
Epidemiology of Treated Diabetes Ocular Complications in France 2008–2018—The LANDSCAPE French Nationwide Study

 , , ,
, , ,
Abstract
:1. Background
2. Methods
2.1. Study Design and Data Sources
2.2. Identification of Treated DME and PDR Patients
2.3. Ethics and Data Protection
2.4. Statistical Analyses
2.4.1. Annual Incidence and Prevalence of Treated DME and PDR
2.4.2. Patient Characteristics and Comorbidities
2.4.3. Statistics
3. Results
3.1. Patient Characteristics
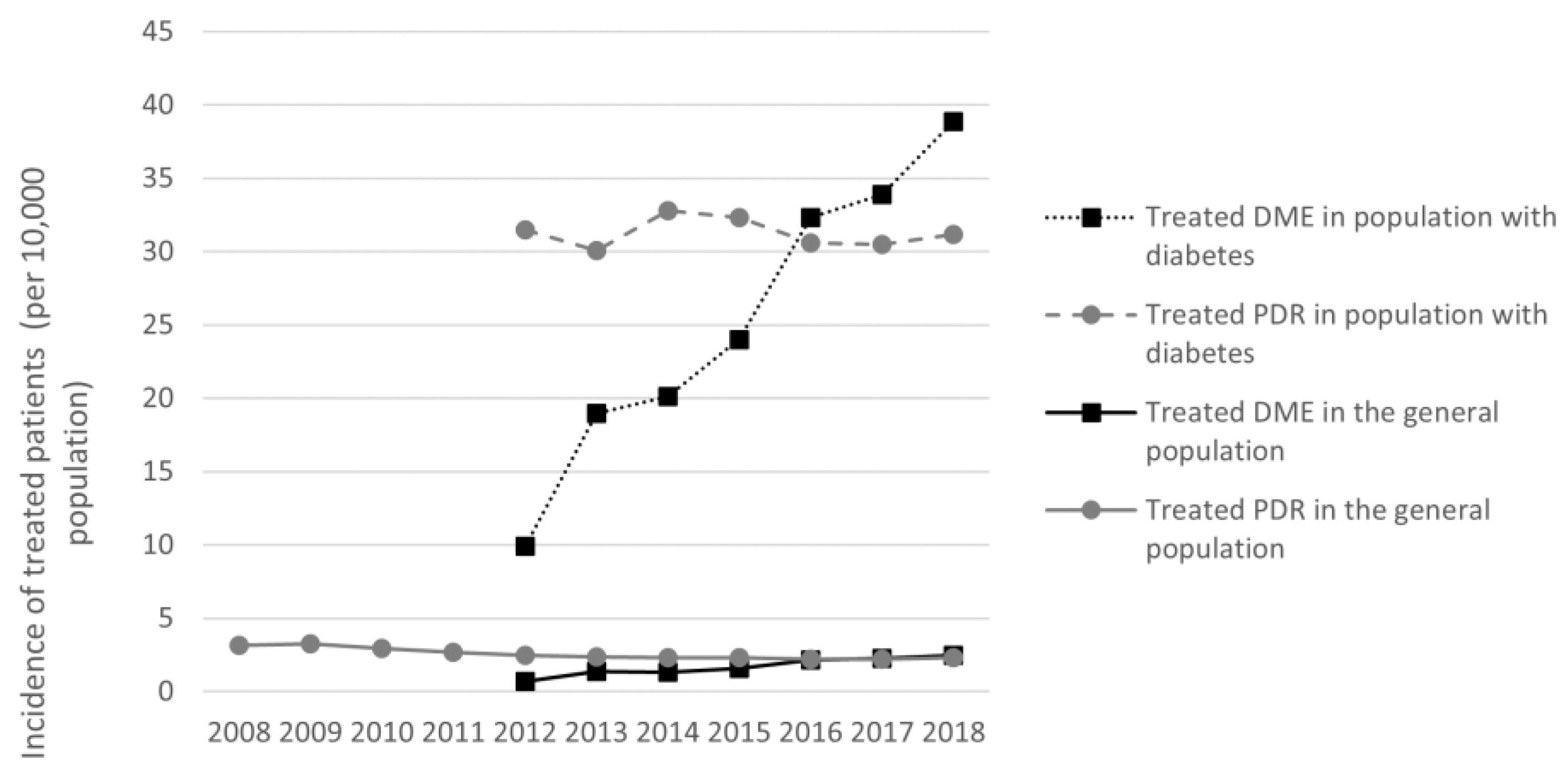
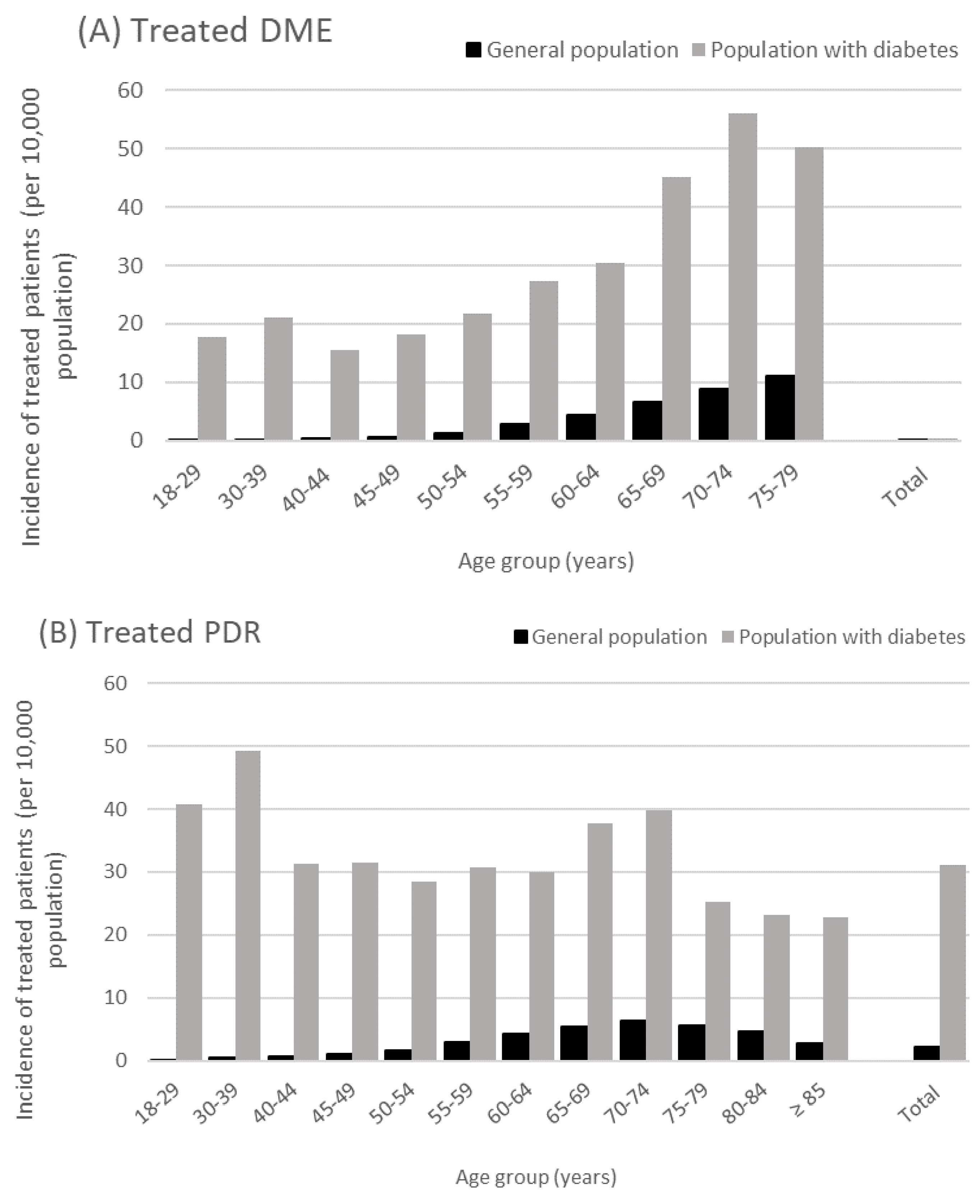
3.2. Treated DME and PDR Incidence 2008–2018
3.3. Treated DME and PDR Prevalence in 2018
3.4. Patients with Both Treated DME and PDR
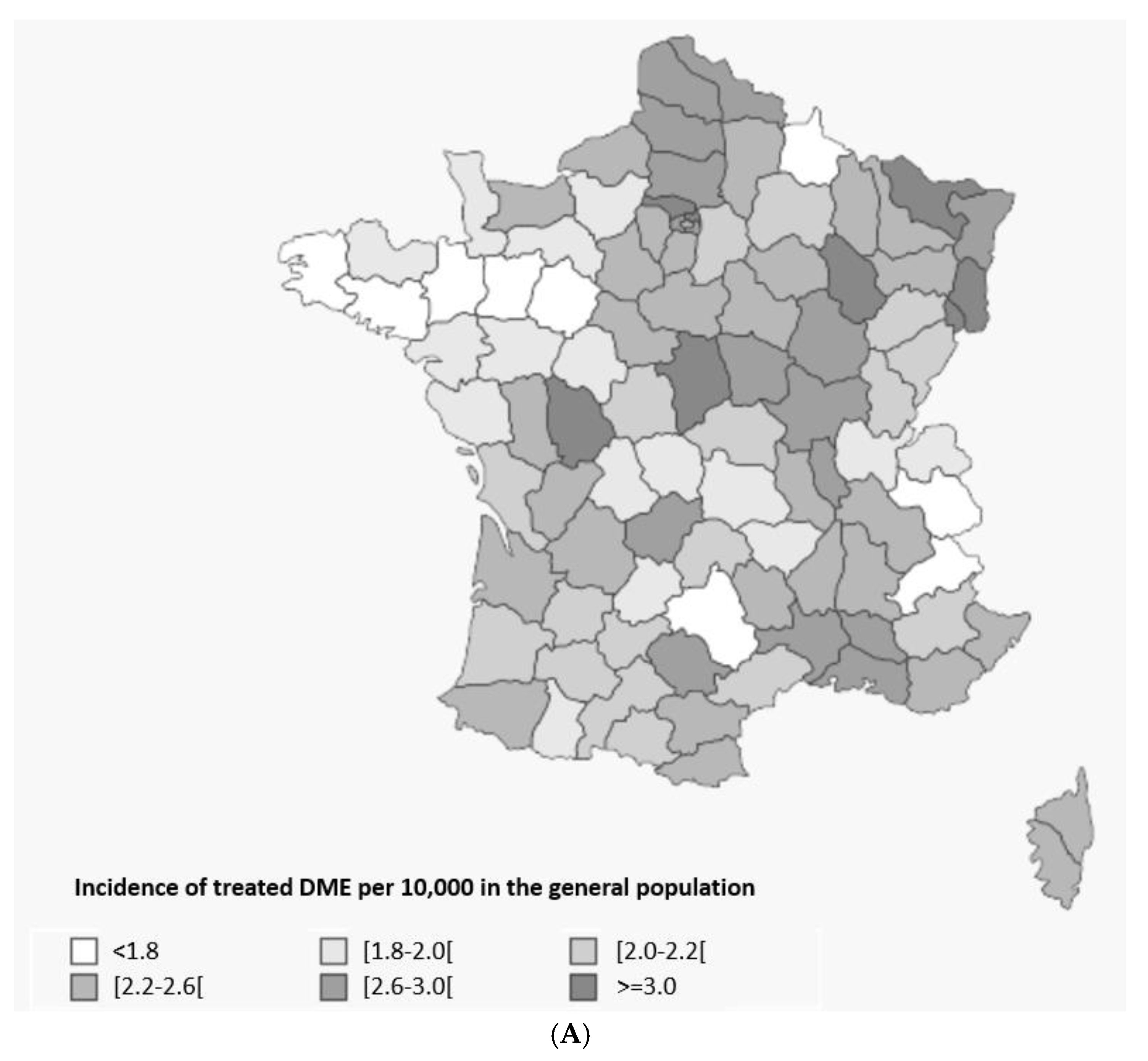
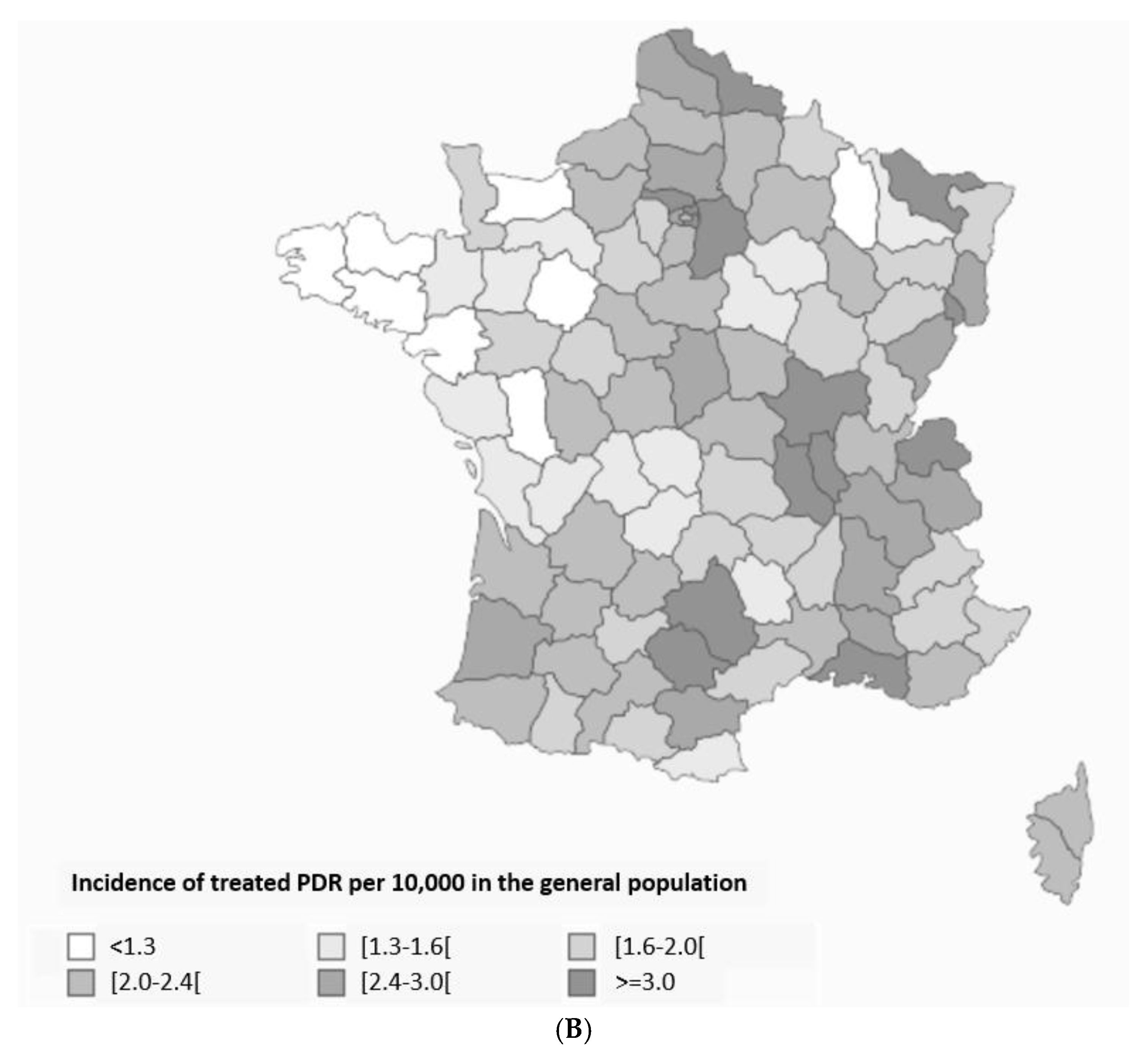
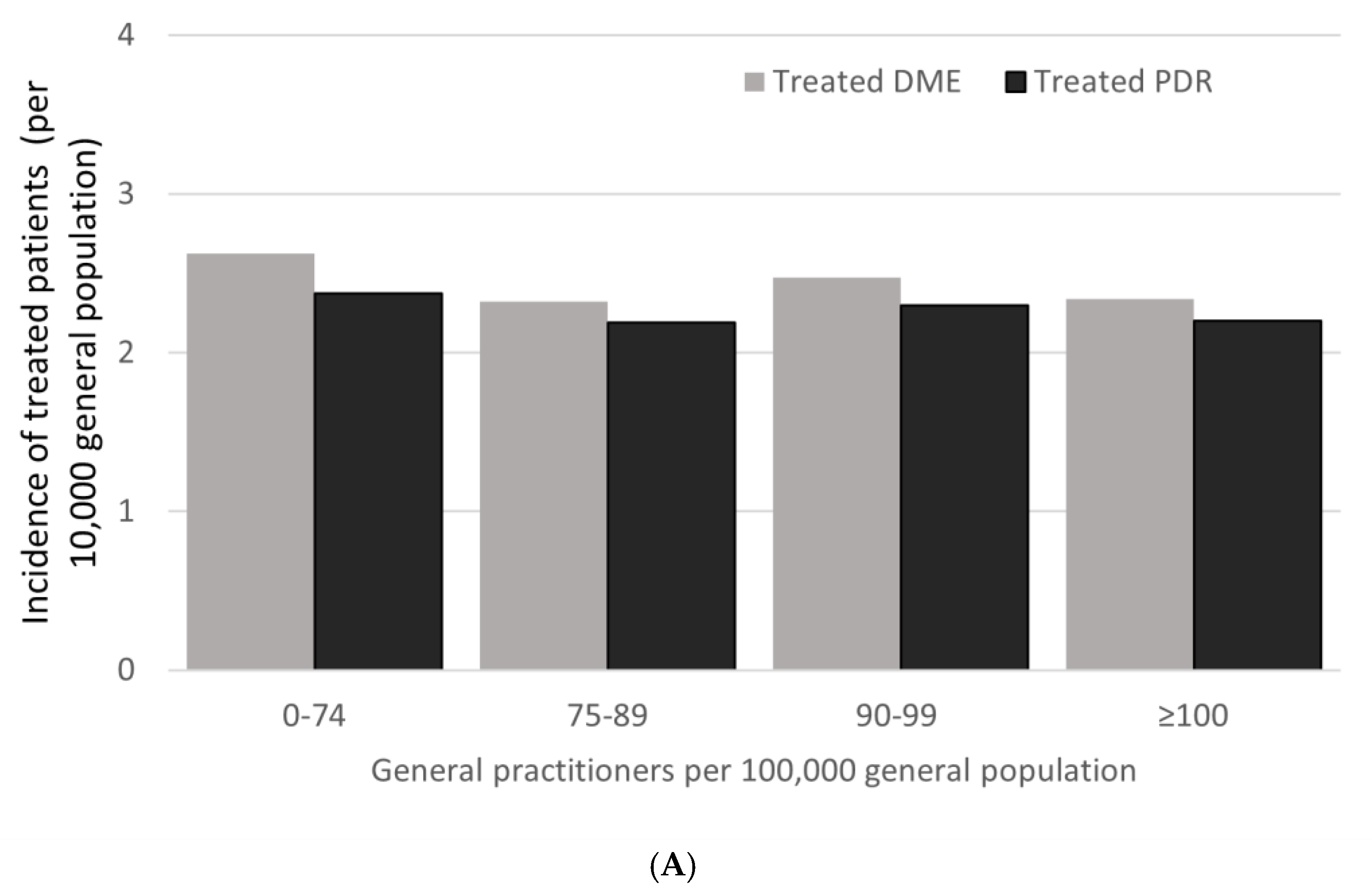
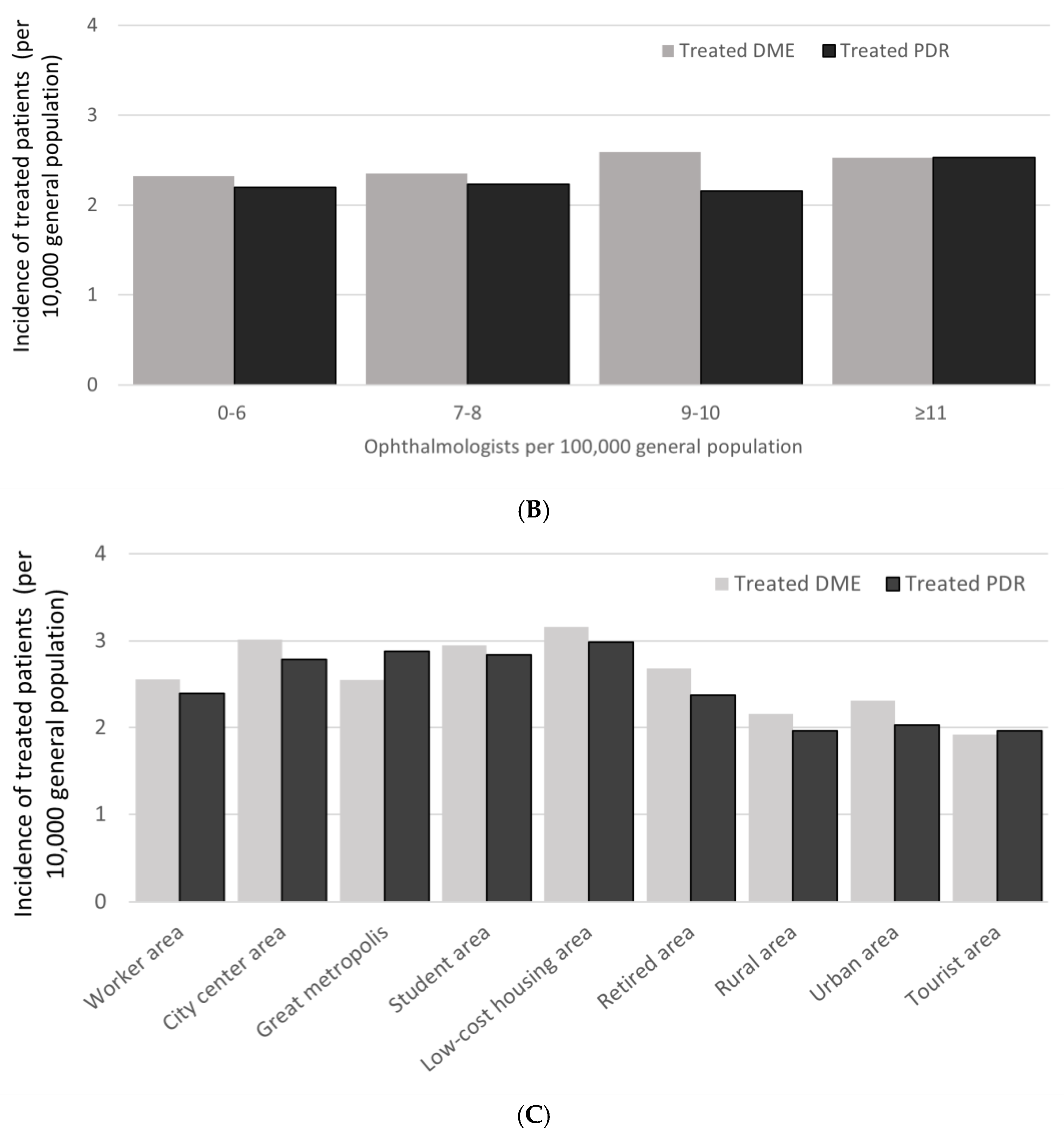
3.5. Impact of Geography and Access to Medical Care
4. Discussion
4.1. Patient Identification and Characteristics
4.2. Treated DME and PDR Epidemiology in People with Diabetes
4.3. Treated PDR Incidence and Prevalence
4.4. Treated DME and PDR Epidemiology in the General Population
4.5. Impact of Geography and Access to Care
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| anti-VEGF | Vascular epithelial growth factor inhibitor |
| DME | Diabetic macular edema |
| ICD-10 | International Classification of Diseases, revision 10 |
| INDS | Institute of Health Data (France) |
| INSEE | National Institute of Statistics and Economic Studies (France) |
| nAMD | Neovascular age-related macular degeneration |
| PDR | Proliferative diabetic retinopathy |
| PRP | Pan-retinal photocoagulation |
| SNDS | National Health Insurance database (Système National des Données de Santé, France) |
References
- GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas; International Diabetes Federation: Lisbon, Portugal, 2021. [Google Scholar]
- Billioti de Gage, S.; Bertrand, M.; Grimaldi, S.; Zureik, M. Intravitreal anti-VEGF use in France: A cross-sectional and longitudinal Nationwide observational study. Acta Ophthalmol. 2022, 100, e502–e511. [Google Scholar] [CrossRef] [PubMed]
- Schulze-Dobold, C.; Erginay, A.; Robert, N.; Chabouis, A.; Massin, P. Ophdiat((R)): Five-year experience of a telemedical screening programme for diabetic retinopathy in Paris and the surrounding area. Diabetes Metab. 2012, 38, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Chamard, C.; Daien, V.; Erginay, A.; Gautier, J.F.; Villain, M.; Tadayoni, R.; Carriere, I.; Massin, P. Ten-year incidence and assessment of safe screening intervals for diabetic retinopathy: The OPHDIAT study. Br. J. Ophthalmol. 2021, 105, 432–439. [Google Scholar] [CrossRef]
- Soulié-Strougar, M.; Charles, A.; Métral, P.; Quercia, P.; Souchier, M.; Chirpaz, L.; Bron, A.; Creuzot-Garcher, C. Screening diabetic retinopathy in Burgundy with an itinerant nonmydriatic camera. J. Fr. D’ophtalmologie 2007, 30, 121–126. [Google Scholar] [CrossRef]
- Scailteux, L.M.; Droitcourt, C.; Balusson, F.; Nowak, E.; Kerbrat, S.; Dupuy, A.; Drezen, E.; Happe, A.; Oger, E. French administrative health care database (SNDS): The value of its enrichment. Therapie 2019, 74, 215–223. [Google Scholar] [CrossRef]
- Institut National de la Statistique et des Études Économiques (INSEE). Demographics Bulletin 2019. Available online: https://www.insee.fr/fr/statistiques/1892088?sommaire=1912926 (accessed on 30 April 2021).
- Assurance Maladie. Personnes Prises en Charge Pour Diabète en 2018. Available online: https://www.ameli.fr/sites/default/files/2018_fiche_diabete.pdf (accessed on 1 December 2021).
- Sante Publique France. Prévalence et Incidence du Diabète. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/diabete/articles/prevalence-et-incidence-du-diabete (accessed on 1 December 2021).
- Fuentes, S.; Cosson, E.; Mandereau-Bruno, L.; Fagot-Campagna, A.; Bernillon, P.; Goldberg, M.; Fosse-Edorh, S.; CONSTANCES-Diab Group. Identifying diabetes cases in health administrative databases: A validation study based on a large French cohort. Int. J. Public Health 2019, 64, 441–450. [Google Scholar] [CrossRef]
- Massin, P.; Creuzot-Garcher, C.; Kodjikian, L.; Girmens, J.F.; Delcourt, C.; Fajnkuchen, F.; Glacet-Bernard, A.; Guillausseau, P.J.; Ponthieux, A.; Blin, P.; et al. Real-World Outcomes with Ranibizumab 0.5 mg in Patients with Visual Impairment due to Diabetic Macular Edema: 12-Month Results from the 36-Month BOREAL-DME Study. Ophthalmic Res. 2019, 62, 101–110. [Google Scholar] [CrossRef]
- Wu, Y.; Ai, P.; Ai, Z.; Xu, G. Subthreshold diode micropulse laser versus conventional laser photocoagulation monotherapy or combined with anti-VEGF therapy for diabetic macular edema: A Bayesian network meta-analysis. Biomed. Pharmacother. Biomed. Pharmacother. 2018, 97, 293–299. [Google Scholar] [CrossRef]
- Hrarat, L.; Fajnkuchen, F.; Boubaya, M.; Levy, V.; Sarda, V.; Grenet, T.; Nghiem-Buffet, S.; Chaine, G.; Giocanti-Auregan, A. Outcomes after a 1-Year Treatment with Ranibizumab for Diabetic Macular Edema in a Clinical Setting. Ophthalmol. J. Int. D’ophtalmol. Int. J. Ophthalmol. Z. Augenheilkd. 2016, 236, 207–214. [Google Scholar] [CrossRef]
- Malcles, A.; Dot, C.; Voirin, N.; Agard, E.; Vie, A.L.; Bellocq, D.; Denis, P.; Kodjikian, L. Real-life study in diabetic macular edema treated with dexamethasone implant: The Reldex Study. Retina 2017, 37, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Korobelnik, J.F.; Daien, V.; Faure, C.; Tadayoni, R.; Giocanti-Auregan, A.; Dot, C.; Kodjikian, L.; Massin, P. Real-world outcomes following 12 months of intravitreal aflibercept monotherapy in patients with diabetic macular edema in France: Results from the APOLLON study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 521–528. [Google Scholar] [CrossRef] [Green Version]
- Lestable, L.; Gabrielle, P.H.; Bron, A.M.; Nguyen, P.; Creuzot-Garcher, C. Twelve-month outcomes of intra-vitreal anti-VEGF agents for treatment-naive neovascular age-related macular degeneration eyes: French data from the fight for retinal blindness! J. Fr. Ophtalmol. 2020, 43, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Bandello, F.; Cicinelli, M.V. 19th EURETINA Congress Keynote Lecture: Diabetic Retinopathy Today. Int. J. Ophthalmol. Z. Augenheilkd. 2020, 243, 163–171. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Chong, V.; Loewenstein, A.; Larsen, M.; Souied, E.; Schlingemann, R.; Eldem, B.; Mones, J.; Richard, G.; Bandello, F.; et al. Guidelines for the management of neovascular age-related macular degeneration by the European Society of Retina Specialists (EURETINA). Br. J. Ophthalmol. 2014, 98, 1144–1167. [Google Scholar] [CrossRef] [PubMed]
- Martin-Merino, E.; Fortuny, J.; Rivero-Ferrer, E.; Garcia-Rodriguez, L.A. Incidence of retinal complications in a cohort of newly diagnosed diabetic patients. PLoS ONE 2014, 9, e100283. [Google Scholar] [CrossRef] [PubMed]
- Varma, R.; Choudhury, F.; Klein, R.; Chung, J.; Torres, M.; Azen, S.P.; Los Angeles Latino Eye Study, G. Four-year incidence and progression of diabetic retinopathy and macular edema: The Los Angeles Latino Eye Study. Am. J. Ophthalmol. 2010, 149, 752–761.e1–3. [Google Scholar] [CrossRef] [Green Version]
- Romero-Aroca, P.; Navarro-Gil, R.; Valls-Mateu, A.; Sagarra-Alamo, R.; Moreno-Ribas, A.; Soler, N. Differences in incidence of diabetic retinopathy between type 1 and 2 diabetes mellitus: A nine-year follow-up study. Br. J. Ophthalmol. 2017, 101, 1346–1351. [Google Scholar] [CrossRef] [Green Version]
- Li, J.Q.; Welchowski, T.; Schmid, M.; Letow, J.; Wolpers, C.; Pascual-Camps, I.; Holz, F.G.; Finger, R.P. Prevalence, incidence and future projection of diabetic eye disease in Europe: A systematic review and meta-analysis. Eur. J. Epidemiol. 2020, 35, 11–23. [Google Scholar] [CrossRef]
- Thomas, R.L.; Halim, S.; Gurudas, S.; Sivaprasad, S.; Owens, D.R. IDF Diabetes Atlas: A review of studies utilising retinal photography on the global prevalence of diabetes related retinopathy between 2015 and 2018. Diabetes Res. Clin. Pract. 2019, 157, 107840. [Google Scholar] [CrossRef]
- Yau, J.W.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Poncelas, A.; Miravet-Jimenez, S.; Casellas, A.; Barrot-De La Puente, J.F.; Franch-Nadal, J.; Lopez-Simarro, F.; Mata-Cases, M.; Mundet-Tuduri, X. Prevalence of diabetic retinopathy in individuals with type 2 diabetes who had recorded diabetic retinopathy from retinal photographs in Catalonia (Spain). Br. J. Ophthalmol. 2015, 99, 1628–1633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vujosevic, S.; Pucci, P.; Casciano, M.; Daniele, A.; Bini, S.; Berton, M.; Cavarzeran, F.; Avogaro, A.; Lapolla, A.; Midena, E. A decade-long telemedicine screening program for diabetic retinopathy in the north-east of Italy. J. Diabetes Complic. 2017, 31, 1348–1353. [Google Scholar] [CrossRef]
- Bursell, S.E.; Fonda, S.J.; Lewis, D.G.; Horton, M.B. Prevalence of diabetic retinopathy and diabetic macular edema in a primary care-based teleophthalmology program for American Indians and Alaskan Natives. PLoS ONE 2018, 13, e0198551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, N.; Hjortdal, J.O.; Schielke, K.C.; Bek, T.; Grauslund, J.; Laugesen, C.S.; Lund-Andersen, H.; Cerqueira, C.; Andresen, J. The Danish Registry of Diabetic Retinopathy. Clin. Epidemiol. 2016, 8, 613–619. [Google Scholar] [CrossRef] [Green Version]
- Dutra Medeiros, M.; Mesquita, E.; Papoila, A.L.; Genro, V.; Raposo, J.F. First diabetic retinopathy prevalence study in Portugal: RETINODIAB Study--evaluation of the screening programme for Lisbon and Tagus Valley region. Br. J. Ophthalmol. 2015, 99, 1328–1333. [Google Scholar] [CrossRef]
- Wong, T.Y.; Klein, R.; Islam, F.M.; Cotch, M.F.; Folsom, A.R.; Klein, B.E.; Sharrett, A.R.; Shea, S. Diabetic retinopathy in a multi-ethnic cohort in the United States. Am. J. Ophthalmol. 2006, 141, 446–455. [Google Scholar] [CrossRef] [Green Version]
- Naik, S.; Wykoff, C.C.; Ou, W.C.; Stevenson, J.; Gupta, S.; Shah, A.R. Identification of factors to increase efficacy of telemedicine screening for diabetic retinopathy in endocrinology practices using the Intelligent Retinal Imaging System (IRIS) platform. Diabetes Res. Clin. Pract. 2018, 140, 265–270. [Google Scholar] [CrossRef]
- Thomas, R.L.; Dunstan, F.; Luzio, S.D.; Roy Chowdury, S.; Hale, S.L.; North, R.V.; Gibbins, R.L.; Owens, D.R. Incidence of diabetic retinopathy in people with type 2 diabetes mellitus attending the Diabetic Retinopathy Screening Service for Wales: Retrospective analysis. BMJ 2012, 344, e874. [Google Scholar] [CrossRef] [Green Version]
- Varma, R.; Torres, M.; Los Angeles Latino Eye Study Group. Prevalence of lens opacities in Latinos: The Los Angeles Latino Eye Study. Ophthalmology 2004, 111, 1449–1456. [Google Scholar] [CrossRef]
- Ondrejkova, M.; Jackuliak, P.; Martinka, E.; Mokan, M.; Foley, J.; Fabkova, J.; Gecik, K.; Tvrda, I.; Helbich, M.; Gajdosova, M.; et al. Prevalence and epidemiological characteristics of patients with diabetic retinopathy in Slovakia: 12-month results from the DIARET SK study. PLoS ONE 2019, 14, e0223788. [Google Scholar] [CrossRef] [Green Version]
- Mathur, R.; Bhaskaran, K.; Edwards, E.; Lee, H.; Chaturvedi, N.; Smeeth, L.; Douglas, I. Population trends in the 10-year incidence and prevalence of diabetic retinopathy in the UK: A cohort study in the Clinical Practice Research Datalink 2004–2014. BMJ Open 2017, 7, e014444. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.L.; Dunstan, F.D.; Luzio, S.D.; Chowdhury, S.R.; North, R.V.; Hale, S.L.; Gibbins, R.L.; Owens, D.R. Prevalence of diabetic retinopathy within a national diabetic retinopathy screening service. Br. J. Ophthalmol. 2015, 99, 64–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zureik, A.; Julla, J.B.; Erginay, A.; Vidal-Trecan, T.; Juddoo, V.; Gautier, J.F.; Massin, P.; Tadayoni, R.; Riveline, J.P.; Couturier, A. Prevalence, severity stages, and risk factors of diabetic retinopathy in 1464 adult patients with type 1 diabetes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 3613–3623. [Google Scholar] [CrossRef]
- Cougnard-Grégoire, A.; Korobelnik, J.F.; Delyfer, M.N.; Rigalleau, V.; Daien, V.; Creuzot-Garcher, C.; Delcourt, C. Trends in the Use of Eye Care Services in Adults Treated for Diabetes between 2008 and 2017 in France: A Nationwide Study. Ophthalmic Res. 2020, 63, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Baudin, F.; Benzenine, E.; Mariet, A.S.; Bron, A.M.; Daien, V.; Korobelnik, J.F.; Quantin, C.; Creuzot-Garcher, C. Association of Acute Endophthalmitis With Intravitreal Injections of Corticosteroids or Anti-Vascular Growth Factor Agents in a Nationwide Study in France. JAMA Ophthalmol. 2018, 136, 1352–1358. [Google Scholar] [CrossRef] [Green Version]
- Fuentes, S.; Mandereau-Bruno, L.; Regnault, N.; Bernillon, P.; Bonaldi, C.; Cosson, E.; Fosse-Edorh, S. Is the type 2 diabetes epidemic plateauing in France? A nationwide population-based study. Diabetes Metab. 2020, 46, 472–479. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treated DME Patients N = 11,901 | Treated PDR Patients N = 11,996 | ||
|---|---|---|---|
| Sex | Male | 6881 (57.8%) | 7078 (59.0%) |
| Female | 5020 (42.2%) | 4918 (41.0%) | |
| Age, years | N | 11,901 (100.0) | 11,996 (100%) |
| Mean (SD) | 66.3 (9.6) | 65.1 (13.0) | |
| Median (Q1–Q3) | 68.0 (61.0–73.0) | 66.0 (58.0–74.0) | |
| Range | (18.0–79.0) | (18.0–99.0) | |
| Ocular diseases | Cataract surgery 1 | 3401 (28.6%) | 3284 (27.4%) |
| Treated dry eye disease 2 | 3608 (30.3%) | 2683 (22.4%) | |
| Treated ocular hypertension 2,3 | 1845 (15.5%) | 1835 (15.3%) | |
| Non-ocular diseases | Hypertension 4 | 9329 (78.4%) | 9065 (75.6%) |
| Acute coronary syndrome | 509 (4.3%) | 567 (4.7%) | |
| Chronic coronary syndrome | 1874 (15.7%) | 1910 (15.9%) | |
| Obliterating peripheral arterial disease | 845 (7.1%) | 930 (7.8%) | |
| Stroke 5 | 1476 (12.4%) | 1821 (15.2%) | |
| Dementia | 160 (1.3%) | 224 (1.9%) | |
| Renal disease | 1535 (12.9%) | 1637 (13.6%) | |
| Non-metastatic cancer | 1533 (12.9%) | 1471 (12.3%) |
| Treated DME Annual Incidence | Treated DME Prevalence | Treated PDR Annual Incidence | Treated PDR Prevalence | |||||
|---|---|---|---|---|---|---|---|---|
| Patients Treated for Condition per 10,000 Population | ||||||||
| General Population | Population with Diabetes | General Population | Population with Diabetes | General Population | Population with Diabetes | General Population | Population with Diabetes | |
| Cumulative age groups (years) | ||||||||
| Total ≥ 18 (All) | 2.5 | 37.3 | 9.5 | 143.7 | 2.3 | 31.2 | 19.9 | 270.3 |
| ≥30 | 3 | 37.5 | 11.7 | 145 | 2.8 | 31.1 | 24.1 | 271.6 |
| ≥40 | 3.8 | 38 | 14.7 | 146.9 | 3.3 | 30.7 | 29 | 270.1 |
| ≥50 | 5.1 | 39.8 | 19.9 | 155.1 | 4.1 | 30.6 | 36.8 | 275.2 |
| ≥60 | 7.2 | 44.7 | 28.6 | 177.7 | 5 | 30.9 | 47.6 | 295.6 |
| ≥70 | 9.8 | 53.2 | 40.5 | 219 | 5 | 28.7 | 54.7 | 313.7 |
| ≥80 | - | - | - | - | 3.7 | 23 | 46.8 | 289.8 |
| Age groups (years) | ||||||||
| 18–29 | 0.1 | 17.7 | 0.2 | 44.1 | 0.2 | 40.8 | 0.7 | 153.7 |
| 30–39 | 0.2 | 21 | 0.7 | 71.8 | 0.5 | 49.3 | 3.3 | 342.1 |
| 40–44 | 0.3 | 15.5 | 1.1 | 49.8 | 0.7 | 31.3 | 4.6 | 217.9 |
| 45–49 | 0.6 | 18.1 | 2.1 | 58.2 | 1.1 | 31.6 | 6.8 | 189.5 |
| 50–54 | 1.3 | 21.7 | 4.6 | 75.1 | 1.7 | 28.4 | 11.3 | 185 |
| 55–59 | 2.7 | 27.4 | 9.3 | 94 | 3 | 30.7 | 19.8 | 200.3 |
| 60–64 | 4.4 | 30.4 | 16.6 | 114.5 | 4.3 | 30 | 32 | 221.4 |
| 65–69 | 6.6 | 45.1 | 25.3 | 173.4 | 5.5 | 37.8 | 46.9 | 320.6 |
| 70–74 | 9 | 56.1 | 36.8 | 232.2 | 6.4 | 39.8 | 60.8 | 383.2 |
| 75–79 | 11.8 | 50.3 | 45.6 | 205.7 | 5.7 | 25.2 | 61.2 | 276.1 |
| 80–84 | - | - | - | - | 4.8 | 23.2 | 55.4 | 274.8 |
| ≥85 years | - | - | - | - | 3.1 | 22.8 | 39.4 | 310.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Creuzot-Garcher, C.; Massin, P.; Srour, M.; Baudin, F.; Dot, C.; Nghiem-Buffet, S.; Girmens, J.-F.; Collin, C.; Ponthieux, A.; Delcourt, C. Epidemiology of Treated Diabetes Ocular Complications in France 2008–2018—The LANDSCAPE French Nationwide Study. Pharmaceutics 2022, 14, 2330. https://doi.org/10.3390/pharmaceutics14112330
Creuzot-Garcher C, Massin P, Srour M, Baudin F, Dot C, Nghiem-Buffet S, Girmens J-F, Collin C, Ponthieux A, Delcourt C. Epidemiology of Treated Diabetes Ocular Complications in France 2008–2018—The LANDSCAPE French Nationwide Study. Pharmaceutics. 2022; 14(11):2330. https://doi.org/10.3390/pharmaceutics14112330
Chicago/Turabian StyleCreuzot-Garcher, Catherine, Pascale Massin, Mayer Srour, Florian Baudin, Corinne Dot, Sylvia Nghiem-Buffet, Jean-Francois Girmens, Cedric Collin, Anne Ponthieux, and Cecile Delcourt. 2022. "Epidemiology of Treated Diabetes Ocular Complications in France 2008–2018—The LANDSCAPE French Nationwide Study" Pharmaceutics 14, no. 11: 2330. https://doi.org/10.3390/pharmaceutics14112330
APA StyleCreuzot-Garcher, C., Massin, P., Srour, M., Baudin, F., Dot, C., Nghiem-Buffet, S., Girmens, J. -F., Collin, C., Ponthieux, A., & Delcourt, C. (2022). Epidemiology of Treated Diabetes Ocular Complications in France 2008–2018—The LANDSCAPE French Nationwide Study. Pharmaceutics, 14(11), 2330. https://doi.org/10.3390/pharmaceutics14112330