
SonoVue® vs. Sonazoid™ vs. Optison™: Which Bubble Is Best for Low-Intensity Sonoporation of Pancreatic Ductal Adenocarcinoma?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Microbubble Characterization
2.1.1. Reconstitution of Microbubbles
2.1.2. Size, Concentration and in Vial Stability
2.1.3. Attenuation Measurements
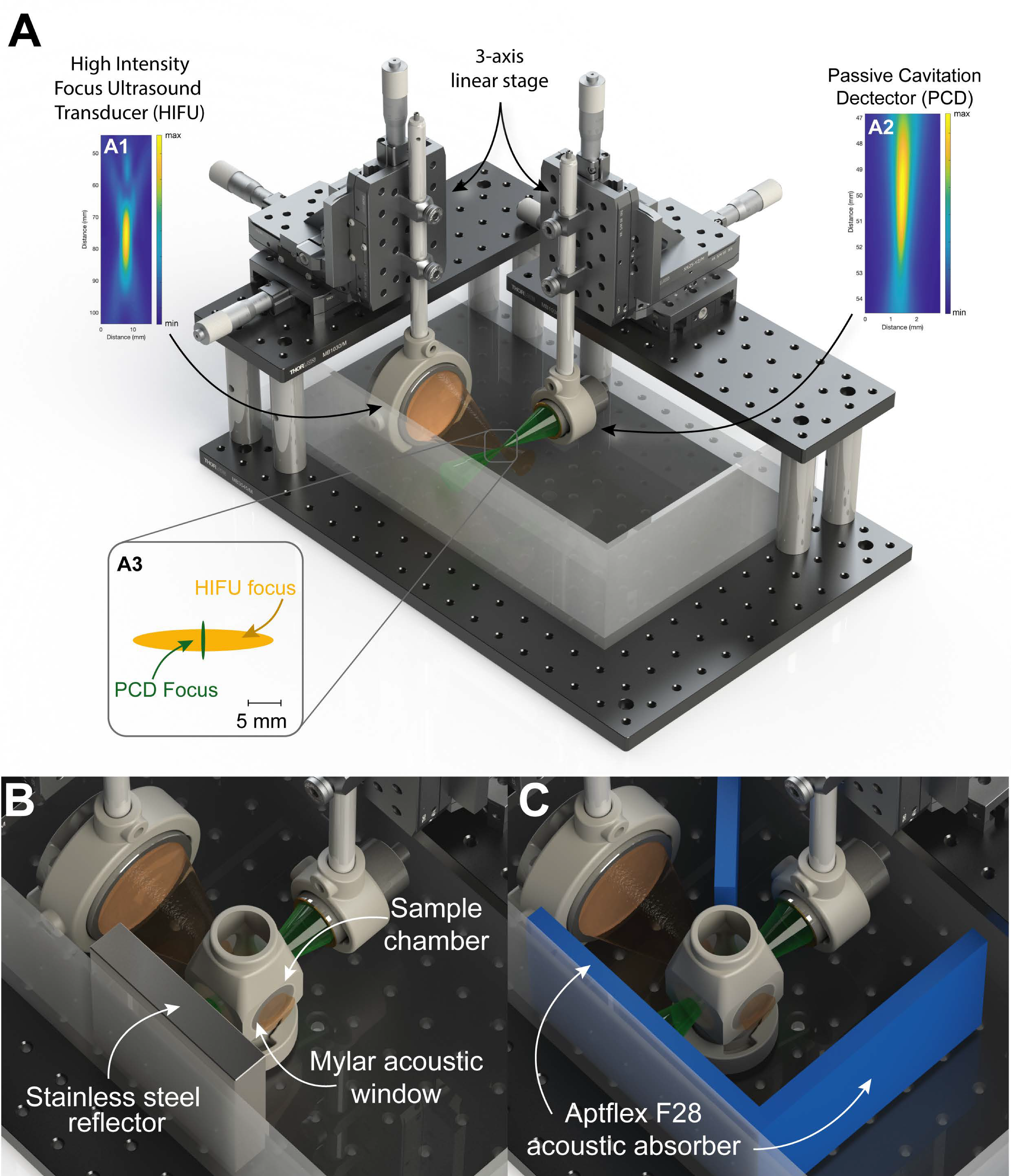
2.1.4. Stable to Inertial Cavitation Transition
2.2. Simulations
2.2.1. Microbubble Pharmacokinetics
2.2.2. Simulated Microbubble Behavior
2.3. In Vitro Cell Experiments
2.3.1. Chemicals
2.3.2. Cell Culture
2.3.3. Microbubble Dilution
2.3.4. In Vitro Sonoporation
2.3.5. Flow Cytometry
2.4. Pre-Clinical Mouse Experiments
2.4.1. Optical Imaging
2.4.2. Ultrasound Imaging
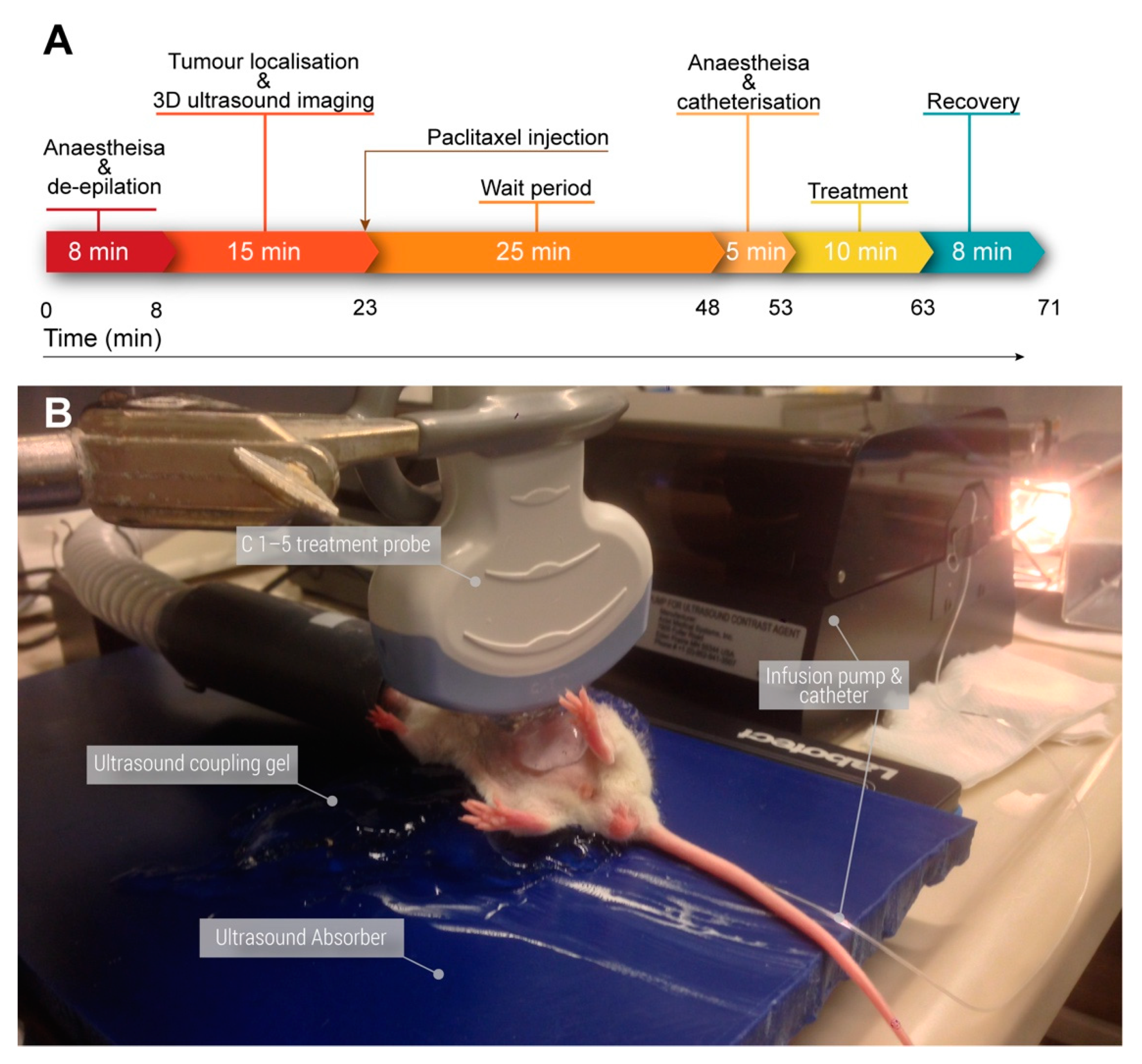
2.4.3. Ultrasound Treatment
2.4.4. Ultrasound Treatment Settings
2.4.5. Tumor Measurements
2.5. Statistical Analysis
3. Results
3.1. Microbubble Characterization
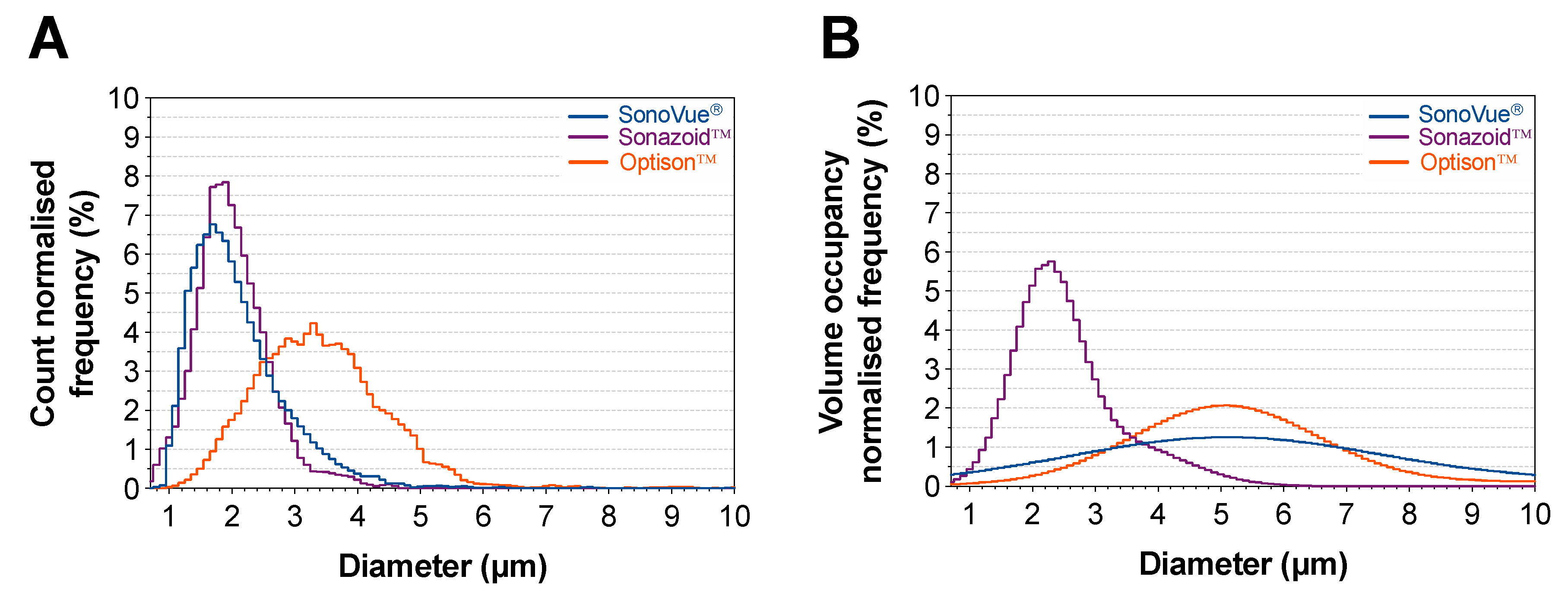
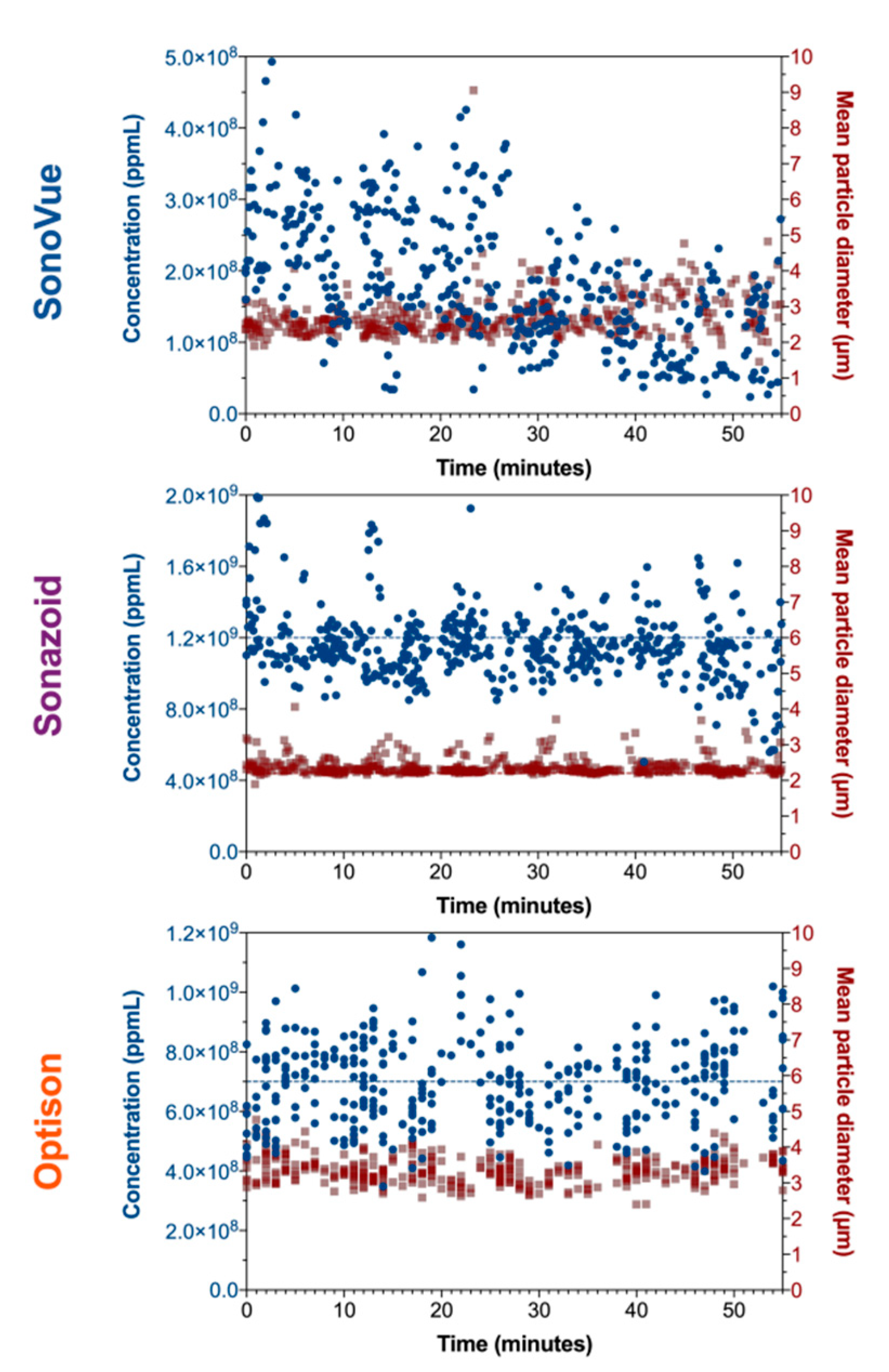
3.1.1. Size, Concentration and in Vial Stability
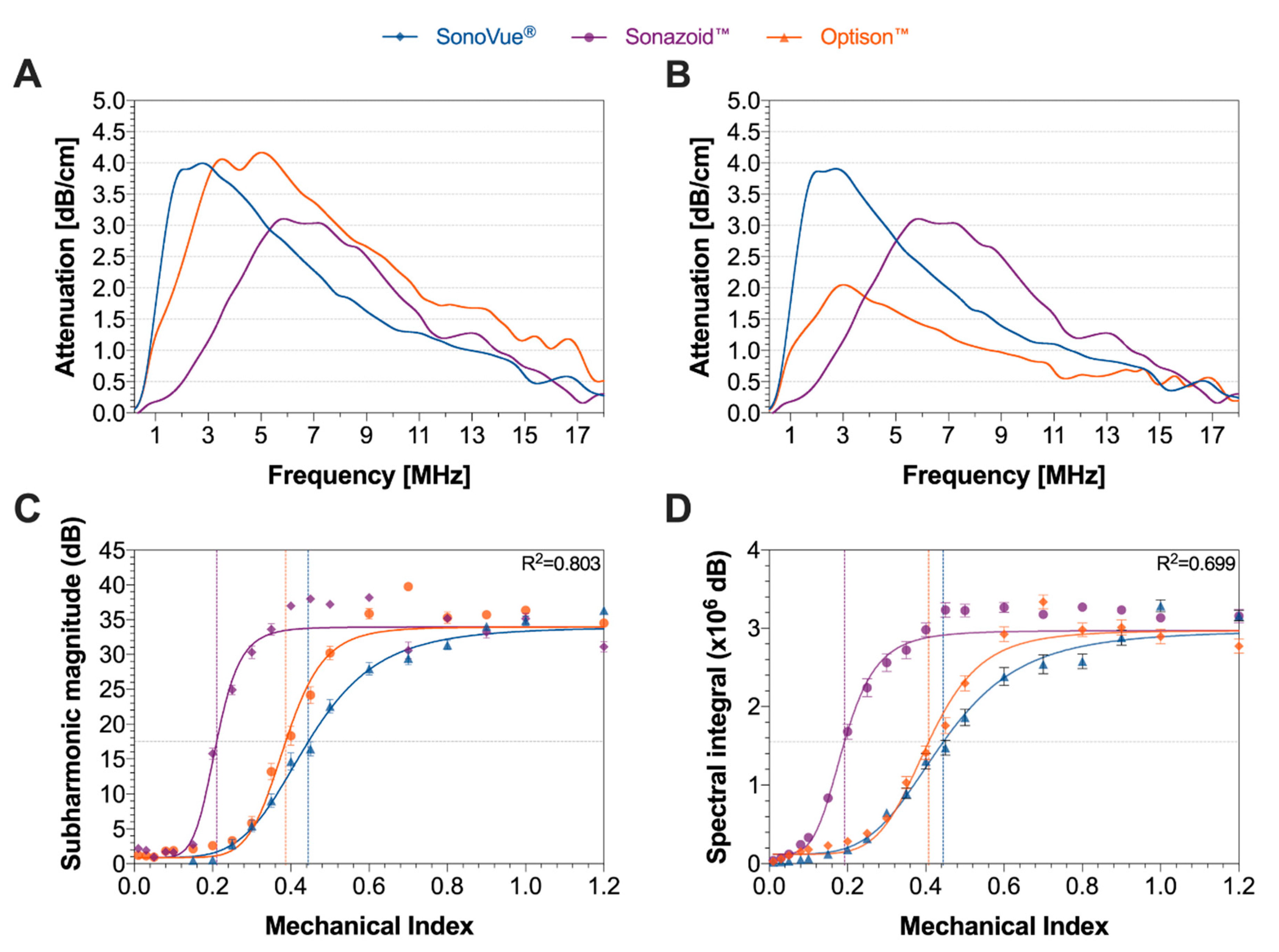
3.1.2. Attenuation and Cavitation Measurements
3.2. Simulations
3.2.1. Microbubble Pharmacokinetics
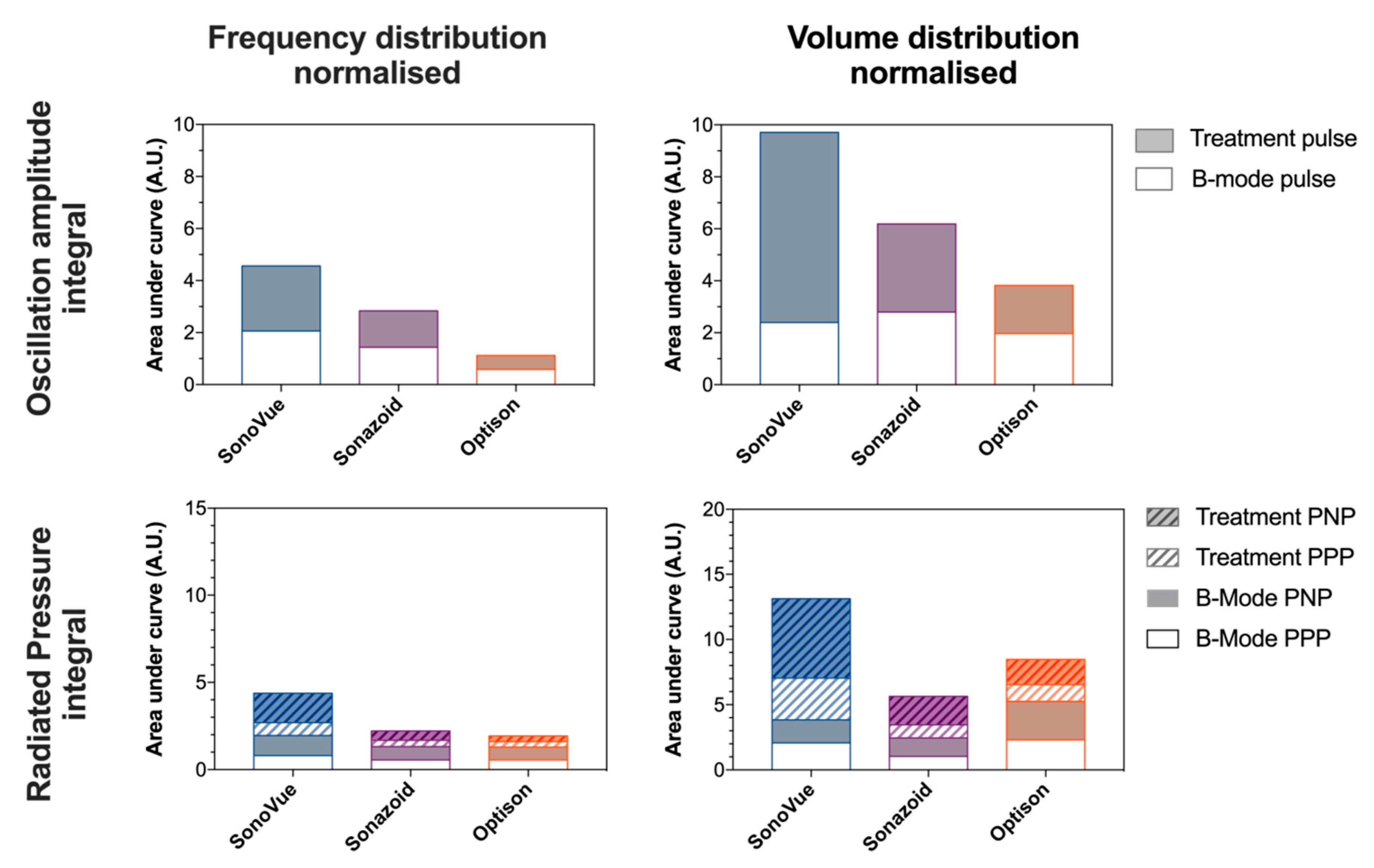
3.2.2. Simulated Microbubble Behavior
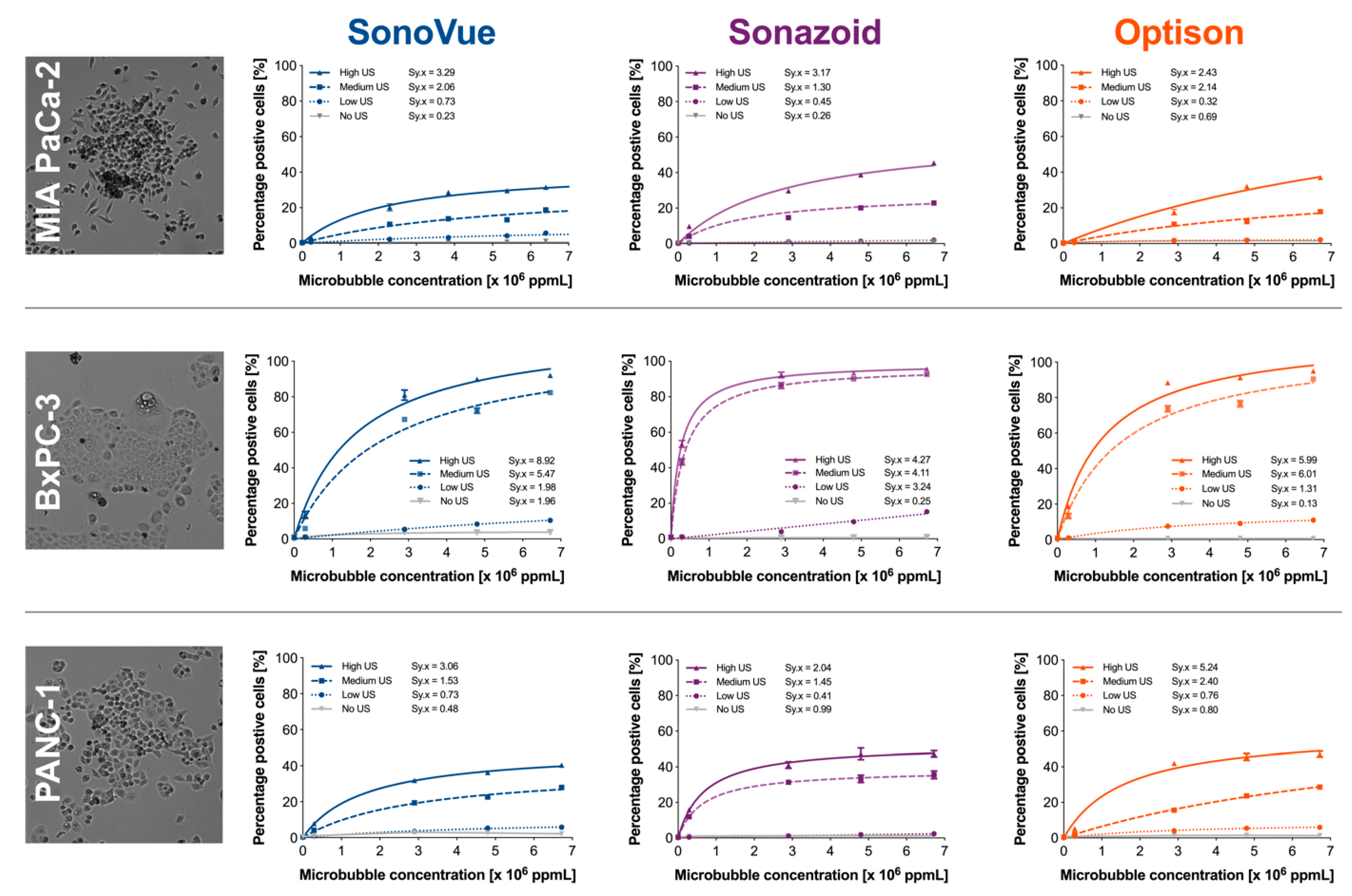
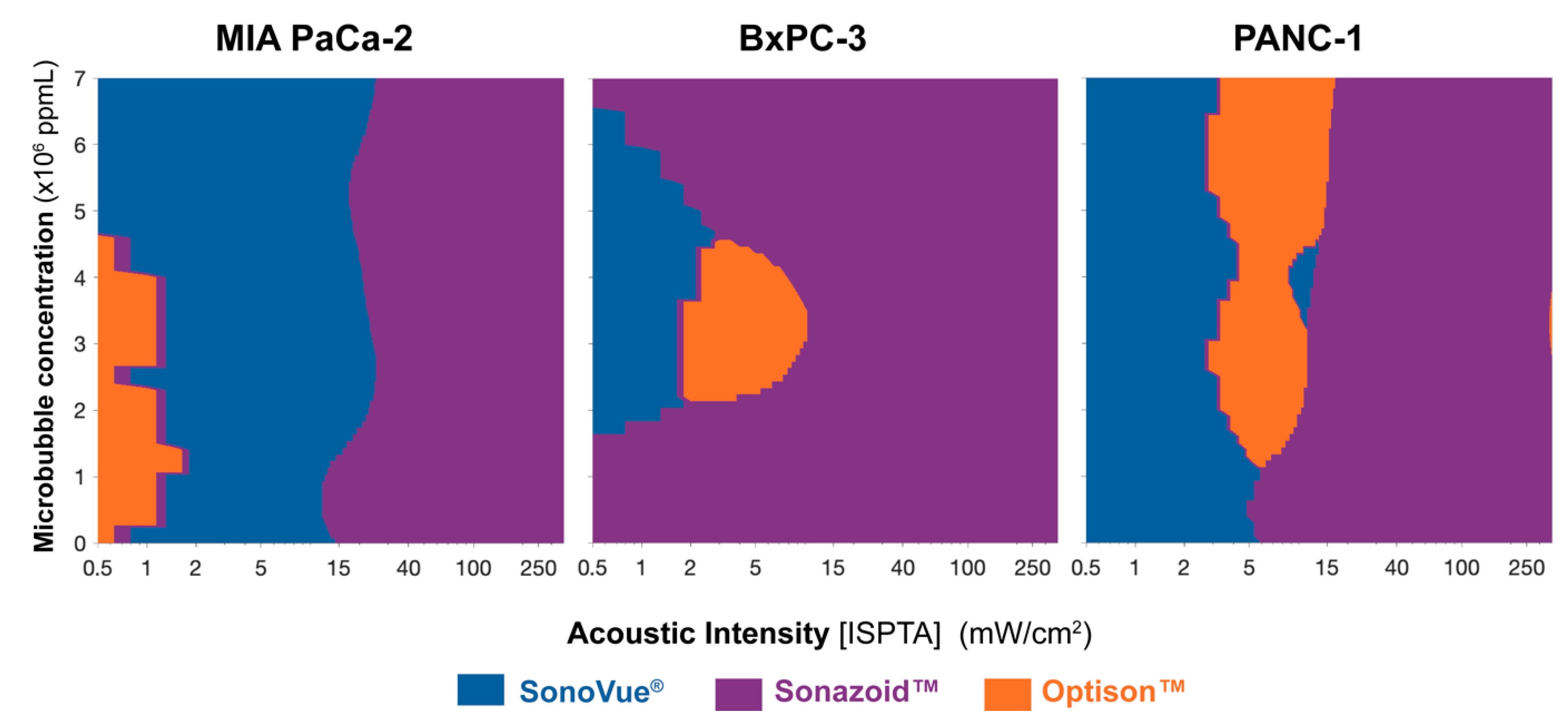
3.3. In Vitro Experiments
3.4. In Vivo Experiments
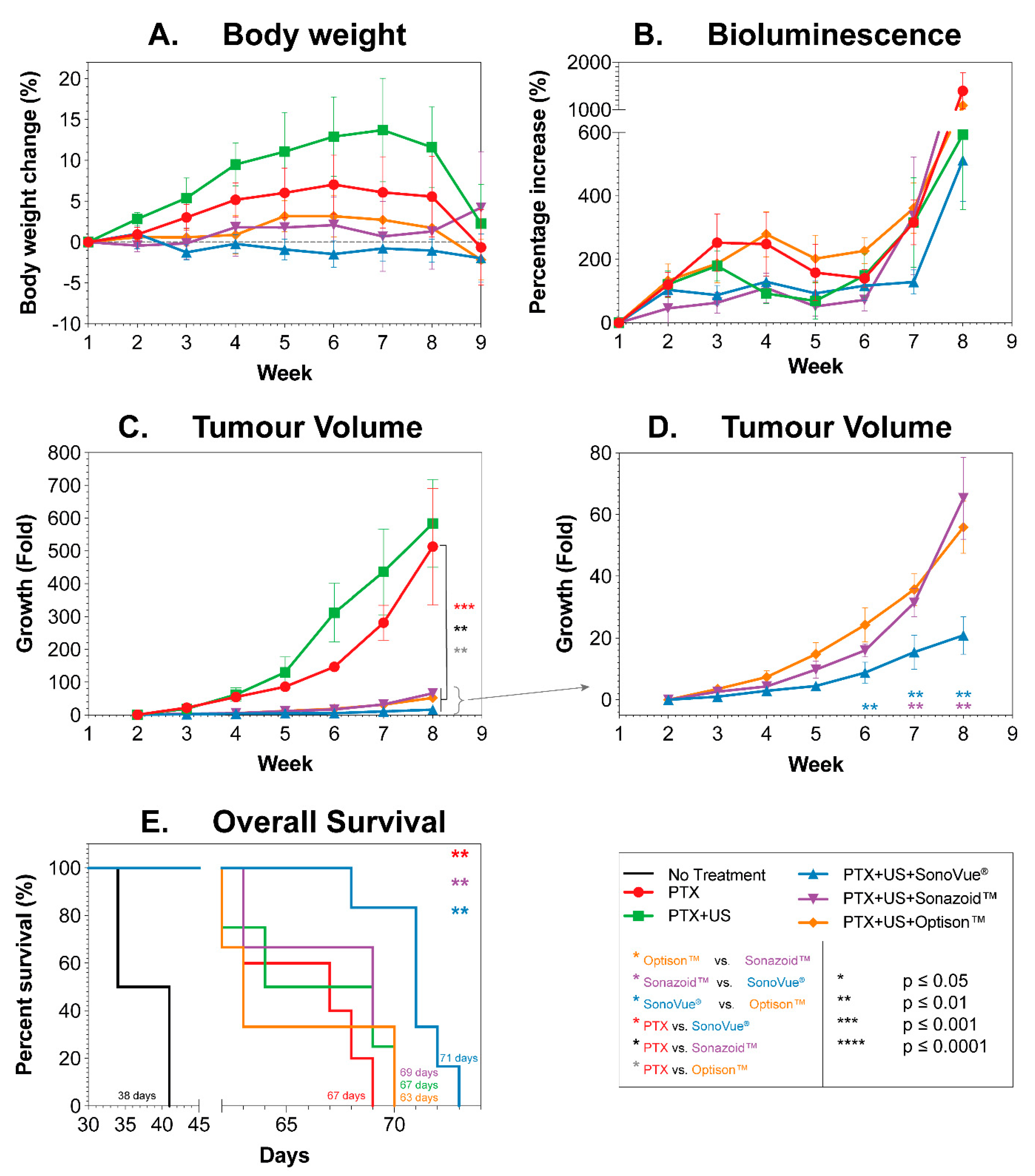
3.4.1. Body Weight
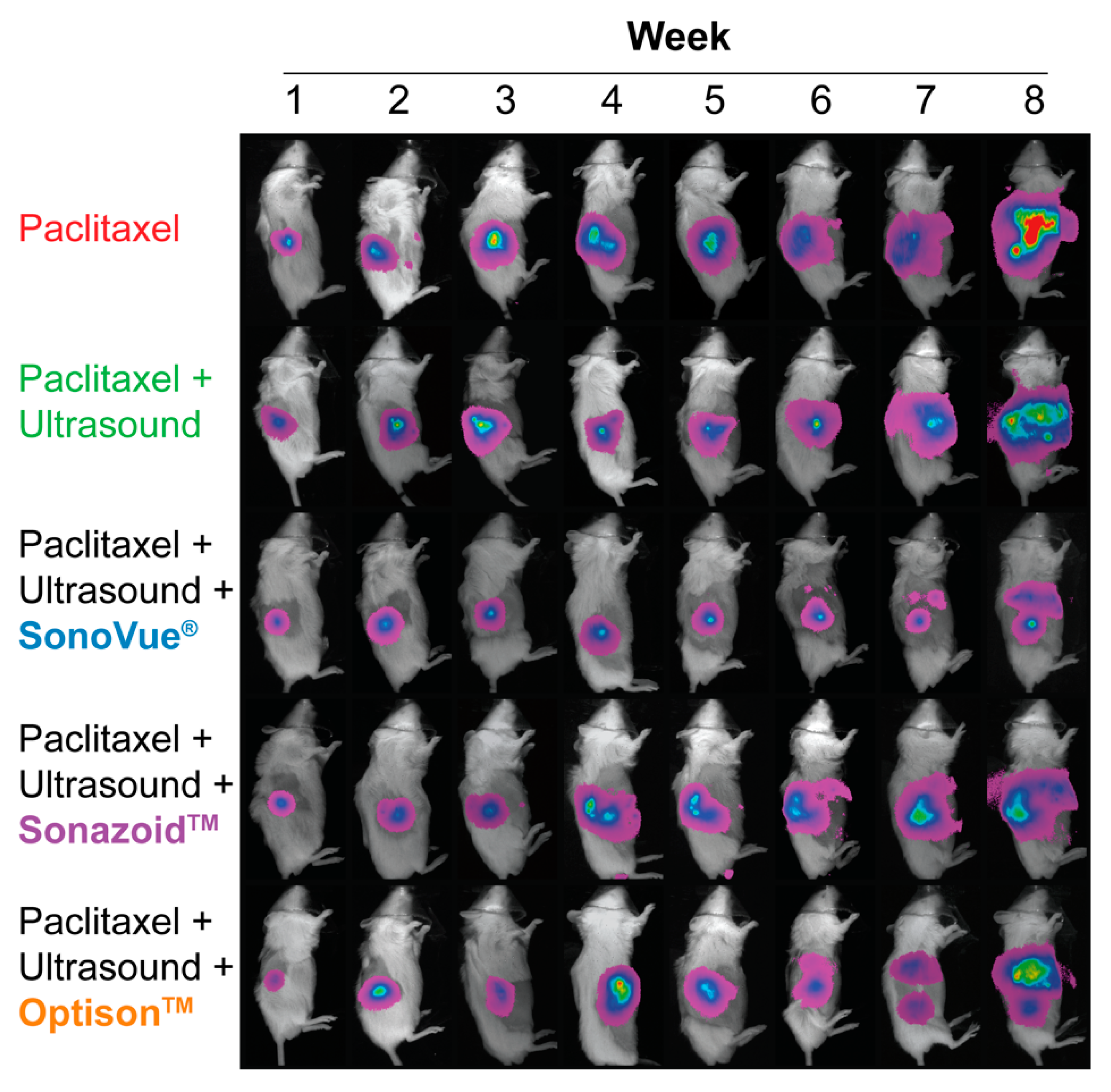
3.4.2. Bioluminescence
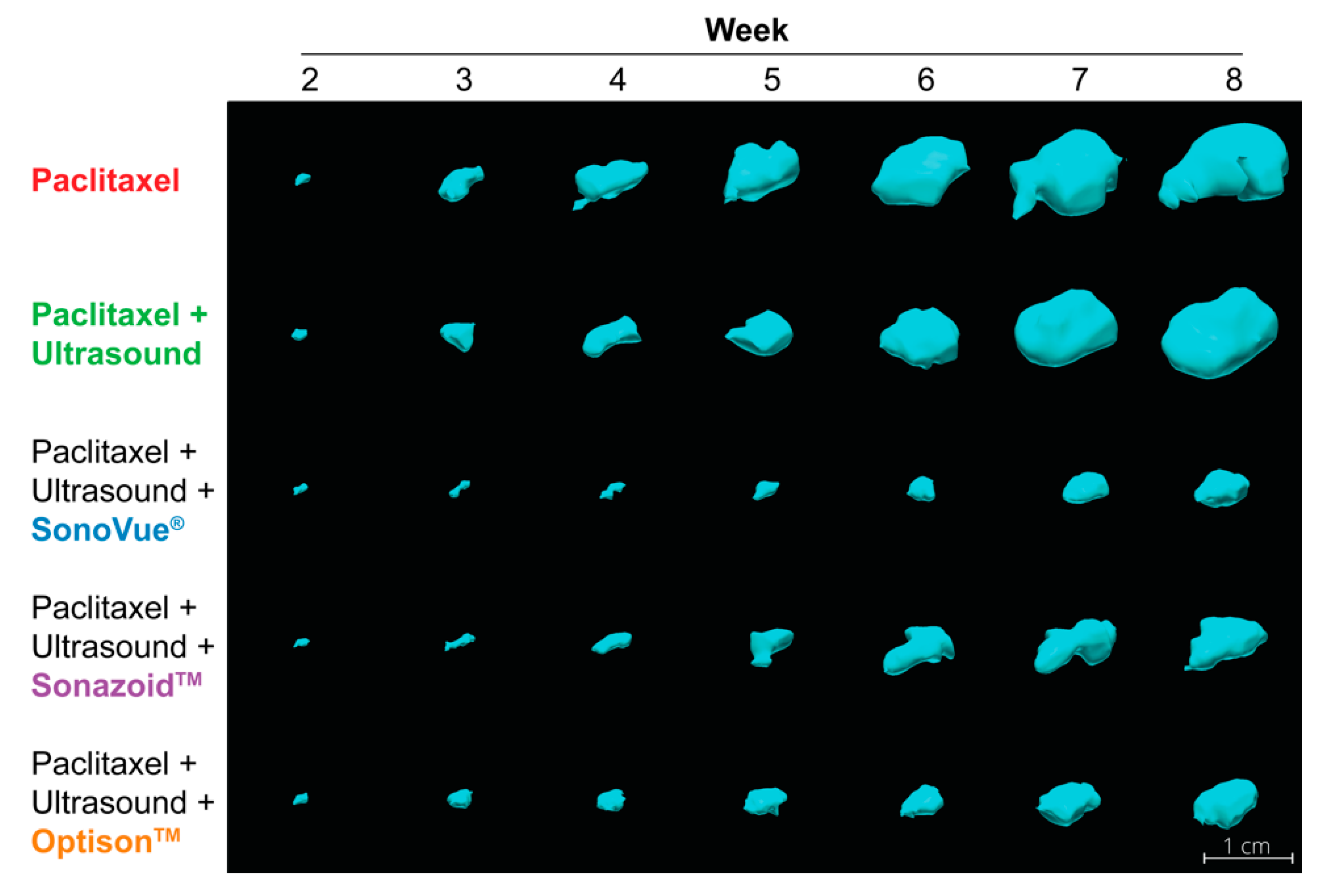
3.4.3. Tumor Volume
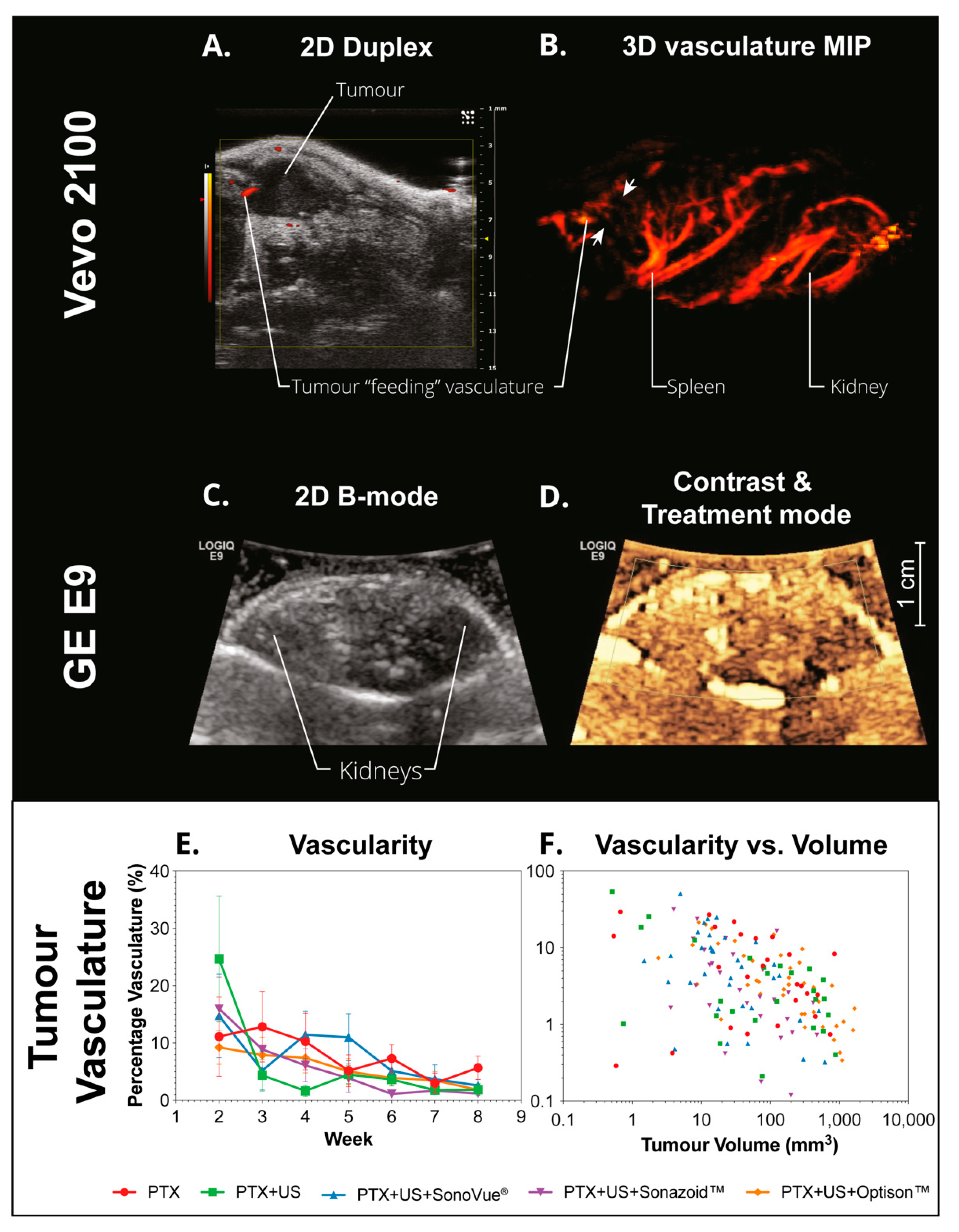
3.4.4. Vascularization
3.4.5. Survival
4. Discussion
4.1. Microbubble Characterization
4.2. Simulations
4.2.1. Microbubble Pharmacokinetics
4.2.2. Simulated Microbubble Behavior
4.3. In Vitro Experiments
4.4. In Vivo Experiments
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bao, S.; Thrall, B.D.; Miller, D.L. Transfection of a reporter plasmid into cultured cells by sonoporation in vitro. Ultrasound Med. Biol. 1997, 23, 953–959. [Google Scholar] [CrossRef]
- Ward, M.; Wu, J.; Chiu, J.-F. Ultrasound-induced cell lysis and sonoporation enhanced by contrast agents. J. Acoust. Soc. Am. 1999, 105, 2951–2957. [Google Scholar] [CrossRef]
- Nizzero, S.; Ziemys, A.; Ferrari, M. Transport Barriers and Oncophysics in Cancer Treatment. Trends Cancer 2018, 4, 277–280. [Google Scholar] [CrossRef] [Green Version]
- Stewart, M.P.; Langer, R.; Jensen, K.F. Intracellular Delivery by Membrane Disruption: Mechanisms, Strategies, and Concepts. Chem. Rev. 2018, 118, 7409–7531. [Google Scholar] [CrossRef]
- Park, K. Focused ultrasound for targeted nanoparticle delivery to tumors. J. Control. Release Off. J. Control. Release Soc. 2010, 146, 263. [Google Scholar] [CrossRef]
- Boissenot, T.; Bordat, A.; Fattal, E.; Tsapis, N. Ultrasound-triggered drug delivery for cancer treatment using drug delivery systems: From theoretical considerations to practical applications. J. Control. Release 2016, 241, 144–163. [Google Scholar] [CrossRef] [PubMed]
- Ojha, T.; Pathak, V.; Shi, Y.; Hennink, W.E.; Moonen, C.T.; Storm, G.; Kiessling, F.; Lammers, T. Pharmacological and physical vessel modulation strategies to improve EPR-mediated drug targeting to tumors. Adv. Drug Deliv. Rev. 2017, 119, 44–60. [Google Scholar] [CrossRef] [Green Version]
- Prabhakar, U.; Maeda, H.; Jain, R.K.; Sevick-Muraca, E.M.; Zamboni, W.; Farokhzad, O.C.; Barry, S.T.; Gabizon, A.; Grodzinski, P.; Blakey, D.C. Challenges and Key Considerations of the Enhanced Permeability and Retention Effect for Nanomedicine Drug Delivery in Oncology. Cancer Res. 2013, 73, 2412–2417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwanaga, K.; Tominaga, K.; Yamamoto, K.; Habu, M.; Maeda, H.; Akifusa, S.; Tsujisawa, T.; Okinaga, T.; Fukuda, J.; Nishihara, T. Local delivery system of cytotoxic agents to tumors by focused sonoporation. Cancer Gene Ther. 2007, 14, 354–363. [Google Scholar] [CrossRef] [Green Version]
- Hirabayashi, F.; Iwanaga, K.; Okinaga, T.; Takahashi, O.; Ariyoshi, W.; Suzuki, R.; Sugii, M.; Maruyama, K.; Tominaga, K.; Nishihara, T. Epidermal growth factor receptor-targeted sonoporation with microbubbles enhances therapeutic efficacy in a squamous cell carcinoma model. PLoS ONE 2017, 12, e0185293. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, Y.; Aoi, A.; Horie, S.; Tomita, N.; Mori, S.; Morikawa, H.; Matsumura, Y.; Vassaux, G.; Kodama, T. Low-intensity ultrasound and microbubbles enhance the antitumor effect of cisplatin. Cancer Sci. 2008, 99, 2525–2531. [Google Scholar] [CrossRef]
- Matsuo, M.; Yamaguchi, K.; Feril, L.B.; Endo, H.; Ogawa, K.; Tachibana, K.; Nakayama, J. Synergistic inhibition of malignant melanoma proliferation by melphalan combined with ultrasound and microbubbles. Ultrason. Sonochem. 2011, 18, 1218–1224. [Google Scholar] [CrossRef]
- Zhao, Y.-Z.; Lu, C.-T.; Zhou, Z.-C.; Jin, Z.; Zhang, L.; Sun, C.-Z.; Xu, Y.-Y.; Gao, H.-S.; Tian, J.-L.; Gao, F.-H.; et al. Enhancing chemotherapeutic drug inhibition on tumor growth by ultrasound: Anin vivoexperiment. J. Drug Target. 2010, 19, 154–160. [Google Scholar] [CrossRef]
- Sorace, A.G.; Warram, J.M.; Umphrey, H.; Hoyt, K. Microbubble-mediated ultrasonic techniques for improved chemotherapeutic delivery in cancer. J. Drug Target. 2011, 20, 43–54. [Google Scholar] [CrossRef]
- Grasso, C.; Jansen, G.; Giovannetti, E. Drug resistance in pancreatic cancer: Impact of altered energy metabolism. Crit. Rev. Oncol. 2017, 114, 139–152. [Google Scholar] [CrossRef]
- Kotopoulis, S.; Delalande, A.; Popa, M.; Mamaeva, V.; Dimcevski, G.; Gilja, O.H.; Postema, M.; Gjertsen, B.T.; McCormack, E. Sonoporation-Enhanced Chemotherapy Significantly Reduces Primary Tumour Burden in an Orthotopic Pancreatic Cancer Xenograft. Mol. Imaging Biol. 2013, 16, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Kotopoulis, S.; Stigen, E.; Popa, M.; Safont, M.M.; Healey, A.; Kvåle, S.; Sontum, P.; Gjertsen, B.T.; Gilja, O.H.; McCormack, E. Sonoporation with Acoustic Cluster Therapy (ACT®) induces transient tumour volume reduction in a subcutaneous xenograft model of pancreatic ductal adenocarcinoma. J. Control. Release 2017, 245, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Bressand, D.; Novell, A.; Girault, A.; Raoul, W.; Fromont-Hankard, G.; Escoffre, J.-M.; Lecomte, T.; Bouakaz, A. Enhancing Nab-Paclitaxel Delivery Using Microbubble-Assisted Ultrasound in a Pancreatic Cancer Model. Mol. Pharm. 2019, 16, 3814–3822. [Google Scholar] [CrossRef] [PubMed]
- Dimcevski, G.; Kotopoulis, S.; Bjånes, T.; Hoem, D.; Schjøtt, J.; Gjertsen, B.T.; Biermann, M.; Molven, A.; Sorbye, H.; Mc Cormack, E.; et al. A human clinical trial using ultrasound and microbubbles to enhance gemcitabine treatment of inoperable pancreatic cancer. J. Control. Release 2016, 243, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Ultrasound-Enhanced Delivery of Chemotherapy to Patients With Liver Metastasis From Breast- and Colorectal Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03477019 (accessed on 15 December 2021).
- KVUS at Neoadjuvant CTx of Breast Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03385200 (accessed on 15 December 2021).
- Targeted Delivery of Chemotherapy with Ultrasound and Microbublles. Available online: https://clinicaltrials.gov/ct2/show/NCT03458975 (accessed on 15 December 2021).
- Acoustic Cluster Therapy (ACT) With Chemotherapy in Metastatic Liver Metastases of Gastrointestinal Origin. Available online: https://clinicaltrials.gov/ct2/show/NCT04021277 (accessed on 15 December 2021).
- Carpentier, A.; Canney, M.; Vignot, A.; Reina, V.; Beccaria, K.; Horodyckid, C.; Karachi, C.; Leclercq, D.; Lafon, C.; Chapelon, J.-Y.; et al. Clinical trial of blood-brain barrier disruption by pulsed ultrasound. Sci. Transl. Med. 2016, 8, 343re2. [Google Scholar] [CrossRef]
- Meng, Y.; Reilly, R.M.; Pezo, R.C.; Trudeau, M.; Sahgal, A.; Singnurkar, A.; Perry, J.; Myrehaug, S.; Pople, C.B.; Davidson, B.; et al. MR-guided focused ultrasound enhances delivery of trastuzumab to Her2-positive brain metastases. Sci. Transl. Med. 2021, 13, eabj4011. [Google Scholar] [CrossRef]
- Dasgupta, A.; Liu, M.; Ojha, T.; Storm, G.; Kiessling, F.; Lammers, T. Ultrasound-mediated drug delivery to the brain: Principles, progress and prospects. Drug Discov. Today Technol. 2016, 20, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Johnston, K.; Tapia-Siles, S.C.; Gerold, B.; Postema, M.; Cochran, S.; Cuschieri, A.; Prentice, P. Periodic shock-emission from acoustically driven cavitation clouds: A source of the subharmonic signal. Ultrasonics 2014, 54, 2151–2158. [Google Scholar] [CrossRef] [Green Version]
- Bazan-Peregrino, M.; Rifai, B.; Carlisle, R.C.; Choi, J.; Arvanitis, C.D.; Seymour, L.W.; Coussios, C.C. Cavitation-enhanced delivery of a replicating oncolytic adenovirus to tumors using focused ultrasound. J. Control. Release 2013, 169, 40–47. [Google Scholar] [CrossRef]
- Hedaya, M.A. Basic Pharmacokinetics, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- Postema, M.; de Jong, N.; Schmitz, G. The physics of nanoshelled microbubbles. Biomed. Tech. 2005, 50, 748–749. [Google Scholar]
- Postema, M.; Schmitz, G. Ultrasonic bubbles in medicine: Influence of the shell. Ultrason. Sonochem. 2007, 14, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Postema, M. Fundamentals of Medical Ultrasonics; Spon Press: London, UK, 2011. [Google Scholar]
- Barău, A.; Ruiz-Sauri, A.; Valencia, G.; Gómez-Mateo, M.D.C.; Sabater, L.; Ferrandez, A.; Llombart-Bosch, A. High microvessel density in pancreatic ductal adenocarcinoma is associated with high grade. Virchows Archiv 2013, 462, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Tu, J.; Guan, J.; Qiu, Y.; Matula, T.J. Estimating the shell parameters of SonoVue microbubbles using light scattering. J. Acoust. Soc. Am. 2009, 126, 2954–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Meer, S.; Versluis, M.; Lohse, D.; Chin, C.; Bouakaz, A.; De Jong, N. The resonance frequency of SonoVue as observed by high-speed optical imaging. IEEE Ultrason. Symp. 2004, 1, 343–345. [Google Scholar] [CrossRef] [Green Version]
- Guan, J.; Matula, T.J. Using light scattering to measure the response of individual ultrasound contrast microbubbles sub-jected to pulsed ultrasound in vitro. J. Acoust. Soc. Am. 2004, 116, 2832–2842. [Google Scholar] [CrossRef]
- Paul, S.; Katiyar, A.; Sarkar, K.; Chatterjee, D.; Shi, W.T.; Forsberg, F. Material characterization of the encapsulation of an ultrasound contrast microbubble and its subharmonic response: Strain-softening interfacial elasticity model. J. Acoust. Soc. Am. 2010, 127, 3846–3857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammi, A.; Cleveland, R.; Mamou, J.; Wang, G.; Bridal, S.L.; Brien, W.D.O. Double passive cavitation detection of OptisonTM shell rupture. IEEE Ultrason. Symp. 2005, 2, 846–849. [Google Scholar] [CrossRef]
- Ammi, A.Y.; Cleveland, R.O.; Mamou, J.; Wang, G.I.; Bridal, S.L.; O’Brien, W.D. Ultrasonic contrast agent shell rupture detected by inertial cavitation and rebound signals. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2006, 53, 126–136. [Google Scholar] [CrossRef]
- Joback, K.; Reid, R. Estimation of pure-component properties from group-contributions. Chem. Eng. Commun. 1987, 57, 233–243. [Google Scholar] [CrossRef]
- Lide, D.R. CRC Handbook of Chemistry and Physics, 89th ed.; CRC Press LLC: Boca Raton, FL, USA, 2008. [Google Scholar]
- Rathjen, I.W.; Straub, I.H.J. Die Temperaturabhängigkeit der Oberflächenspannung von reinen Kältemitteln vom Tripelpunkt bis zum kritischen Punkt. Wärme-Und Stoffübertrag. 1980, 14, 59–73. [Google Scholar] [CrossRef]
- Hernandez, C.; Nieves, L.; de Leon, A.C.; Advincula, R.; Exner, A.A. Role of Surface Tension in Gas Nanobubble Stability Under Ultrasound. ACS Appl. Mater. Interfaces 2018, 10, 9949–9956. [Google Scholar] [CrossRef] [PubMed]
- Church, C.C.; Carstensen, E.L. “Stable” inertial cavitation. Ultrasound Med. Biol. 2001, 27, 1435–1437. [Google Scholar] [CrossRef]
- Chatterjee, D.; Sarkar, K. A Newtonian rheological model for the interface of microbubble contrast agents. Ultrasound Med. Biol. 2003, 29, 1749–1757. [Google Scholar] [CrossRef]
- Riches, A.C.; Sharp, J.G.; Thomas, D.B.; Smith, S.V. Blood volume determination in the mouse. J. Physiol. 1973, 228, 279–284. [Google Scholar] [CrossRef]
- Windberger, U.; Bartholovitsch, A.; Plasenzotti, R.; Korak, K.J.; Heinze, G. Whole blood viscosity, plasma viscosity and erythrocyte aggregation in nine mammalian species: Reference values and comparison of data. Exp. Physiol. 2003, 88, 431–440. [Google Scholar] [CrossRef] [Green Version]
- Bjånes, T.; Kotopoulis, S.; Murvold, E.T.; Kamčeva, T.; Gjertsen, B.T.; Gilja, O.H.; Schjøtt, J.; Riedel, B.; McCormack, E. Ultrasound- and Microbubble-Assisted Gemcitabine Delivery to Pancreatic Cancer Cells. Pharmaceutics 2020, 12, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yddal, T.; Cochran, S.; Gilja, O.H.; Postema, M.; Kotopoulis, S. Open-source, high-throughput ultrasound treatment chamber. Biomed. Tech. Eng. 2015, 60, 77–87. [Google Scholar] [CrossRef]
- Zeghimi, A.; Escoffre, J.M.; Bouakaz, A. Role of endocytosis in sonoporation-mediated membrane permeabilization and uptake of small molecules: A electron microscopy study. Phys. Biol. 2015, 12, 066007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Directive 2010/63/EU. Directive 2010/63/EU of the European Parliament and of the Council of 22 September 2010 on the protection of animals used for scientific purposes. Off. J. Eur. Union 2010. [Google Scholar]
- Haugse, R.; Langer, A.; Gullaksen, S.-E.; Sundøy, S.M.; Gjertsen, B.T.; Kotopoulis, S.; McCormack, E. Intracellular Signaling in Key Pathways Is Induced by Treatment with Ultrasound and Microbubbles in a Leukemia Cell Line, but Not in Healthy Peripheral Blood Mononuclear Cells. Pharmaceutics 2019, 11, 319. [Google Scholar] [CrossRef] [Green Version]
- Hather, G.; Liu, R.; Bandi, S.; Mettetal, J.; Manfredi, M.; Shyu, W.-C.; Donelan, J.; Chakravarty, A. Growth Rate Analysis and Efficient Experimental Design for Tumor Xenograft Studies. Cancer Inform. 2014, 13, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sassaroli, E.; Hynynen, K. Resonance frequency of microbubbles in small blood vessels: A numerical study. Phys. Med. Biol. 2005, 50, 5293. [Google Scholar] [CrossRef]
- Patel, A.; Schoen, S.J.; Arvanitis, C.D. Closed-Loop Spatial and Temporal Control of Cavitation Activity With Passive Acoustic Mapping. IEEE Trans. Biomed. Eng. 2018, 66, 2022–2031. [Google Scholar] [CrossRef]
- Salgaonkar, V.A.; Datta, S.; Holland, C.K.; Mast, T.D. Passive cavitation imaging with ultrasound arrays. J. Acoust. Soc. Am. 2009, 126, 3071–3083. [Google Scholar] [CrossRef] [Green Version]
- Shi, W.T.; Forsberg, F.; Tornes, A.; Østensen, J.; Goldberg, B.B. Destruction of contrast microbubbles and the association with inertial cavitation. Ultrasound Med. Biol. 2000, 26, 1009–1019. [Google Scholar] [CrossRef]
- Bader, K.B.; Holland, C. Gauging the likelihood of stable cavitation from ultrasound contrast agents. Phys. Med. Biol. 2013, 58, 127–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apfel, R.E.; Holland, C.K. Gauging the likelihood of cavitation from short-pulse, low-duty cycle diagnostic ultrasound. Ultrasound Med. Biol. 1991, 17, 179–185. [Google Scholar] [CrossRef]
- Doinikov, A.A.; Bouakaz, A. Review of shell models for contrast agent microbubbles. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Eikrem, O.; Kotopoulis, S.; Popa, M.; Safont, M.M.; Fossan, K.O.; Leh, S.; Landolt, L.; Babickova, J.; Gudbrandsen, O.A.; Gilja, O.H.; et al. Ultrasound and Microbubbles Enhance Uptake of Doxorubicin in Murine Kidneys. Pharmaceutics 2021, 13, 2038. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Property | Unit | Abbreviation | SonoVue® | Sonazoid™ | Optison™ |
|---|---|---|---|---|---|
| Shell stiffness | N/m | χ | 0.22 [34,35,36] | 0.53 [37] | 4.00 [38,39] |
| Specific heat ratio of gas [40] | A.U. | γ | (SF6) 1.0934 | (C4F10) 1.0699 | (C3F8) 1.0731 |
| Gas compressibility [41] | ×10−6 m2/N | κ | 9.173 | 6.537 | 7.458 |
| Surface tension | N/m | σ | 0.052 [35,42] | 0.042 [43,44] | 0.9 [45] |
| Mouse Blood | |||||
| Fluid density | kg m3 | ρ | 1 057 [46] | ||
| Liquid viscosity | mPa s | ν | 5.996 [47] | ||
| Name | Frequency (MHz) | No. of Cycles | Duty Cycle (%) | Pulse Repetition Frequency (Hz) | MI | Intensity | |
|---|---|---|---|---|---|---|---|
| ISPTA (mW/cm2) | ISPPA (W/cm2) | ||||||
| Low | 2.00 | 20 | 0.4 | 22 | 0.10 | 3 | 1 |
| Medium | 2.00 | 80 | 1.8 | 22 | 0.20 | 50 | 3 |
| High | 2.00 | 160 | 3.6 | 22 | 0.39 | 358 | 10 |
| Parameter | Value |
|---|---|
| Frequency (MHz) | 32 |
| Power (%) | 100 |
| PRF (kHz) | 2 |
| Gate | 1 |
| Doppler Gain (dB) | 35 |
| 2D Gain (dB) | 22 |
| Depth (mm) | Variable |
| Width (mm) | 14.08 |
| Beam Angle (º) | 0 |
| Sensitivity | 5 |
| Line Density | Full |
| Persistence | Off |
| ECG/Resp Gate | Off/On |
| 3D range | Variable |
| 3D step | Variable |
| Group | Microbubble | Dilution | Ultrasound | Drug | n |
|---|---|---|---|---|---|
| 1 | - | - – | - | 2 | |
| 2 | - | - - | ✓ | 5 | |
| 3 | - | ✓ | 4 | ||
| 4 | SonoVue® | None | ✓ | 6 | |
| 5 | Sonazoid™ | 1:4 | ✓ | 6 | |
| 6 | Optison™ | 1:1 | ✓ | 6 | |
| Centre Frequency (MHz) | Duty Cycle (%) | Mechanical Index | Acoustic Intensity, ISPTA (mW/cm2) | Peak Negative Acoustic Pressure (MPa) |
|---|---|---|---|---|
| 1.8 | 1.1% | 0.2 | 16 | 0.268 |
| Microbubble | Diameter (µm), Percentage (%), PSD d90/d10 | Fresh➝After 30 min | |||
|---|---|---|---|---|---|
| Count Normalized | Volume Normalized | Concentration (×109 ppmL) | Roundness | Mean Diameter | |
| SonoVue® | 1.7 µm, 6.8%, 2.46 | 5.1 µm, 1.3%, 6.36 | 0.239 ± 0.015→ 0.126±0.013 | 0.94→0.93 | 2.51 ± 0.07→ 3.20 ± 0.18 |
| Sonazoid™ | 1.9 µm, 7.8%, 2.06 | 2.3 µm, 5.8%, 2.50 | 1.269 ± 0.035→ 1.111 ± 0.039 | 0.95→0.94 | 2.45 ± 0.08→ 2.43 ± 0.07 |
| Optison™ | 3.3 µm, 4.2%, 2.15 | 5.1 µm, 2.1%, 4.89 | 0.607 ± 0.061→ 0.609 ± 0.118 | 0.92→0.88 | 3.55 ± 0.19→ 3.02 ± 0.07 |
| Method | SonoVue® | Sonazoid™ | Optison™ |
|---|---|---|---|
| Subharmonic Magnitude | 0.44 (0.440–0.453) | 0.21(0.205–0.215) | 0.39 (0.380–0.394) |
| Spectral integral | 0.44 (0.433–0.456) | 0.19 (0.185–0.200) | 0.41(0.400–0.417) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotopoulis, S.; Popa, M.; Mayoral Safont, M.; Murvold, E.; Haugse, R.; Langer, A.; Dimcevski, G.; Lam, C.; Bjånes, T.; Gilja, O.H.; et al. SonoVue® vs. Sonazoid™ vs. Optison™: Which Bubble Is Best for Low-Intensity Sonoporation of Pancreatic Ductal Adenocarcinoma? Pharmaceutics 2022, 14, 98. https://doi.org/10.3390/pharmaceutics14010098
Kotopoulis S, Popa M, Mayoral Safont M, Murvold E, Haugse R, Langer A, Dimcevski G, Lam C, Bjånes T, Gilja OH, et al. SonoVue® vs. Sonazoid™ vs. Optison™: Which Bubble Is Best for Low-Intensity Sonoporation of Pancreatic Ductal Adenocarcinoma? Pharmaceutics. 2022; 14(1):98. https://doi.org/10.3390/pharmaceutics14010098
Chicago/Turabian StyleKotopoulis, Spiros, Mihaela Popa, Mireia Mayoral Safont, Elisa Murvold, Ragnhild Haugse, Anika Langer, Georg Dimcevski, Christina Lam, Tormod Bjånes, Odd Helge Gilja, and et al. 2022. "SonoVue® vs. Sonazoid™ vs. Optison™: Which Bubble Is Best for Low-Intensity Sonoporation of Pancreatic Ductal Adenocarcinoma?" Pharmaceutics 14, no. 1: 98. https://doi.org/10.3390/pharmaceutics14010098
APA StyleKotopoulis, S., Popa, M., Mayoral Safont, M., Murvold, E., Haugse, R., Langer, A., Dimcevski, G., Lam, C., Bjånes, T., Gilja, O. H., & Cormack, E. M. (2022). SonoVue® vs. Sonazoid™ vs. Optison™: Which Bubble Is Best for Low-Intensity Sonoporation of Pancreatic Ductal Adenocarcinoma? Pharmaceutics, 14(1), 98. https://doi.org/10.3390/pharmaceutics14010098