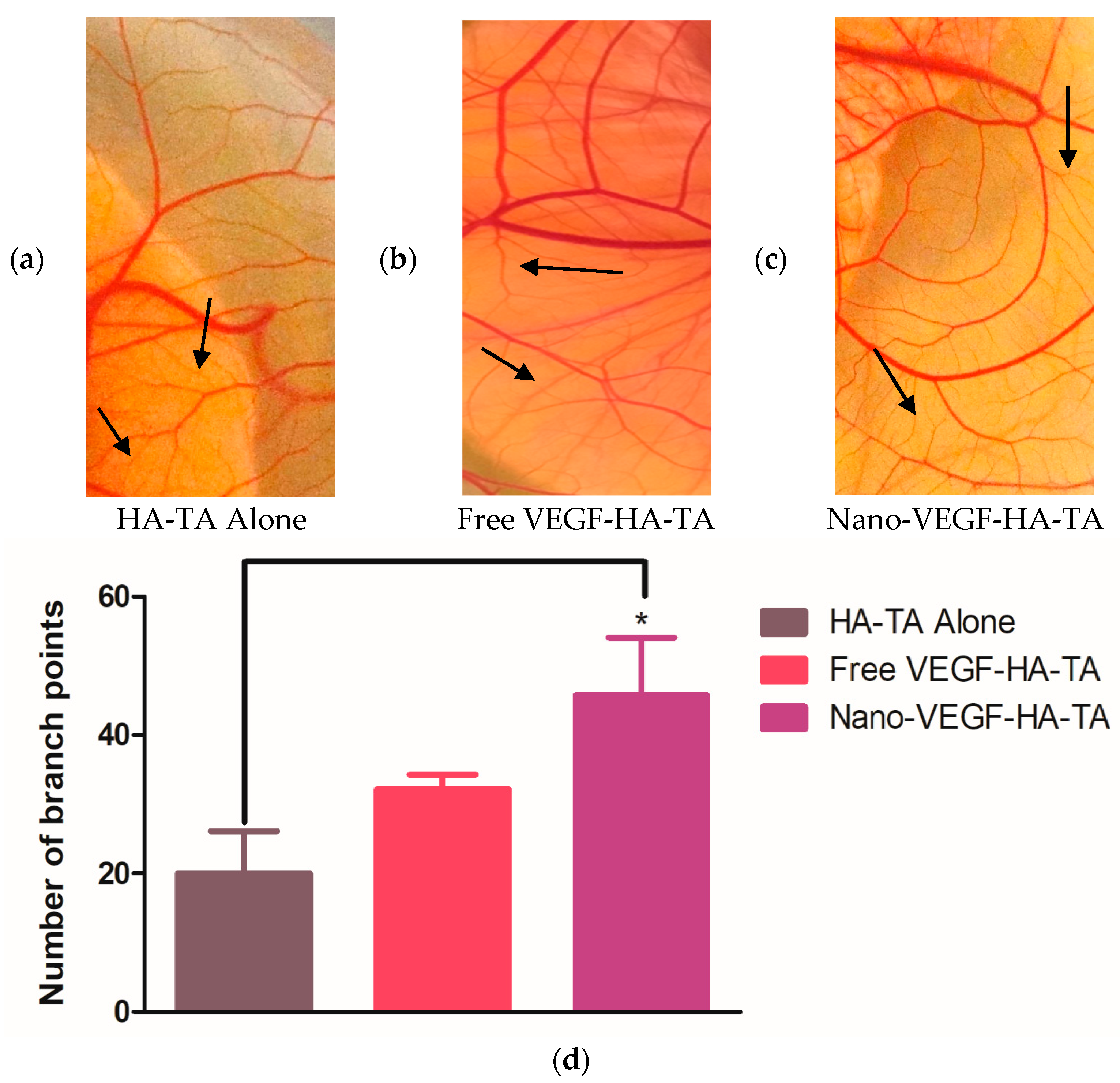
3.1.3. Angiogenic Effects of Nano-VEGF-HA-TA—Vessel Branching
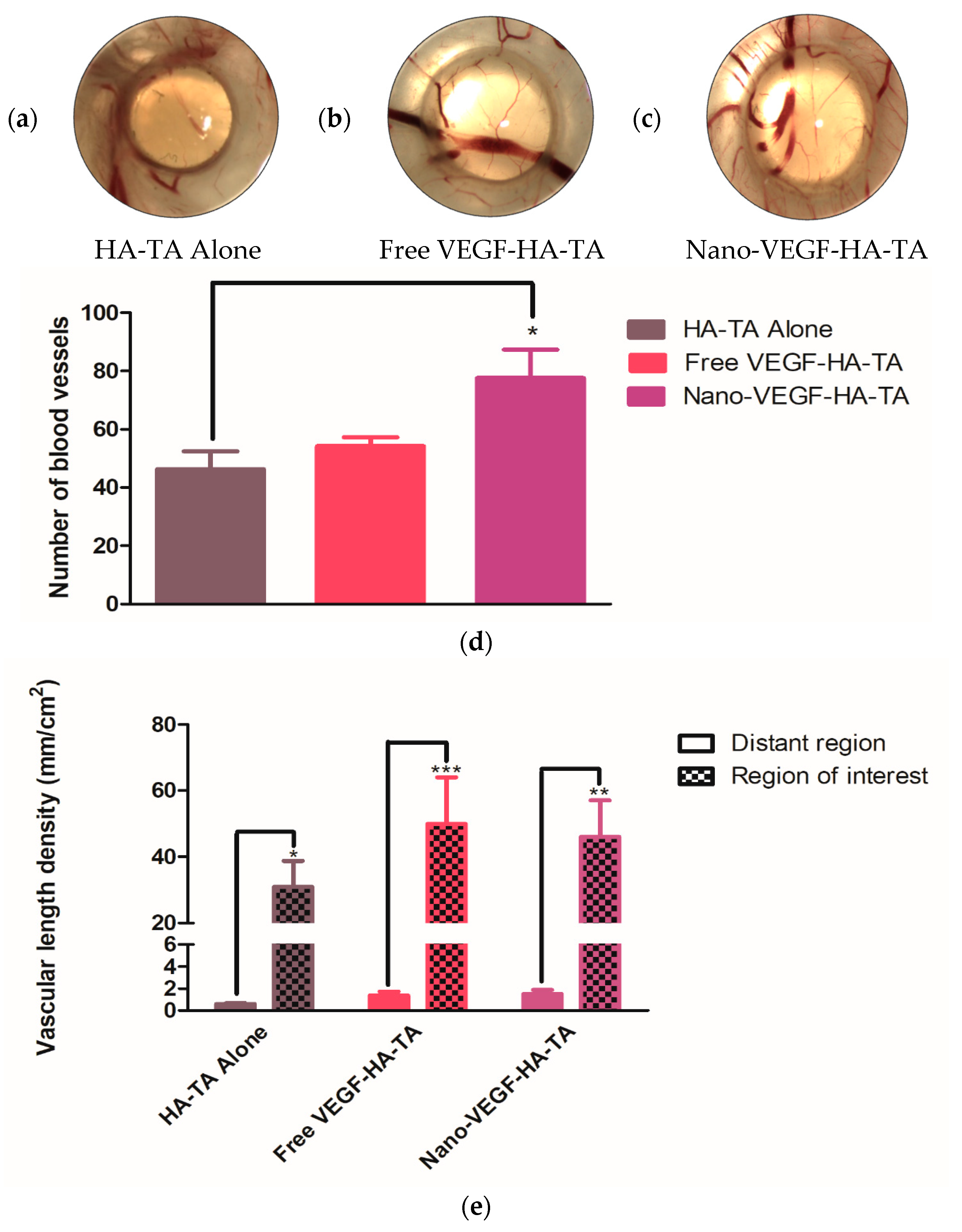
3.1.4. Angiogenic Effects of Nano-VEGF-HA-TA—Quantification of Vessel Formation
3.2. Injection of Nano-VEGF-HA-TA through the AMCath Catheter
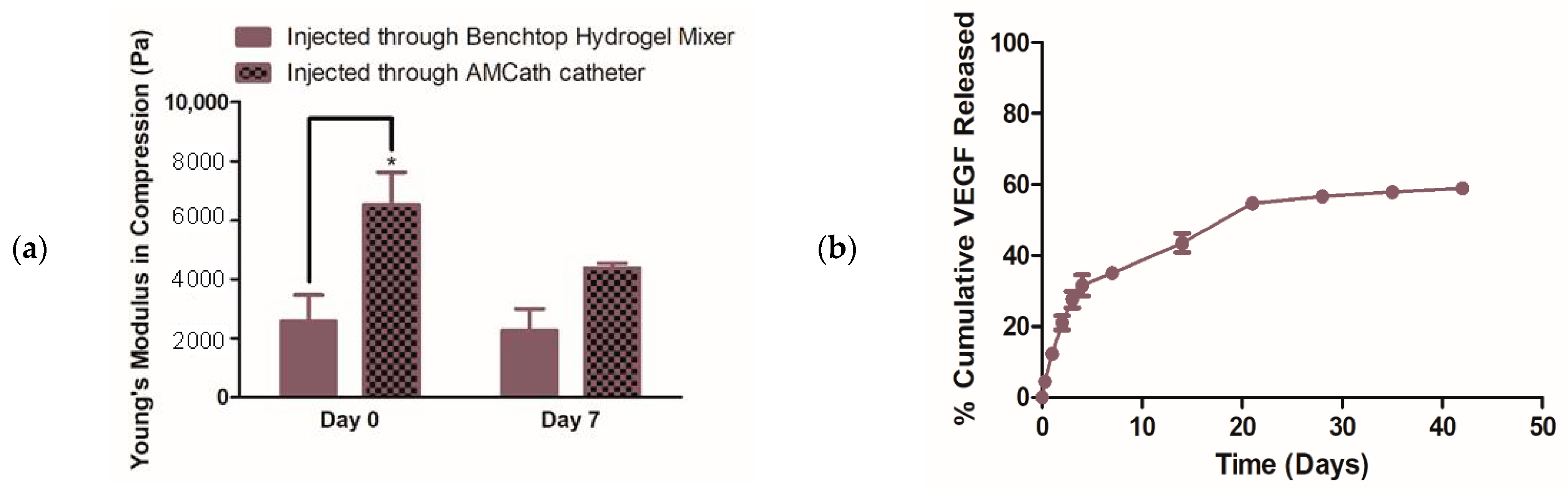
3.2.1. Mechanical Testing and VEGF Release from Nano-VEGF- HA-TA Gels after Injection through the AMCath Catheter
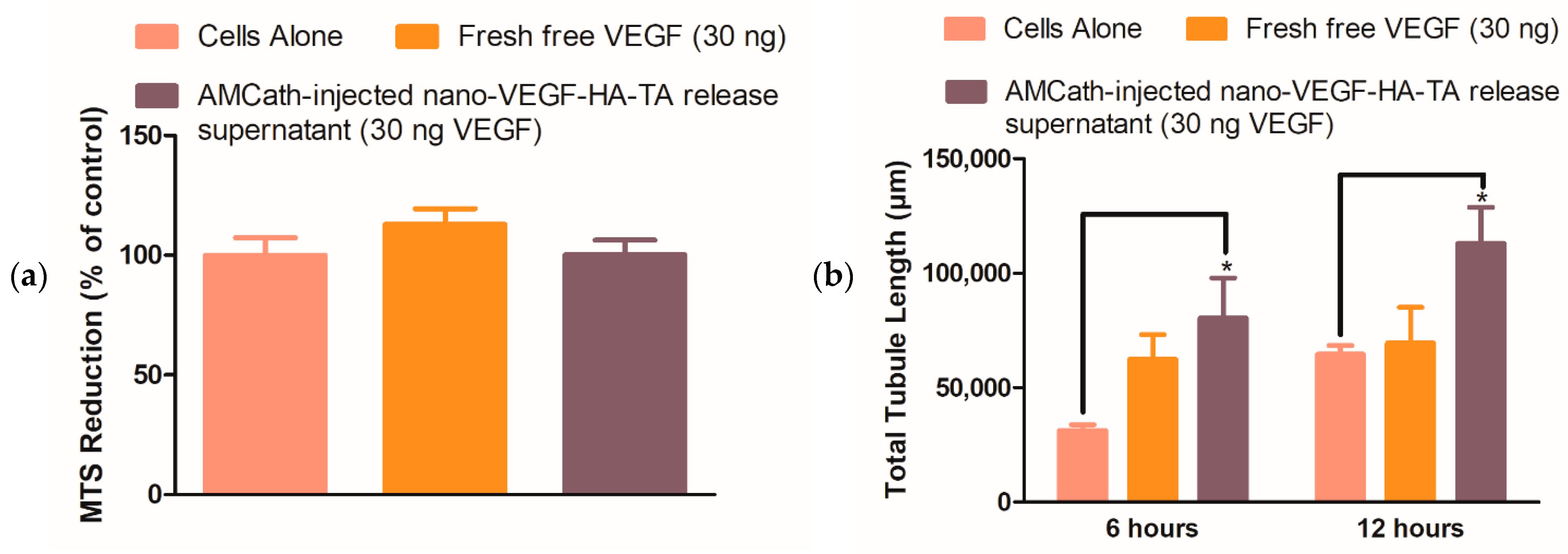
3.2.2. Formulation, Biocompatibility and Bioactivity Post-Injection through AMCath—Metabolic Activity, Matrigel®, Scratch and Transwell® Migration Assays
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stewart, S.; MacIntyre, K.; Hole, D.; Capewell, S.; McMurray, J.J.V. More ‘malignant’ than cancer? Five-year survival following a first admission for heart failure. Eur. J. Heart Fail. 2001, 3, 315–322. [Google Scholar] [CrossRef]
- Levy, D.; Kenchaiah, S.; Larson, M.G.; Benjamin, E.J.; Kupka, M.J.; Ho, K.K.; Murabito, J.M.; Vasan, R.S. Long-Term Trends in the Incidence of and Survival with Heart Failure. N. Engl. J. Med. 2002, 347, 1397–1402. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence. Chronic Heart Failure. In National Clinical Guideline for Diagnosis and Management in Primary and Secondary Care; Royal College of Physicians: London, UK, 2010. [Google Scholar]
- Kemp, C.D.; Conte, J.V. The pathophysiology of heart failure. Cardiovasc. Pathol. 2012, 21, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Rouleau, J.L. New and Emerging Drugs and Device Therapies for Chronic Heart Failure in Patients with Systolic Ventricular Dysfunction. Can. J. Cardiol. 2011, 27, 296–301. [Google Scholar] [CrossRef]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar]
- Taylor, C.J.; Ryan, R.; Nichols, L.; Gale, N.; Hobbs, F.D.R.; Marshall, T. Survival following a diagnosis of heart failure in primary care. Fam. Pract. 2017, 34, 161–168. [Google Scholar] [CrossRef]
- Segers, V.F.M.; Lee, R.T. Protein Therapeutics for Cardiac Regeneration after Myocardial Infarction. J. Cardiovasc. Transl. Res. 2010, 3, 469–477. [Google Scholar] [CrossRef] [Green Version]
- Liau, B.; Zhang, D.; Bursac, N. Functional cardiac tissue engineering. Regen. Med. 2012, 7, 187–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D. ESC/ACCF/AHA/WHF Expert Consensus Document Third Universal Definition of Myocardial Infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevationThe Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Ertl, G.; Frantz, S. Healing after myocardial infarction. Cardiovasc. Res. 2005, 66, 22–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.M.; Mann, D.L. In Search of New Therapeutic Targets and Strategies for Heart Failure: Recent Advances in Basic Science. Lancet 2011, 378, 704–712. [Google Scholar] [CrossRef] [Green Version]
- Cochain, C.; Channon, K.M.; Silvestre, J.-S. Angiogenesis in the Infarcted Myocardium. Antioxid. Redox Signal. 2013, 18, 1100–1113. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, G.; Cohen, T.; Gengrinovitch, G.; Poltorak, Z. Vascular endothelial growth factor (VEGF) and its receptors. Off. J. Fed. Am. Soc. Exp. Biol. 1999, 13, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Simon-Yarza, T.; Formiga, F.R.; Tamayo, E.; Pelacho, B.; Prosper, F.; Blanco-Prieto, M.J. Vascular endothelial growth factor-delivery systems for cardiac repair: An overview. Theranostics 2012, 2, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Hendel, R.C.; Henry, T.D.; Rocha-Singh, K.; Isner, J.M.; Kereiakes, D.J.; Giordano, F.J.; Simons, M.; Bonow, R.O. Effect of Intracoronary Recombinant Human Vascular Endothelial Growth Factor on Myocardial Perfusion. Circulation 2000, 101, 118–121. [Google Scholar] [CrossRef] [Green Version]
- Henry, T.D.; Annex, B.H.; McKENDALL, G.R.; Azrin, M.A.; Lopez, J.J.; Giordano, F.J.; Shah, P.; Willerson, J.T.; Benza, R.L.; Berman, D.S.; et al. The VIVA Trial. Circulation 2003, 107, 1359–1365. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, J.; Murphy, R.; Dolan, E.B.; Kovarova, L.; Pravda, M.; Velebny, V.; Heise, A.; Duffy, G.P.; Cryan, S.A. Development of a nanomedicine-loaded hydrogel for sustained delivery of an angiogenic growth factor to the ischaemic myocardium. Drug Deliv. Transl. Res. 2020, 10, 440–454. [Google Scholar] [CrossRef]
- Nowak-Sliwinska, P.; Alitalo, K.; Allen, E.; Anisimov, A.; Aplin, A.C.; Auerbach, R.; Augustin, H.G.; Bates, D.O.; Van Beijnum, J.R.; Bender, R.H.F.; et al. Consensus guidelines for the use and interpretation of angiogenesis assays. Angiogenesis 2018, 21, 425–532. [Google Scholar] [CrossRef] [Green Version]
- Wells, D.J. Animal welfare and the 3Rs in European biomedical research. Ann. N. Y. Acad. Sci. 2011, 1245, 14–16. [Google Scholar] [CrossRef]
- Kue, C.S.; Tan, K.Y.; Lam, M.L.; Lee, H.B. Chick embryo chorioallantoic membrane (CAM): An alternative predictive model in acute toxicological studies for anti-cancer drugs. Exp. Anim. 2015, 64, 129–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, P.C.; Montgomery, A.M.P.; Cheresh, D.A. Use of the 10-Day-Old Chick Embryo Model for Studying Angiogenesis. In Integrin Protocols; Howlett, A., Ed.; Humana Press: Totowa, NJ, USA, 1999; pp. 257–269. [Google Scholar]
- Deryugina, E.I.; Quigley, J.P. Chick embryo chorioallantoic membrane model systems to study and visualize human tumor cell metastasis. Histochem. Cell Biol. 2008, 130, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Ribatti, D. The chick embryo chorioallantoic membrane (CAM). A multifaceted experimental model. Mech. Dev. 2016, 141, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, R.; Lewis, R.; Shinners, B.; Kubai, L.; Akhtar, N. Angiogenesis Assays: A Critical Overview. Clin. Chem. 2003, 49, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Staton, C.A.; Reed, M.; Brown, N.J. A critical analysis of current in vitro and in vivo angiogenesis assays. Int. J. Exp. Pathol. 2009, 90, 195–221. [Google Scholar] [CrossRef] [PubMed]
- Tahergorabi, Z.; Khazaei, M. A Review on Angiogenesis and Its Assays. Iran J. Basic Med. Sci. 2012, 15, 1110–1126. [Google Scholar] [PubMed]
- Banovic, M.; Ostojic, M.C.; Bartunek, J.; Nedeljkovic, M.; Beleslin, B.; Terzic, A. Brachial Approach to NOGA-Guided Procedures Electromechanical Mapping and Transendocardial Stem-Cell Injections. Texas Heart Inst. J. 2011, 38, 179–182. [Google Scholar]
- O’Dwyer, J.; Cullen, M.; Fattah, S.; Murphy, R.; Stefanovic, S.; Kovarova, L.; Pravda, M.; Velebny, V.; Heise, A.; Duffy, G.P.; et al. Development of a Sustained Release Nano-In-Gel Delivery System for the Chemotactic and Angiogenic Growth Factor Stromal-Derived Factor 1α. Pharmaceutics 2020, 12, 513. [Google Scholar] [CrossRef]
- Luo, J.; Redies, C. Ex ovo electroporation for gene transfer into older chicken embryos. Dev. Dyn. 2005, 233, 1470–1477. [Google Scholar] [CrossRef]
- do Amaral, R.J.F.C.; Zayed, N.M.A.; Pascu, E.I.; Cavanagh, B.; Hobbs, C.; Santarella, F.; Simpson, C.R.; Murphy, C.M.; Sridharan, R.; González-Vázquez, A. Functionalising Collagen-Based Scaffolds With Platelet-Rich Plasma for Enhanced Skin Wound Healing Potential. Front. Bioeng. Biotechnol. 2019, 7, 371. [Google Scholar] [CrossRef] [Green Version]
- Hamburger, V.; Hamilton, H.L. A series of normal stages in the development of the chick embryo. Dev. Dyn. 1992, 195, 231–272. [Google Scholar] [CrossRef]
- Anderson, S.M.; Siegman, S.N.; Segura, T. The effect of vascular endothelial growth factor (VEGF) presentation within fibrin matrices on endothelial cell branching. Biomaterials 2011, 32, 7432–7443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolan, E.B.; Kovarova, L.; O’Neill, H.; Pravda, M.; Sulakova, R.; Scigalkova, I.; Velebny, V.; Daro, D.; Braun, N.; Cooney, G.M.; et al. Advanced Material Catheter (AMCath), a minimally invasive endocardial catheter for the delivery of fast-gelling covalently cross-linked hyaluronic acid hydrogels. J. Biomater. Appl. 2018, 33, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Dunn, L.K.; Gruenloh, S.K.; Dunn, B.E.; Reddy, D.S.; Falck, J.R.; Jacobs, E.R.; Medhora, M. Chick chorioallantoic membrane as an in vivo model to study vasoreactivity: Characterization of development-dependent hyperemia induced by epoxyeicosatrienoic acids (EETs). Anat. Rec. Part A 2005, 285, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Nowak-Sliwinska, P.; Segura, T.; Iruela-Arispe, M.L. The chicken chorioallantoic membrane model in biology, medicine and bioengineering. Angiogenesis 2014, 17, 779–804. [Google Scholar] [CrossRef] [Green Version]
- Yla-Herttuala, S.; Rissanen, T.T.; Vajanto, I.; Hartikainen, J. Vascular endothelial growth factors: Biology and current status of clinical applications in cardiovascular medicine. J. Am. Coll. Cardiol. 2007, 49, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Koch, S.; Yao, C.; Grieb, G.; Prével, P.; Noah, E.M.; Steffens, G.C.M. Enhancing angiogenesis in collagen matrices by covalent incorporation of VEGF. J. Mater. Sci. Mater. Electron. 2006, 17, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Kornowski, R.; Leon, M.B.; Fuchs, S.; Vodovotz, Y.; Flynn, M.A.; Gordon, D.A.; Pierre, A.; Kovesdi, I.; Keiser, J.A.; Epstein, S.E. Electromagnetic guidance for catheter-based transendocardial injection: A platform for intramyocardial angiogenesis therapy: Results in normal and ischemic porcine models. J. Am. Coll. Cardiol. 2000, 35, 1031–1039. [Google Scholar] [CrossRef] [Green Version]
- Bastings, M.M.C.; Koudstaal, S.; Kieltyka, R.E.; Nakano, Y.; Pape, A.C.H.; Feyen, D.A.M.; van Slochteren, F.J.; Doevendans, P.A.; Sluijter, J.; Meijer, E.W.; et al. A Fast pH-Switchable and Self-Healing Supramolecular Hydrogel Carrier for Guided, Local Catheter Injection in the Infarcted Myocardium. Adv. Health Mater. 2014, 3, 70–78. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.C.; Wall, S.T.; Klepach, D.; Ge, L.; Zhang, Z.; Lee, R.J.; Hinson, A.; Gorman, J.H.; Gorman, R.C.; Guccione, J.M. Algisyl-LVR™ with coronary artery bypass grafting reduces left ventricular wall stress and improves function in the failing human heart. Int. J. Cardiol. 2013, 168, 2022–2028. [Google Scholar] [CrossRef] [Green Version]
- Lee, F.; Chung, J.E.; Kurisawa, M. An injectable enzymatically crosslinked hyaluronic acid–tyramine hydrogel system with independent tuning of mechanical strength and gelation rate. Soft Matter 2008, 4, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.; Chung, J.E.; Kurisawa, M. An injectable hyaluronic acid–tyramine hydrogel system for protein delivery. J. Control. Release 2009, 134, 186–193. [Google Scholar] [CrossRef] [PubMed]
- des Rieux, A.; Ucakar, B.; Mupendwa, B.P.K.; Colau, D.; Feron, O.; Carmeliet, P.; Préat, V. 3D systems delivering VEGF to promote angiogenesis for tissue engineering. J. Control. Release 2011, 150, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Briquez, P.S.; Clegg, L.E.; Martino, M.M.; Mac Gabhann, F.; Hubbell, J.A. Design principles for therapeutic angiogenic materials. Nat. Rev. Mater. 2016, 1, 15006. [Google Scholar] [CrossRef]
- Silva, E.A.; Mooney, D.J. Effects of VEGF temporal and spatial presentation on angiogenesis. Biomaterials 2010, 31, 1235–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minguell, J.J.; Lorino, R.; LaSala, G.P. Myocardial implantation of a combination stem cell product by using a transendocardial MYOSTAR injection catheter: A technical assessment. Acute Card. Care 2011, 13, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Fu, K.; Klibanov, A.M.; Langer, R. Protein stability in controlled-release systems. Nat. Biotechnol. 2000, 18, 24–25. [Google Scholar] [CrossRef]
- Mitragotri, S.; Burke, P.A.; Langer, R. Overcoming the challenges in administering biopharmaceuticals: Formulation and delivery strategies. Nat. Rev. Drug Discov. 2014, 13, 655–672. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Description | VEGF | Star-PGA |
|---|---|---|---|
| HA-TA alone | 1% HA-TA alone | - | - |
| Free VEGF-HA-TA | 1% HA-TA + free VEGF | 500 ng | - |
| Nano-VEGF-HA-TA | 1% HA-TA + star-PGA-VEGF 50:1 nanoparticles | 500 ng | 25 µg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Dwyer, J.; Murphy, R.; González-Vázquez, A.; Kovarova, L.; Pravda, M.; Velebny, V.; Heise, A.; Duffy, G.P.; Cryan, S.A. Translational Studies on the Potential of a VEGF Nanoparticle-Loaded Hyaluronic Acid Hydrogel. Pharmaceutics 2021, 13, 779. https://doi.org/10.3390/pharmaceutics13060779
O’Dwyer J, Murphy R, González-Vázquez A, Kovarova L, Pravda M, Velebny V, Heise A, Duffy GP, Cryan SA. Translational Studies on the Potential of a VEGF Nanoparticle-Loaded Hyaluronic Acid Hydrogel. Pharmaceutics. 2021; 13(6):779. https://doi.org/10.3390/pharmaceutics13060779
Chicago/Turabian StyleO’Dwyer, Joanne, Robert Murphy, Arlyng González-Vázquez, Lenka Kovarova, Martin Pravda, Vladimir Velebny, Andreas Heise, Garry P. Duffy, and Sally Ann Cryan. 2021. "Translational Studies on the Potential of a VEGF Nanoparticle-Loaded Hyaluronic Acid Hydrogel" Pharmaceutics 13, no. 6: 779. https://doi.org/10.3390/pharmaceutics13060779
APA StyleO’Dwyer, J., Murphy, R., González-Vázquez, A., Kovarova, L., Pravda, M., Velebny, V., Heise, A., Duffy, G. P., & Cryan, S. A. (2021). Translational Studies on the Potential of a VEGF Nanoparticle-Loaded Hyaluronic Acid Hydrogel. Pharmaceutics, 13(6), 779. https://doi.org/10.3390/pharmaceutics13060779