

TIMolol Nasal Spray as a Treatment for Epistaxis in Hereditary Hemorrhagic Telangiectasia (TIM-HHT)—A Prospective, Randomized, Double-Blind, Controlled, Cross-Over Trial
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
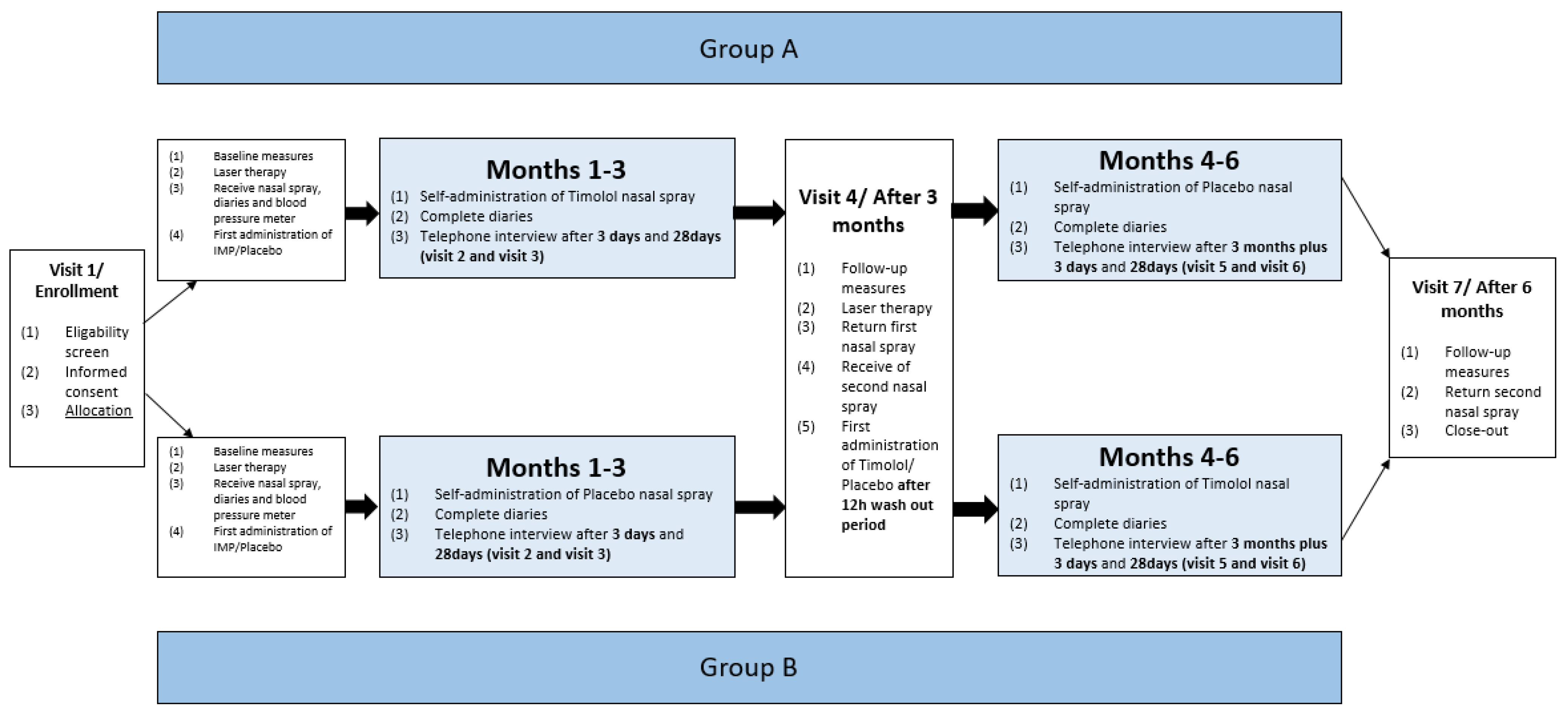
2.1. Study Design, Approval and Registration
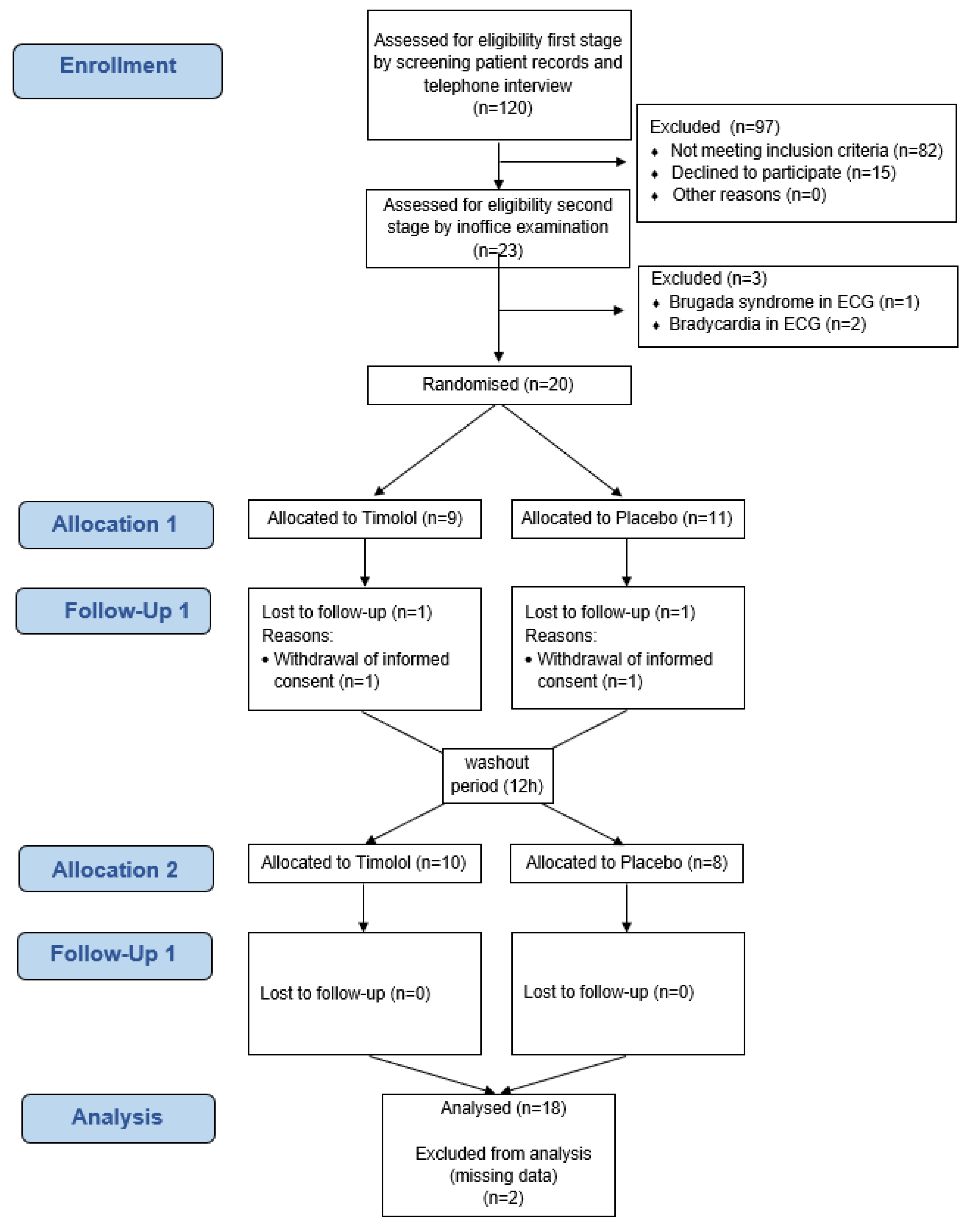
2.2. Recruitment of Patients
2.3. Randomization and Blinding
2.4. Methodology
2.5. Sample Size
2.6. Study Medication
2.7. Study Endpoints
2.8. Safety and Compliance
2.9. Statistical Analyses
3. Results
3.1. Trial Population
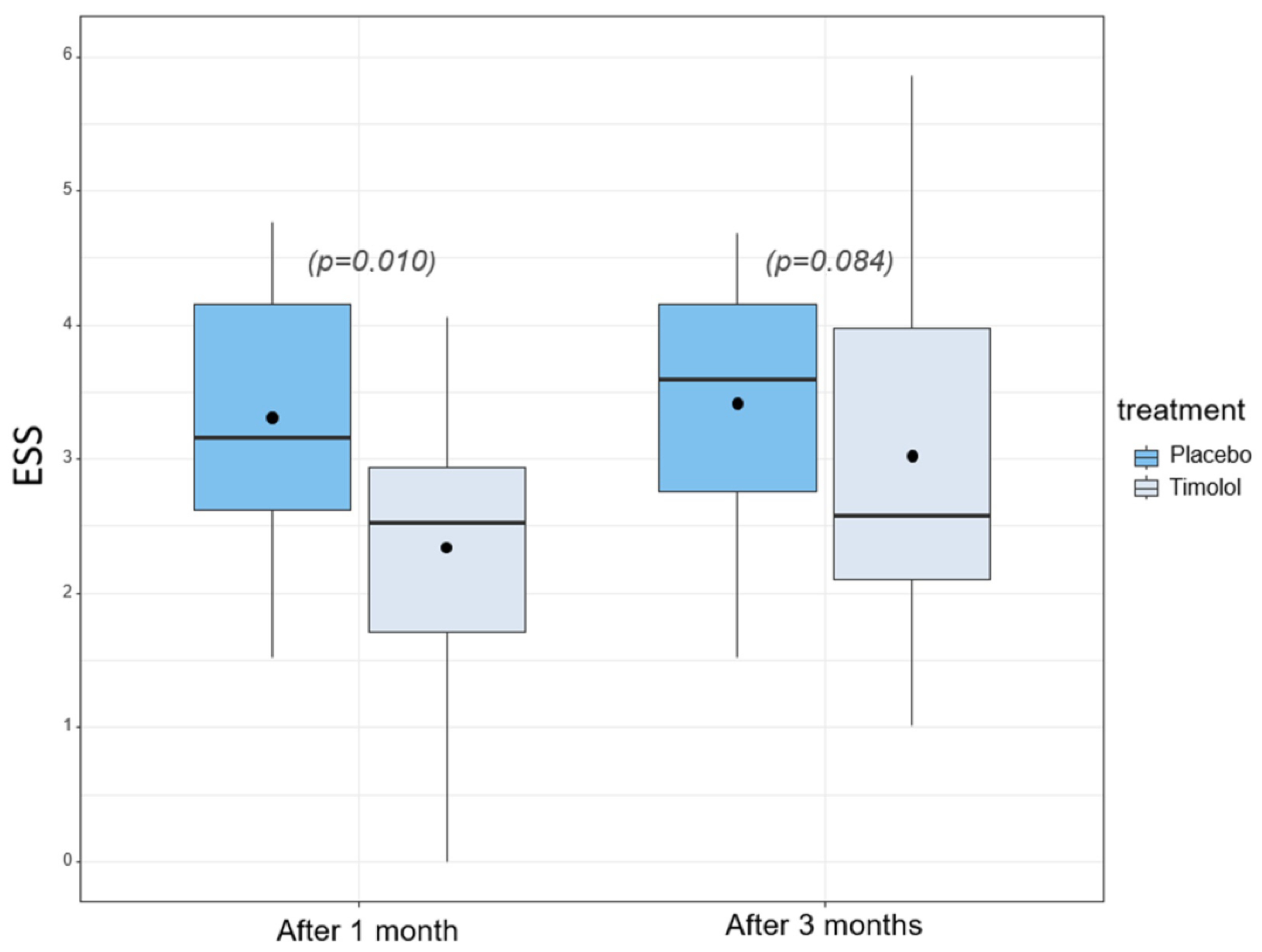
3.2. Response to Treatment
3.3. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Geisthoff, U.W.; Schneider, G.; Fischinger, J.; Plinkert, P.K. Hereditäre hämorrhagische Teleangiektasie (Morbus Osler). Eine interdisziplinäre Herausforderung. HNO 2002, 50, 114–128. [Google Scholar] [CrossRef] [PubMed]
- Zarrabeitia, R.; Fariñas-Álvarez, C.; Santibáñez, M.; Señaris, B.; Fontalba, A.; Botella, L.M.; Parra, J.A. Quality of life in patients with hereditary haemorrhagic telangiectasia (HHT). Health Qual. Life Outcomes 2017, 15, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faughnan, M.E.; Mager, J.J.; Hetts, S.W.; Palda, V.A.; Lang-Robertson, K.; Buscarini, E.; Deslandres, E.; Kasthuri, R.S.; Lausman, A.; Poetker, D.; et al. Second International Guidelines for the Diagnosis and Management of Hereditary Hemorrhagic Telangiectasia. Ann. Intern. Med. 2020, 173, 989–1001. [Google Scholar] [CrossRef]
- Olitsky, S.E. Topical timolol for the treatment of epistaxis in hereditary hemorrhagic telangiectasia. Am. J. Otolaryngol. 2012, 33, 375–376. [Google Scholar] [CrossRef]
- Stiles, J.; Amaya, C.; Pham, R.; Rowntree, R.K.; Lacaze, M.; Mulne, A.; Bischoff, J.; Kokta, V.; Boucheron, L.E.; Mitchell, D.C.; et al. Propranolol treatment of infantile hemangioma endothelial cells: A molecular analysis. Exp. Ther. Med. 2012, 4, 594–604. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.; Hardy, K.L.; Kitajewski, A.M.; Shawber, C.J.; Kitajewski, J.K.; Wu, J.K. Propranolol accelerates adipogenesis in hemangioma stem cells and causes apoptosis of hemangioma endothelial cells. Plast. Reconstr. Surg. 2012, 130, 1012–1021. [Google Scholar] [CrossRef] [Green Version]
- Seebauer, C.T.; Graus, M.S.; Huang, L.; McCann, A.; Wylie-Sears, J.; Fontaine, F.; Karnezis, T.; Zurakowski, D.; Staffa, S.J.; Meunier, F.; et al. Non-beta blocker enantiomers of propranolol and atenolol inhibit vasculogenesis in infantile hemangioma. J. Clin. Investig. 2022, 132, 3. [Google Scholar] [CrossRef]
- Ichimura, K.; Kikuchi, H.; Imayoshi, S.; Dias, M.S. Topical application of timolol decreases the severity and frequency of epistaxis in patients who have previously undergone nasal dermoplasty for hereditary hemorrhagic telangiectasia. Auris Nasus Larynx 2016, 43, 429–432. [Google Scholar] [CrossRef]
- Epperla, N.; Brilliant, M.H.; Vidaillet, H. Topical timolol for treatment of epistaxis in hereditary haemorrhagic telangiectasia associated with bradycardia: A look at CYP2D6 metabolising variants. Case Rep. 2014, 2014, bcr2013203056. [Google Scholar] [CrossRef] [Green Version]
- Andorfer, K.E.C.; Seebauer, C.T.; Koller, M.; Zeman, F.; Berneburg, M.; Fischer, R.; Vielsmeier, V.; Bohr, C.; Kühnel, T.S. TIMolol nasal spray as a treatment for epistaxis in hereditary hemorrhagic telangiectasia (HHT)—Study protocol of the prospective, randomized, double-blind, controlled cross-over TIM-HHT trial. Clin. Hemorheol. Microcirc. 2022, 80, 307–315. [Google Scholar] [CrossRef]
- Wirsching, K.E.C.; Kühnel, T.S. Update on Clinical Strategies in Hereditary Hemorrhagic Telangiectasia from an ENT Point of View. Clin. Exp. Otorhinolaryngol. 2017, 10, 153–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seebauer, C.T.; Kuehnel, T.; Uller, W.; Bohr, C.; Andorfer, K.E. Diagnostik und Behandlung der hereditären hämorrhagischen Teleangiektasie. Laryngo Rhino Otol. 2020, 99, 682–693. [Google Scholar] [CrossRef]
- Volotinen, M.; Hakkola, J.; Pelkonen, O.; Vapaatalo, H.; Mäenpää, J. Metabolism of ophthalmic timolol: New aspects of an old drug. Basic Clin. Pharmacol. Toxicol. 2011, 108, 297–303. [Google Scholar] [CrossRef]
- Hoag, J.B.; Terry, P.; Mitchell, S.; Reh, D.; Merlo, C.A. An epistaxis severity score for hereditary hemorrhagic telangiectasia. Laryngoscope 2010, 120, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.X.; Reh, D.D.; Hoag, J.B.; Mitchell, S.E.; Mathai, S.C.; Robinson, G.M.; Merlo, C.A. The minimal important difference of the epistaxis severity score in hereditary hemorrhagic telangiectasia. Laryngoscope 2016, 126, 1029–1032. [Google Scholar] [CrossRef] [PubMed]
- Slotosch, D.; Koller, M.; Werner, J.A.; Folz, B.J. Rezidivierende Epistaxis bei hereditärer hämorrhagischer Teleangiektasie–Isoliertes Symptom oder Einschränkung der Lebensqualität? Dtsch. Med. Wochenschr. 2006, 131, 535–539. [Google Scholar] [CrossRef] [PubMed]
- The EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Mäenpää, J.; Pelkonen, O. Cardiac safety of ophthalmic timolol. Expert Opin. Drug Saf. 2016, 15, 1549–1561. [Google Scholar] [CrossRef]
- Dupuis-Girod, S.; Pitiot, V.; Bergerot, C.; Fargeton, A.-E.; Beaudoin, M.; Decullier, E.; Bréant, V.; Colombet, B.; Philouze, P.; Faure, F.; et al. Efficacy of TIMOLOL nasal spray as a treatment for epistaxis in hereditary hemorrhagic telangiectasia. A double-blind, randomized, placebo-controlled trial. Sci. Rep. 2019, 9, 11986. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, K.J.; Sautter, N.B.; McWilliams, J.P.; Chakinala, M.M.; Merlo, C.A.; Johnson, M.H.; James, M.; Everett, E.M.; Clancy, M.S.; Faughnan, M.E.; et al. Effect of Topical Intranasal Therapy on Epistaxis Frequency in Patients With Hereditary Hemorrhagic Telangiectasia: A Randomized Clinical Trial. JAMA 2016, 316, 943–951. [Google Scholar] [CrossRef]
- Peterson, A.M.; Lee, J.J.; Kallogjeri, D.; Schneider, J.S.; Chakinala, M.M.; Piccirillo, J.F. Efficacy of Timolol in a Novel Intranasal Thermosensitive Gel for Hereditary Hemorrhagic Telangiectasia-Associated Epistaxis: A Randomized Clinical Trial. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Peterson, A.M.; Kallogjeri, D.; Spitznagel, E.; Chakinala, M.M.; Schneider, J.S.; Piccirillo, J.F. Development and Validation of the Nasal Outcome Score for Epistaxis in Hereditary Hemorrhagic Telangiectasia (NOSE HHT). JAMA Otolaryngol. Head Neck Surg. 2020, 146, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Haubner, F.; Schneider, A.; Schinke, H.; Bertlich, M.; Weiss, B.G.; Canis, M.; Kashani, F. Classification of endonasal HHT lesions using digital microscopy. Orphanet J. Rare Dis. 2021, 16, 182. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | Value | Study Population (n = 18) |
|---|---|---|
| Age | Mean (SD), range | 49.9 (12.9), 24–76 |
| Gender (male/female) | No. (%) | 11 (61%)/7 (39%) |
| Blood pressure systolic | Mean (SD), range | 136 (16), 103–171 |
| Blood pressure diastolic | Mean (SD), range | 84 (10), 68–106 |
| Hemoglobin [g/dL] | Median (IQR) | 12.1 (10.0, 14.3) |
| Ferritin [ug/L] | Median (IQR) | 39.4 (13.6, 56.8) |
| Transferrin [mg/dL] | Median (IQR) | 294.5 (257.8, 346.3) |
| ESS baseline | Mean (SD), range | 3.9 (1.4), 2.07–6.88 |
| NRS baseline | Mean (SD), range | 5.9 (2.4), 0–9 |
| EQ-5D-3L score (utility score) | Mean (SD), range | 0.96 (0.06), 0.89–1 |
| EQ-5D-3L VAS | Mean (SD), range | 75 (18), 30–95 |
| HHT-related QoL | Median (IQR) | 4 (3, 7) |
| Placebo (n = 18) | Timolol (n = 18) | Method of Analysis | Δ (95% CI) | p Value |
|---|---|---|---|---|
| 3.4 (SD 1.0) | 3.0 (SD 1.4) | Paired t-Test | −0.39 (−0.84, 0.06) | 0.084 |
| Mixed model a | −0.42 (−0.86, 0.01) | 0.057 |
| Placebo (n = 18) | Timolol (n = 18) | Δ (95% CI) | p Value | |
|---|---|---|---|---|
| 1 month assessments | ||||
| ESS | 3.3 (SD 1.1) | 2.3 (SD 1.1) | −0.97 (−1.67, −0.27) | 0.010 |
| NRS | 5.8 (SD 1.9) | 7.5 (SD 1.8) | 1.7 (0.6, 2.7) | 0.005 |
| 3 months assessments | ||||
| NRS | 5.8 (SD 2.3) | 6.8 (SD 2.6) | 1.0 (−0.3, 2.3) | 0.117 |
| Hemoglobin a [g/dL] | 11.9 (10.3, 14.8) | 12.4 (11.5, 14.5) | 0.35(−0.25, 1.10) * | 0.236 |
| Ferritin [ug/L] | 27.2 (11.9, 41.6) | 36.9 (23.4, 56.9) | 9.9 (0.3, 20.9) * | 0.043 |
| Transferrin [mg/dL] | 309 (288, 345) | 301 (250, 332) | −22 (−37, −1) * | 0.039 |
| EQ-5D-3L (utility score) | 0.96 (SD 0.05) | 0.96 (SD 0.10) | 0.00 (−0.06, 0.05) | 0.863 |
| EQ-5D-3L (VAS) | 72.8 (SD 18.2) | 75.2 (SD 17.4) | 2.4 (−3.9, 8.6) | 0.439 |
| HHT-related QoL | 4 (3, 7) | 4 (2, 7) | −1 (−2, 0) * | 0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andorfer, K.E.C.; Zeman, F.; Koller, M.; Zeller, J.; Fischer, R.; Seebauer, C.T.; Vielsmeier, V.; Bohr, C.; Kühnel, T.S. TIMolol Nasal Spray as a Treatment for Epistaxis in Hereditary Hemorrhagic Telangiectasia (TIM-HHT)—A Prospective, Randomized, Double-Blind, Controlled, Cross-Over Trial. Pharmaceutics 2022, 14, 2335. https://doi.org/10.3390/pharmaceutics14112335
Andorfer KEC, Zeman F, Koller M, Zeller J, Fischer R, Seebauer CT, Vielsmeier V, Bohr C, Kühnel TS. TIMolol Nasal Spray as a Treatment for Epistaxis in Hereditary Hemorrhagic Telangiectasia (TIM-HHT)—A Prospective, Randomized, Double-Blind, Controlled, Cross-Over Trial. Pharmaceutics. 2022; 14(11):2335. https://doi.org/10.3390/pharmaceutics14112335
Chicago/Turabian StyleAndorfer, Kornelia E. C., Florian Zeman, Michael Koller, Judith Zeller, René Fischer, Caroline T. Seebauer, Veronika Vielsmeier, Christopher Bohr, and Thomas S. Kühnel. 2022. "TIMolol Nasal Spray as a Treatment for Epistaxis in Hereditary Hemorrhagic Telangiectasia (TIM-HHT)—A Prospective, Randomized, Double-Blind, Controlled, Cross-Over Trial" Pharmaceutics 14, no. 11: 2335. https://doi.org/10.3390/pharmaceutics14112335
APA StyleAndorfer, K. E. C., Zeman, F., Koller, M., Zeller, J., Fischer, R., Seebauer, C. T., Vielsmeier, V., Bohr, C., & Kühnel, T. S. (2022). TIMolol Nasal Spray as a Treatment for Epistaxis in Hereditary Hemorrhagic Telangiectasia (TIM-HHT)—A Prospective, Randomized, Double-Blind, Controlled, Cross-Over Trial. Pharmaceutics, 14(11), 2335. https://doi.org/10.3390/pharmaceutics14112335