
Understanding the Impact of Age-Related Changes in Pediatric GI Solubility by Multivariate Data Analysis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Instrumentation
2.3. Drugs
2.4. Solubility Studies
2.5. Chromatographic Conditions for the Analysis of the Solubility Samples
2.6. Treatment of In Vitro Solubility Data
2.7. Statistical Analysis
3. Results
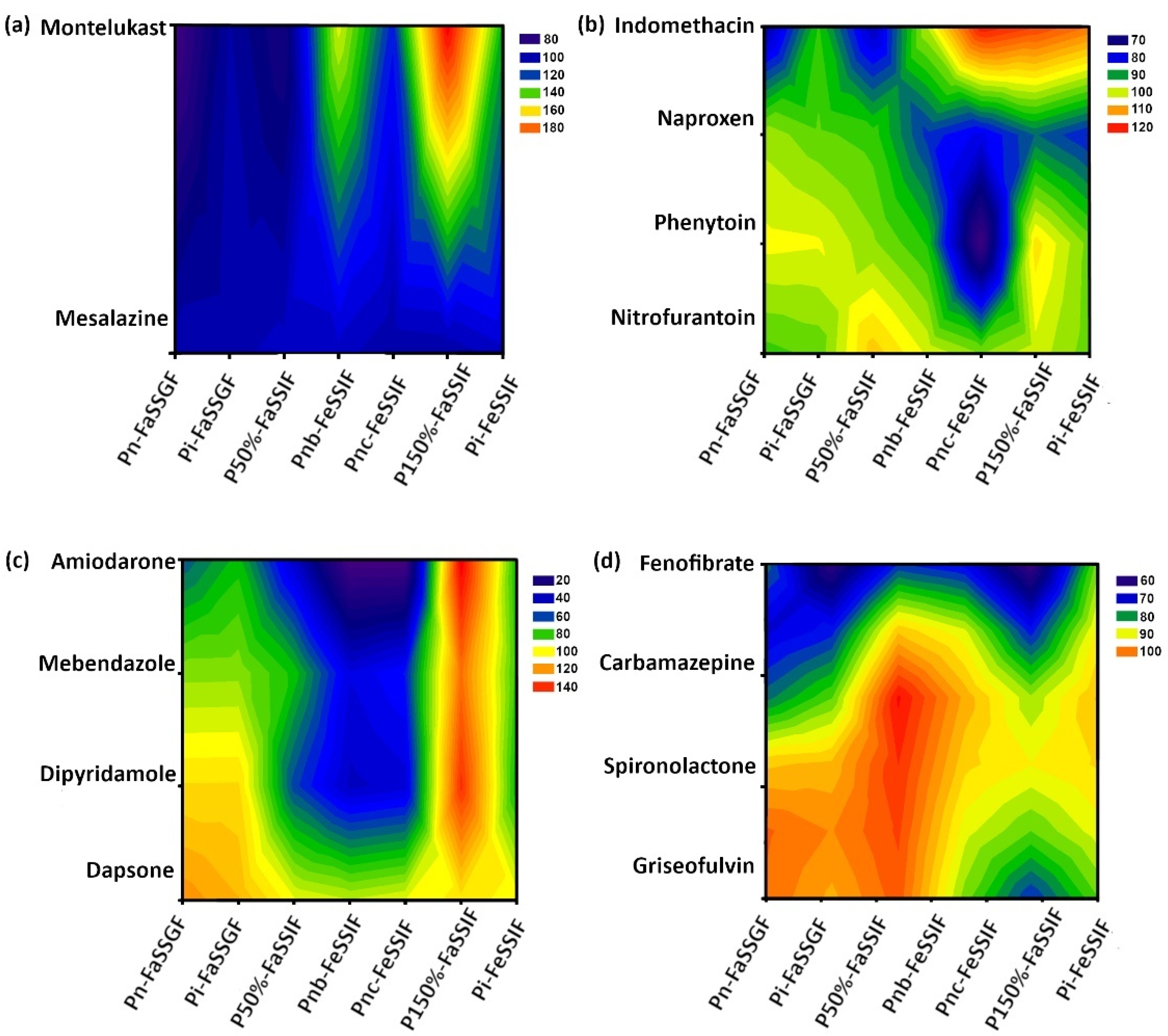
3.1. Drug Solubility Assessments
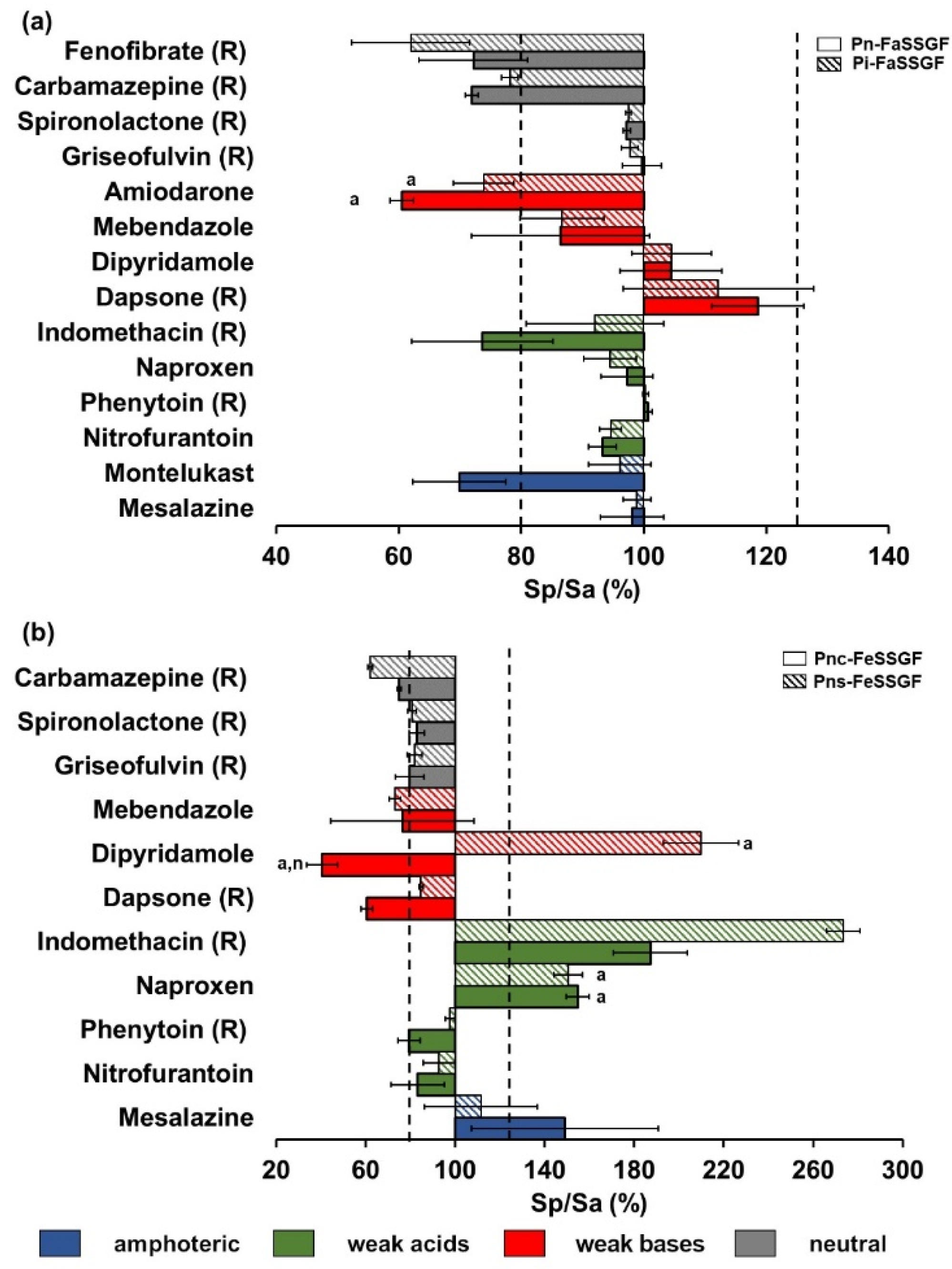
3.1.1. Fasted Gastric Simulated Fluids
3.1.2. Fed Gastric Simulated Fluids
3.1.3. Fasted Intestinal Simulated Fluids
3.1.4. Fed Intestinal Simulated Fluids
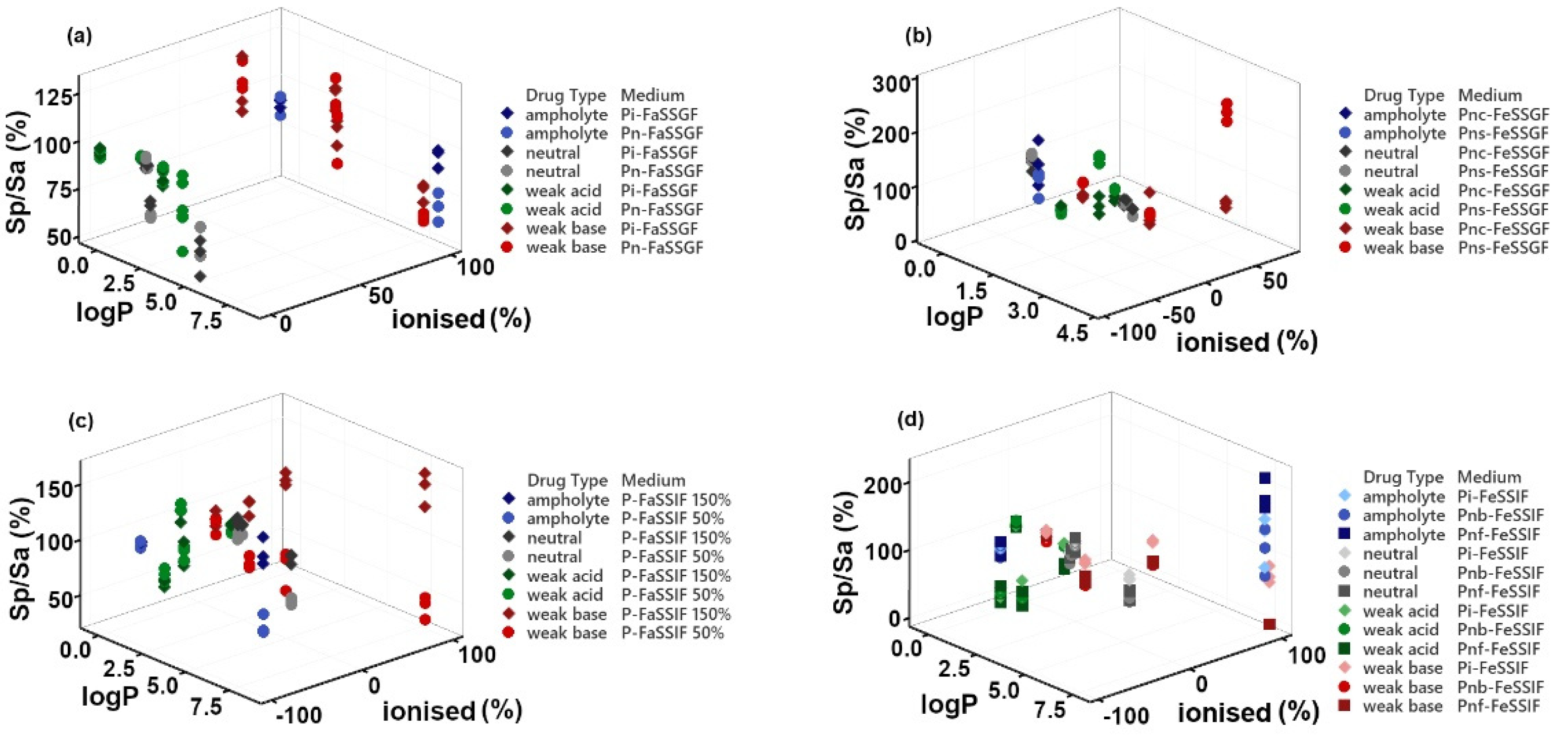
3.2. Correlation of Drugs’ Physicochemical Properties and Solubility Ratio
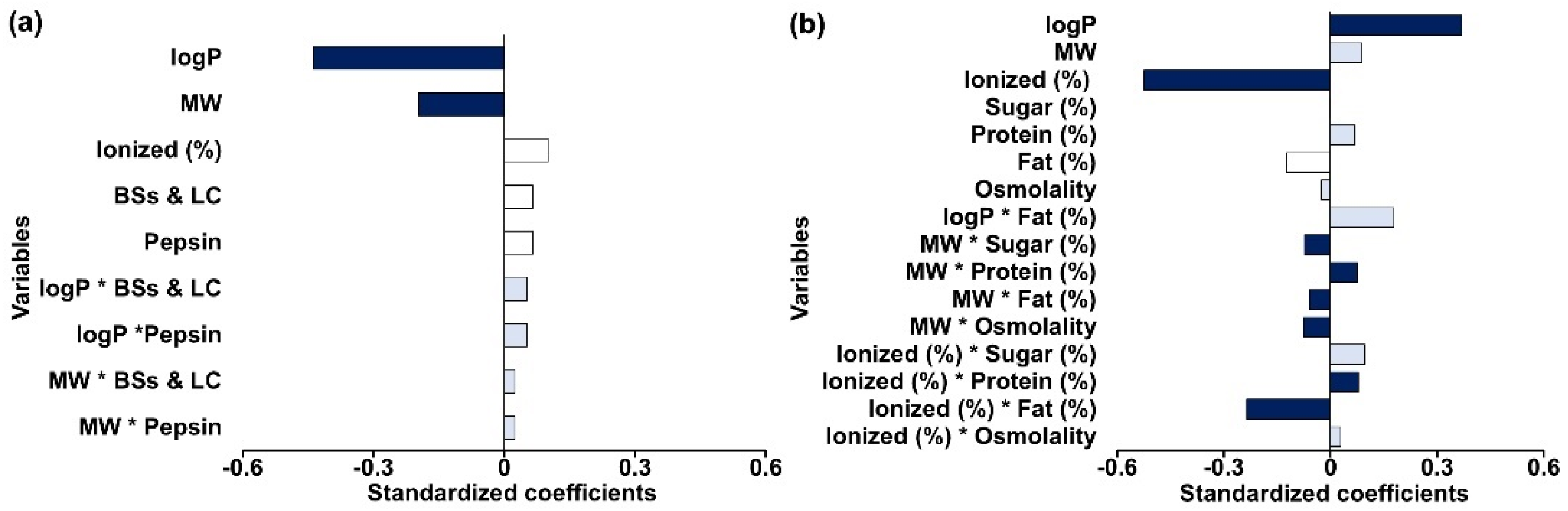
3.3. Multivariate Statistical Analysis
3.3.1. Fasted Gastric Simulated Fluids
3.3.2. Fed Gastric Simulated Fluids
3.3.3. Fasted Intestinal Simulated Fluids
3.3.4. Fed Intestinal Simulated Fluids
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| BCS | Biopharmaceutics Classification System |
| BSs and LC | Bile salts and lecithin |
| FaSSGF | Adult fasted state gastric media |
| FaSSIF-V2 | Adult fasted state intestinal media Version 2 |
| FeSSGF | Adult fed state gastric media |
| FeSSIF-V2 | Adult fed state intestinal media Version 2 |
| GI | Gastrointestinal |
| logP | log (octanol/water partition coefficient) |
| MW | Molecular weight |
| NaTC | Sodium taurocholate |
| P50%-FaSSIF | Pediatric fasted state intestinal media formulated with bile salt concentrations 50% (i.e., 1.5 mM) of adult levels |
| P150%-FaSSIF | Pediatric fasted state intestinal media formulated with bile salt concentrations 150% (i.e., 4.5 mM) of adult levels |
| pBCS | Pediatric Biopharmaceutics Classification System |
| PBPK | Physiologically based pharmacokinetics |
| Pi-FaSSGF | Pediatric fasted state gastric media representative of infants (1–12 months) |
| Pi-FeSSIF | Pediatric fed state intestinal media representative of infants (1–12 months) |
| Pn-FaSSGF | Pediatric fasted state gastric media representative of newborns (0–28 days) |
| Pnc-FeSSGF | Pediatric fed state gastric media representative of newborns (0–28 days) fed cow’s milk-based formula |
| Pns-FeSSGF | Pediatric fed state gastric media representative of newborns (0–28 days) fed soy-based formula |
| PLS-R | Partial Least Squares Regression |
| Q2 | Goodness of prediction |
| R2 | Coefficient of determination |
| SD | Standard Deviation |
| Sp/Sa (%) | Pediatrics-to-adult solubility ratio |
References
- Dressman, J.B.; Vertzoni, M.; Goumas, K.; Reppas, C. Estimating drug solubility in the gastrointestinal tract. Adv. Drug Deliv. Rev. 2007, 59, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, M.; Statelova, M.; Holm, R.; Reppas, C.; Symilllides, M.; Vertzoni, M.; Fotaki, N. Biopharmaceutical considerations in paediatrics with a view to the evaluation of orally administered drug products—A PEARRL review. J. Pharm. Pharmacol. 2019, 71, 603–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amidon, G.; Lennernas, H.; Shah, V.; Crison, J. A theoretical basis for a biopharmaceutic drug classification: The correlation of In Vitro drug product dissolution and In Vivo bioavailability. Pharm. Res. 1995, 12, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maharaj, A.R.; Edginton, A.N.; Fotaki, N. Assessment of Age-Related Changes in Pediatric Gastrointestinal Solubility. Pharm. Res. 2016, 33, 52–71. [Google Scholar] [CrossRef]
- Batchelor, H.K.; Fotaki, N.; Klein, S. Paediatric oral biopharmaceutics: Key considerations and current challenges. Adv. Drug Deliv. Rev. 2014, 73, 102–126. [Google Scholar] [CrossRef] [Green Version]
- Batchelor, H.K. Paediatric biopharmaceutics classification system: Current status and future decisions. Int. J. Pharm. 2014, 469, 251–253. [Google Scholar] [CrossRef]
- Gandhi, S.V.; Rodriguez, W.; Khan, M.; Polli, J.E. Considerations for a Pediatric Biopharmaceutics Classification System (BCS): Application to Five Drugs. AAPS PharmSciTech 2014, 15, 601–611. [Google Scholar] [CrossRef]
- Fadda, H.M.; Sousa, T.; Carlsson, A.S.; Abrahamsson, B.; Williams, J.G.; Kumar, D.; Basit, A.W. Drug Solubility in Luminal Fluids from Different Regions of the Small and Large Intestine of Humans. Mol. Pharm. 2010, 7, 1527–1532. [Google Scholar] [CrossRef]
- Benet, L.Z.; Broccatelli, F.; Oprea, T.I. BDDCS applied to over 900 drugs. AAPS J. 2011, 13, 519–547. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, S.; Yadav, L.; Aggarwal, D. Prediction of in vivo drug performance using in vitro dissolution coupled with STELLA: A study with selected drug products. Drug Dev. Ind. Pharm. 2015, 41, 1667–1673. [Google Scholar] [CrossRef]
- Okumu, A.; Dimaso, M.; Löbenberg, R. Dynamic Dissolution Testing to Establish In Vitro/In Vivo Correlations for Montelukast Sodium, a Poorly Soluble Drug. Pharm. Res. 2008, 25, 2778–2785. [Google Scholar] [CrossRef]
- Rana, N.S.; Rajesh, K.S.; Patel, N.N.; Patel, P.R.; Limbachiya, U.; Pasha, T.Y. Development and Validation of RP-HPLC Method for the Simultaneous Estimation of Montelukast Sodium and Ebastine in Tablet Dosage Form. Indian J. Pharm. Sci. 2013, 75, 599–602. [Google Scholar] [PubMed]
- Macheras, P.E.; Koupparis, M.A.; Antimisiaris, S.G. Drug binding and solubility in milk. Pharm. Res. 1990, 7, 537–541. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Proposal to Waive In Vivo Bioequivalence Requirements for WHO Model List of Essential Medicines Immediate-Release, Solid Oral Dosage Forms (Annex 8). WHO Technical Report Series, No. 937, 2006: World Health Organization (WHO). 2006. Available online: http://www.who.int/medicines/areas/quality_safety/quality_assurance/ProposalWaiveVivoBioequivalenceRequirementsModelListEssentialMedicinesImmediateReleaseSolidOralDosageFormsTRS937Annex8.pdf (accessed on 12 December 2020).
- Mandal, T.; Ace, L. High–performance liquid chromatographic determination of nitrofurantoin in plasma. J. Clin. Pharm. Ther. 1993, 18, 347–350. [Google Scholar] [CrossRef]
- Bouchard, G.; Carrupt, P.A.; Testa, B.; Gobry, V.; Girault, H.H. Lipophilicity and solvation of anionic drugs. Chemistry 2002, 8, 3478–3484. [Google Scholar] [CrossRef]
- Bergström, C.A.S.; Andersson, S.B.E.; Fagerberg, J.H.; Ragnarsson, G.; Lindahl, A. Is the full potential of the biopharmaceutics classification system reached? Eur. J. Pharm. Sci. 2014, 57, 224–231. [Google Scholar] [CrossRef]
- Yilmaz, B.; Asci, A.; Erdem, F. HPLC Method for Naproxen Determination in Human Plasma and Its Application to a Pharmacokinetic Study in Turkey. J. Chromatogr. Sci. 2014, 52, 584–589. [Google Scholar] [CrossRef] [Green Version]
- Kalantzi, L.; Persson, E.; Polentarutti, B.; Abrahamsson, B.; Goumas, K.; Dressman, J.B.; Reppas, C. Canine Intestinal Contents vs. Simulated Media for the Assessment of Solubility of Two Weak Bases in the Human Small Intestinal Contents. Pharm. Res. 2006, 23, 1373–1381. [Google Scholar] [CrossRef]
- Carlert, S.; Akesson, P.; Jerndal, G.; Lindfors, L.; Lennernas, H.; Abrahamsson, B. In Vivo dog intestinal precipitation of mebendazole: A basic BCS class II drug. Mol. Pharm. 2012, 9, 2903–2911. [Google Scholar] [CrossRef]
- Söderlind, E.; Karlsson, E.; Carlsson, A.; Kong, R.; Lenz, A.; Lindborg, A.; Sheng, J.J. Simulating fasted human intestinal fluids: Understanding the roles of lecithin and bile acids. Mol. Pharm. 2010, 7, 1498–1507. [Google Scholar] [CrossRef]
- Daniel-Mwambete, K.; Torrado, S.; Cuesta-Bandera, C.; Ponce-Gordo, F.; Torrado, J. The effect of solubilization on the oral bioavailability of three benzimidazole carbamate drugs. Int. J. Pharm. 2004, 272, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, G.; Gosling, D.J.; Patissier, C.; Rodde, S.; Zhou, L.; Faller, B. What is modulating solubility in simulated intestinal fluids? Eur. J. Pharm. Sci. 2010, 41, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Baxevanis, F.; Kuiper, J.; Fotaki, N. Strategic drug analysis in fed-state gastric biorelevant media based on drug physicochemical properties. Eur. J. Pharm. Biopharm. 2018, 127, 326–341. [Google Scholar] [CrossRef]
- Eriksson, L.; Johansson, E.; Kettaneh-Wold, N.; Wikström, C.; Wold, S. Design of Experiments: Principles and Applications, 3rd ed.; Umetrics AB: Ume, Sweden, 2008. [Google Scholar]
- Lu, H.; Rosenbaum, S. Developmental Pharmacokinetics in Pediatric Populations. J. Pediatr. Pharmacol. Ther. 2014, 19, 262–276. [Google Scholar] [CrossRef]
- SAS Institute Inc. SAS/STAT 9.3 User’s Guide, Book Chapter: The PLS Procedure; SAS Institute Inc.: Cary, NC, USA, 2011; pp. 5640–5650, 5670–5675. [Google Scholar]
- Wold, S.; Sjöström, M.; Eriksson, L. PLS-regression: A basic tool of chemometrics. Chemom. Intell. Lab. Syst. 2001, 58, 109–130. [Google Scholar] [CrossRef]
- Eriksson, L.; Byrne, T.; Johansson, E.; Trygg, J.; Vikström, C. Multi- and Megavariate Data Analysis: Basic Principles and Applications, 3rd ed.; Umetrics AB: Ume, Sweden, 2013. [Google Scholar]
- Zarmpi, P.; Flanagan, T.; Meehan, E.; Mann, J.; Fotaki, N. Biopharmaceutical Understanding of Excipient Variability on Drug Apparent Solubility Based on Drug Physicochemical Properties. Case Study: Superdisintegrants. AAPS J. 2020, 22, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diakidou, A.; Vertzoni, M.; Dressman, J.B.; Reppas, C. Estimation of intragastric drug solubility in the fed state: Comparison of various media with data in aspirates. Biopharm. Drug Dispos. 2009, 30, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Khadra, I.; Zhou, Z.; Dunn, C.; Wilson, C.G.; Halbert, G. Statistical investigation of simulated intestinal fluid composition on the equilibrium solubility of biopharmaceutics classification system class II drugs. Eur. J. Pharm. Sci. 2015, 67, 65–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrier, J.; Zhou, Z.; Dunn, C.; Khadra, I.; Wilson, C.G.; Halbert, G. Statistical investigation of the full concentration range of fasted and fed simulated intestinal fluid on the equilibrium solubility of oral drugs. Eur. J. Pharm. Sci. 2018, 111, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Dunn, C.; Khadra, I.; Wilson, C.G.; Halbert, G.W. Statistical investigation of simulated fed intestinal media composition on the equilibrium solubility of oral drugs. Eur. J. Pharm. Sci. 2017, 99, 95–104. [Google Scholar] [CrossRef]
- Wallace, S.J.; Li, J.; Nation, R.L.; Boyd, B.J. Drug release from nanomedicines: Selection of appropriate encapsulation and release methodology. Drug Deliv. Transl. Res. 2012, 2, 284–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, B.J. Characterisation of drug release from cubosomes using the pressure ultrafiltration method. Int. J. Pharm. 2003, 260, 239–247. [Google Scholar] [CrossRef]
- Williams, H.D.; Trevaskis, N.L.; Charman, S.A.; Shanker, R.M.; Charman, W.N.; Pouton, C.W.; Porter, C.J. Strategies to address low drug solubility in discovery and development. Pharmacol. Rev. 2013, 65, 315–499. [Google Scholar] [CrossRef] [PubMed]
- Elder, D.P.; Holm, R.; de Diego, H.L. Use of pharmaceutical salts and cocrystals to address the issue of poor solubility. Int. J. Pharm. 2013, 453, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Mithani, S.D.; Bakatselou, V.; TenHoor, C.N.; Dressman, J.B. Estimation of the increase in solubility of drugs as a function of bile salt concentration. Pharm. Res. 1996, 13, 163–167. [Google Scholar] [CrossRef]
- Hörter, D.; Dressman, J.B. Influence of physicochemical properties on dissolution of drugs in the gastrointestinal tract. Adv. Drug Deliv. Rev. 1997, 25, 3–14. [Google Scholar] [CrossRef]
- Fagerberg, J.H.; Tsinman, O.; Sun, N.; Tsinman, K.; Avdeef, A.; Bergström, C.A.S. Dissolution Rate and Apparent Solubility of Poorly Soluble Drugs in Biorelevant Dissolution Media. Mol. Pharm. 2010, 7, 1419–1430. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | logP | pKa | MW (g/mol) | BCS Class | Column | Mobile Phase | Flow Rate (mL/min) | T (°C) | Injection Volume (µL) | λ (nm) | Run Time (Min) | HPLC Method Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mesalazine | 0.98 [8] | 2.3 (acidic) and 5.69 (basic) [8] | 153 [9] | IV [10] | c | MeOH: H2O with 0.01% TFA (5:95) | 1 | 40 | 20 | 304 | 10 | [8] |
| Montelukast | 8.79 [11] | 2.7 (basic) and 5.8 (acidic) [11] | 586 [9] | II [11] | b | MeOH: Ammonium acetate buffer pH 5.5 gradient e | 1 | 20 | 100 | 284 | 15 | [12] |
| Nitrofurantoin | −0.47 [9] | 7.2 (acidic) [13] | 238 [9] | II [14] | b | MeOH: Phosphate buffer 0.05 M pH 3 (40:60) | 1 | 25 | 50 | 360 | 6.5 | [15] |
| Naproxen | 3.18 [9] | 4.18 (acidic) [16] | 230 [9] | II [17] | IACN: H2O with 0.1 % Formic acid (40:60) | 1 | 40 | 100 | 239 | 6 | [18] | |
| Dipyridamole | 2.74 [19] | 5.7–6.4 (basic) [19,20] | 505 [9] | II [20] | b | ACN: H2O with 0.1 % TFA (30:70) | 1 | 25 | 50 | 284 | 8 | [21] |
| Mebendazole | 2.80 | 3.5 (basic) | 295 [9] | II [9] | a | MeOH: Ammonium phosphate 0.05 M pH 5.5(70:30) | 1 | 25 | 100 | 313 | 6 | [22] |
| Amiodarone | 7.57 [23] | 8.73 (basic) [23] | 645 [9] | II [17] | d | MeOH: Phosphate buffer 0.05 M pH3 (70:30) | 1 | 25 | 20 | 241 | 5 | [22] |
| Adult Biorelevant Media | Solubility (µg/mL) | ||||||
|---|---|---|---|---|---|---|---|
| Mesalazine | Montelukast | Nitrofurantoin | Naproxen | Dipyridamole | Mebendazole | Amiodarone | |
| FaSSGF | 3202.04 ± 119.20 | 0.85 ± 0.18 | 196.08 ± 11.73 | 30.65 ± 1.32 | 11524.19 ± 570.44 | 39.51 ± 4.45 | 18.82 ± 1.90 |
| FeSSGF | 1717.76 ± 392.37 | - | 389.56 ± 6.35 | 710.24 ± 26.65 | 158.27 ± 7.22 | 4.37 ± 0.90 | - |
| FaSSIF-V2 | 2664.58 ± 145.74 | 8.28 ± 1.02 | 215.67 ± 1.96 | 1910.34 ± 94.91 | 11.86 ± 0.17 | 1.39 ± 0.16 | 24.88 ± 4.84 |
| FeSSIF-V2 | 2882.02 ± 68.37 | 38.57 ± 9.15 | 209.40 ± 3.22 | 944.61 ± 42.83 | 81.38 ± 1.74 | 3.51 ± 0.17 | 652.19 ± 74.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guimarães, M.; Maharaj, A.; Edginton, A.; Vertzoni, M.; Fotaki, N. Understanding the Impact of Age-Related Changes in Pediatric GI Solubility by Multivariate Data Analysis. Pharmaceutics 2022, 14, 356. https://doi.org/10.3390/pharmaceutics14020356
Guimarães M, Maharaj A, Edginton A, Vertzoni M, Fotaki N. Understanding the Impact of Age-Related Changes in Pediatric GI Solubility by Multivariate Data Analysis. Pharmaceutics. 2022; 14(2):356. https://doi.org/10.3390/pharmaceutics14020356
Chicago/Turabian StyleGuimarães, Mariana, Anil Maharaj, Andrea Edginton, Maria Vertzoni, and Nikoletta Fotaki. 2022. "Understanding the Impact of Age-Related Changes in Pediatric GI Solubility by Multivariate Data Analysis" Pharmaceutics 14, no. 2: 356. https://doi.org/10.3390/pharmaceutics14020356
APA StyleGuimarães, M., Maharaj, A., Edginton, A., Vertzoni, M., & Fotaki, N. (2022). Understanding the Impact of Age-Related Changes in Pediatric GI Solubility by Multivariate Data Analysis. Pharmaceutics, 14(2), 356. https://doi.org/10.3390/pharmaceutics14020356