
Application of a Physiologically Based Pharmacokinetic Model to Predict Cefazolin and Cefuroxime Disposition in Obese Pregnant Women Undergoing Caesarean Section

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Model Building
- (a)
- Non–obese (lean), non–pregnant (BMI 18.50–24.99 kg/m2),
- (b)
- Obese non–pregnant (BMI ≥ 30 kg/m2),
- (c)
- Pregnant non–obese (lean pregnant) (BMI 18.50–24.99 kg/m2) and
- (d)
- Obese pregnant (BMI ≥ 30 kg/m2) populations.
2.1.1. Physiologically Based Pharmacokinetic Simulation Design
2.1.2. Evaluation and Refinement of Cefazolin PBPK Model in Lean Non–Pregnant, Obese Non–Pregnant, Lean Pregnant, and Obese Pregnant Subjects
2.1.3. Evaluation and Refinement of Cefuroxime PBPK Model in Lean Non–Pregnant, Obese Non–Pregnant, and Lean Pregnant Subjects
2.2. Acceptance Criteria
2.3. Application of Obese Pregnant Model to Predict Cefuroxime Disposition
3. Results
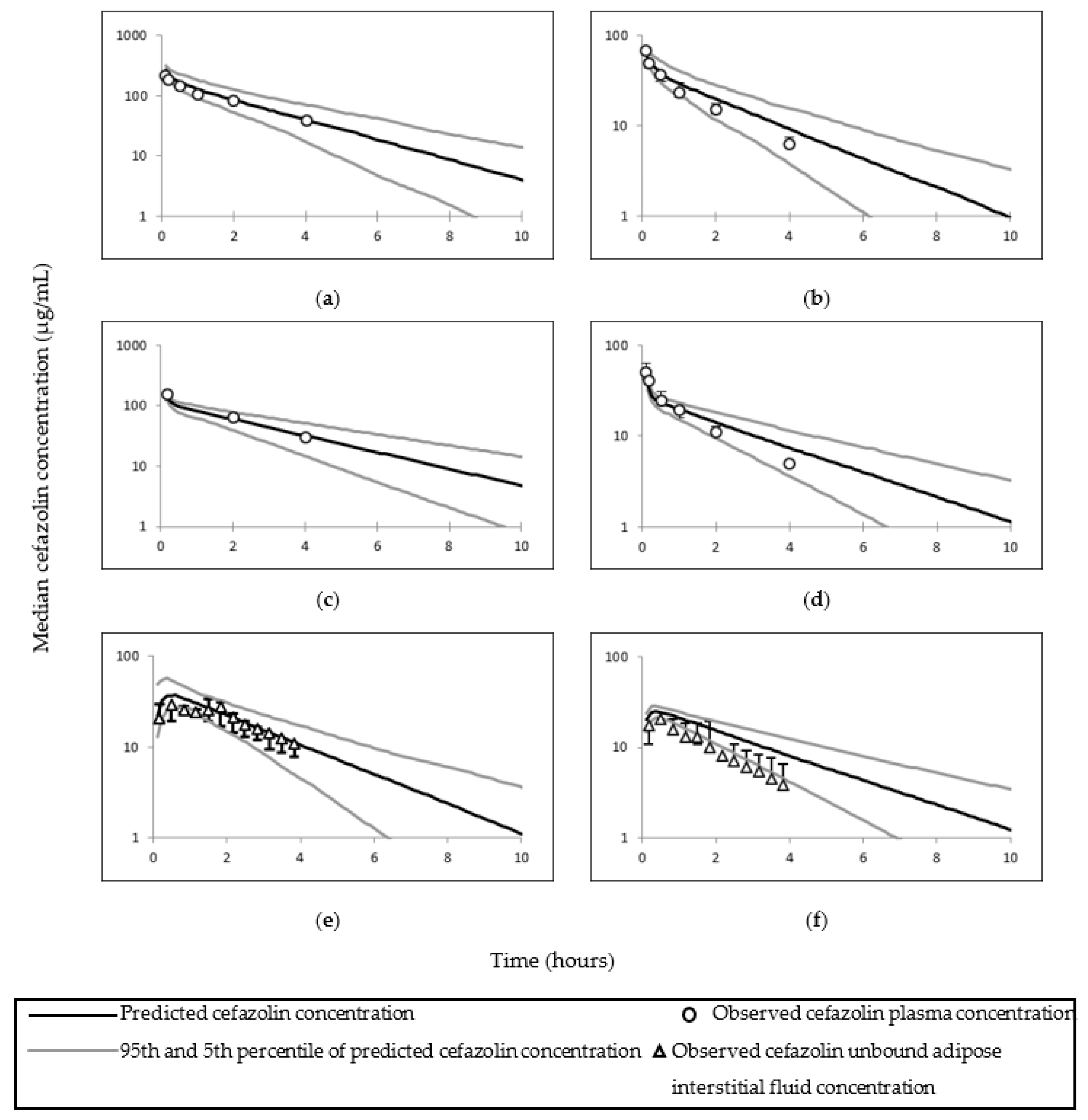
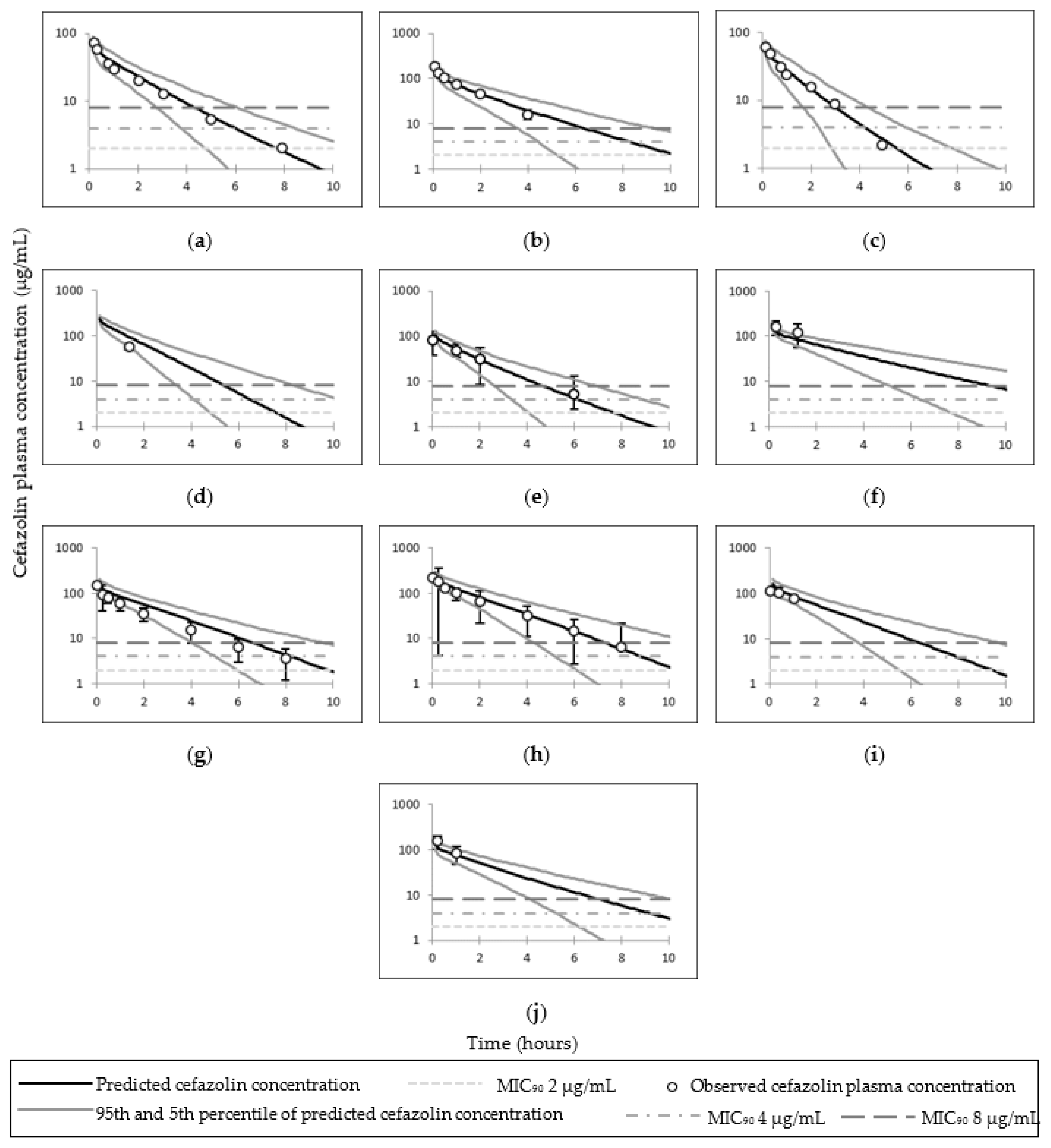
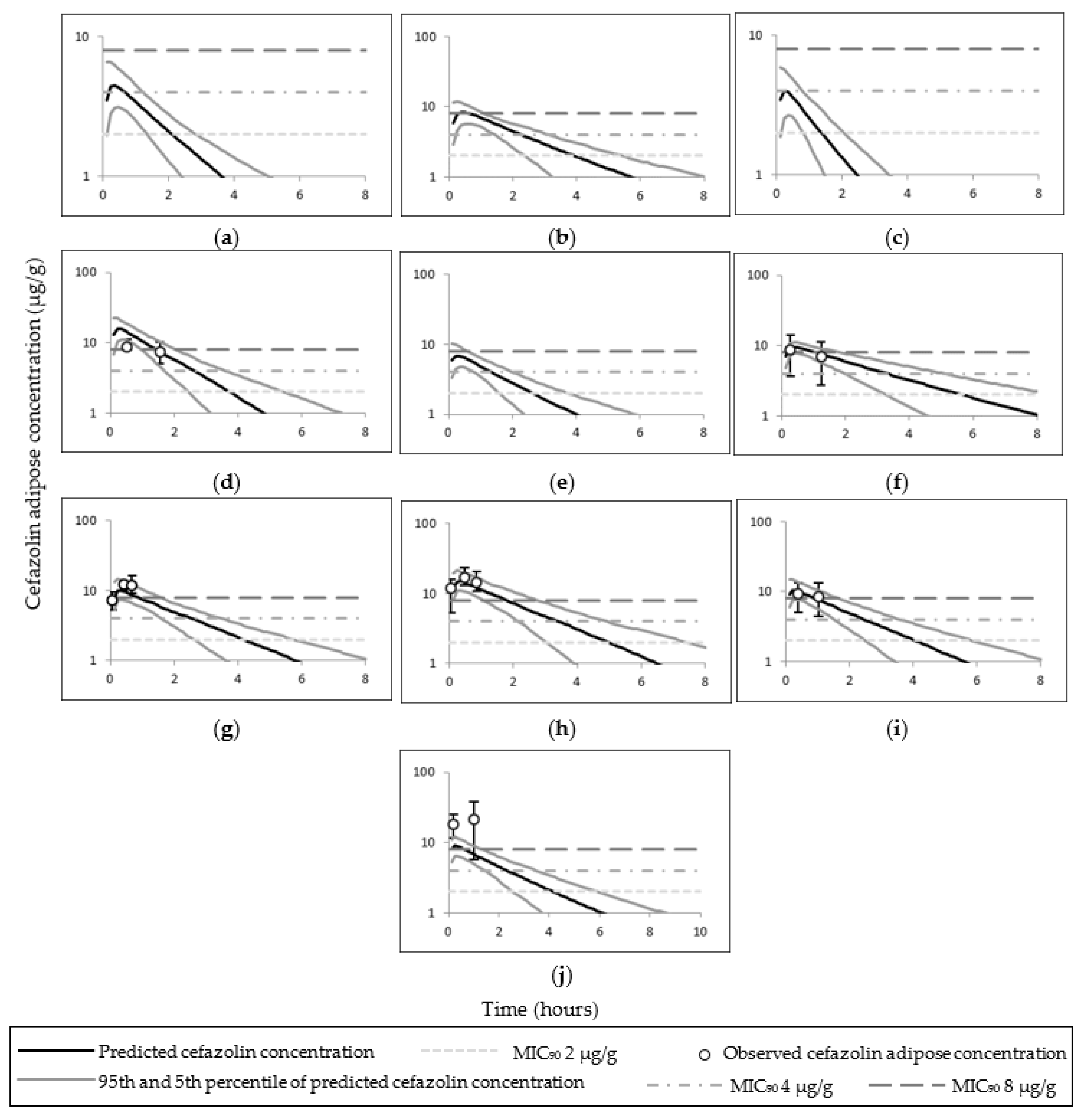
3.1. Cefazolin PBPK Model
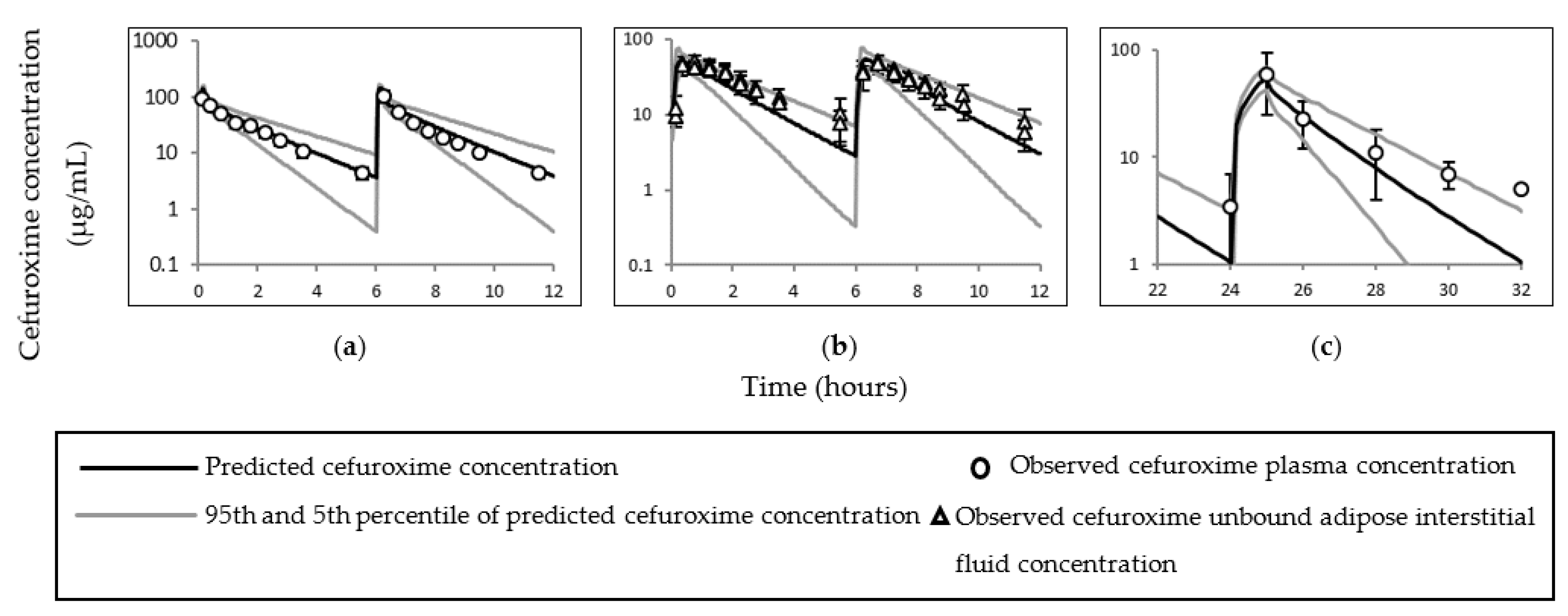
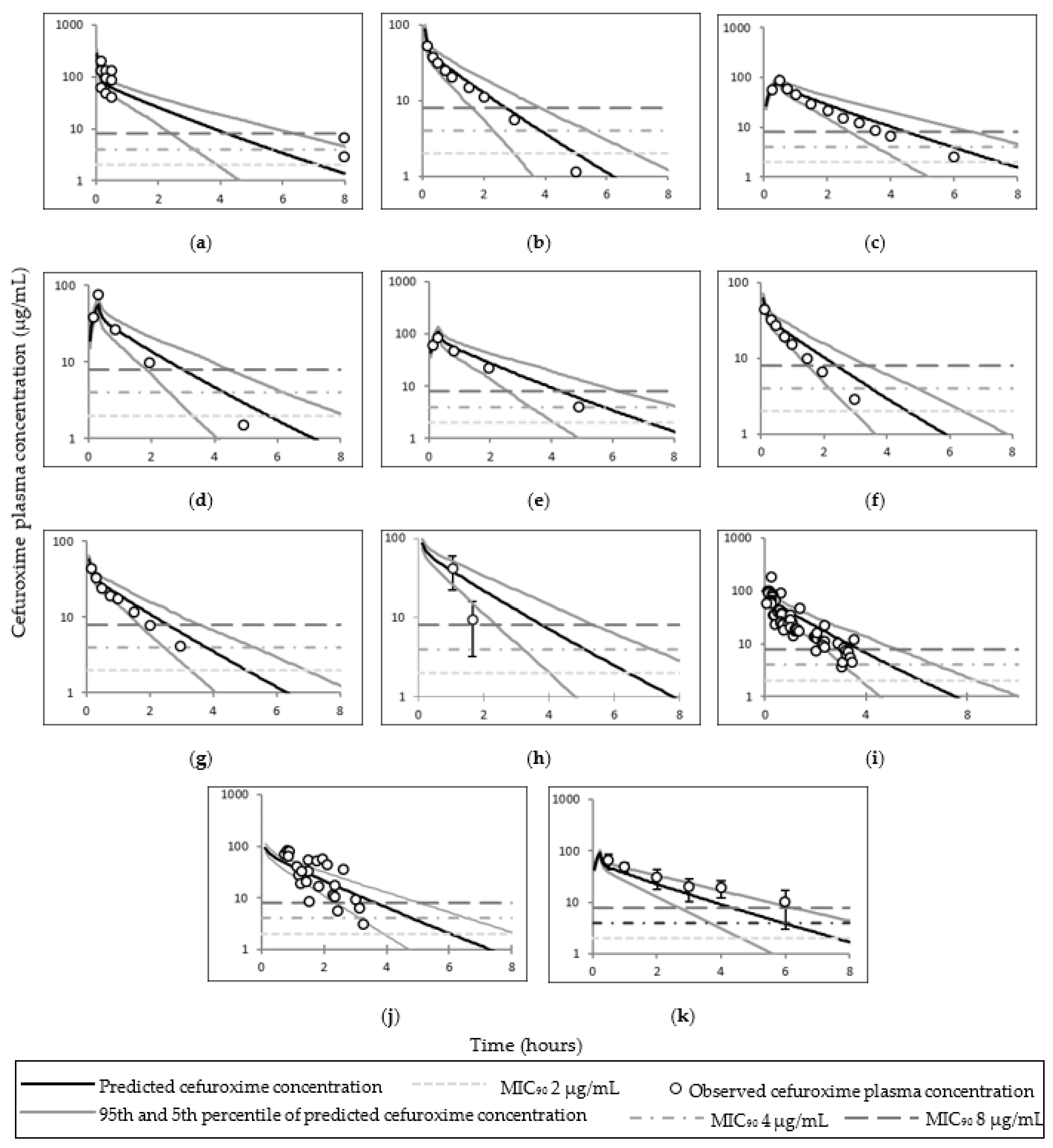
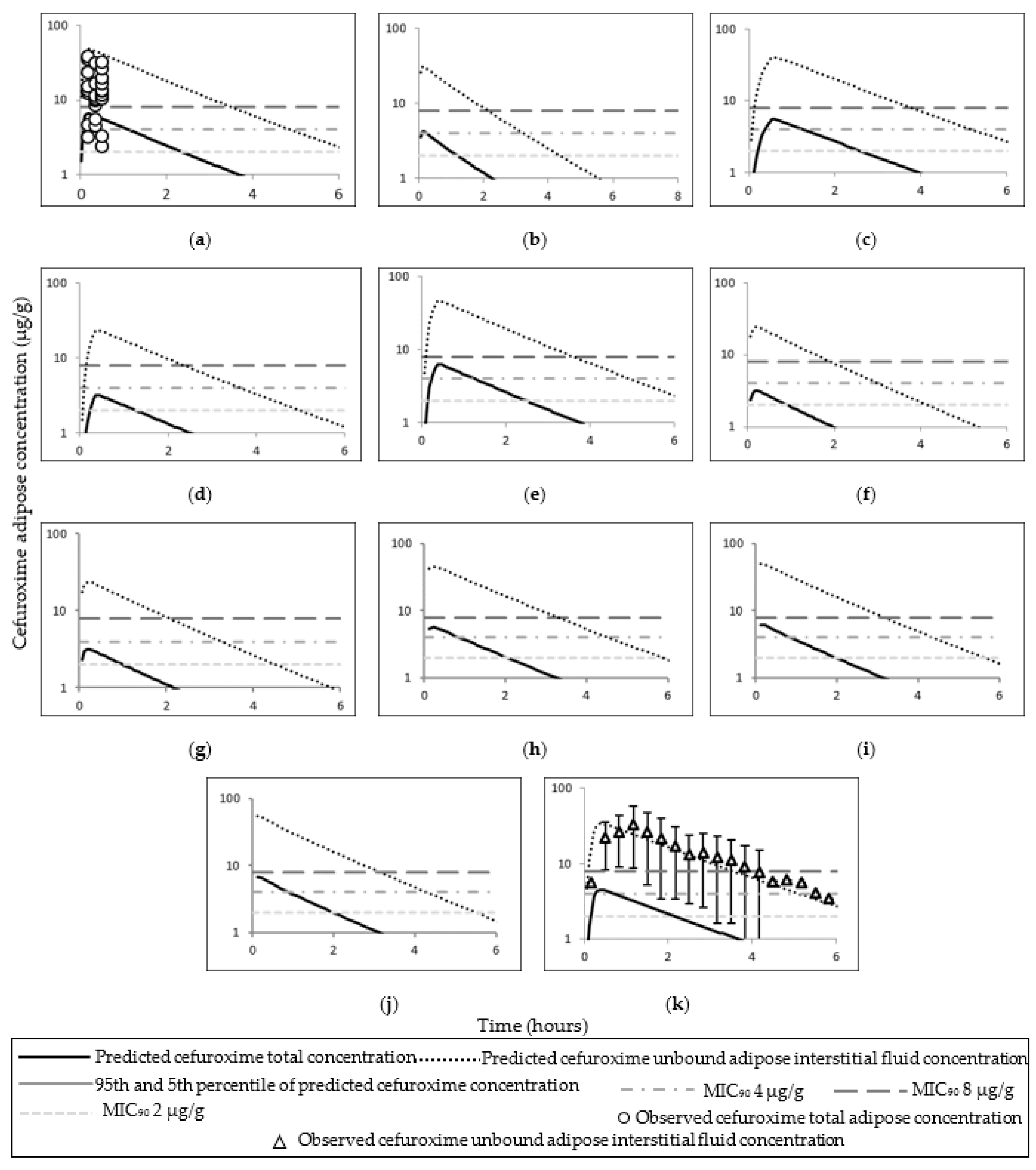
3.2. Cefuroxime PBPK Model
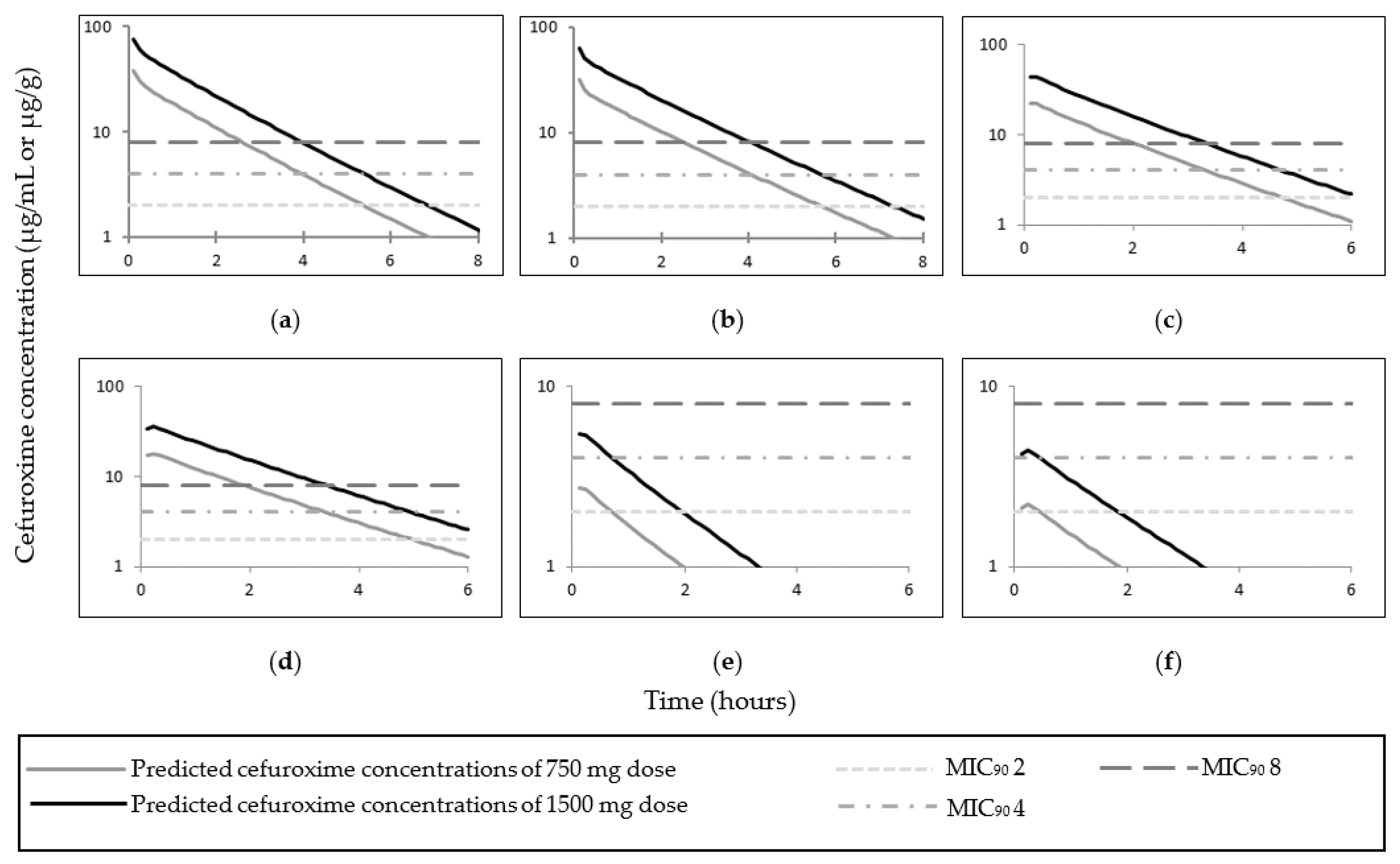
3.3. Cefuroxime PBPK Model Application in the Obese Pregnant Population
4. Discussion
4.1. Cefazolin
4.2. Cefuroxime
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lalic-Popovic, M.; Paunkovic, J.; Grujic, Z.; Golocorbin-Kon, S.; Milasinovic, L.; Al-Salami, H.; Mikov, M. Decreased placental and transcellular permeation of cefuroxime in pregnant women with diabetes. J. Diabetes 2016, 8, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Swank, M.L.; Wing, D.A.; Nicolau, D.P.; McNulty, J.A. Increased 3-gram cefazolin dosing for cesarean delivery prophylaxis in obese women. Am. J. Obstet. Gynecol. 2015, 213, 415.e1–415.e8. [Google Scholar] [CrossRef] [PubMed]
- Foord, R. Cefuroxime: Human pharmacokinetics. Antimicrob. Agents Chemother. 1976, 9, 741–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vella-Brincat, J.W.; Begg, E.J.; Kirkpatrick, C.M.; Zhang, M.; Chambers, S.T.; Gallagher, K. Protein binding of cefazolin is saturable in vivo both between and within patients. Br. J. Clin. Pharmacol. 2007, 63, 753–757. [Google Scholar] [CrossRef] [Green Version]
- Decroix, M.O.; Zini, R.; Chaumeil, J.C.; Tillement, J.P. Cefazolin serum protein binding and its inhibition by bilirubin, fatty acids and other drugs. Biochem. Pharmacol. 1988, 37, 2807–2814. [Google Scholar] [CrossRef]
- ChemSpider. Cefuroxime|C16H16N4O8S|ChemSpider. 2020. Available online: http://www.chemspider.com/Chemical-Structure.4514699.html (accessed on 26 August 2020).
- Zeilmaker-Roest, G.A.; van Saet, A.; van Rosmalen, J.; Bahmany, S.; van Dijk, A.; Wildschut, E.D.; Tibboel, D.; Bogers, A.J.J.C. Potentially clinically relevant concentrations of Cefazolin, Midazolam, Propofol, and Sufentanil in auto-transfused blood in congenital cardiac surgery. J. Cardiothorac. Surg. 2018, 13, 64. [Google Scholar] [CrossRef]
- Philipson, A.; Stiernstedt, G.; Ehrnebo, M. Comparison of the pharmacokinetics of cephradine and cefazolin in pregnant and non-pregnant women. Clin. Pharmacokinet. 1987, 12, 136–144. [Google Scholar] [CrossRef]
- Philipson, A.; Stiernstedt, G. Pharmacokinetics of cefuroxime in pregnancy. Am. J. Obstet. Gynecol. 1982, 142, 823–828. [Google Scholar] [CrossRef]
- Ueo, H.; Motohashi, H.; Katsura, T.; Inui, K.-i. Human organic anion transporter hOAT3 is a potent transporter of cephalosporin antibiotics, in comparison with hOAT1. Biochem. Pharmacol. 2005, 70, 1104–1113. [Google Scholar] [CrossRef]
- Uwai, Y.; Saito, H.; Inui, K.-i. Rat renal organic anion transporter rOAT1 mediates transport of urinary-excreted cephalosporins, but not of biliary-excreted cefoperazone. Drug Metab. Pharmacokinet. 2002, 17, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Ci, L.; Kusuhara, H.; Adachi, M.; Schuetz, J.D.; Takeuchi, K.; Sugiyama, Y. Involvement of MRP4 (ABCC4) in the luminal efflux of ceftizoxime and cefazolin in the kidney. Mol. Pharmacol. 2007, 71, 1591–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, V.; de L. T. Vieira, M.; Zhao, P.; Zhang, L.; Zheng, J.H.; Nordmark, A.; Berglund, E.G.; Giacomini, K.M.; Huang, S.M. Towards quantitation of the effects of renal impairment and probenecid inhibition on kidney uptake and efflux transporters, using physiologically based pharmacokinetic modelling and simulations. Clin. Pharmacokinet. 2014, 53, 283–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodwall, E.K.; Bergan, T.; Orjavik, O. Kidney transport of cefazolin in normal and impaired renal function. J. Antimicrob. Chemother. 1977, 3, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Koren, G.; Pariente, G. Pregnancy-associated changes in pharmacokinetics and their clinical implications. Pharm. Res. 2018, 35, 61. [Google Scholar] [CrossRef] [PubMed]
- Abduljalil, K.; Pansari, A.; Jamei, M. Prediction of maternal pharmacokinetics using physiologically based pharmacokinetic models: Assessing the impact of the longitudinal changes in the activity of CYP1A2, CYP2D6 and CYP3A4 enzymes during pregnancy. J. Pharmacokinet. Pharmacodyn. 2020, 47, 361–383. [Google Scholar] [CrossRef]
- Smit, C.; De Hoogd, S.; Brüggemann, R.J.M.; Knibbe, C.A.J. Obesity and drug pharmacology: A review of the influence of obesity on pharmacokinetic and pharmacodynamic parameters. Expert Opin. Drug Metab. Toxicol. 2018, 14, 275–285. [Google Scholar] [CrossRef]
- Chan, K.; Krepel, C.; Edmiston, C., Jr.; Pevzner, L.; Swank, M.; Wing, D.A. Effects of maternal obesity on tissue concentrations of prophylactic cefazolin during cesarean delivery. Am. J. Obstet. Gynecol. 2011, 204 (Suppl. 1), S24. [Google Scholar] [CrossRef]
- Groff, S.M.; Fallatah, W.; Yang, S.; Murphy, J.; Crutchfield, C.; Marzinke, M.; Kurtzberg, J.; Lee, C.K.K.; Burd, I.; Azadeh, F. Effect of maternal obesity on maternal-fetal transfer of preoperative cefazolin at cesarean section. J. Pediatr. Pharmacol. Ther. 2017, 22, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Kram, J.J.F.; Greer, D.M.; Cabrera, O.; Burlage, R.; Forgie, M.M.; Siddiqui, D.S. Does current cefazolin dosing achieve adequate tissue and blood concentrations in obese women undergoing cesarean section? Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 210, 334–341. [Google Scholar] [CrossRef]
- Maggio, L.; Nicolau, D.P.; DaCosta, M.; Rouse, D.J.; Hughes, B.L. Cefazolin prophylaxis in obese women undergoing cesarean delivery: A randomized controlled trial. Obstet. Gynecol. 2015, 125, 1205–1210. [Google Scholar] [CrossRef]
- Stitely, M.; Sweet, M.; Slain, D.; Alons, L.; Holls, W.; Hochberg, C.; Briggs, F. Plasma and tissue cefazolin concentrations in obese patients undergoing cesarean delivery and receiving differing pre-operative doses of drug. Surg. Infect. 2013, 14, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Young, O.M.; Shaik, I.H.; Twedt, R.; Binstock, A.; Althouse, A.D.; Venkataramanan, R.; Simhan, H.N.; Wiesenfeld, H.C.; Caritis, S.N. Pharmacokinetics of cefazolin prophylaxis in obese gravidae at time of cesarean delivery. Am. J. Obstet. Gynecol. 2015, 213, 541.e1–547.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alrammaal, H.H.; Batchelor, H.K.; Morris, K.; Chong, H.P. Efficacy of perioperative cefuroxime as a prophylactic antibiotic in women requiring caesarean section: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 242, 71–78. [Google Scholar] [CrossRef] [PubMed]
- UK NICE Guideline [NG125]. Surgical Site Infections: Prevention and Treatment. 2019. Available online: https://www.nice.org.uk/guidance/ng125 (accessed on 20 July 2019).
- Holt, D.E.; Broadbent, M.; Spencer, J.A.D.; Delouvois, J.; Hurley, R.; Harvey, D. The placental-transfer of cefuroxime at parturition. Eur. J. Obstet. Gynecol. 1994, 54, 177–180. [Google Scholar] [CrossRef]
- Skhirtladze-Dworschak, K.; Hutschala, D.; Reining, G.; Dittrich, P.; Bartunek, A.; Dworschak, M.; Tschernko, E.M. Cefuroxime plasma and tissue concentrations in patients undergoing elective cardiac surgery: Continuous vs bolus application. A pilot study. Br. J. Clin. Pharmacol. 2019, 85, 818–826. [Google Scholar] [CrossRef] [Green Version]
- Abduljalil, K.; Badhan, R.K.S. Drug dosing during pregnancy—Opportunities for physiologically based pharmacokinetic models. J. Pharmacokinet. Pharmacodyn. 2020, 47, 319–340. [Google Scholar] [CrossRef]
- Jamsen, K.M.; McLeay, S.C.; Barras, M.A.; Green, B. Reporting a population pharmacokinetic–pharmacodynamic study: A journal’s perspective. Clin. Pharmacokinet. 2014, 53, 111–122. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, T.; Rowland, M. Physiologically based pharmacokinetic modelling 2: Predicting the tissue distribution of acids, very weak bases, neutrals and zwitterions. J. Pharm. Sci. 2006, 95, 1238–1257. [Google Scholar] [CrossRef]
- Jamei, M.; Bajot, F.; Neuhoff, S.; Barter, Z.; Yang, J.; Rostami-Hodjegan, A.; Rowland-Yeo, K. A mechanistic framework for in vitro-in vivo extrapolation of liver membrane transporters: Prediction of drug-drug interaction between rosuvastatin and cyclosporine. Clin. Pharmacokinet. 2014, 53, 73–87. [Google Scholar] [CrossRef] [Green Version]
- Spruill, W.J.; Wade, W.E.; Cobb, H.H., 3rd. Estimating glomerular filtration rate with a modification of diet in renal disease equation: Implications for pharmacy. Am. J. Health Syst. Pharm. 2007, 64, 652–660. [Google Scholar] [CrossRef]
- Ghobadi, C.; Johnson, T.N.; Aarabi, M.; Almond, L.M.; Allabi, A.C.; Rowland-Yeo, K.; Jamei, M.; Rostami-Hodjegan, A. Application of a systems approach to the bottom-up assessment of pharmacokinetics in obese patients. Clin. Pharmacokinet. 2011, 50, 809–822. [Google Scholar] [CrossRef] [PubMed]
- Burt, H.J.; Neuhoff, S.; Almond, L.; Gaohua, L.; Harwood, M.D.; Jamei, M.; Rostami-Hodjegan, A.; Tucker, G.T.; Rowland-Yeo, K. Metformin and cimetidine: Physiologically based pharmacokinetic modelling to investigate transporter mediated drug–drug interactions. Eur. J. Pharm. Sci. 2016, 88, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Neuhoff, S.; Gaohua, L.; Burt, H.; Jamei, M.; Li, L.; Tucker, G.T.; Rostami-Hodjegan, A. Accounting for transporters in renal clearance: Towards a mechanistic kidney model (Mech KiM). In Transporters in Drug Development: Discovery, Optimization, Clinical Study and Regulation; Sugiyama, Y., Steffansen, B., Eds.; Springer: New York, NY, USA, 2013; pp. 155–177. [Google Scholar]
- Abduljalil, K.; Furness, P.; Johnson, T.N.; Rostami-Hodjegan, A.; Soltani, H. Anatomical, physiological and metabolic changes with gestational age during normal pregnancy: A database for parameters required in physiologically based pharmacokinetic modelling. Clin. Pharmacokinet. 2012, 51, 365–396. [Google Scholar] [CrossRef] [PubMed]
- Gaohua, L.; Abduljalil, K.; Jamei, M.; Johnson, T.N.; Rostami-Hodjegan, A. A pregnancy physiologically based pharmacokinetic (p-PBPK) model for disposition of drugs metabolized by CYP1A2, CYP2D6 and CYP3A4. Br. J. Clin. Pharmacol. 2012, 74, 873–885. [Google Scholar] [CrossRef] [Green Version]
- De Sarro, A.; Ammendola, D.; Zappala, M.; Grasso, S.; De Sarro, G. Relationship between structure and convulsant properties of some beta-lactam antibiotics following intracerebroventricular microinjection in rats. Antimicrob. Agents Chemother. 1995, 39, 232. [Google Scholar] [CrossRef] [Green Version]
- Pubchem; National Center for Biotechnology Information. PubChem Compound Catabase; CID=33255, Cefazolin. 2021. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/33255 (accessed on 22 October 2018).
- Mathialagan, S.; Piotrowski, M.A.; Tess, D.A.; Feng, B.; Litchfield, J.; Varma, M.V. Quantitative prediction of human renal clearance and drug-drug interactions of organic anion transporter substrates using in vitro transport data: A relative activity factor approach. Drug Metab. Dispos. 2017, 45, 409–417. [Google Scholar] [CrossRef] [Green Version]
- Nishida, M.; Matsubara, T.; Murakawa, T.; Mine, Y.; Yokota, Y.; Goto, S.; Kuwahara, S. Cefazolin, a new semisynthetic cephalosporin antibiotic. III Absorption, excretion and tissue distribution in parenteral administration. J. Antibiot. 1970, 23, 184–194. [Google Scholar] [CrossRef]
- Tsuji, A.; Nishide, K.; Minami, H.; Nakashima, E.; Terasaki, T.; Yamana, T. Physiologically based pharmacokinetic model for cefazolin in rabbits and its preliminary extrapolation to man. Drug Metab. Dispos. 1985, 13, 729–739. [Google Scholar]
- Rodgers, T.; Leahy, D.; Rowland, M. Physiologically based pharmacokinetic modeling 1: Predicting the tissue distribution of moderate-to-strong bases. J. Pharm. Sci. 2005, 94, 1259–1276. [Google Scholar] [CrossRef]
- Rattie, E.S.; Ravin, L.J. Pharmacokinetic interpretation of blood levels and urinary excretion data for cefazolin and cephalothin after intravenous and intramuscular administration in humans. Antimicrob. Agents Chemother. 1975, 7, 606–613. [Google Scholar] [CrossRef] [Green Version]
- Pevzner, L.; Swank, M.; Krepel, C.; Wing, D.A.; Chan, K.; Edmiston, C.E.J. Effects of maternal obesity on tissue concentrations of prophylactic cefazolin during cesarean delivery. Obstet. Gynecol. 2011, 117, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Elkomy, M.H.; Sultan, P.; Drover, D.R.; Epshtein, E.; Galinkin, J.L.; Carvalho, B. Pharmacokinetics of prophylactic cefazolin in parturients undergoing cesarean delivery. Antimicrob. Agents Chemother. 2014, 58, 3504–3513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Brathwaite, C.E.; Barkan, A.; Hall, K.; Chu, G.; Cherasard, P.; Wang, S.; Nicolau, D.P.; Islam, S.; Cunha, B.A. Optimal cefazolin prophylactic dosing for bariatric surgery: No need for higher doses or intraoperative redosing. Obes. Surg. 2017, 27, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Lovering, A.M.; Perez, J.; Bowker, K.E.; Reeves, D.S.; MacGowan, A.P.; Bannister, G. A comparison of the penetration of cefuroxime and cephamandole into bone, fat and haematoma fluid in patients undergoing total hip replacement. J. Antimicrob. Chemother. 1997, 40, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Kagedal, M.; Nilsson, D.; Huledal, G.; Reinholdsson, I.; Cheng, Y.-F.; Asenblad, N.; Pekar, D.; Borga, O. A study of organic acid transporter-mediated pharmacokinetic interaction between NXY-059 and cefuroxime. J. Clin. Pharmacol. 2007, 47, 1043–1049. [Google Scholar] [CrossRef]
- Garton, A.; Rennie, R.; Gilpin, J.; Marrelli, M.; Shafran, S. Comparison of dose doubling with probenecid for sustaining serum cefuroxime levels. J. Antimicrob. Chemother. 1997, 40, 903–906. [Google Scholar] [CrossRef] [Green Version]
- Bousfield, P.; Mullinger, B.M.; Elstein, M. Cefuroxime: Potential use in pregnant women at term. Br. J. Obstet. Gynaecol. 1981, 88, 146–149. [Google Scholar] [CrossRef]
- Barbour, A.; Schmidt, S.; Rout, W.R.; Ben-David, K.; Burkhardt, O.; Derendorf, H. Soft tissue penetration of cefuroxime determined by clinical microdialysis in morbidly obese patients undergoing abdominal surgery. Int. J. Antimicrob. Agents 2009, 34, 231–235. [Google Scholar] [CrossRef]
- Abduljalil, K.; Ning, J.; Pansari, A.; Pan, X.; Jamei, M. Prediction of maternal and fetoplacental concentrations of cefazolin, cefuroxime and amoxicillin during pregnancy using bottom-up physiologically based pharmacokinetic models. Drug Metab. Dispos. 2022, 50, 386–400. [Google Scholar] [CrossRef]
- Nightingale, C.H.; Greene, D.S.; Quintiliani, R. Pharmacokinetics and clinical use of cephalosporin antibiotics. J. Pharm. Sci. 1975, 64, 1899–1927. [Google Scholar] [CrossRef]
- Peng, J.; Ladumor, M.K.; Unadkat, J.D. Prediction of pregnancy-induced changes in secretory and total renal clearance of drugs transported by organic anion transporters. Drug Metab. Dispos. 2021, 49, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Abduljalil, K.; Cain, T.; Humphries, H.; Rostami-Hodjegan, A. Deciding on success criteria for predictability of pharmacokinetic parameters from in vitro studies: An analysis based on in vivo observations. Drug Metab. Dispos. 2014, 42, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Shebley, M.; Sandhu, P.; Emami Riedmaier, A.; Jamei, M.; Narayanan, R.; Patel, A.; Peters, S.A.; Reddy, V.P.; Zheng, M.; de Zwart, L. Physiologically based pharmacokinetic model qualification and reporting procedures for regulatory submissions: A consortium perspective. Clin. Pharmacol. Ther. 2018, 104, 88–110. [Google Scholar] [CrossRef] [PubMed]
- Brill, M.J.; Houwink, A.P.; Schmidt, S.; Van Dongen, E.P.; Hazebroek, E.J.; van Ramshorst, B.; Deneer, V.H.; Mouton, J.W.; Knibbe, C.A. Reduced subcutaneous tissue distribution of cefazolin in morbidly obese versus non-obese patients determined using clinical microdialysis. J. Antimicrob. Chemother. 2014, 69, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Hanberg, P.; Bue, M.; Kabel, J.; Jørgensen, A.R.; Jessen, C.; Søballe, K.; Stilling, M. Effects of tourniquet inflation on peri- and postoperative cefuroxime concentrations in bone and tissue. Acta Orthop. 2021, 92, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Hosmann, A.; Ritscher, L.C.; Burgmann, H.; Oesterreicher, Z.; Jager, W.; Poschner, S.; Knosp, E.; Reinprecht, A.; Gruber, A.; Zeitlinger, M. Concentrations of cefuroxime in brain tissue of neurointensive care patients. Antimicrob. Agents Chemother. 2018, 62, e02164-17. [Google Scholar] [CrossRef] [Green Version]
- Knibbe, C.A.; Brill, M.J.; van Rongen, A.; Diepstraten, J.; van der Graaf, P.H.; Danhof, M. Drug disposition in obesity: Toward evidence-based dosing. Annu. Rev. Pharmacol. Toxicol. 2015, 55, 149–167. [Google Scholar] [CrossRef]
- Chopra, T.; Zhao, J.J.; Alangaden, G.; Wood, M.H.; Kaye, K.S. Preventing surgical site infections after bariatric surgery: Value of perioperative antibiotic regimens. Expert Rev. Pharmacoecon. Outcomes Res. 2010, 10, 317–328. [Google Scholar] [CrossRef]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg. Infect. 2013, 14, 73–156. [Google Scholar] [CrossRef]
- Bossung, V.; Lupatsii, M.; Dashdorj, L.; Tassiello, O.; Jonassen, S.; Pagel, J.; Demmert, M.; Wolf, E.A.; Rody, A.; Waschina, S.; et al. Timing of antimicrobial prophylaxis for cesarean section is critical for gut microbiome development in term born infants. Gut Microbes 2022, 14, 2038855. [Google Scholar] [CrossRef]
- Eley, V.A.; Christensen, R.; Ryan, R.; Jackson, D.; Parker, S.L.; Smith, M.; Van Zundert, A.A.; Wallis, S.C.; Lipman, J.; Roberts, J.A. Prophylactic cefazolin dosing in women with body mass index >35 kg·m2 undergoing cesarean delivery: A pharmacokinetic study of plasma and interstitial fluid. Anesth. Analg. 2020, 131, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Viberg, A.; Lannergård, A.; Larsson, A.; Cars, O.; Karlsson, M.O.; Sandström, M. A population pharmacokinetic model for cefuroxime using cystatin C as a marker of renal function. Br. J. Clin. Pharmacol. 2006, 62, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Alrammaal, H.H.; Batchelor, H.K.; Chong, H.P.; Hodgetts Morton, V.; Morris, R.K. Prophylactic perioperative cefuroxime levels in plasma and adipose tissue at the time of caesarean section (C-LACE): A protocol for a pilot experimental, prospective study with non-probability sampling to determine interpatient variability. Pilot Feasibility Stud. 2021, 7, 54. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | Cefazolin | Cefuroxime | ||
|---|---|---|---|---|
| Parameter | Value | References | Value | References |
| Molecular weight (g/mol) | 454.5 | [38] | 424.39 | [6] |
| Log p | −0.58 | [39] | −1.5 1 | |
| Compound Type | Monoprotic Acid | MonoproticAcid | [6] | |
| Acid PKa | 3.6 | [39] | 3.15 | [6] |
| B/P | 0.55 | [40] | 0.56 | [13] |
| fu | 0.225 | [4,5] | 0.67 | [3] |
| Vss (L/Kg) | 0.1 2 | 0.226 2 | ||
| Kp Scalar | 1 | 1 | ||
| Adipose permeability limited CLPD L/h | 0.1 | 0.1 | ||
| Lung tissue: plasma partition coefficient | 0.2 3 | [41] | Default (0.43) | |
| Muscle tissue: plasma partition coefficient | 0.03 3 | [41] | Default (0.25) | |
| Skin tissue: plasma partition coefficient | 0.09 | [42] | Default (0.53) | |
| Kidney tissue: plasma partition coefficient | Default (0.21) | Default (0.36) | ||
| ClPD, basel (mL/min/106 cells) | 2.07 × 10−8 | [40] | N/A | |
| ClPD, apical (mL/min/106 cells) | 2.07 × 10−8 | [40] | N/A | |
| fuKidney cell | 1 | N/A | ||
| fuUrine | 1 | N/A | ||
| CLint,T (µL/min/106 cells) by Tup,b (OAT1) | 0.208 | [40] | 9.62 4 | [13] |
| CLint,T (µL/min/106 cells) by Tup,b (OAT3) | 7.28 | [40] | N/A | |
| CLint,T (µL/min/106 cells) by Teff,a (MRP4) | 41.43 | [12] | 10 5 | [13] |
| Population | Study Code and Reference | Population Model Used | Dose (mg) | Infusion Time (min) | Number of Subjects (Proportion of Female) | Age Years (Minimum-Maximum) | Weight (kg) | Mean GA (Weeks) |
|---|---|---|---|---|---|---|---|---|
| Lean non–pregnant | 001 [8] | Sim-Healthy Volunteers | 500 | 2 | 6 (1) | N/S 1 | 62.3 | N/A |
| 002 [44] | Sim-Healthy Volunteers | 1000 | N/S (used 2 min) | 17 (0) | 21–42 | N/S 1 | N/A | |
| Pregnant | 003 [8] | Sim-Pregnancy | 500 | 2 | 6 (1) | N/S 1 | 67.9 2 | 24.5 |
| 004 [2,45] | Sim-Pregnancy | 2000 | 4 | 10 (1) | 28 (23–32) | 65.7 2 | 39.1 | |
| 005 [46] | Sim-Pregnancy | 1000 | IV bolus (N/S used 1 min) | 20 (1) | 32.5 (23–43) | 79.3 2 | 39 | |
| Obese | 006 [47] | Sim-Obese | 2000 | IV bolus (N/S used 1 min) | 37 (0.7) | 18–60 | 127 2 | N/A |
| Obese–pregnant | 007 [23] | Sim-Pregnancy 3 | 2000 | 3 | 13 (1) | 29 (23.5–34) | 113.6 2,4 | 39.3 |
| 008 [23] | Sim-Pregnancy 3 | 3000 | 3 | 13 (1) | 31(30–35) | 108 2,5 | 39 | |
| 009 [21] | Sim-Pregnancy 3 | 2000 | IV bolus (N/S used 1 min) | 28 (1) | 30 (25.5–34) | 103 2,6 | 39.2 | |
| Morbidly obese–pregnant | 0091 [22] | Sim-Pregnancy 7 | 2000 | IV bolus (0.75 min) | 11 (1) | 31.09 1 | 129.14 2 | 38.75 |
| Population | Study Code and Reference | Population Model Used | Dose (mg) | Infusion (min) | Number of Subjects (Proportion of Female) | Age (Minimum–Maximum) Years | Weight (kg) | Mean GA (Weeks) |
|---|---|---|---|---|---|---|---|---|
| Lean non–pregnant | 01 [48] | Sim-Healthy Volunteers | 1500 | N/S (used 2 min) | 12 (N/S 1) | N/S 1 | N/S 1 | N/A |
| 02 [9] | Sim-Healthy Volunteers | 750 | 1 | 7 (1) | N/S 1 | 61.7 2 | N/A | |
| 03 [49] | Sim-Healthy Volunteers | 1500 | 30 | 23 (0.26) | (19–31) | 76 2 | N/A | |
| 04 [50] | Sim-Healthy Volunteers | 750 | 20 | 10 (0.5) | 32 (18–48) | 72 | N/A | |
| 05 [50] | Sim-Healthy Volunteers | 1500 | 20 | 10 (0.5) | 32 (18–48) | 72 2 | N/A | |
| Pregnant | 06 [9] | Sim-Pregnancy | 750 | 1 | 7 (1) | N/S 1 | 64.4 | 29 |
| 07 [9] | Sim-Pregnancy | 750 | 1 | 7 (1) | N/S 1 | 74 | 41 (used 40) | |
| 08 [1] | Sim-Pregnancy | 1500 | 1 | 18 (1) | 23–37 | 78.94 | 39.5 | |
| 09 [51] | Sim-Pregnancy | 1500 | IV bolus (N/S used 1 min) | 10 (1) | 16–32 3 | 74.4 2 | At term (used 39) | |
| 091 [51] | Sim-Pregnancy | 1500 | IV bolus (N/S used 1 min) | 10 (1) | 17–36 3 | 70.3 2 | At term (used 39) | |
| Obese | 092 [52] | Sim-Morbidly Obese | 1500 | 15 4 | 6 (1) | 19–76 | 131.66 2 | N/A |
| Obese–pregnant | 1 | Sim-Pregnancy 5 | 750 | 1 | 50 (1) | 23–37 | 97.8 6 | 39.5 |
| 2 | Sim-Pregnancy 5 | 1500 | 1 | 50 (1) | 23–37 | 97.8 6 | 39.5 | |
| Morbidly obese–pregnant | 3 | Sim-Pregnancy 7 | 750 | 1 | 50 (1) | 23–37 | 128 8 | 39.5 |
| 4 | Sim-Pregnancy 7 | 1500 | 1 | 50 (1) | 23–37 | 128 8 | 39.5 |
| Study Code and Reference | Dose (mg) | AUC (mg/L·h) | Cefazolin Serum Concentration (µg/mL) at Different Time Point | Clearance (L/h) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Obs. | Sim. | Ratio 1 | Time Point (min) | Obs. | Sim. (5th, 95th Percentile) | Ratio 1 | Obs. | Sim. | Ratio 1 | ||
| 001 [8] | 500 | 110 | 130.27 | 1.18 | C10.8 | 73.24 | 66.26 (51.82, 82.85) | 0.90 | 4.04 | 3.91 | 0.97 |
| 002 [44] | 1000 | 236.15 2 | 262.60 | 1.11 | C4.4 | 188.6 | 152.72 (128.60, 179.57) | 0.81 | 3.8 | 4.01 | 1.06 |
| 003 [8] | 500 | 75.7 | 84.37 | 1.11 | C9 | 60.07 | 57.38 (45.56, 73.06) | 0.96 | 7.3 | 6.22 | 0.85 |
| 004 [2,45] | 2000 | N/R 3 | 362.97 | N/A | C82 | 57.2 | 95.74 (60.07, 135.05) | 1.67 | N/R | 5.76 | N/A |
| 005 [46] | 1000 | 139.27 2 | 172.24 | 1.24 | Cmax | 82.53 | 105.60 (86.73, 126.67) | 1.28 | 7.18 | 5.99 | 0.83 |
| 006 [47] | 2000 | N/R 3 | 415.86 | N/A | C16 | 159.96 | 131.55 (110.07, 155.41) | 0.82 | N/R | 5.04 | N/A |
| 007 [23] | 2000 | 234.3 | 307.48 | 1.31 | Cmax | 146.15 | 163.31 (133.85, 203.67) | 1.12 | 8.4 | 6.17 | 0.73 |
| 008 [23] | 3000 | 453.4 | 446.82 | 0.99 | Cmax | 223.74 | 249.68 (199.69, 301.13) | 1.12 | 6.6 | 6.35 | 0.96 |
| 009 [21] | 2000 | N/R 3 | 316.33 | N/A | C24.5 | 100.7 | 116.01 (84.16, 161.83) | 1.15 | N/R | 6.53 | N/A |
| 0091 [22] | 2000 | N/R 3 | 294.52 | N/A | C12 | 155.45 | 115.28 (85.84, 153.94) | 0.74 | N/R | 7.04 | N/A |
| Study Code and Reference | Dose (mg) | Adipose Tissue Concentration (µg/g) at Time Point | Simulated Time (Hour) of Total Adipose Tissue Concentration above MIC90 | Simulated Time (Hour) of Free ISF Adipose Tissue Concentration above MIC90 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time Point (min) | Obs. | Pred. (5th, 95th Percentile) | Ratio 1 | T > MIC of 2 µg/g | T > MIC of 4 µg/g | T > MIC of 8 µg/g | T > MIC of 2 µg/g | T > MIC of 4 µg/g | T > MIC of 8 µg/g | ||
| 001 [8] | 500 | Cmax | N/R | 4.52 (3.12, 6.29) | N/A | 2.04 | 0.6 | NA | 4.08 | 2.52 | 1.08 |
| 002 [44] | 1000 | Cmax | N/R | 7.62 (5.17, 10.84) | N/A | 3.6 | 2.04 | NA | 6 | 4.2 | 2.52 |
| 003 [8] | 500 | Cmax | N/R | 4.01 (2.56, 5.72) | N/A | 1.32 | 0.24 | NA | 3 | 1.8 | 0.72 |
| 004 [2,45] | 2000 | C31.5 | 8.7 | 14.21 (10.90, 18.55) | 1.63 | 3.72 | 2.52 | 1.44 | 5.76 | 4.56 | 3.24 |
| 005 [46] | 1000 | Cmax | N/R | 6.88 (4.47, 10.11) | N/A | 2.52 | 1.32 | NA | 4.8 | 3.36 | 2.04 |
| 006 [47] | 2000 | C16 | 8.78 | 9.18 (7.33, 10.91) | 1.05 | 5.52 | 3.24 | 0.96 | 9 | 6.48 | 4.08 |
| 007 [23] | 2000 | C25 | 12.4 | 9.85 (7.30, 13.86) | 0.79 | 4.08 | 2.4 | 0.84 | 7.08 | 5.28 | 3.48 |
| 008 [23] | 3000 | C28 | 16.8 | 14.39 (10.78, 19.59) | 0.86 | 5.04 | 3.36 | 1.8 | 8.04 | 6.24 | 4.44 |
| 009 [21] | 2000 | C24.5 | 9.4 | 10.08 (7.67, 13.79) | 1.07 | 4.08 | 2.4 | 0.96 | 6.96 | 5.16 | 3.48 |
| 0091 [22] | 2000 | C12 | 18.36 ± 6.68 | 8.89 (6.16, 12.05) | 0.48 2 | 4.08 | 2.28 | 0.6 | 7.44 | 5.4 | 3.48 |
| C60 | 21.73 ± 16.02 | 6.85 (4.95, 9.01) | 0.32 2 | ||||||||
| Study Code and Reference | Dose(mg) | AUC (mg/L·h) | Cefuroxime Serum Concentration (µg/mL) at Time Point | Clearance (L/h) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Obs. | Sim. | Ratio 1 | Time Point (min) | Obs. | Sim. (5th, 95th Percentile) | Ratio 1 | Obs. | Sim. | Ratio 1 | ||
| 01 [48] | 1500 | N/R 2 | 150.99 | N/A | C10 | 130.8 | 91.04 (69.23, 114.79) | 0.70 | N/R | 11.36 | N/A |
| 02 [9] | 750 | 60.8 | 75.79 | 1.25 | C9.6 | 51.48 | 52.19 (41.15, 63.31) | 1.01 | 11.9 | 12.14 | 1.02 |
| 03 [49] | 1500 | 124 | 153.89 | 1.24 | C16.8 | 56.35 | 65.21 (53.63, 78.74) | 1.16 | 12.09 3 | 10.99 | 0.91 |
| 04 [50] | 750 | 77 | 78.03 | 1.01 | C20 | 75.29 | 58.61 (45.73, 73.63) | 0.78 | 9.74 3 | 11.48 | 1.18 |
| 05 [50] | 1500 | 137 | 157.20 | 1.15 | C18 | 82.08 | 110.83 (86.74, 138.67) | 1.35 | 10.9 3 | 11.48 | 1.05 |
| 06 [9] | 750 | 42.0 | 61.09 | 1.45 | C7.8 | 43.56 | 45.29 (37.65, 53.94) | 1.04 | 16.9 | 11.98 | 0.71 |
| 07 [9] | 750 | 46.7 | 63.33 | 1.36 | C9 | 43.83 | 39.73 (33.94, 46.55) | 0.91 | 15.5 | 11.57 | 0.75 |
| 09 [51] | 1500 | N/R | 121.51 | N/A | C30 | 55.2 | 56.02 (42.21, 71.86) | 1.01 | N/R | 11.92 | N/A |
| 091 [51] | 1500 | N/R | 123.86 | N/A | C48 | 74.8 | 45.51 (31.75, 57.04) | 0.61 | N/R | 11.57 | N/A |
| 092 [52] | 1500 | 158.7 | 130.76 | 0.82 | C30 | 64.25 | 48.13 (39.02, 57.18) | 0.75 | 8.39 | 12.33 | 1.47 |
| Scenario 1 | 750 | N/A | 60.98 | N/A | Cmax | N/A | 37.75 (30.74, 45.99) | N/A | N/A | 11.98 | N/A |
| Scenario 2 | 1500 | N/A | 121.97 | N/A | Cmax | N/A | 75.51 (61.48, 91.97) | N/A | N/A | 11.98 | N/A |
| Scenario 3 | 750 | N/A | 57.40 | N/A | Cmax | N/A | 31.76 (25.84, 38.35) | N/A | N/A | 12.85 | N/A |
| Scenario 4 | 1500 | N/A | 114.79 | N/A | Cmax | N/A | 63.52 (51.67, 76.70) | N/A | N/A | 12.85 | N/A |
| Study Code and Reference | Dose (mg) | Adipose Tissue Concentration (µg/g) at Time Point | Simulated Time (Hour) of Total Adipose Tissue Concentration above MIC90 | Simulated Time (Hour) of Free ISF Adipose Tissue Concentration above MIC90 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time Point (min) | Obs. | Pred. (5th, 95th Percentile) | Ratio 1 | T > MIC of 2 µg/g | T > MIC of 4 µg/g | T > MIC of 8 µg/g | T > MIC of 2 µg/g | T > MIC of 4 µg/g | T > MIC of 8 µg/g | ||
| 01 [48] | 1500 | C10 | 16.5 | 6.55 (3.38, 10.48) | 0.40 2 | 2.35 | 1.09 | N/A | 6.32 | 4.88 | 3.49 |
| 02 [9] | 750 | Cmax | N/R | 4.24 (2.44, 6.83) | N/A | 1.14 | 0.18 | N/A | 4.32 | 3.18 | 2.10 |
| 03 [49] | 1500 | Cmax | N/R | 5.53 (3.51, 7.93) | N/A | 2.52 | 1.26 | N/A | 6.60 | 5.10 | 3.72 |
| 04 [50] | 750 | Cmax | N/R | 3.19 (1.87, 4.60) | N/A | 1.215 | N/A | N/A | 4.95 | 3.60 | 2.30 |
| 05 [50] | 1500 | Cmax | N/R | 6.36 (3.84, 9.10) | N/A | 2.46 | 1.20 | N/A | 6.36 | 4.92 | 3.60 |
| 06 [9] | 750 | Cmax | N/R | 3.15 (2.25, 4.49) | N/A | 0.9 | N/A | N/A | 4.14 | 3.00 | 1.86 |
| 07 [9] | 750 | Cmax | N/R | 2.88 (2.16, 3.80) | N/A | 0.84 | NA | N/A | 4.50 | 3.24 | 2.04 |
| 08 [1] | 1500 | Cmax | N/R | 5.72 (4.35, 7.32) | N/A | 2.04 | 0.84 | N/A | 5.76 | 4.44 | 3.24 |
| 09 [51] | 1500 | Cmax | N/R | 6.14 (3.75, 10.81) | N/A | 1.92 | 0.84 | N/A | 5.52 | 4.32 | 3.12 |
| 091 [51] | 1500 | Cmax | N/R | 6.88 (3.86, 10.45) | N/A | 1.92 | 0.84 | NA | 5.40 | 4.20 | 3.12 |
| 092 [52] | 1500 | Cmax | 36.06 3 | 33.74 3 (29.62, 37.84) | 0.94 | 2.1 | 0.66 | N/A | 6.72 | 5.10 | 3.48 |
| Scenario 1 4 | 750 | Cmax | N/A | 2.72 (1.82, 4.05) | N/A | 0.6 | N/A | N/A | 4.68 | 3.24 | 1.92 |
| Scenario 2 4 | 1500 | Cmax | N/A | 5.43 (3.64, 8.10) | N/A | 1.92 | 0.6 | N/A | 6.12 | 4.68 | 3.24 |
| Scenario 3 4 | 750 | Cmax | N/A | 2.22 (1.68, 2.88) | N/A | 0.36 | N/A | N/A | 4.92 | 3.36 | 1.8 |
| Scenario 4 4 | 1500 | Cmax | N/A | 4.44 (3.36, 5.75) | N/A | 1.8 | 0.36 | N/A | 6.48 | 4.92 | 3.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alrammaal, H.H.; Abduljalil, K.; Hodgetts Morton, V.; Morris, R.K.; Marriott, J.F.; Chong, H.P.; Batchelor, H.K. Application of a Physiologically Based Pharmacokinetic Model to Predict Cefazolin and Cefuroxime Disposition in Obese Pregnant Women Undergoing Caesarean Section. Pharmaceutics 2022, 14, 1162. https://doi.org/10.3390/pharmaceutics14061162
Alrammaal HH, Abduljalil K, Hodgetts Morton V, Morris RK, Marriott JF, Chong HP, Batchelor HK. Application of a Physiologically Based Pharmacokinetic Model to Predict Cefazolin and Cefuroxime Disposition in Obese Pregnant Women Undergoing Caesarean Section. Pharmaceutics. 2022; 14(6):1162. https://doi.org/10.3390/pharmaceutics14061162
Chicago/Turabian StyleAlrammaal, Hanadi H., Khaled Abduljalil, Victoria Hodgetts Morton, R. Katie Morris, John F. Marriott, Hsu P. Chong, and Hannah K. Batchelor. 2022. "Application of a Physiologically Based Pharmacokinetic Model to Predict Cefazolin and Cefuroxime Disposition in Obese Pregnant Women Undergoing Caesarean Section" Pharmaceutics 14, no. 6: 1162. https://doi.org/10.3390/pharmaceutics14061162
APA StyleAlrammaal, H. H., Abduljalil, K., Hodgetts Morton, V., Morris, R. K., Marriott, J. F., Chong, H. P., & Batchelor, H. K. (2022). Application of a Physiologically Based Pharmacokinetic Model to Predict Cefazolin and Cefuroxime Disposition in Obese Pregnant Women Undergoing Caesarean Section. Pharmaceutics, 14(6), 1162. https://doi.org/10.3390/pharmaceutics14061162