
Advantages and Disadvantages of Using Magnetic Nanoparticles for the Treatment of Complicated Ocular Disorders


Abstract
:1. Introduction
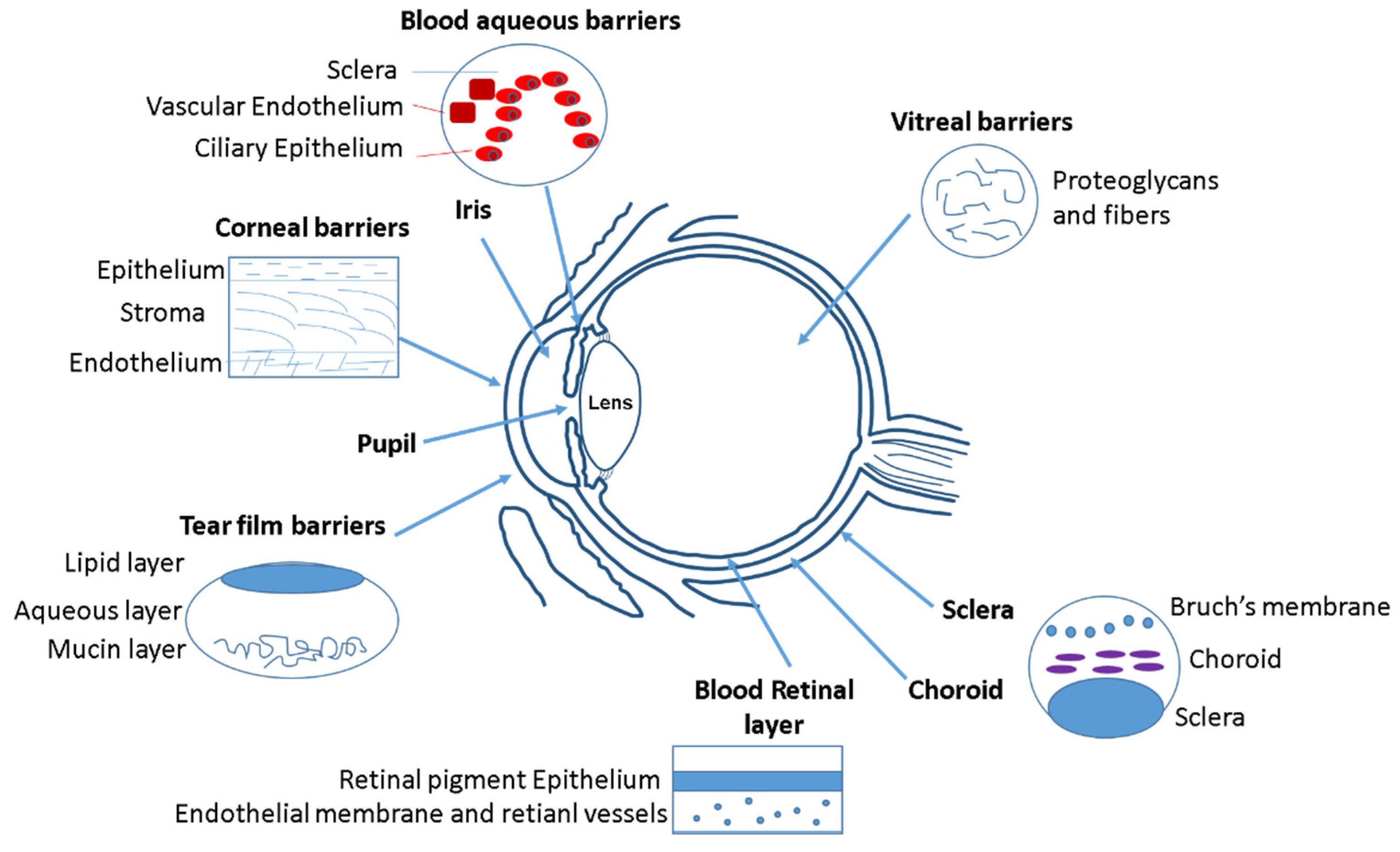
2. Ocular Barriers for Drug Delivery Systems
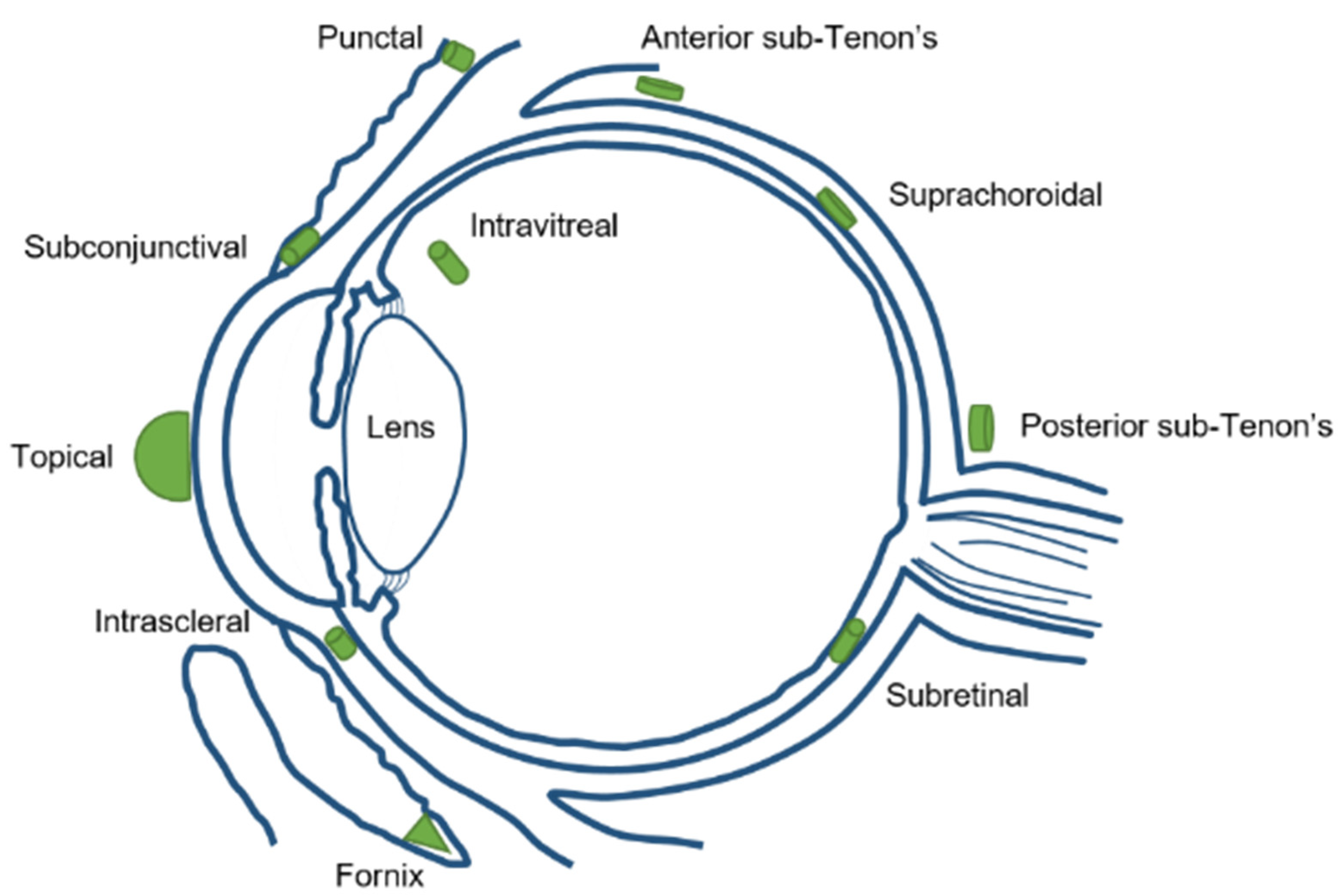
3. Ocular Delivery Routes and Their Limitations
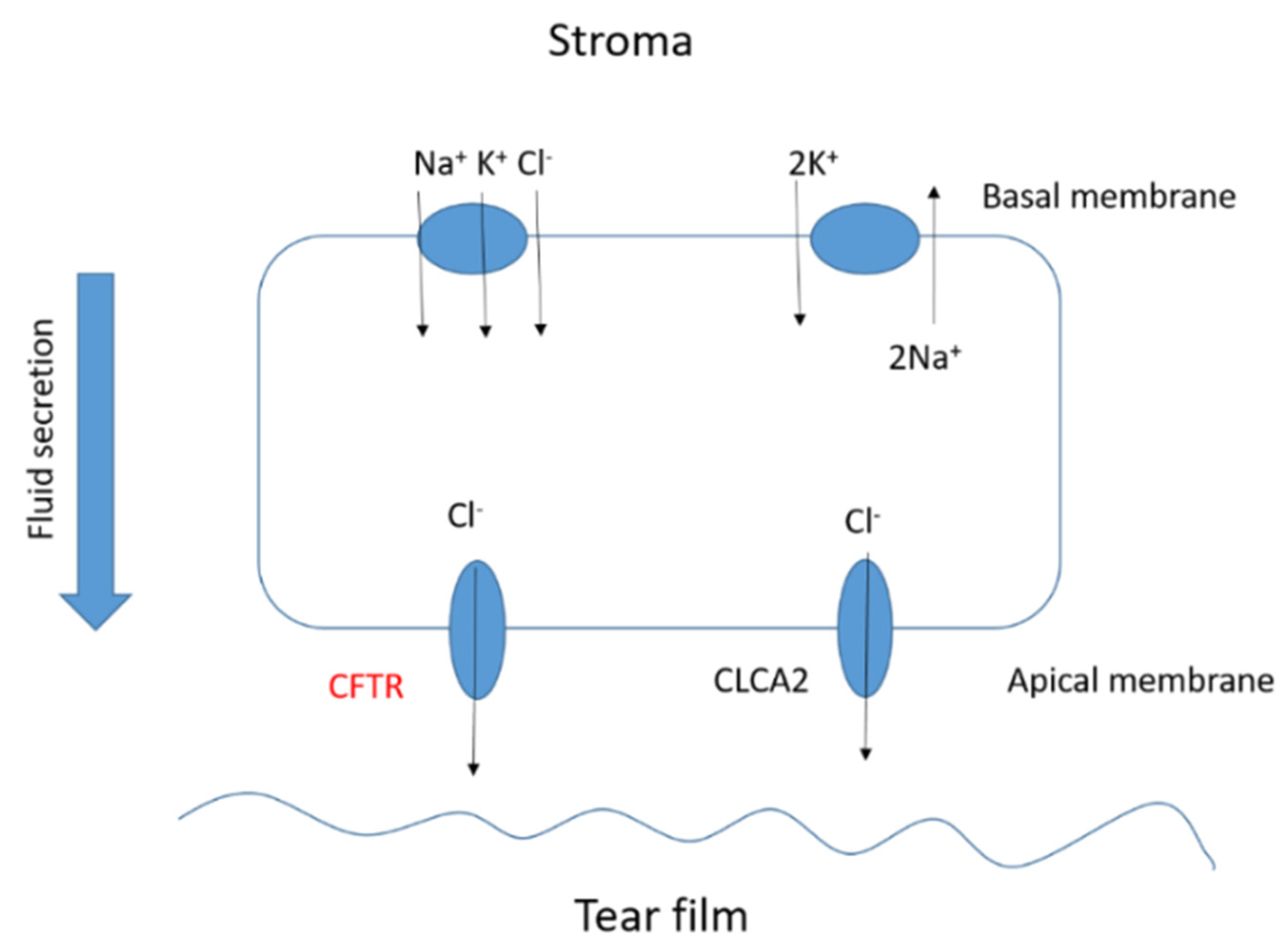
4. Ocular Disorders Derived from Cystic Fibrosis Disease
5. MNPs as Carriers for Drug Delivery
6. Current Uses of MNPs as Pharmaceutical Formulations: Ocular Cancer Diagnosis and Treatment
6.1. Ocular Diagnosis Techniques
6.2. Magnetic Nanoparticles for Ocular Cancer Treatment
6.3. Advantages of the Use of MNPs in Ocular Applications
6.4. Limitations of the Use of MNPs in Ocular Applications
6.5. Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Akter, F. Chapter 5—Ophthalmic Tissue Engineering. In Tissue Engineering Made Easy; Akter, F., Ed.; Academic Press: Waltham, MA, USA, 2016; pp. 43–54. [Google Scholar]
- Shah, S.S.; Denham, L.V.; Elison, J.R.; Bhattacharjee, P.S.; Clement, C.; Huq, T.; Hill, J.M. Drug delivery to the posterior segment of the eye for pharmacologic therapy. Expert Rev. Ophthalmol. 2010, 5, 75–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, Y.; Liu, J.; Jin, S.; Guo, W.; Liang, X.; Hu, Z. Nanotechnology-based strategies for treatment of ocular disease. Acta Pharm. Sin. B 2017, 7, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Kwatra, D.M.A. Drug delivery in ocular diseases: Barriers and strategies. World J. Pharmacol. 2013, 2, 78–83. [Google Scholar] [CrossRef]
- Schneider-Futschik, E.K. Beyond cystic fibrosis transmembrane conductance regulator therapy: A perspective on gene therapy and small molecule treatment for cystic fibrosis. Gene Ther. 2019, 26, 354–362. [Google Scholar] [CrossRef]
- Ghelani, D.P.; Schneider-Futschik, E.K. Emerging Cystic Fibrosis Transmembrane Conductance Regulator Modulators as New Drugs for Cystic Fibrosis: A Portrait of in Vitro Pharmacology and Clinical Translation. ACS Pharmacol. Transl. Sci. 2019, 3, 4–10. [Google Scholar] [CrossRef]
- Quintana-Gallego, E.; Ruiz-Ramos, M.; Delgado-Pecellin, I.; Calero, C.; Soriano, J.B.; Lopez-Campos, J.L. Mortality from cystic fibrosis in Europe: 1994–2010. Pediatr. Pulmonol. 2016, 51, 133–142. [Google Scholar] [CrossRef]
- Farrell, P.M. The prevalence of cystic fibrosis in the European Union. J. Cyst. Fibros. 2008, 7, 450–453. [Google Scholar] [CrossRef] [Green Version]
- Hull, J. Cystic fibrosis transmembrane conductance regulator dysfunction and its treatment. J. R. Soc. Med. 2012, 105 (Suppl. S2), 2–8. [Google Scholar] [CrossRef] [Green Version]
- Qiu, F.; Habgood, M.; Schneider-Futschik, E.K. The Balance between the Safety of Mother, Fetus, and Newborn Undergoing Cystic Fibrosis Transmembrane Conductance Regulator Treatments during Pregnancy. ACS Pharmacol. Transl. Sci. 2020, 3, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Liou, T.G. The Clinical Biology of Cystic Fibrosis Transmembrane Regulator Protein: Its Role and Function in Extrapulmonary Disease. Chest 2019, 155, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Chaudary, N. Triplet CFTR modulators: Future prospects for treatment of cystic fibrosis. Ther. Clin. Risk Manag. 2018, 14, 2375–2383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, R.B.; Hsu, Y.-P.; Olds, L. Cytokine dysregulation in activated cystic fibrosis (CF) peripheral lymphocytes. Clin. Exp. Immunol. 2000, 120, 518–525. [Google Scholar] [CrossRef]
- Mores, A.M.; Casey, S.D.; Felix, C.M.; Phuan, P.W.; Verkman, A.S.; Levin, M.H. Small-molecule CFTR activators increase tear secretion and prevent experimental dry eye disease. FASEB J. 2016, 30, 1789–1797. [Google Scholar] [CrossRef] [Green Version]
- Dakin, C.J.; Numa, A.H.; Wang, H.; Morton, J.R.; Vertzyas, C.C.; Henry, R.L. Inflammation, Infection, and Pulmonary Function in Infants and Young Children with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2002, 165, 904–910. [Google Scholar] [CrossRef]
- Cao, L.; Zhang, X.-D.; Liu, X.; Chen, T.-Y.; Zhao, M. Chloride channels and transporters in human corneal epithelium. Exp. Eye Res. 2010, 90, 771–779. [Google Scholar] [CrossRef] [Green Version]
- Castagna, I.; Roszkowska, A.M.; Famà, F.; Sinicropi, S.; Ferreri, G. The Eye in Cystic Fibrosis. Eur. J. Ophthalmol. 2001, 11, 9–14. [Google Scholar] [CrossRef]
- Seliger, V.; Bai, Y.; Volkova, N.; Tian, S.; Waltz, D. 196 Prevalence of cataracts in a population of cystic fibrosis patients homozygous for the F508del mutation. J. Cyst. Fibros. 2015, 14, S108. [Google Scholar] [CrossRef]
- Incorporated, V.P. Safety Study An Ocular of Ivacaftor-Treated Pediatric Patients 11 Years of Age or Younger with Cystic Fibrosis. Available online: https://clinicaltrials.gov/ct2/show/NCT01863238 (accessed on 31 May 2021).
- Starr, M.R.; Norby, S.M.; Scott, J.P.; Bakri, S.J. Acute retinal vein occlusion and cystic fibrosis. Int. J. Retina Vitreous 2018, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Rottner, M.; Freyssinet, J.-M.; Martínez, M.C. Mechanisms of the noxious inflammatory cycle in cystic fibrosis. Respir. Res. 2009, 10, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nebbioso, M.; Quattrucci, S.; Leggieri, E.; Spadea, L.; Vingolo, E.M. Cystic Fibrosis and New Trends by Ophthalmological Evaluation: A Pilot Study. BioMed. Res. Int. 2014, 2014, 580373. [Google Scholar] [CrossRef] [Green Version]
- Gorantla, S.; Rapalli, V.K.; Waghule, T.; Singh, P.P.; Dubey, S.K.; Saha, R.N.; Singhvi, G. Nanocarriers for ocular drug delivery: Current status and translational opportunity. RSC Adv. 2020, 10, 27835–27855. [Google Scholar] [CrossRef]
- Maldonado-Camargo, L.; Unni, M.; Rinaldi, C. Magnetic Characterization of Iron Oxide Nanoparticles for Biomedical Applications. Methods Mol. Biol. 2017, 1570, 47–71. [Google Scholar]
- Chatterjee, D.K.; Diagaradjane, P.; Krishnan, S. Nanoparticle-mediated hyperthermia in cancer therapy. Ther. Deliv. 2011, 2, 1001–1014. [Google Scholar] [CrossRef] [Green Version]
- Reyes-Ortega, F.; Checa Fernández, B.L.; Delgado, A.V.; Iglesias, G.R. Hyperthermia-Triggered Doxorubicin Release from Polymer-Coated Magnetic Nanorods. Pharmaceutics 2019, 11, 517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iglesias, G.R.; Reyes-Ortega, F.; Checa Fernandez, B.L.; Delgado, Á.V. Hyperthermia-Triggered Gemcitabine Release from Polymer-Coated Magnetite Nanoparticles. Polymers 2018, 10, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bi, Q.; Song, X.; Hu, A.; Luo, T.; Jin, R.; Ai, H.; Nie, Y. Magnetofection: Magic magnetic nanoparticles for efficient gene delivery. Chin. Chem. Lett. 2020, 31, 3041–3046. [Google Scholar] [CrossRef]
- Demirci, H.; Slimani, N.; Pawar, M.; Kumon, R.E.; Vaishnava, P.; Besirli, C.G. Magnetic Hyperthermia in Y79 Retinoblastoma and ARPE-19 Retinal Epithelial Cells: Tumor Selective Apoptotic Activity of Iron Oxide Nanoparticle. Transl. Vis. Sci. Technol. 2019, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Bhardwaj, A.; Parekh, K.; Jain, N. In vitro hyperthermic effect of magnetic fluid on cervical and breast cancer cells. Sci. Rep. 2020, 10, 15249. [Google Scholar] [CrossRef] [PubMed]
- Anilkumar, T.S.; Lu, Y.-J.; Chen, J.-P. Optimization of the Preparation of Magnetic Liposomes for the Combined Use of Magnetic Hyperthermia and Photothermia in Dual Magneto-Photothermal Cancer Therapy. Int. J. Mol. Sci. 2020, 21, 5187. [Google Scholar]
- Sridhar, M.S. Anatomy of cornea and ocular surface. Indian J. Ophthalmol. 2018, 66, 190–194. [Google Scholar]
- Bachu, R.D.; Chowdhury, P.; Al-Saedi, Z.H.F.; Karla, P.K.; Boddu, S.H.S. Ocular Drug Delivery Barriers-Role of Nanocarriers in the Treatment of Anterior Segment Ocular Diseases. Pharmaceutics 2018, 10, 28. [Google Scholar] [CrossRef] [Green Version]
- Zamboulis, A.; Nanaki, S.; Michailidou, G.; Koumentakou, I.; Lazaridou, M.; Ainali, N.M.; Xanthopoulou, E.; Bikiaris, D.N. Chitosan and its Derivatives for Ocular Delivery Formulations: Recent Advances and Developments. Polymers 2020, 12, 1519. [Google Scholar] [CrossRef]
- Delamere, N.A. Ciliary Body and Ciliary Epithelium. Adv. Organ. Biol. 2005, 10, 127–148. [Google Scholar]
- Swetledge, S.; Jung, J.P.; Carter, R.; Sabliov, C. Distribution of polymeric nanoparticles in the eye: Implications in ocular disease therapy. J. Nanobiotechnol. 2021, 19, 10. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-López, E.; Espina, M.; Doktorovova, S.; Souto, E.B.; García, M.L. Lipid nanoparticles (SLN, NLC): Overcoming the anatomical and physiological barriers of the eye—Part I—Barriers and determining factors in ocular delivery. Eur. J. Pharm. Biopharm. 2017, 110, 70–75. [Google Scholar] [CrossRef]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-Álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannaccini, M.; Giannini, M.; Calatayud, M.P.; Goya, G.F.; Cuschieri, A.; Dente, L.; Raffa, V. Magnetic Nanoparticles as Intraocular Drug Delivery System to Target Retinal Pigmented Epithelium (RPE). Int. J. Mol. Sci. 2014, 15, 1590–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannaccini, M.; Pedicini, L.; De Matienzo, G.; Chiellini, F.; Dente, L.; Raffa, V. Magnetic nanoparticles: A strategy to target the choroidal layer in the posterior segment of the eye. Sci. Rep. 2017, 7, 43092. [Google Scholar] [CrossRef] [Green Version]
- Awwad, S.; Ahmed, A.M.; Sharma, G.; Heng, J.; Khaw, P.T.; Brocchini, S.; Lockwood, A. Principles of pharmacology in the eye. Br. J. Pharmacol. 2017, 174, 4205–4223. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Xiang, C.D.; Gale, D.; Carreiro, S.; Wu, E.Y.; Zhang, E.Y. Drug Transporter and Cytochrome P450 mRNA Expression in Human Ocular Barriers: Implications for Ocular Drug Disposition. Drug Metab. Dispos. 2008, 36, 1300–1307. [Google Scholar] [CrossRef] [Green Version]
- Aukunuru, J.; Sunkara, G.; Bandi, N.; Thoreson, W.; Kompella, U.B. Expression of Multidrug Resistance-Associated Protein (MRP) in Human Retinal Pigment Epithelial Cells and Its Interaction with BAPSG, a Novel Aldose Reductase Inhibitor. Pharm. Res. 2001, 18, 565–572. [Google Scholar] [CrossRef]
- Joseph, R.R.; Venkatraman, S.S. Drug delivery to the eye: What benefits do nanocarriers offer? Nanomedicine 2017, 12, 683–702. [Google Scholar] [CrossRef] [Green Version]
- Agrahari, V.; Mandal, A.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Ray, A.; Hadji, H.; Mitra, R.; Pal, D.; Mitra, A.K. A comprehensive insight on ocular pharmacokinetics. Drug Deliv. Transl. Res. 2016, 6, 735–754. [Google Scholar] [CrossRef] [PubMed]
- You, S.; Luo, J.; Grossniklaus, H.E.; Gou, M.-L.; Meng, K.; Zhang, Q. Nanomedicine in the application of uveal melanoma. Int. J. Ophthalmol. 2016, 9, 1215–1225. [Google Scholar] [PubMed]
- Botelho, S.Y.; Goldstein, A.M.; Rosenlund, M.L. Tear sodium, potassium, chloride, and calcium at various flow rates: Children with cystic fibrosis and unaffected siblings with and without corneal staining. J. Pediatr. 1973, 83, 601–606. [Google Scholar] [CrossRef]
- Morkeberg, J.C.; Edmund, C.; Prause, J.U.; Lanng, S.; Koch, C.; Michaelsen, K.F. Ocular findings in cystic fibrosis patients receiving vitamin A supplementation. Graefe’s Arch. Clin. Exp. Ophthalmol. 1995, 233, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Mrugacz, M.; Kaczmarski, M.; Bakunowicz-Lazarczyk, A.; Zelazowska, B.; Wysocka, J.; Minarowska, A. IL-8 and IFN-γ in Tear Fluid of Patients with Cystic Fibrosis. J. Interferon Cytokine Res. 2006, 26, 71–75. [Google Scholar] [CrossRef]
- Ansari, E.A.; Sahni, K.; Etherington, C.; Morton, A.; Conway, S.P.; Moya, E.; Littlewood, J.M. Ocular signs and symptoms and vitamin A status in patients with cystic fibrosis treated with daily vitamin A supplements. Br. J. Ophthalmol. 1999, 83, 688–691. [Google Scholar] [CrossRef] [Green Version]
- Alghadyan, A.; Aljindan, M.; Alhumeidan, A.; Kazi, G.; Mcmhon, R. Lacrimal glands in cystic fibrosis. Saudi J. Ophthalmol. 2013, 27, 113–116. [Google Scholar] [CrossRef] [Green Version]
- Joshi, D.; Dhawan, A.; Baker, A.J.; Heneghan, M.A. An atypical presentation of cystic fibrosis: A case report. J. Med. Case Rep. 2008, 2, 201. [Google Scholar] [CrossRef] [Green Version]
- Gelman, R.; DiMango, E.A.; Schiff, W.M. Sequential bilateral central retinal vein occlusions in a cystic fibrosis patient with hyperhomocysteinemia and hypergamma-globulinemia. Retin Cases Brief Rep. 2013, 7, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Hiscox, R.J.; Purslow, C.; North, R.; Ketchell, I.; Evans, K.S.E. Branch Retinal Vein Occlusion in an Asymptomatic Adult with Cystic Fibrosis. Optom. Vis. Sci. 2014, 91, S52–S54. [Google Scholar] [CrossRef]
- Lass, J.H.; Spurney, R.V.; Dutt, R.M.; Andersson, H.; Kochar, H.; Rodman, H.M.; Stern, R.C.; Doershuk, C.F. A Morphologic and Fluorophotometric Analysis of the Corneal Endothelium in Type I Diabetes Mellitus and Cystic Fibrosis. Am. J. Ophthalmol. 1985, 100, 783–788. [Google Scholar] [CrossRef]
- Abelson, M.B.; Workman, A.; Taylor, A.; Mass, N.A. Eavesdropping on Blepharitis. 2007. Available online: https://www.reviewofophthalmology.com/article/eavesdropping-on-blepharitis (accessed on 7 May 2021).
- Mrugacz, M.; Tobolczyk, J.; Minarowska, A. Retinol binding protein status in relation to ocular surface changes in patients with cystic fibrosis treated with daily vitamin A supplements. Eur. J. Pediatr. 2005, 164, 202–206. [Google Scholar] [CrossRef]
- Vernon, S.A.; Neugebauer, M.A.Z.; Brimlow, G.; Tyrell, J.C.; Hiller, E.J. Conjunctival Xerosis in Cystic Fibrosis. J. R. Soc. Med. 1989, 82, 46–47. [Google Scholar] [CrossRef] [Green Version]
- Brooks, H.L.; Driebe, W.T., Jr.; Schemmer, G.G. Xerophthalmia and Cystic Fibrosis. Arch. Ophthalmol. 1990, 108, 354–357. [Google Scholar] [CrossRef]
- Wamsley, S.; Patel, S.M.; Wood, M.G.; Villalobos, R.; Albert, D.M.; Mootha, V.V. Advanced Keratomalacia with Descemetocele in an Infant With Cystic Fibrosis. Arch. Ophthalmol. 2005, 123, 1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schupp, C.; Olano-Martin, E.; Gerth, C.; Morrissey, B.M.; Cross, C.E.; Werner, J.S. Lutein, zeaxanthin, macular pigment, and visual function in adult cystic fibrosis patients. Am. J. Clin. Nutr. 2004, 79, 1045–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, L.G.M.; De Grande, V.; Stella, S.; Reibaldi, M.; Lionetti, E.; Franzonello, C.; Leonardi, S.; Gagliano, C.; Russo, A.; La Rosa, M. Tear Osmolarity in Pediatric Patients with Cystic Fibrosis. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4289. [Google Scholar]
- Mrugacz, M.M.A.; Bakunowicz-Lazarczyk, A.; Zywalewska, N. Dry eye syndrome in children with cystic fibrosis. Med. Wieku Rozw. 2004, 8, 865–870. [Google Scholar]
- Ito, A.; Shinkai, M.; Honda, H.; Kobayashi, T. Medical application of functionalized magnetic nanoparticles. J. Biosci. Bioeng. 2005, 100, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Reyes-Ortega, F.; Delgado, Á.V.; Iglesias, G.R. Modulation of the Magnetic Hyperthermia Response Using Different Superparamagnetic Iron Oxide Nanoparticle Morphologies. Nanomaterials 2021, 11, 627. [Google Scholar] [CrossRef]
- Tan, M.; Reyes-Ortega, F.; Schneider-Futschik, E.K. Successes and Challenges: Inhaled Treatment Approaches Using Magnetic Nanoparticles in Cystic Fibrosis. Magnetochemistry 2020, 6, 25. [Google Scholar] [CrossRef]
- Avasthi, A.; Caro, C.; Pozo-Torres, E.; Leal, M.P.; García-Martín, M.L. Magnetic Nanoparticles as MRI Contrast Agents. Top. Curr. Chem. 2020, 378, 1–43. [Google Scholar]
- Shabatina, T.I.; Vernaya, O.I.; Shabatin, V.P.; Melnikov, M.Y. Magnetic Nanoparticles for Biomedical Purposes: Modern Trends and Prospects. Magnetochemistry 2020, 6, 30. [Google Scholar] [CrossRef]
- Malhotra, N.; Lee, J.-S.; Liman, R.A.D.; Ruallo, J.M.S.; Villaflores, O.B.; Ger, T.-R.; Hsiao, C.-D. Potential Toxicity of Iron Oxide Magnetic Nanoparticles: A Review. Molecules 2020, 25, 3159. [Google Scholar] [CrossRef]
- Schweiger, C.; Hartmann, R.; Zhang, F.; Parak, W.J.; Kissel, T.H.; Gil, P.R. Quantification of the internalization patterns of superparamagnetic iron oxide nanoparticles with opposite charge. J. Nanobiotechnol. 2012, 10, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tassa, C.; Shaw, S.Y.; Weissleder, R. Dextran-Coated Iron Oxide Nanoparticles: A Versatile Platform for Targeted Molecular Imaging, Molecular Diagnostics, and Therapy. Acc. Chem. Res. 2011, 44, 842–852. [Google Scholar] [CrossRef] [Green Version]
- Gómez Pérez, A.; González-Martínez, E.; Díaz Águila, C.R.; González-Martínez, D.A.; González Ruiz, G.; García Artalejo, A.; Yee-Madeira, H. Chitosan-coated magnetic iron oxide nanoparticles for DNA and rhEGF separation. Coll. Surf. A Physicochem. Eng. Aspects 2020, 591, 124500. [Google Scholar] [CrossRef]
- Khandhar, A.P.; Keselman, P.; Kemp, S.J.; Ferguson, R.M.; Goodwill, P.W.; Conolly, S.M.; Krishnan, K.M. Evaluation of PEG-coated iron oxide nanoparticles as blood pool tracers for preclinical magnetic particle imaging. Nanoscale 2017, 9, 1299–1306. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, M.R.; Geninatti Crich, S.; Sieni, E.; Sgarbossa, P.; Cavallari, E.; Stefania, R.; Dughiero, F.; Aime, S. Iron oxide/PLGA nanoparticles for magnetically controlled drug release. Int. J. Appl. Electromagn. Mech. 2017, 53, S53–S60. [Google Scholar] [CrossRef]
- Hedayatnasab, Z.; Dabbagh, A.; Abnisa, F.; Daud, W.M.A.W. Polycaprolactone-coated superparamagnetic iron oxide nanoparticles for in vitro magnetic hyperthermia therapy of cancer. Eur. Polym. J. 2020, 133, 109789. [Google Scholar] [CrossRef]
- Ketebo, A.A.; Shin, T.H.; Jun, M.; Lee, G.; Park, S. Effect of silica-coated magnetic nanoparticles on rigidity sensing of human embryonic kidney cells. J. Nanobiotechnol. 2020, 18, 170. [Google Scholar] [CrossRef] [PubMed]
- Toro-Cordova, A.; Flores-Cruz, M.; Santoyo-Salazar, J.; Carrillo-Nava, E.; Jurado, R.; Figueroa-Rodriguez, P.A.; Lopez-Sanchez, P.; Medina, L.A.; Garcia-Lopez, P. Liposomes Loaded with Cisplatin and Magnetic Nanoparticles: Physicochemical Characterization, Pharmacokinetics, and In-Vitro Efficacy. Molecules 2018, 23, 2272. [Google Scholar] [CrossRef] [Green Version]
- Bobo, D.; Robinson, K.; Islam, J.; Thurecht, K.J.; Corrie, S.R. Nanoparticle-Based Medicines: A Review of FDA-Approved Materials and Clinical Trials to Date. Pharm. Res. 2016, 33, 2373–2387. [Google Scholar] [CrossRef] [PubMed]
- Sjöstrand, S.; Evertsson, M.; Jansson, T. Magnetomotive Ultrasound Imaging Systems: Basic Principles and First Applications. Ultrasound Med. Biol. 2020, 46, 2636–2650. [Google Scholar] [CrossRef]
- Oldenburg, A.L.; Blackmon, R.L.; Sierchio, J.M. Magnetic and Plasmonic Contrast Agents in Optical Coherence Tomography. IEEE J. Sel. Top Quantum Electron. 2016, 22, 6803913. [Google Scholar] [CrossRef] [Green Version]
- Shin, T.-H.; Choi, Y.; Kim, S.; Cheon, J. Recent advances in magnetic nanoparticle-based multi-modal imaging. Chem. Soc. Rev. 2015, 44, 4501–4516. [Google Scholar] [CrossRef]
- Goel, S.; England, C.G.; Chen, F.; Cai, W. Positron emission tomography and nanotechnology: A dynamic duo for cancer theranostics. Adv. Drug Deliv. Rev. 2017, 113, 157–176. [Google Scholar] [CrossRef] [Green Version]
- Xie, W.; Guo, Z.; Gao, F.; Gao, Q.; Wang, D.; Liaw, B.-S.; Cai, Q.; Sun, X.; Wang, X.; Zhao, L. Shape-, size- and structure-controlled synthesis and biocompatibility of iron oxide nanoparticles for magnetic theranostics. Theranostics 2018, 8, 3284–3307. [Google Scholar] [CrossRef]
- Schachar, R.A.; Chen, W.; Woo, B.K.; Pierscionek, B.K.; Zhang, X.; Ma, L. Diffusion of nanoparticles into the capsule and cortex of a crystalline lens. Nanotechnology 2007, 19, 025102. [Google Scholar] [CrossRef]
- Tzameret, A.; Ketter-Katz, H.; Edelshtain, V.; Sher, I.; Corem-Salkmon, E.; Levy, I.; Last, D.; Guez, D.; Mardor, Y.; Margel, S.; et al. In vivo MRI assessment of bioactive magnetic iron oxide/human serum albumin nanoparticle delivery into the posterior segment of the eye in a rat model of retinal degeneration. J. Nanobiotechnol. 2019, 17, 3. [Google Scholar] [CrossRef]
- Paschalis, E.I.; Chodosh, J.; Sperling, R.A.; Salvador-Culla, B.; Dohlman, C. A Novel Implantable Glaucoma Valve Using Ferrofluid. PLoS ONE 2013, 8, e67404. [Google Scholar] [CrossRef] [Green Version]
- Snider, E.J.; Kubelick, K.P.; Tweed, K.; Kim, R.K.; Li, Y.; Gao, K.; Read, A.T.; Emelianov, S.; Ethier, C.R. Improving Stem Cell Delivery to the Trabecular Meshwork Using Magnetic Nanoparticles. Sci. Rep. 2018, 8, 12251. [Google Scholar] [CrossRef] [Green Version]
- Krause, M.; Kwong, K.K.; Xiong, J.; Gragoudas, E.S.; Young, L.H.Y. MRI of Blood Volume and Cellular Uptake of Superparamagnetic Iron in an Animal Model of Choroidal Melanoma. Ophthalmic Res. 2002, 34, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Orynbayeva, Z.; Sensenig, R.; Polyak, B. Metabolic and structural integrity of magnetic nanoparticle-loaded primary endothelial cells for targeted cell therapy. Nanomedicine 2015, 10, 1555–1568. [Google Scholar] [CrossRef] [Green Version]
- Latorre, A.; Latorre, A.; Castellanos, M.; Lafuente-Gómez, N.; Diaz, C.R.; Crespo-Barreda, A.; Lecea, M.; Cordani, M.; Martín-Duque, P.; Somoza, Á. Albumin-based nanostructures for uveal melanoma treatment. Nanomed. Nanotechnol. Biol. Med. 2021, 35, 102391. [Google Scholar] [CrossRef] [PubMed]
- Yanai, A.H.U.; Metcalfe, A.L.; Soema, P.; Addo, L.; Gregory-Evans, C.Y.; Po, K.; Shan, X.; Moritz, O.L.; Gregory-Evans, K. Focused magnetic stem cell targeting to the retina using superparamagnetic iron oxide nanoparticles. Cell Transplant. 2012, 21, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Prow, T.W. Toxicity of nanomaterials to the eye. WIREs Nanomed. Nanobiotechnol. 2010, 2, 317–333. [Google Scholar] [CrossRef] [PubMed]
- Söderstjerna, E.; Bauer, P.; Cedervall, T.; Abdshill, H.; Johansson, F.; Johansson, U.E. Silver and Gold Nanoparticles Exposure to In Vitro Cultured Retina—Studies on Nanoparticle Internalization, Apoptosis, Oxidative Stress, Glial- and Microglial Activity. PLoS ONE 2014, 9, e105359. [Google Scholar] [CrossRef] [PubMed]
- Raju, H.B.; Hu, Y.; Vedula, A.; Dubovy, S.R.; Goldberg, J.L. Evaluation of Magnetic Micro- and Nanoparticle Toxicity to Ocular Tissues. PLoS ONE 2011, 6, e17452. [Google Scholar] [CrossRef] [PubMed]
- Thakor, A.S.; Jokerst, J.V.; Ghanouni, P.; Campbell, J.L.; Mittra, E.; Gambhir, S.S. Clinically Approved Nanoparticle Imaging Agents. J. Nucl. Med. 2016, 57, 1833–1837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, L.M.; Marzola, P.; Nicolato, E.; Fiorini, S.; Guillamón, M.d.l.H.; Piñol, R.; Gabilondo, L.; Millán, A.; Palacio, F. Polymer-coated superparamagnetic iron oxide nanoparticles as T2 contrast agent for MRI and their uptake in liver. Future Sci. 2019, 5, FSO235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, C.; Xu, K.; Gu, H.; Zheng, R.; Liu, H.; Zhang, X.; Guo, Z.; Xu, B. Dopamine as A Robust Anchor to Immobilize Functional Molecules on the Iron Oxide Shell of Magnetic Nanoparticles. J. Am. Chem. Soc. 2004, 126, 9938–9939. [Google Scholar] [CrossRef]
- Amstad, E.; Zurcher, S.; Mashaghi, A.; Wong, J.Y.; Textor, M.; Reimhult, E. Surface Functionalization of Single Superparamagnetic Iron Oxide Nanoparticles for Targeted Magnetic Resonance Imaging. Small 2009, 5, 1334–1342. [Google Scholar] [CrossRef]
- Li, J.; Nickel, R.; Wu, J.; Lin, F.; van Lierop, J.; Liu, S. A new tool to attack biofilms: Driving magnetic iron-oxide nanoparticles to disrupt the matrix. Nanoscale 2019, 11, 6905–6915. [Google Scholar] [CrossRef]
- Han, C.; Romero, N.; Fischer, S.; Dookran, J.; Berger, A.; Doiron, A.L. Recent developments in the use of nanoparticles for treatment of biofilms. Nanotechnol. Rev. 2017, 6, 383–404. [Google Scholar] [CrossRef]
- Yeh, Y.-C.; Huang, T.-H.; Yang, S.-C.; Chen, C.-C.; Fang, J.-Y. Nano-Based Drug Delivery or Targeting to Eradicate Bacteria for Infection Mitigation: A Review of Recent Advances. Front. Chem. 2020, 8. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Size (nm) | Diagnosis Technique | Application | Reference |
|---|---|---|---|---|
| IONPS | 10 | Confocal microscopy | Retinal detachment | [83] |
| IONPS | 50 | MRI | Retinal degeneration | [84] |
| Ferrofluid | 10–100 | X-Ray Diffraction | Glaucoma treatment | [85] |
| Nanocubes | 20 | Fluorescein angiography | Glaucoma treatment | [86] |
| IONPS | 60 | Confocal microcopy | Aged Macular Degeneration (AMD), Retinal Pigment Epithelium (RPE) | [39,40] |
| IONPS | 30 | MRI | Choroidal melanoma | [87] |
| IONPS | 200 | Fluorescent confocal microscopy | Retinal degeneration | [88] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider-Futschik, E.K.; Reyes-Ortega, F. Advantages and Disadvantages of Using Magnetic Nanoparticles for the Treatment of Complicated Ocular Disorders. Pharmaceutics 2021, 13, 1157. https://doi.org/10.3390/pharmaceutics13081157
Schneider-Futschik EK, Reyes-Ortega F. Advantages and Disadvantages of Using Magnetic Nanoparticles for the Treatment of Complicated Ocular Disorders. Pharmaceutics. 2021; 13(8):1157. https://doi.org/10.3390/pharmaceutics13081157
Chicago/Turabian StyleSchneider-Futschik, Elena K., and Felisa Reyes-Ortega. 2021. "Advantages and Disadvantages of Using Magnetic Nanoparticles for the Treatment of Complicated Ocular Disorders" Pharmaceutics 13, no. 8: 1157. https://doi.org/10.3390/pharmaceutics13081157
APA StyleSchneider-Futschik, E. K., & Reyes-Ortega, F. (2021). Advantages and Disadvantages of Using Magnetic Nanoparticles for the Treatment of Complicated Ocular Disorders. Pharmaceutics, 13(8), 1157. https://doi.org/10.3390/pharmaceutics13081157