
Mesenchymal Stromal Cells Perspective: New Potential Therapeutic for the Treatment of Neurological Diseases


Abstract
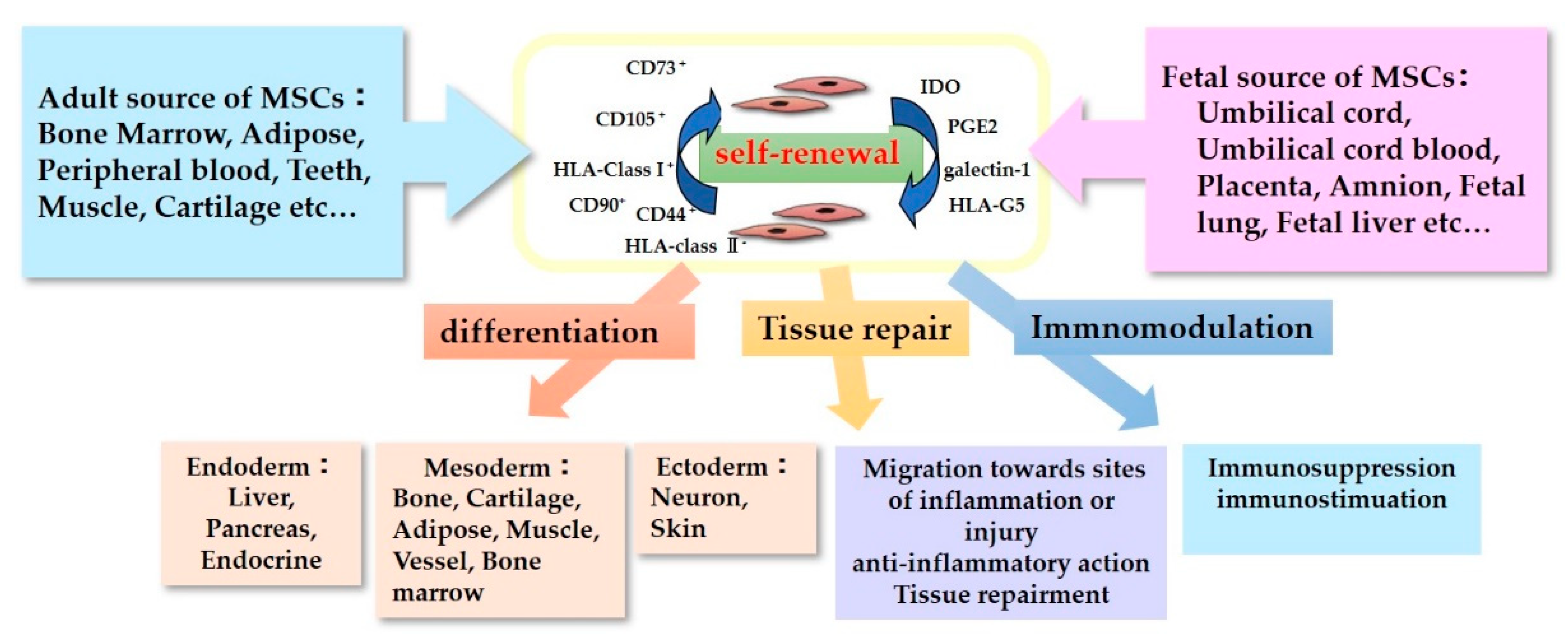
:1. Introduction
2. Mechanisms of ACTION of MSC on Neurological Injury Models
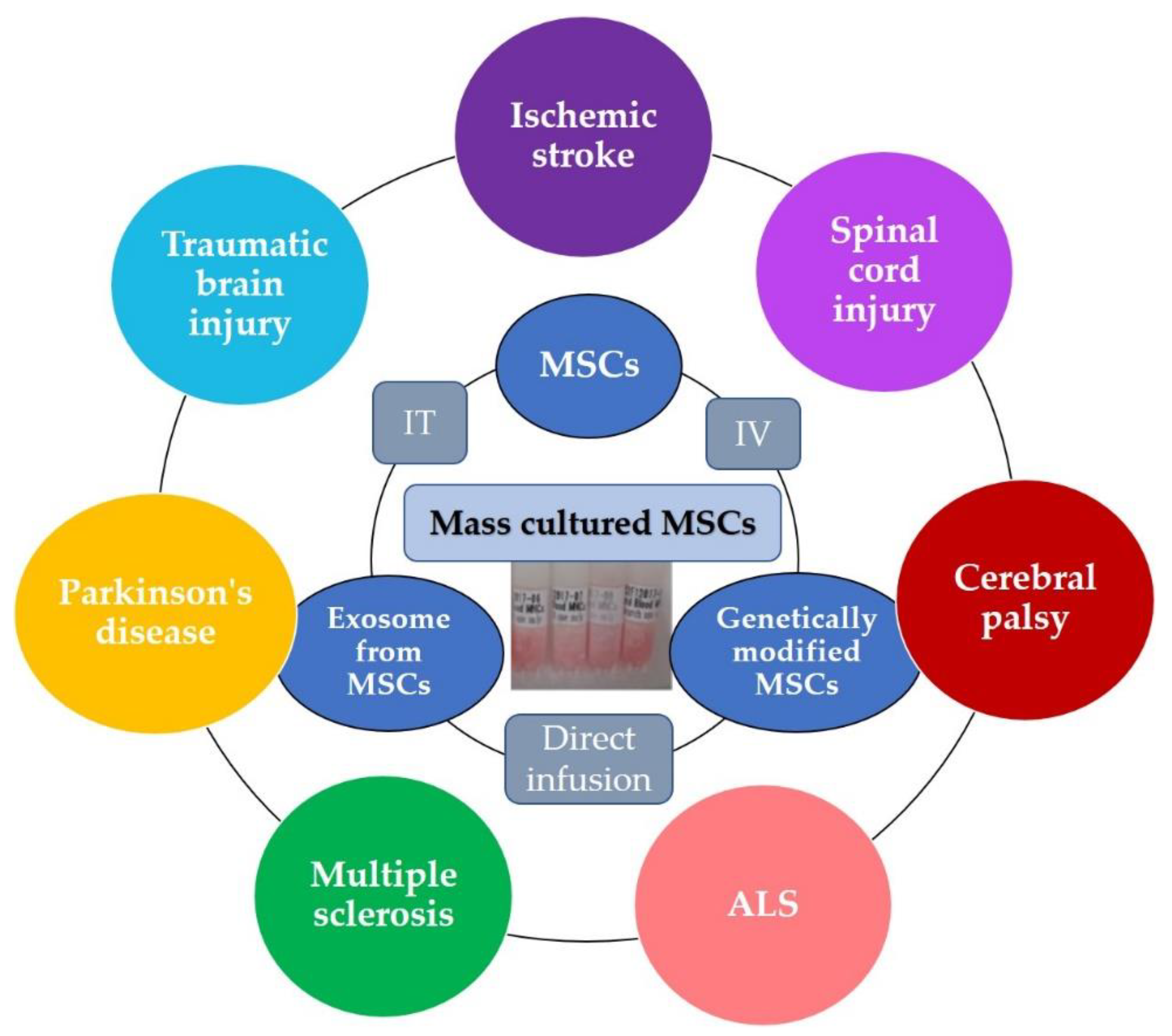
3. Clinical Application of MSCs for Neurological Disorders
3.1. Ischemic Stroke
3.2. Spinal Cord Injury
3.3. Cerebral Palsy
3.4. Amyotrophic Lateral Sclerosis (ALS)
3.5. Multiple Sclerosis
3.6. Parkinson’s Disease
3.7. Traumatic Brain Injury
4. Room for Improvement of MSCs Therapy and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nagamura-Inoue, T.; Mukai, T. Umbilical Cord is a Rich Source of Mesenchymal Stromal Cells for Cell Therapy. Curr. Stem Cell Res. Ther. 2016, 11, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I. Mesenchymal stem cells. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 1991, 9, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Gnecchi, M.; Melo, L.G. Bone marrow-derived mesenchymal stem cells: Isolation, expansion, characterization, viral transduction, and production of conditioned medium. Methods Mol. Biol. 2009, 482, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Bieback, K.; Kluter, H. Mesenchymal stromal cells from umbilical cord blood. Curr. Stem Cell Res. Ther. 2007, 2, 310–323. [Google Scholar] [CrossRef] [PubMed]
- In’t Anker, P.S.; Scherjon, S.A.; Kleijburg-van der Keur, C.; de Groot-Swings, G.M.; Claas, F.H.; Fibbe, W.E.; Kanhai, H.H. Isolation of mesenchymal stem cells of fetal or maternal origin from human placenta. Stem Cells 2004, 22, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Gruber, H.E.; Deepe, R.; Hoelscher, G.L.; Ingram, J.A.; Norton, H.J.; Scannell, B.; Loeffler, B.J.; Zinchenko, N.; Hanley, E.N.; Tapp, H. Human adipose-derived mesenchymal stem cells: Direction to a phenotype sharing similarities with the disc, gene expression profiling, and coculture with human annulus cells. Tissue Eng. Part A 2010, 16, 2843–2860. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.F.; Chen, K.W.; Chien, Y.; Lai, Y.H.; Hsieh, S.T.; Ma, H.Y.; Wang, K.C.; Shiau, C.Y. Dental Pulp Stem Cell-Derived Factors Alleviate Subarachnoid Hemorrhage-Induced Neuroinflammation and Ischemic Neurological Deficits. Int. J. Mol. Sci. 2019, 20, 3747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliaghaei, A.; Boroujeni, M.E.; Ahmadi, H.; Bayat, A.H.; Tavirani, M.R.; Abdollahifar, M.A.; Pooyafar, M.H.; Mansouri, V. Dental pulp stem cell transplantation ameliorates motor function and prevents cerebellar atrophy in rat model of cerebellar ataxia. Cell Tissue Res. 2019, 376, 179–187. [Google Scholar] [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, E.M.; Le Blanc, K.; Dominici, M.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Deans, R.J.; Krause, D.S.; Keating, A.; International Society for Cellular Therapy. Clarification of the nomenclature for MSC: The International Society for Cellular Therapy position statement. Cytotherapy 2005, 7, 393–395. [Google Scholar] [CrossRef] [PubMed]
- Nagamura-Inoue, T.; He, H. Umbilical cord-derived mesenchymal stem cells: Their advantages and potential clinical utility. World J. Stem Cells 2014, 6, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.L.; Anderson, C.; Medicetty, S.; Seshareddy, K.B.; Weiss, R.J.; VanderWerff, I.; Troyer, D.; McIntosh, K.R. Immune properties of human umbilical cord Wharton’s jelly-derived cells. Stem Cells 2008, 26, 2865–2874. [Google Scholar] [CrossRef] [PubMed]
- Seshareddy, K.; Troyer, D.; Weiss, M.L. Method to isolate mesenchymal-like cells from Wharton’s Jelly of umbilical cord. Methods Cell Biol. 2008, 86, 101–119. [Google Scholar] [CrossRef]
- Mukai, T.; Tojo, A.; Nagamura-Inoue, T. Mesenchymal stromal cells as a potential therapeutic for neurological disorders. Regen. Ther. 2018, 9, 32–37. [Google Scholar] [CrossRef]
- Mukai, T.; Mori, Y.; Shimazu, T.; Takahashi, A.; Tsunoda, H.; Yamaguchi, S.; Kiryu, S.; Tojo, A.; Nagamura-Inoue, T. Intravenous injection of umbilical cord-derived mesenchymal stromal cells attenuates reactive gliosis and hypomyelination in a neonatal intraventricular hemorrhage model. Neuroscience 2017, 355, 175–187. [Google Scholar] [CrossRef]
- Mukai, T.; Tojo, A.; Nagamura-Inoue, T. Umbilical Cord-Derived Mesenchymal Stromal Cells Contribute to Neuroprotection in Neonatal Cortical Neurons Damaged by Oxygen-Glucose Deprivation. Front. Neurol. 2018, 9, 466. [Google Scholar] [CrossRef] [PubMed]
- Fuloria, S.; Subramaniyan, V.; Dahiya, R.; Dahiya, S.; Sudhakar, K.; Kumari, U.; Sathasivam, K.; Meenakshi, D.U.; Wu, Y.S.; Sekar, M.; et al. Mesenchymal Stem Cell-Derived Extracellular Vesicles: Regenerative Potential and Challenges. Biology 2021, 10, 172. [Google Scholar] [CrossRef]
- Nakano, M.; Fujimiya, M. Potential effects of mesenchymal stem cell derived extracellular vesicles and exosomal miRNAs in neurological disorders. Neural Regen Res. 2021, 16, 2359–2366. [Google Scholar] [CrossRef]
- Yu-Taeger, L.; Stricker-Shaver, J.; Arnold, K.; Bambynek-Dziuk, P.; Novati, A.; Singer, E.; Lourhmati, A.; Fabian, C.; Magg, J.; Riess, O.; et al. Intranasal Administration of Mesenchymal Stem Cells Ameliorates the Abnormal Dopamine Transmission System and Inflammatory Reaction in the R6/2 Mouse Model of Huntington Disease. Cells 2019, 8, 595. [Google Scholar] [CrossRef] [Green Version]
- Sukhinich, K.K.; Namestnikova, D.D.; Gubskii, I.L.; Gabashvili, A.N.; Mel’nikov, P.A.; Vitushev, E.Y.; Vishnevskii, D.A.; Revkova, V.A.; Solov’eva, A.A.; Voitkovskaya, K.S.; et al. Distribution and Migration of Human Placental Mesenchymal Stromal Cells in the Brain of Healthy Rats after Stereotaxic or Intra-Arterial Transplantation. Bull. Exp. Biol. Med. 2020, 168, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Leong, K.H.; Zhou, L.L.; Lin, Q.M.; Wang, P.; Yao, L.; Huang, Z.T. Therapeutic effects of various methods of MSC transplantation on cerebral resuscitation following cardiac arrest in rats. Mol. Med. Rep. 2016, 13, 3043–3051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xin, H.; Li, Y.; Buller, B.; Katakowski, M.; Zhang, Y.; Wang, X.; Shang, X.; Zhang, Z.G.; Chopp, M. Exosome-mediated transfer of miR-133b from multipotent mesenchymal stromal cells to neural cells contributes to neurite outgrowth. Stem Cells 2012, 30, 1556–1564. [Google Scholar] [CrossRef] [Green Version]
- Han, M.; Cao, Y.; Xue, H.; Chu, X.; Li, T.; Xin, D.; Yuan, L.; Ke, H.; Li, G.; Wang, Z. Neuroprotective Effect of Mesenchymal Stromal Cell-Derived Extracellular Vesicles Against Cerebral Ischemia-Reperfusion-Induced Neural Functional Injury: A Pivotal Role for AMPK and JAK2/STAT3/NF-κB Signaling Pathway Modulation. Drug Des. Dev. Ther. 2020, 14, 2865–2876. [Google Scholar] [CrossRef]
- Jiang, M.; Wang, H.; Jin, M.; Yang, X.; Ji, H.; Jiang, Y.; Zhang, H.; Wu, F.; Wu, G.; Lai, X.; et al. Exosomes from MiR-30d-5p-ADSCs Reverse Acute Ischemic Stroke-Induced, Autophagy-Mediated Brain Injury by Promoting M2 Microglial/Macrophage Polarization. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2018, 47, 864–878. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhou, Y.; Li, H.; Wang, R.; Yang, D.; Li, B.; Fu, J. Intravenous administration of DPSCs and BDNF improves neurological performance in rats with focal cerebral ischemia. Int. J. Mol. Med. 2018, 41, 3185–3194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Xu, W.; Chen, H.; Li, S.; Dou, R.; Shen, H.; Liu, X.; Liu, X.; Hong, Y.; He, J. Comparison of the differentiation of dental pulp stem cells and periodontal ligament stem cells into neuron-like cells and their effects on focal cerebral ischemia. Acta Biochim. Biophys. Sin. 2020, 52, 1016–1029. [Google Scholar] [CrossRef]
- Lu, Y.; Zhou, Y.; Zhang, R.; Wen, L.; Wu, K.; Li, Y.; Yao, Y.; Duan, R.; Jia, Y. Bone Mesenchymal Stem Cell-Derived Extracellular Vesicles Promote Recovery Following Spinal Cord Injury via Improvement of the Integrity of the Blood-Spinal Cord Barrier. Front. Neurosci. 2019, 13, 209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Wen, L.L.; Li, Y.F.; Wu, K.M.; Duan, R.R.; Yao, Y.B.; Jing, L.J.; Gong, Z.; Teng, J.F.; Jia, Y.J. Exosomes derived from bone marrow mesenchymal stem cells protect the injured spinal cord by inhibiting pericyte pyroptosis. Neural Regen. Res. 2022, 17, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Jiao, G.; Wu, W.; Wang, H.; Ren, S.; Zhang, L.; Zhou, H.; Liu, H.; Chen, Y. Exosomes from Bone Marrow Mesenchymal Stem Cells Inhibit Neuronal Apoptosis and Promote Motor Function Recovery via the Wnt/β-catenin Signaling Pathway. Cell Transplant. 2019, 28, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Sisa, C.; Kholia, S.; Naylor, J.; Herrera Sanchez, M.B.; Bruno, S.; Deregibus, M.C.; Camussi, G.; Inal, J.M.; Lange, S.; Hristova, M. Mesenchymal Stromal Cell Derived Extracellular Vesicles Reduce Hypoxia-Ischaemia Induced Perinatal Brain Injury. Front. Physiol. 2019, 10, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomi, G.; Surbek, D.; Haesler, V.; Joerger-Messerli, M.; Schoeberlein, A. Exosomes derived from umbilical cord mesenchymal stem cells reduce microglia-mediated neuroinflammation in perinatal brain injury. Stem Cell Res. Ther. 2019, 10, 105. [Google Scholar] [CrossRef] [PubMed]
- Drommelschmidt, K.; Serdar, M.; Bendix, I.; Herz, J.; Bertling, F.; Prager, S.; Keller, M.; Ludwig, A.K.; Duhan, V.; Radtke, S.; et al. Mesenchymal stem cell-derived extracellular vesicles ameliorate inflammation-induced preterm brain injury. Brain Behav. Immun. 2017, 60, 220–232. [Google Scholar] [CrossRef] [Green Version]
- Bonafede, R.; Turano, E.; Scambi, I.; Busato, A.; Bontempi, P.; Virla, F.; Schiaffino, L.; Marzola, P.; Bonetti, B.; Mariotti, R. ASC-Exosomes Ameliorate the Disease Progression in SOD1(G93A) Murine Model Underlining Their Potential Therapeutic Use in Human ALS. Int J. Mol. Sci 2020, 21, 3651. [Google Scholar] [CrossRef]
- Corti, S.; Nizzardo, M.; Nardini, M.; Donadoni, C.; Salani, S.; Simone, C.; Falcone, M.; Riboldi, G.; Govoni, A.; Bresolin, N.; et al. Systemic transplantation of c-kit+ cells exerts a therapeutic effect in a model of amyotrophic lateral sclerosis. Hum. Mol. Genet. 2010, 19, 3782–3796. [Google Scholar] [CrossRef] [Green Version]
- Marconi, S.; Bonaconsa, M.; Scambi, I.; Squintani, G.M.; Rui, W.; Turano, E.; Ungaro, D.; D’Agostino, S.; Barbieri, F.; Angiari, S.; et al. Systemic treatment with adipose-derived mesenchymal stem cells ameliorates clinical and pathological features in the amyotrophic lateral sclerosis murine model. Neuroscience 2013, 248, 333–343. [Google Scholar] [CrossRef]
- Clark, K.; Zhang, S.; Barthe, S.; Kumar, P.; Pivetti, C.; Kreutzberg, N.; Reed, C.; Wang, Y.; Paxton, Z.; Farmer, D.; et al. Placental Mesenchymal Stem Cell-Derived Extracellular Vesicles Promote Myelin Regeneration in an Animal Model of Multiple Sclerosis. Cells 2019, 8, 1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riazifar, M.; Mohammadi, M.R.; Pone, E.J.; Yeri, A.; Lässer, C.; Segaliny, A.I.; McIntyre, L.L.; Shelke, G.V.; Hutchins, E.; Hamamoto, A.; et al. Stem Cell-Derived Exosomes as Nanotherapeutics for Autoimmune and Neurodegenerative Disorders. ACS Nano 2019, 13, 6670–6688. [Google Scholar] [CrossRef]
- Choi, H.S.; Kim, H.J.; Oh, J.H.; Park, H.G.; Ra, J.C.; Chang, K.A.; Suh, Y.H. Therapeutic potentials of human adipose-derived stem cells on the mouse model of Parkinson’s disease. Neurobiol. Aging 2015, 36, 2885–2892. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.H.; Salem, A.M.; Atta, H.M.; Eskandar, E.F.; Farrag, A.R.; Ghazy, M.A.; Salem, N.A.; Aglan, H.A. Updates in the pathophysiological mechanisms of Parkinson’s disease: Emerging role of bone marrow mesenchymal stem cells. World J. Stem Cells 2016, 8, 106–117. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Y.; Chopp, M.; Zhang, Z.G.; Mahmood, A.; Xiong, Y. Mesenchymal Stem Cell-Derived Exosomes Improve Functional Recovery in Rats After Traumatic Brain Injury: A Dose-Response and Therapeutic Window Study. Neurorehabil Neural Repair 2020, 34, 616–626. [Google Scholar] [CrossRef]
- Xu, H.; Jia, Z.; Ma, K.; Zhang, J.; Dai, C.; Yao, Z.; Deng, W.; Su, J.; Wang, R.; Chen, X. Protective effect of BMSCs-derived exosomes mediated by BDNF on TBI via miR-216a-5p. Med. Sci. Monit. 2020, 26, e920855. [Google Scholar] [CrossRef]
- Ruzicka, J.; Kulijewicz-Nawrot, M.; Rodrigez-Arellano, J.J.; Jendelova, P.; Sykova, E. Mesenchymal Stem Cells Preserve Working Memory in the 3xTg-AD Mouse Model of Alzheimer’s Disease. Int J. Mol. Sci. 2016, 17, 152. [Google Scholar] [CrossRef] [PubMed]
- Boutajangout, A.; Noorwali, A.; Atta, H.; Wisniewski, T. Human Umbilical Cord Stem Cell Xenografts Improve Cognitive Decline and Reduce the Amyloid Burden in a Mouse Model of Alzheimer’s Disease. Curr. Alzheimer Res. 2017, 14, 104–111. [Google Scholar] [CrossRef]
- Dey, N.D.; Bombard, M.C.; Roland, B.P.; Davidson, S.; Lu, M.; Rossignol, J.; Sandstrom, M.I.; Skeel, R.L.; Lescaudron, L.; Dunbar, G.L. Genetically engineered mesenchymal stem cells reduce behavioral deficits in the YAC 128 mouse model of Huntington’s disease. Behav. Brain Res. 2010, 214, 193–200. [Google Scholar] [CrossRef]
- Pollock, K.; Dahlenburg, H.; Nelson, H.; Fink, K.D.; Cary, W.; Hendrix, K.; Annett, G.; Torrest, A.; Deng, P.; Gutierrez, J.; et al. Human Mesenchymal Stem Cells Genetically Engineered to Overexpress Brain-derived Neurotrophic Factor Improve Outcomes in Huntington’s Disease Mouse Models. Mol. Ther. 2016, 24, 965–977. [Google Scholar] [CrossRef] [PubMed]
- Luzuriaga, J.; Polo, Y.; Pastor-Alonso, O.; Pardo-Rodríguez, B.; Larrañaga, A.; Unda, F.; Sarasua, J.R.; Pineda, J.R.; Ibarretxe, G. Advances and Perspectives in Dental Pulp Stem Cell Based Neuroregeneration Therapies. Int. J. Mol. Sci. 2021, 22, 3564. [Google Scholar] [CrossRef]
- Nagpal, A.; Kremer, K.L.; Hamilton-Bruce, M.A.; Kaidonis, X.; Milton, A.G.; Levi, C.; Shi, S.; Carey, L.; Hillier, S.; Rose, M.; et al. TOOTH (The Open study Of dental pulp stem cell Therapy in Humans): Study protocol for evaluating safety and feasibility of autologous human adult dental pulp stem cell therapy in patients with chronic disability after stroke. Int. J. Stroke Off. J. Int. Stroke Soc. 2016, 11, 575–585. [Google Scholar] [CrossRef]
- Chung, J.W.; Chang, W.H.; Bang, O.Y.; Moon, G.J.; Kim, S.J.; Kim, S.K.; Lee, J.S.; Sohn, S.I.; Kim, Y.H. Efficacy and Safety of Intravenous Mesenchymal Stem Cells for Ischemic Stroke. Neurology 2021, 96, e1012–e1023. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, A.; Kumaran, S.S.; Bhatia, R.; Mohanty, S.; Srivastava, M.V.P. Safety and Feasibility of Autologous Mesenchymal Stem Cell Transplantation in Chronic Stroke in Indian patients. A four-year follow up. J. Stem Cells Regen. Med. 2017, 13, 14–19. [Google Scholar] [CrossRef]
- Bhasin, A.; Srivastava, M.V.; Mohanty, S.; Bhatia, R.; Kumaran, S.S.; Bose, S. Stem cell therapy: A clinical trial of stroke. Clin. Neurol. Neurosurg. 2013, 115, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Honmou, O.; Houkin, K.; Matsunaga, T.; Niitsu, Y.; Ishiai, S.; Onodera, R.; Waxman, S.G.; Kocsis, J.D. Intravenous administration of auto serum-expanded autologous mesenchymal stem cells in stroke. Brain 2011, 134, 1790–1807. [Google Scholar] [CrossRef] [Green Version]
- Qiao, L.Y.; Huang, F.J.; Zhao, M.; Xie, J.H.; Shi, J.; Wang, J.; Lin, X.Z.; Zuo, H.; Wang, Y.L.; Geng, T.C. A two-year follow-up study of cotransplantation with neural stem/progenitor cells and mesenchymal stromal cells in ischemic stroke patients. Cell Transplant. 2014, 23, S65–S72. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Zhu, W.; Zhu, J.; Wu, L.; Xu, G.; Liu, X. Feasibility of delivering mesenchymal stem cells via catheter to the proximal end of the lesion artery in patients with stroke in the territory of the middle cerebral artery. Cell Transplant. 2013, 22, 2291–2298. [Google Scholar] [CrossRef] [PubMed]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Aguayo, C.; Bonilla, C.; Marin, E.; Tapiador, N.; Sevilla, M.; Vazquez, D.; Carballido, J.; et al. Intrathecal administration of autologous mesenchymal stromal cells for spinal cord injury: Safety and efficacy of the 100/3 guideline. Cytotherapy 2018, 20, 806–819. [Google Scholar] [CrossRef] [PubMed]
- Hur, J.W.; Cho, T.H.; Park, D.H.; Lee, J.B.; Park, J.Y.; Chung, Y.G. Intrathecal transplantation of autologous adipose-derived mesenchymal stem cells for treating spinal cord injury: A human trial. J. Spinal Cord Med. 2016, 39, 655–664. [Google Scholar] [CrossRef]
- Xiao, Z.; Tang, F.; Zhao, Y.; Han, G.; Yin, N.; Li, X.; Chen, B.; Han, S.; Jiang, X.; Yun, C.; et al. Significant Improvement of Acute Complete Spinal Cord Injury Patients Diagnosed by a Combined Criteria Implanted with NeuroRegen Scaffolds and Mesenchymal Stem Cells. Cell Transplant. 2018, 27, 907–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.K.; Choi, K.H.; Yoo, J.Y.; Kim, D.Y.; Kim, S.J.; Jeon, S.R. A Phase III Clinical Trial Showing Limited Efficacy of Autologous Mesenchymal Stem Cell Therapy for Spinal Cord Injury. Neurosurgery 2016, 78, 436–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Aguayo, C.; Fernandez, C.; Rodriguez-Boto, G.; Marin, E.; Tapiador, N.; Sevilla, M.; Carballido, J.; et al. Cell therapy with autologous mesenchymal stromal cells in post-traumatic syringomyelia. Cytotherapy 2018, 20, 796–805. [Google Scholar] [CrossRef]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Bonilla, C.; Aguayo, C.; Fernández, C.; Tapiador, N.; Sevilla, M.; Morejón, C.; Montilla, J.; et al. Repeated subarachnoid administrations of autologous mesenchymal stromal cells supported in autologous plasma improve quality of life in patients suffering incomplete spinal cord injury. Cytotherapy 2017, 19, 349–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satti, H.S.; Waheed, A.; Ahmed, P.; Ahmed, K.; Akram, Z.; Aziz, T.; Satti, T.M.; Shahbaz, N.; Khan, M.A.; Malik, S.A. Autologous mesenchymal stromal cell transplantation for spinal cord injury: A Phase I pilot study. Cytotherapy 2016, 18, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, M.V.; Larocca, T.F.; de Freitas Souza, B.S.; Villarreal, C.F.; Silva, L.F.; Matos, A.C.; Novaes, M.A.; Bahia, C.M.; de Oliveira Melo Martinez, A.C.; Kaneto, C.M.; et al. Safety and neurological assessments after autologous transplantation of bone marrow mesenchymal stem cells in subjects with chronic spinal cord injury. Stem Cell Res. Ther. 2014, 5, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, H.; Liu, X.; Hua, R.; Dai, G.; Wang, X.; Gao, J.; An, Y. Clinical observation of umbilical cord mesenchymal stem cell transplantation in treatment for sequelae of thoracolumbar spinal cord injury. J. Transl. Med. 2014, 12, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, G.; Liu, X.; Zhang, Z.; Yang, Z.; Dai, Y.; Xu, R. Transplantation of autologous bone marrow mesenchymal stem cells in the treatment of complete and chronic cervical spinal cord injury. Brain Res. 2013, 1533, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Karamouzian, S.; Nematollahi-Mahani, S.N.; Nakhaee, N.; Eskandary, H. Clinical safety and primary efficacy of bone marrow mesenchymal cell transplantation in subacute spinal cord injured patients. Clin. Neurol. Neurosurg. 2012, 114, 935–939. [Google Scholar] [CrossRef]
- Huang, L.; Zhang, C.; Gu, J.; Wu, W.; Shen, Z.; Zhou, X.; Lu, H. A Randomized, Placebo-Controlled Trial of Human Umbilical Cord Blood Mesenchymal Stem Cell Infusion for Children With Cerebral Palsy. Cell Transplant. 2018, 27, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Fu, X.; Dai, G.; Wang, X.; Zhang, Z.; Cheng, H.; Zheng, P.; An, Y. Comparative analysis of curative effect of bone marrow mesenchymal stem cell and bone marrow mononuclear cell transplantation for spastic cerebral palsy. J. Transl. Med. 2017, 15, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, J.; Huang, L.; Zhang, C.; Wang, Y.; Zhang, R.; Tu, Z.; Wang, H.; Zhou, X.; Xiao, Z.; Liu, Z.; et al. Therapeutic evidence of umbilical cord-derived mesenchymal stem cell transplantation for cerebral palsy: A randomized, controlled trial. Stem Cell Res. Ther. 2020, 11, 43. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.Y.; Chang, Y.S.; Sung, S.I.; Park, W.S. Mesenchymal Stem Cells for Severe Intraventricular Hemorrhage in Preterm Infants: Phase I Dose-Escalation Clinical Trial. Stem Cells Transl. Med. 2018, 7, 847–856. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Hu, H.; Hua, R.; Yang, J.; Zheng, P.; Niu, X.; Cheng, H.; Dai, G.; Liu, X.; Zhang, Z.; et al. Effect of umbilical cord mesenchymal stromal cells on motor functions of identical twins with cerebral palsy: Pilot study on the correlation of efficacy and hereditary factors. Cytotherapy 2015, 17, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cheng, H.; Hua, R.; Yang, J.; Dai, G.; Zhang, Z.; Wang, R.; Qin, C.; An, Y. Effects of bone marrow mesenchymal stromal cells on gross motor function measure scores of children with cerebral palsy: A preliminary clinical study. Cytotherapy 2013, 15, 1549–1562. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.D.; Cudkowicz, M.E.; Windebank, A.J.; Staff, N.P.; Owegi, M.; Nicholson, K.; McKenna-Yasek, D.; Levy, Y.S.; Abramov, N.; Kaspi, H.; et al. NurOwn, phase 2, randomized, clinical trial in patients with ALS: Safety, clinical, and biomarker results. Neurology 2019, 93, e2294–e2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrou, P.; Gothelf, Y.; Argov, Z.; Gotkine, M.; Levy, Y.S.; Kassis, I.; Vaknin-Dembinsky, A.; Ben-Hur, T.; Offen, D.; Abramsky, O.; et al. Safety and Clinical Effects of Mesenchymal Stem Cells Secreting Neurotrophic Factor Transplantation in Patients With Amyotrophic Lateral Sclerosis: Results of Phase 1/2 and 2a Clinical Trials. JAMA Neurol. 2016, 73, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Syková, E.; Rychmach, P.; Drahorádová, I.; Konrádová, Š.; Růžičková, K.; Voříšek, I.; Forostyak, S.; Homola, A.; Bojar, M. Transplantation of Mesenchymal Stromal Cells in Patients With Amyotrophic Lateral Sclerosis: Results of Phase I/IIa Clinical Trial. Cell Transplant. 2017, 26, 647–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.W.; Moon, C.; Kim, H.Y.; Oh, S.I.; Park, J.; Lee, J.H.; Chang, I.Y.; Kim, K.S.; Kim, S.H. Phase I trial of repeated intrathecal autologous bone marrow-derived mesenchymal stromal cells in amyotrophic lateral sclerosis. Stem Cells Transl. Med. 2015, 4, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Staff, N.P.; Madigan, N.N.; Morris, J.; Jentoft, M.; Sorenson, E.J.; Butler, G.; Gastineau, D.; Dietz, A.; Windebank, A.J. Safety of intrathecal autologous adipose-derived mesenchymal stromal cells in patients with ALS. Neurology 2016, 87, 2230–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rushkevich, Y.N.; Kosmacheva, S.M.; Zabrodets, G.V.; Ignatenko, S.I.; Goncharova, N.V.; Severin, I.N.; Likhachev, S.A.; Potapnev, M.P. The Use of Autologous Mesenchymal Stem Cells for Cell Therapy of Patients with Amyotrophic Lateral Sclerosis in Belarus. Bull. Exp. Biol. Med. 2015, 159, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Kim, H.; Oh, K.W.; Oh, S.I.; Koh, S.H.; Baik, W.; Noh, M.Y.; Kim, K.S.; Kim, S.H. Biological markers of mesenchymal stromal cells as predictors of response to autologous stem cell transplantation in patients with amyotrophic lateral sclerosis: An investigator-initiated trial and in vivo study. Stem Cells 2014, 32, 2724–2731. [Google Scholar] [CrossRef]
- Mazzini, L.; Mareschi, K.; Ferrero, I.; Miglioretti, M.; Stecco, A.; Servo, S.; Carriero, A.; Monaco, F.; Fagioli, F. Mesenchymal stromal cell transplantation in amyotrophic lateral sclerosis: A long-term safety study. Cytotherapy 2012, 14, 56–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrou, P.; Kassis, I.; Levin, N.; Paul, F.; Backner, Y.; Benoliel, T.; Oertel, F.C.; Scheel, M.; Hallimi, M.; Yaghmour, N.; et al. Beneficial effects of autologous mesenchymal stem cell transplantation in active progressive multiple sclerosis. Brain 2020, 143, 3574–3588. [Google Scholar] [CrossRef] [PubMed]
- Riordan, N.H.; Morales, I.; Fernández, G.; Allen, N.; Fearnot, N.E.; Leckrone, M.E.; Markovich, D.J.; Mansfield, D.; Avila, D.; Patel, A.N.; et al. Clinical feasibility of umbilical cord tissue-derived mesenchymal stem cells in the treatment of multiple sclerosis. J. Transl. Med. 2018, 16, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández, O.; Izquierdo, G.; Fernández, V.; Leyva, L.; Reyes, V.; Guerrero, M.; León, A.; Arnaiz, C.; Navarro, G.; Páramo, M.D.; et al. Adipose-derived mesenchymal stem cells (AdMSC) for the treatment of secondary-progressive multiple sclerosis: A triple blinded, placebo controlled, randomized phase I/II safety and feasibility study. PLoS ONE 2018, 13, e0195891. [Google Scholar] [CrossRef] [Green Version]
- Harris, V.K.; Stark, J.; Vyshkina, T.; Blackshear, L.; Joo, G.; Stefanova, V.; Sara, G.; Sadiq, S.A. Phase I Trial of Intrathecal Mesenchymal Stem Cell-derived Neural Progenitors in Progressive Multiple Sclerosis. EBioMedicine 2018, 29, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Dahbour, S.; Jamali, F.; Alhattab, D.; Al-Radaideh, A.; Ababneh, O.; Al-Ryalat, N.; Al-Bdour, M.; Hourani, B.; Msallam, M.; Rasheed, M.; et al. Mesenchymal stem cells and conditioned media in the treatment of multiple sclerosis patients: Clinical, ophthalmological and radiological assessments of safety and efficacy. CNS Neurosci. Ther. 2017, 23, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Llufriu, S.; Sepúlveda, M.; Blanco, Y.; Marín, P.; Moreno, B.; Berenguer, J.; Gabilondo, I.; Martínez-Heras, E.; Sola-Valls, N.; Arnaiz, J.A.; et al. Randomized placebo-controlled phase II trial of autologous mesenchymal stem cells in multiple sclerosis. PLoS ONE 2014, 9, e113936. [Google Scholar] [CrossRef] [PubMed]
- Li, J.F.; Zhang, D.J.; Geng, T.; Chen, L.; Huang, H.; Yin, H.L.; Zhang, Y.Z.; Lou, J.Y.; Cao, B.; Wang, Y.L. The potential of human umbilical cord-derived mesenchymal stem cells as a novel cellular therapy for multiple sclerosis. Cell Transplant. 2014, 23, S113–S122. [Google Scholar] [CrossRef]
- Bonab, M.M.; Sahraian, M.A.; Aghsaie, A.; Karvigh, S.A.; Hosseinian, S.M.; Nikbin, B.; Lotfi, J.; Khorramnia, S.; Motamed, M.R.; Togha, M.; et al. Autologous mesenchymal stem cell therapy in progressive multiple sclerosis: An open label study. Curr. Stem Cell Res. Ther. 2012, 7, 407–414. [Google Scholar] [CrossRef]
- Lee, P.H.; Lee, J.E.; Kim, H.S.; Song, S.K.; Lee, H.S.; Nam, H.S.; Cheong, J.W.; Jeong, Y.; Park, H.J.; Kim, D.J.; et al. A randomized trial of mesenchymal stem cells in multiple system atrophy. Ann. Neurol. 2012, 72, 32–40. [Google Scholar] [CrossRef]
- Connick, P.; Kolappan, M.; Crawley, C.; Webber, D.J.; Patani, R.; Michell, A.W.; Du, M.Q.; Luan, S.L.; Altmann, D.R.; Thompson, A.J.; et al. Autologous mesenchymal stem cells for the treatment of secondary progressive multiple sclerosis: An open-label phase 2a proof-of-concept study. Lancet Neurol 2012, 11, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Canesi, M.; Giordano, R.; Lazzari, L.; Isalberti, M.; Isaias, I.U.; Benti, R.; Rampini, P.; Marotta, G.; Colombo, A.; Cereda, E.; et al. Finding a new therapeutic approach for no-option Parkinsonisms: Mesenchymal stromal cells for progressive supranuclear palsy. J. Transl. Med. 2016, 14, 127. [Google Scholar] [CrossRef] [Green Version]
- Carstens, M.; Haq, I.; Martinez-Cerrato, J.; Dos-Anjos, S.; Bertram, K.; Correa, D. Sustained clinical improvement of Parkinson’s disease in two patients with facially-transplanted adipose-derived stromal vascular fraction cells. J. Clin. Neurosci. 2020, 81, 47–51. [Google Scholar] [CrossRef]
- Wang, S.; Cheng, H.; Dai, G.; Wang, X.; Hua, R.; Liu, X.; Wang, P.; Chen, G.; Yue, W.; An, Y. Umbilical cord mesenchymal stem cell transplantation significantly improves neurological function in patients with sequelae of traumatic brain injury. Brain Res. 2013, 1532, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Tian, C.; Wang, X.; Wang, X.; Wang, L.; Wang, X.; Wu, S.; Wan, Z. Autologous bone marrow mesenchymal stem cell therapy in the subacute stage of traumatic brain injury by lumbar puncture. Exp. Clin. Transplant. 2013, 11, 176–181. [Google Scholar] [CrossRef] [Green Version]
- Lo Furno, D.; Mannino, G.; Giuffrida, R. Functional role of mesenchymal stem cells in the treatment of chronic neurodegenerative diseases. J. Cell. Physiol. 2018, 233, 3982–3999. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.M.; Dawson, G.; Franz, L.; Howard, J.; McLaughlin, C.; Kistler, B.; Waters-Pick, B.; Meadows, N.; Troy, J.; Kurtzberg, J. Infusion of human umbilical cord tissue mesenchymal stromal cells in children with autism spectrum disorder. Stem Cells Transl. Med. 2020, 9, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Nooshabadi, V.T.; Mardpour, S.; Yousefi-Ahmadipour, A.; Allahverdi, A.; Izadpanah, M.; Daneshimehr, F.; Ai, J.; Banafshe, H.R.; Ebrahimi-Barough, S. The extracellular vesicles-derived from mesenchymal stromal cells: A new therapeutic option in regenerative medicine. J. Cell. Biochem. 2018, 119, 8048–8073. [Google Scholar] [CrossRef]
- Shekari, F.; Nazari, A.; Assar Kashani, S.; Hajizadeh-Saffar, E.; Lim, R.; Baharvand, H. Pre-clinical investigation of mesenchymal stromal cell-derived extracellular vesicles: A systematic review. Cytotherapy 2021, 23, 277–284. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Disease | Source | Number | Mean Age (Range), Year | Route of Administration | Number of Cells | Number of Treatments | Results | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|
| Trial | Control | |||||||||
| Chung et al. [48] | Ischemic stroke (Phase 3) | BM | 39 | 15 | 68 (28–83) | IV | 1 × 106/kg | 1 | Lower extremity motor functional recovery after 3 months | No |
| Bhasin et al. [49] | Ischemic stroke | BM | 6 | 6 | 42.8 (20–60) | IV | 5–6 × 107 cells | 1 | Improvement in the activities of daily living (ADL) after 156 and 208 weeks | No |
| Qiao et al. [52] | Ischemic stroke (Phase 1/2) | UC | 6 | 0 | 56.17 (3–85) | IVIV + IC | IV:MSC 0.5 × 106/kg IC:MSC 5 × 106 cells NSPC 6 × 106 cells at one-week interval | 4 or 1 + 3 | Improvement in the neurological functions and ADL after 3, 12, 24 months | Fever, dizziness |
| Jiang et al. [53] | Ischemic and hemorrhagic stroke | UC | 4 | 0 | 40–59 | IA (intra-arterial) via catheterization | 2 × 107 cells | 1 | Motor functional recovery and improvement in the ADL after 3 and 6 months | No |
| Bhasin et al. [50] | Ischemic stroke | BM | 20 MSC6 MNC14 | 20 | 45.1 | IV | 5–6 × 107 cells | 1 | Improvement in the ADL after 8 and 24 weeks | No |
| Honmou et al. [51] | Ischemic stroke (Phase 1) | BM | 12 | 0 | 59.2 (41–73) | IV | 0.6–1.8 × 108 cells | 1 | Incremental daily rate of change in the disability scales during 12 months | Fever, nausea, itching |
| Reference | Disease | Source | Number | Mean Age (Range), Year | Route of Administration | Number of Cells | Number of Treatments | Results | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|
| Trial | Control | |||||||||
| Xiao et al. [56] | Spinal cord injury (Phase 1) | UCB | 2 | 0 | 28, 30 | Transplantation into the lesion with collagen scaffolds | 4 × 107 cells | 1 | Motor functional recovery after 3, 6, 12 months Sensory functional recovery after 2, 4, 12 months | No |
| Vaquero et al. [54] | Spinal cord injury (Phase 2) | BM | 11 | 0 | 44.91 (28–62) | IT | 100 × 106 cells at 3 months interval | 3 | Motor, sensory and bladder–bowel functional recovery after 4, 7, 10 months | No |
| Vaquero et al. [58] | Post-traumatic syringomyelia (Phase 2) | BM | 6 | 0 | 39 (30–50) | Direct injection into the lesion | 300 × 106 cells | 1 | Achieving reduction of syrinx and valiable clinical improvements after 6 months | No |
| Vaquero et al. [59] | Spinal cord injury (Phase 2) | BM | 10 | 0 | 42.2 (34–59) | IT | 30 × 106 cells at 3-months interval | 4 | Motor, sensory and bladder–bowel functional recovery after 3, 6, 9, 12 months | Headache, puncture pain |
| Satti et al. [60] | Spinal cord injury (Phase 1) | BM | 9 | 0 | 31.6 (24–38) | IT | 1.2 × 106/kg at 4 weeks interval | 2 or 3 | Only safety assessment | No |
| Oh et al. [57] | Spinal cord injury (Phase 3) | BM | 16 | 0 | 40.9 (18–65) | Direct injection into the lesion + IT | 1.6 × 107 cells 3.2 × 107 cells | 1 | Very weak therapeutic efficacy after 6 months | Sensory deterioration, muscle rigidity, tingling sense |
| Hur et al. [55] | Spinal cord injury (Phase 1) | AD | 14 | 0 | 41.9 (20–66) | IT | 3 × 107 at 1-month interval | 3 | Motor and sensory functional recovery after 8 months | Nausea, vomit, headache |
| Mendonça et al. [61] | Spinal cord injury (Phase 1) | BM | 14 | 0 | 35.7 (23–61) | Direct injection into the lesion | 5 × 106 cells/cm3 per lesion volume | 1 | Motor, sensory, and bladder–bowel functional recovery after 6 months | Low-intensity pain at the incision site, cerebrospinal fluid leak |
| Cheng et al. [62] | Spinal cord injury (Phase 2) | UC | 10 | 34 | 35.3 (19–57) | Direct injection into the lesion | 2 × 107 cells at 10 days interval | 2 | Motor, sensory, and bladder functional recovery after 6 months Superior efficacy than that of rehabilitation therapy | Radiating neuralgia |
| Dai et al. [63] | Spinal cord injury (Phase 1/2) | BM | 20 | 20 | 22–54 | Direct injection into the lesion | 20 × 106 cells | 1 | Motor, sensory, and bladder functional recovery after 6 months | Fever, headache, pain |
| Karamouzian et al. [64] | Spinal cord injury (Phase 1/2) | BM | 11 | 20 | 33.2 (23–48) | IT | 0.7–1.2 × 106 cells | 1 | Possible efficacy in the motor and sensory function | No |
| Reference | Disease | Source | Number | Mean Age (Range), Year | Route of Administration | Number of Cells | Number of Treatments | Results | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|
| Trial | Control | |||||||||
| Gu et al. [67] | Cerebral palsy (Phase 1/2) | UC | 19 | 20 | 4.29 | IV | 4.5–5.5 × 107 cells at 7-day intervals | 4 | Gross motor and comprehensive functional recovery and improvement in the ADL after 3, 6, 12 months | No |
| Ahn et al. [68] | Intraventricular hemorrhage (Phase 1) | UCB | 9 | 0 | 11.6 (7–15) (days) | Intraventricular | 5 × 106/kg or 1 × 107/kg | 1 | Only safety assessment | No |
| Huang et al. [65] | Cerebral palsy (Phase 1/2) | UCB | 27 | 27 | 7.4 (3–12) | IV | 5 × 107 cells at 7-day intervals | 4 | Gross motor and comprehensive functional recovery after 3, 6, 12, 24 months | No |
| Liu et al. [66] | Cerebral palsy (Phase 1/2) | BM | MSC 33 MNC34 | 35 | 7–132 (months) | IT | 1 × 106/kg at 3–4-day intervals | 4 | Motor functional recovery after 12 months | No |
| Wang et al. [69] | Cerebral palsy (Phase 4) | UC | 16 (8 twins) | 0 | 6.29 (3–12) | IT | 1–2 × 106 cells at 3–5-day intervals | 4 | Motor functional recovery after 1 and 6 months | No |
| Wang X et al. [70] | Cerebral palsy | BM | 46 | 0 | 6–180 (months) | IT Intra-Parenchymal | 2 × 107 cells 4 × 107 cells at 5-day intervals | 2 + 1 or 4 | Gross motor functional recovery after 1, 6, 18 months | No |
| Reference | Disease | Source | Number | Mean Age (Range), Year | Route of Administration | Number of Cells | Number of Treatments | Results | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|
| Trial | Control | |||||||||
| Berry et al. [71] | ALS (Phase 2) | BM-NTF | 36 | 12 | 51.1 (26–71) | IM + IT | IM: 48 × 106 cells IT: 125 × 106 cells | 1 | Improvement in the rate of disease progression after 6 months | Headache, fever, back pain, injection site bruising |
| Syková et al. [73] | ALS (Phase 1/2) | BM | 26 | 0 | 51.2 (33–64) | IT | 15 ± 4.5 × 106 cells | 1 | Slowing down of the diseaseprogression after 3, 6, 9 months | Headache |
| Staff et al. [75] | ALS (Phase 1) | AD | 27 | 0 | 36–75 | IT | 1 × 107, 5 × 107, 5 × 107 × 2, 1 × 108, 1 × 108 × 2 | 1 or 2 | Only safety assessment | Temporary back and leg pain in the highest dose |
| Petrou et al. [72] | ALS (Phase 1/2) | BM-NTF | 26 | 0 | 48.1, 50.8 (23–65) | IM IT IM + IT | IM: 2.4–4.8 × 107 cells IT: 1.0–2.0 × 106 /kg | 1 | Improvement in the rate of disease progression after 6 months | Fever, vomiting, headache |
| Rushkevich et al. [76] | ALS | BM-MSC and neural induced MSC | 10 | 15 | 54.5, 55.0 (37–66) | IV + IT | 0.5–1.5 × 106/kg 5.0–9.7 × 106 cells at 5–7-month intervals | 1 or 2 | Slowing down of the disease progression after 12 months | Fever, headache |
| Oh et al. [74] | ALS (Phase 1) | BM | 8 | 0 | 45.7 (29–62) | IT | 1 × 106/kg at 26-day intervals | 2 | No efficacy after 6 months | Fever, pain, headache |
| Kim et al. [77] | ALS | BM | 37 | 0 | 52.7, 48.8 | IT | 1 × 106/kg at one-month intervals | 2 | Trophic factors associated with a positive response to treat | No |
| Mazzini et al. [78] | ALS (Phase 1) | BM | 19 | 0 | 20–75 | Direct injection into spinal cord | 7–152 × 106 cells | 1 | No long-term adverse effect after nearly 9 years | No |
| Reference | Disease | Source | Number | Mean Age (Range), Year | Route of Administration | Number of Cells | Number of Treatments | Results | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|
| Trial | Control | |||||||||
| Petrou et al. [79] | Multiple sclerosis (Phase 2) | BM | 16, 16 | 16 | 47.6 (37.9–57.3) | IT or IV | 1 × 106/kg at 6-month intervals | 1 or 2 | Improvement in the course of the disease and comprehensive functional recovery after 3, 6, 12 months. IT is more efficacious than IV | No |
| Fernández et al. [81] | Multiple sclerosis (phase 1/2) | AD | 10, 9 | 11 | 44.8 47.8 46.3 | IV | 1 × 106/kg or 4 × 106/kg | 1 | Partial efficacy in the imaging studies and evoked potentials after 12 months | urinary infection |
| Riordan et al. [80] | Multiple sclerosis (phase 1/2) | UC | 20 | 0 | 41.15 | IV | 20 × 106 cells at 1–4-day intervals | 7 | Comprehensive functional recovery after one month | Headache, fatigue |
| Harris et al. [82] | Multiple sclerosis (Phase 1) | BM MSC -derived neural progenitors | 20 | 0 | 27–65 | IT | 5.3–10 × 106 cells at 3-month intervals | 3 | Motor, bladder and comprehensive functional recovery after 3 months | headache, fever |
| Dahbour et al. [83] | Multiple sclerosis (Phase 1/2) | BM MSC-CM | 10 | 0 | 34.9 (18–54) | IT | 93–168 × 106 cells CM:13–20 mL at 1-month intervals | 1 + 1 | Comprehensive functional recovery after 12 months | Pain, headache, fever |
| Llufriu et al. [84] | Multiple sclerosis (Phase 2) | BM | 9 | 0 | 36.8 (23–48) | IV | 1–2 × 106/kg | 1 | Improvement in the imaging studies after 6 months | No |
| Li et al. [85] | Multiple sclerosis | UC | 13 | 10 | 41.7, 39.4 | IV | 4 × 106 cells/kg at 2-week intervals | 3 | Improvement in the overall symptoms and fewer incidences of relapse during 12 months | No |
| Bonab et al. [86] | Multiple sclerosis (Phase 2) | BM | 25 | 0 | 34.7 (23–50) | IT | 2.95 × 107 cells | 1 | Improvement or stabilization in the course of the disease during 12 months | Fever, nausea, weakness in the lower limbs, headache |
| Lee et al. [87] | Multiple sclerosis (Phase 2) | BM | 16 | 17 | 56.1, 55.8 | IA (intra-arterial) + IV | IA: 4 × 107 cells IV: 4 × 107 cells at 30-day intervals | 1 + 3 | Efficacy in preventing the progression of neurological deficits during 12 months | Small ischemic lesions |
| Connick et al. [88] | Multiple sclerosis (Phase 2) | BM | 10 | 0 | 48.8 (40–53) | IV | 1.6 × 106/kg | 1 | Visual functional recovery after 10 months | Macular rash, self-limiting infections |
| Reference | Disease | Source | Number | Mean Age (Range), Year | Route of Administration | Number of Cells | Number of Treatments | Results | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|
| Trial | Control | |||||||||
| Canesi et al. [89] | Progressive supranuclear palsy (Phase 1) | BM | 5 | 0 | 60–68 | IA (intra-arterial) via catheterization | 1.7 (1.2–2.0) × 106/kg | 1 | Clinical stabilization for at least 6 months during the one-year follow-up | Transient left hemiparesis |
| Carstens et al. [90] | Parkinson’s disease (Case studies) | AD MSC-derived stromal vascular fraction | 2 | 0 | 72, 50 | Facial and nasal transplantation | 6.0 × 107 cells | 1 | Subjective functional recovery after 2 weeks and up to 5 years | No |
| Reference | Disease | Source | Number | Mean Age (Range), Year | Route of Administration | Number of Cells | Number of Treatments | Results | Adverse Events | |
|---|---|---|---|---|---|---|---|---|---|---|
| Trial | Control | |||||||||
| Wang et al. [91] | Traumatic brain injury (Phase 2) | UC | 20 | 20 | 27.5 ± 9.4 28.6 ± 10.1 | IT | 6.0 × 107 cells | 4 | Comprehensive functional recovery and improvement in the ADL after 6 months | Mild dizziness, headache |
| Tian et al. [92] | Traumatic brain injury | BM | 97 | 0 | - | IT | 3.0–5.0 × 106 cells | 1 | Improvement of consciousness and motor function after 14 days | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mukai, T.; Sei, K.; Nagamura-Inoue, T. Mesenchymal Stromal Cells Perspective: New Potential Therapeutic for the Treatment of Neurological Diseases. Pharmaceutics 2021, 13, 1159. https://doi.org/10.3390/pharmaceutics13081159
Mukai T, Sei K, Nagamura-Inoue T. Mesenchymal Stromal Cells Perspective: New Potential Therapeutic for the Treatment of Neurological Diseases. Pharmaceutics. 2021; 13(8):1159. https://doi.org/10.3390/pharmaceutics13081159
Chicago/Turabian StyleMukai, Takeo, Kenshi Sei, and Tokiko Nagamura-Inoue. 2021. "Mesenchymal Stromal Cells Perspective: New Potential Therapeutic for the Treatment of Neurological Diseases" Pharmaceutics 13, no. 8: 1159. https://doi.org/10.3390/pharmaceutics13081159
APA StyleMukai, T., Sei, K., & Nagamura-Inoue, T. (2021). Mesenchymal Stromal Cells Perspective: New Potential Therapeutic for the Treatment of Neurological Diseases. Pharmaceutics, 13(8), 1159. https://doi.org/10.3390/pharmaceutics13081159