
A Composite System Based upon Hydroxypropyl Cyclodextrins and Soft Hydrogel Contact Lenses for the Delivery of Therapeutic Doses of Econazole to the Cornea, In Vitro

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Solubility Determinations
2.3. Corneal Delivery of Econazole In Vitro
2.4. HPLC Analysis
2.5. Statistical Analysis
2.6. Molecular Dynamic Simulation
2.7. Mycological Evaluation
3. Results
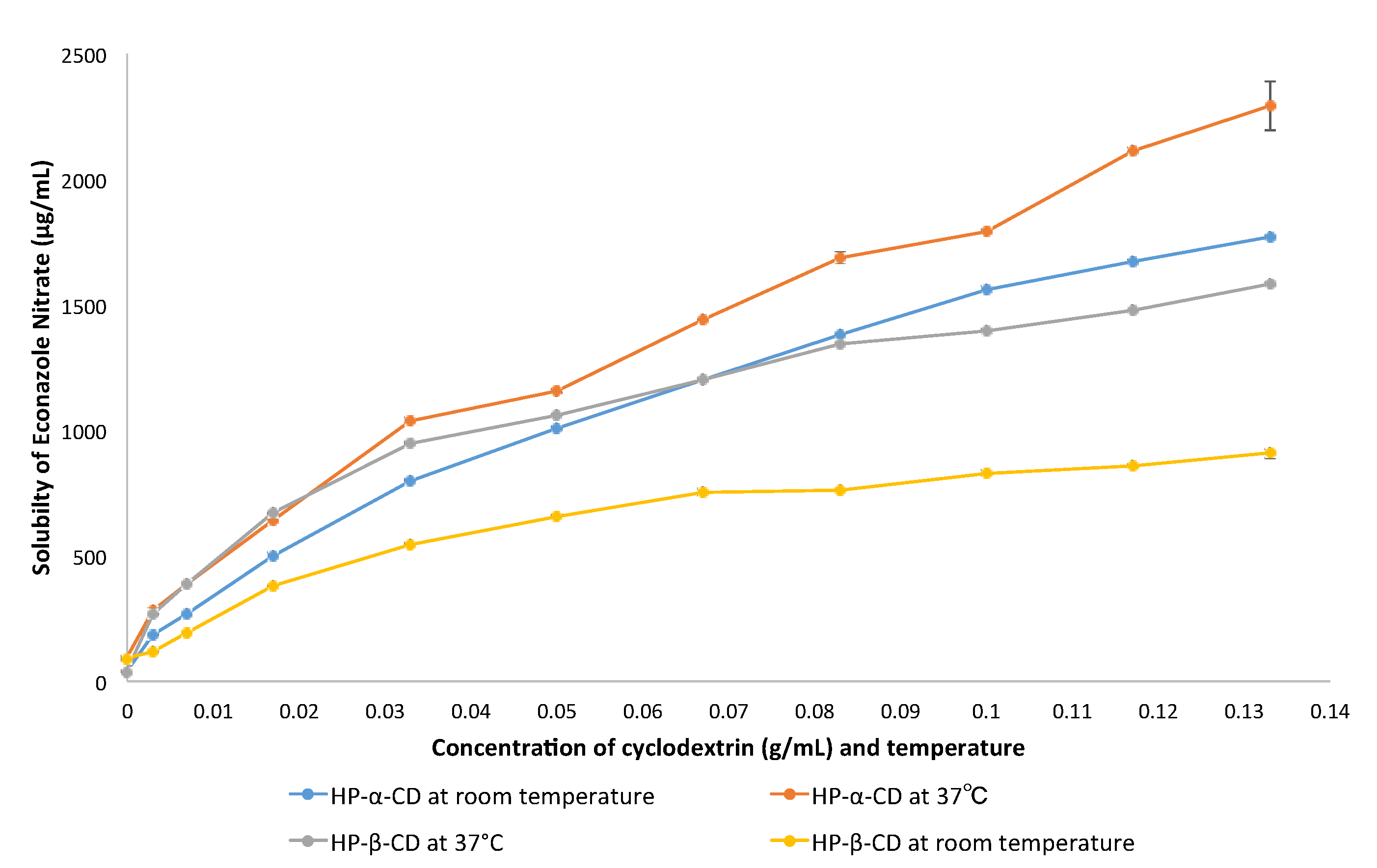
3.1. Econazole Solubility
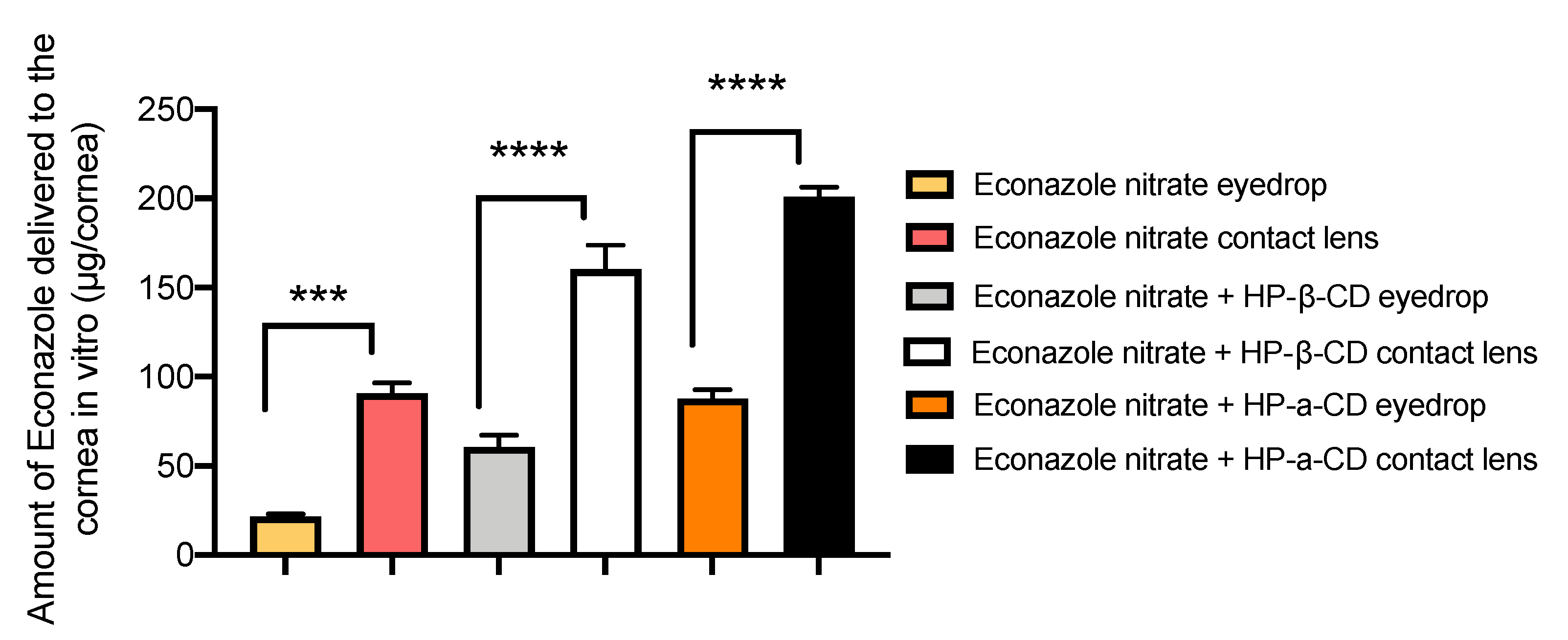
3.2. Corneal Delivery of Econazole in the Presence of Cyclodextrin and Contact Lenses
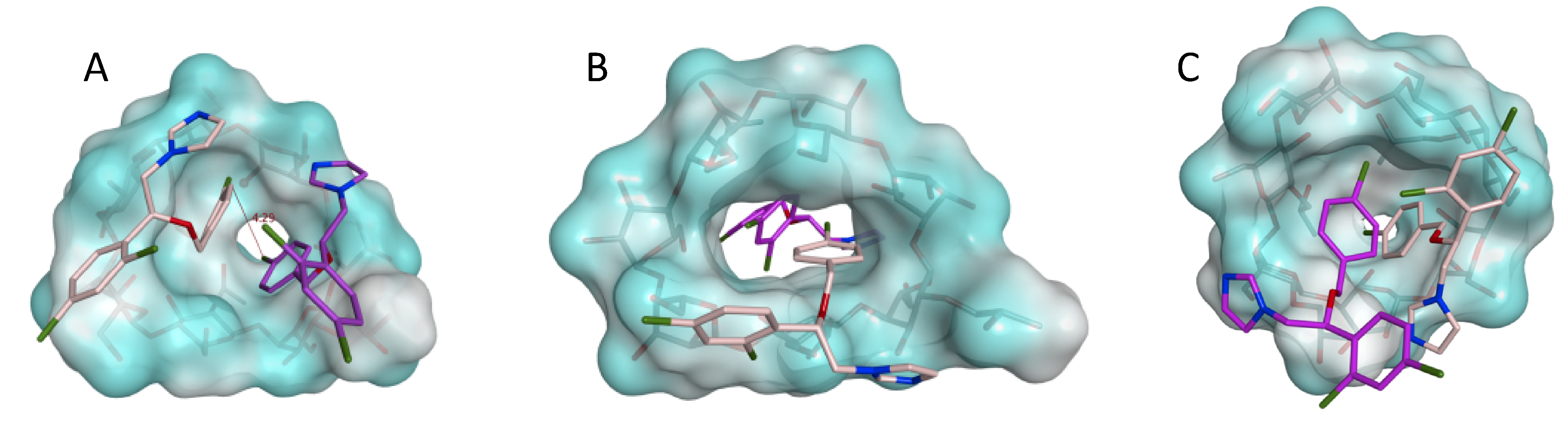
3.3. Molecular Dynamic Simulations
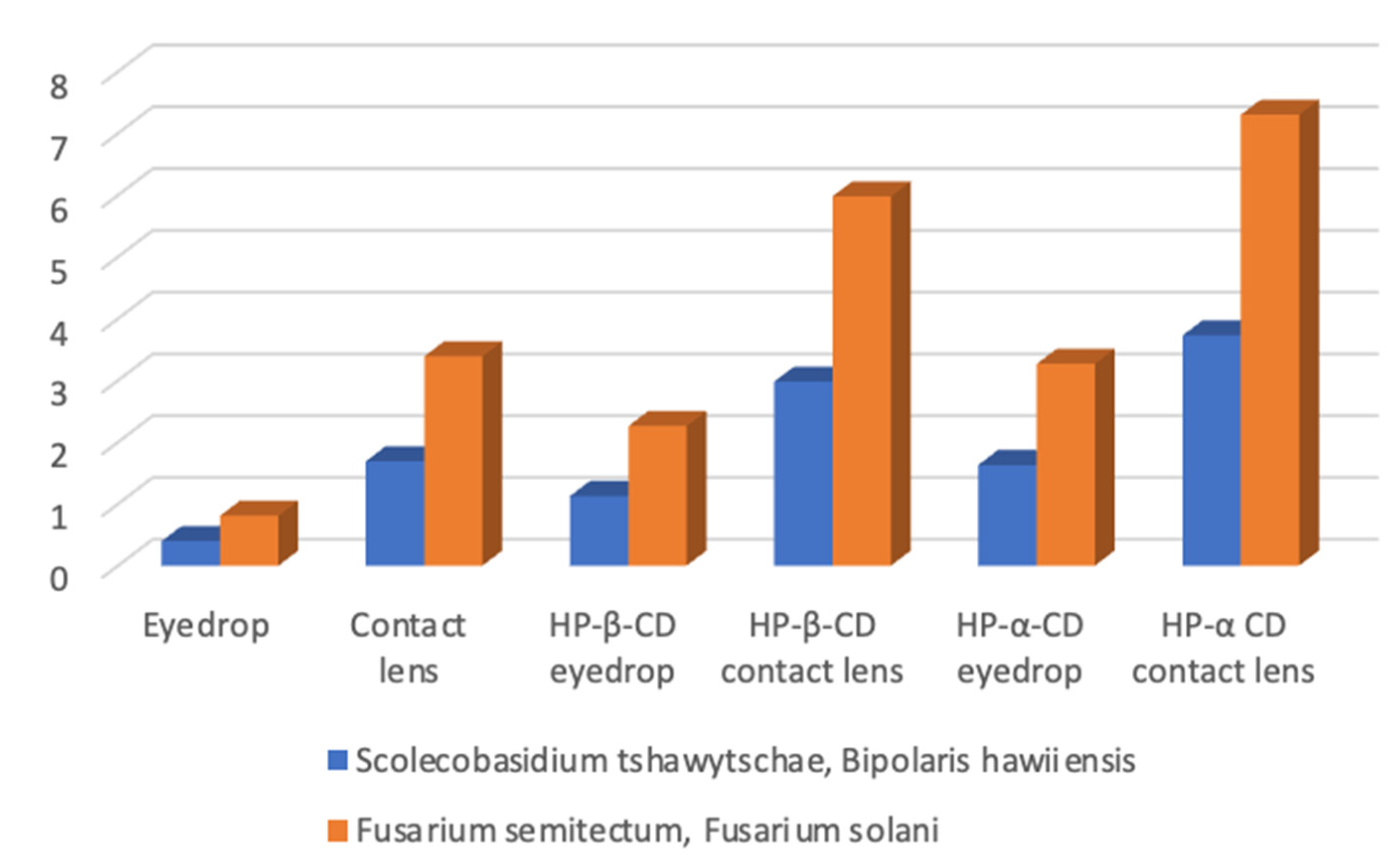
3.4. Antifungal Activity
4. Discussion
4.1. Solubility Enhancement by Cyclodextrins
4.2. The Relationship between Solubility Enhancement of Econazole and Amount of Added HP-α-CD and HP-β-CD
4.3. Effect of HP-β-CD on the Corneal Delivery of Econazole
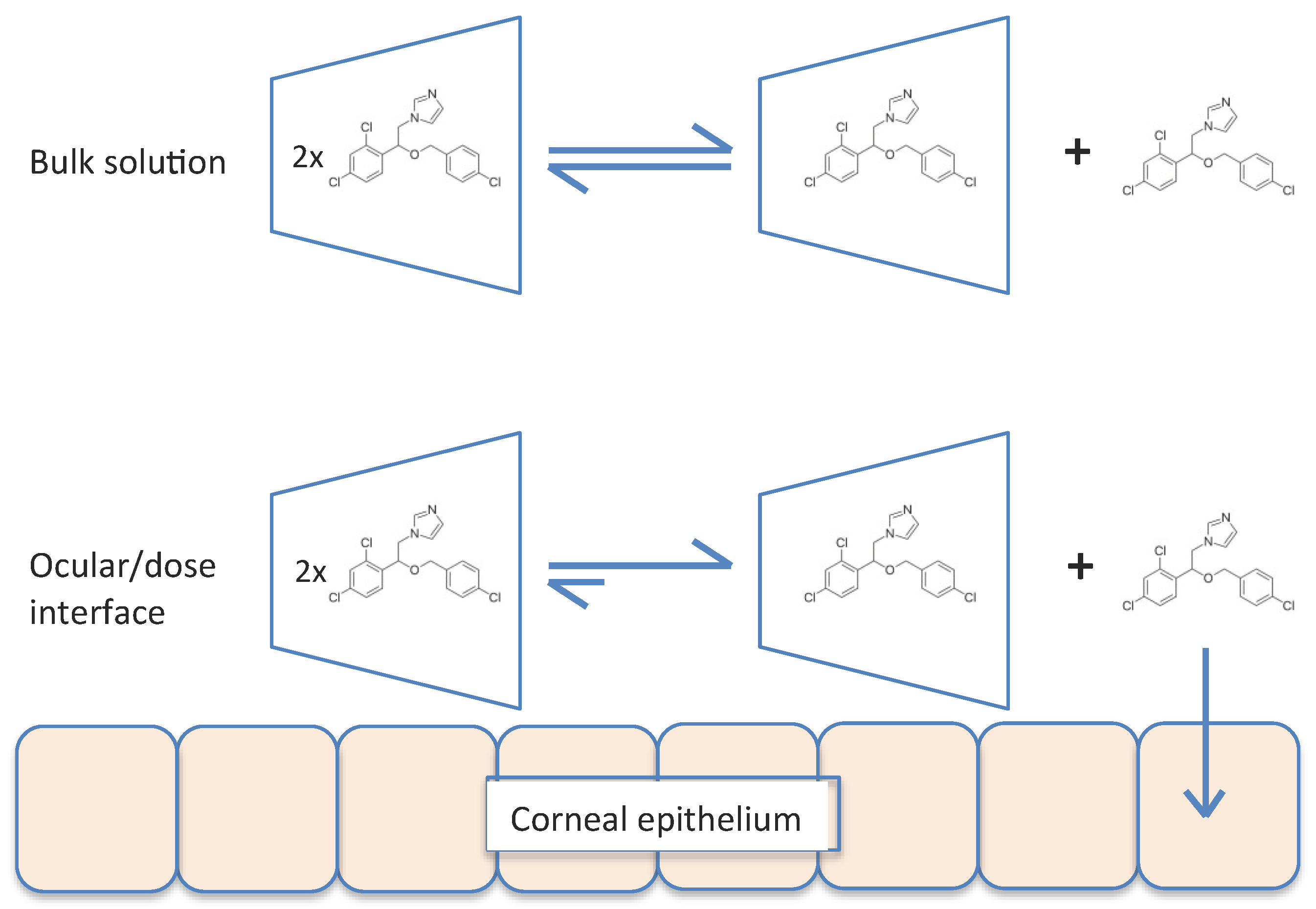
4.4. Mechanism for the Enhanced Corneal Delivery Econazole Using the Composite Contact Lens–HP-α-CD System
4.5. Clinical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ansari, Z.; Miller, D.; Galor, A. Current thoughts in fungal keratitis: Diagnosis and Treatment. Curr. Fungal Infect. Rep. 2013, 7, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.; Verma, A. Fungal Keratitis Treatment & Management: Medical Care, Surgical Care. Medscape. Available online: http://emedicine.medscape.com/article/1194167-treatment#d9 (accessed on 13 January 2017).
- Hendricks, R.L. Corneal nerve damage in microbial keratitis. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, A.; Loughnan, M. Anterior Eye Disease and Therapeutics A–Z, 2nd ed.; Elsevier: Chatswood, Australia, 2011; ISBN 9780729579575. [Google Scholar]
- McGhee, C.; Kim, B. Fungal keratitis: Dealing with a diverse kingdom of ocular assailants. Clin. Experiment. Ophthalmol. 2016, 44, 755–756. [Google Scholar] [CrossRef] [PubMed]
- Prajna, N.; John, R.; Nirmalan, P.; Lalitha, P.; Srinivasan, M. A randomised clinical trial comparing 2% econazole and 5% natamycin for the treatment of fungal keratitis. Br. J. Ophthalmol. 2003, 87, 1235–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ananthula, H.K.; Vaishya, R.D.; Barot, M.; Mitra, A.K. Duane’s Ophthalmology. In Bioavailability; Tasman, W., Jaeger, E.A., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009. [Google Scholar]
- Patel, A.; Cholkar, K.; Agrahari, V.; Mitra, A.K. Ocular drug delivery systems: An overview. World Pharmacol. 2013, 2, 47–64. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Tomé, V.; Luaces-Rodríguez, A.; Silva-Rodríguez, J.; Blanco-Dorado, S.; García-Quintanilla, L.; Llovo-Taboada, J.; Blanco-Méndez, J.; García-Otero, X.; Varela-Fernández, R.; Herranz, M.; et al. Ophthalmic econazole hydrogels for the treatment of fungal keratitis. J. Pharm. Sci. 2018, 107, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Loftsson, T.; Järvinen, T. Cyclodextrins in ophthalmic drug delivery. Adv. Drug Deliv. Rev. 1999, 36, 59–79. [Google Scholar] [CrossRef]
- Loftsson, T.; Hreinsdóttir, D.; Másson, M. Evaluation of cyclodextrin solubilization of drugs. Int. J. Pharm. 2005, 302, 18–28. [Google Scholar] [CrossRef]
- Loftsson, T.; Stefansson, E. Cyclodextrins in eye drop formulations: Enhanced topical delivery of corticosteroids to the eye. Acta Ophthalmol. Scand. 2002, 80, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Mura, P.; Liguori, A.; Bramanti, G.; Bettinetti, G.P.; Campisi, E.; Faggi, E. Improvement of dissolution properties and microbiological activity of miconazole and econazole by cyclodextrin complexation. Eur. J. Pharm. Biopharm. 1992, 38, 119–123. [Google Scholar]
- Abd El-Gawad, A.E.H.; Soliman, O.A.; El-Dahan, M.S.; Al-Zuhairy, S.A.S. Improvement of the ocular bioavailability of econazole nitrate upon complexation with cyclodextrins. AAPS PharmSciTech. 2017, 18, 1795–1809. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.R. Drug delivery through soft contact lenses. Br. J. Ophthalmol. 1988, 72, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Cho, S.; Park, H.S.; Kwon, I. Ocular Drug Delivery through pHEMA-hydrogel contact lenses co-loaded with lipophilic vitamins. Sci. Rep. 2016, 6, 34194. [Google Scholar] [CrossRef] [PubMed]
- Li, C.C.; Chauhan, A. Modeling ophthalmic drug delivery by soaked contact lenses. Ind. Eng. Chem. Res. 2006, 45, 3718–3734. [Google Scholar] [CrossRef]
- Li, X.; Zhao, Y.; Wang, K.; Wang, L.; Yang, X.; Zhu, S. Cyclodextrin-containing hydrogels as an intraocular lens for sustained drug release. PLoS ONE 2017, 12, 0189778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irie, T.; Uekama, K. Pharmaceutical applications of cyclodextrins III, toxicological issues and safety evaluation. J. Pharm. Sci. 1997, 86, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Cyclodextrins Used as Excipients. European Medicines Agency. 2017. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2017/10/WC500235904.pdf (accessed on 18 January 2019).
- Chan, W.; Akhbanbetova, A.; Quantock, A.J.; Heard, C.M. Topical delivery of a Rho-kinase inhibitor to the cornea via mucoadhesive film. Eur. J. Pharm. Sci. 2016, 97, 256–264. [Google Scholar] [CrossRef] [Green Version]
- Molecular Operating Environment (MOE); Chemical Computing Group ULC: Montreal, QC, Canada, 2022.
- Schrödinger Release 2017-1: Maestro; Schrödinger, LLC: New York, NY, USA, 2017.
- Faucci, M.T.; Melani, F.; Mura, P. 1H-NMR and molecular modelling techniques for the investigation of the inclusion complex of econazole with α-cyclodextrin in the presence of malic acid. J. Pharm. Biomed. Anal. 2000, 23, 25–31. [Google Scholar] [CrossRef]
- Drugbank. Econazole. Available online: https://www.drugbank.ca/drugs/DB01127 (accessed on 10 August 2018).
- Drugbank. HP-β-CD. Available online: https://go.drugbank.com/ (accessed on 27 May 2022).
- Schrödinger Release 2017-1: Desmond Molecular Dynamics System; D.E. Shaw Research: New York, NY, USA, 2017.
- Walther, G.; Stasch, S.; Kaerger, K.; Hamprecht, A.; Roth, M.; Cornely, O.A.; Geerling, G.; Mackenzie, C.R.; Kurzai, O.; von Lilienfeld-Toal, M. Fusarium keratitis in Germany. J. Clin. Microbiol. 2017, 55, 2983–2995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willey, J.D. The effect of ionic strength on the solubility of an electrolyte. J. Chem. Educ. 2004, 81, 1644–1646. [Google Scholar] [CrossRef]
- Harris, D.C. Quantitative Chemical Analysis, 9th ed.; W.H. Freeman and Company: New York, NY, USA, 2016. [Google Scholar]
- Chemicalbook. Available online: https://www.chemicalbook.com/ProductChemicalPropertiesCB8416047_EN.htm (accessed on 10 August 2018).
- Chen, G.; Chen, J.; Cheng, C.; Cong, Y.; Du, C.; Zhao, H. Solubility and preferential solvation of econazole nitrate in binary solvent mixtures of methanol, ethanol and 1,4-dioxane in water. J. Chem. Thermodyn. 2017, 111, 228–237. [Google Scholar] [CrossRef]
- Pedersen, M.; Edelsten, M.; Nielsen, V.F.; Scarpellini, A.; Skytte, S.; Slot, C. Formation and antimycotic effect of cyclodextrin inclusion complexes of econazole and miconazole. Int. J. Pharm. 1993, 90, 247–254. [Google Scholar] [CrossRef]
- Acuvue Brand Contact Lenses. Available online: https://www.acuvue.co.uk/Unique (accessed on 13 August 2018).
- Siefert, B.; Keipert, S. Influence of alpha-cyclodextrin and hydroxyalkylated β-cyclodextrin derivatives on the in vitro corneal uptake and permeation of aqueous pilocarpine-HCl solutions. J. Pharm. Sci. 1997, 86, 716–720. [Google Scholar] [CrossRef] [PubMed]
- Tkacova, M.; Zivcak, J.; Foffova, P. A Reference for Human Eye Surface Temperature Measurements in Diagnostic Process of Ophthalmologic Diseases. 2011. Available online: http://www.measurement.sk/M2011/doc/proceedings/406_Tkacova-2.pdf (accessed on 5 October 2016).
- Morin, N.; Crini, G.; Cosentino, C.; Millet, J.; Vebrel, J.; Rouland, J.-C. Formation of two particular structures between β-cyclodextrin and bifonazole: β-cyclodextrin–bifonazole and (β-cyclodextrin)i–bifonazole (where 2 < i < 3). J. Chem. Soc. Perkin Trans. 1999, 2, 2647–2651. [Google Scholar]
- Loftsson, T.; Magnúsdóttir, A.; Másson, M.; Sigurjónsdóttir, J.F. Self-association and cyclodextrin solubilization of drugs. J. Pharm. Sci. 2002, 91, 2307–2316. [Google Scholar] [CrossRef]
- Stella, V.; Rao, V.; Zannou, E.; Zia, V. Mechanisms of drug release from cyclodextrin complexes. Adv. Drug Deliv. Rev. 1999, 36, 3–16. [Google Scholar] [CrossRef]
- Hara, H.; Cooper, D. Xenotransplantation-the future of corneal transplantation? Cornea 2011, 30, 371–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarho, P.; Urtti, A.; Pate, D.; Suhonen, P.; Järvinen, T. Increase in aqueous solubility, stability and in vitro corneal permeability of anandamide by hydroxypropyl-β-cyclodextrin. Int. J. Pharm. 1996, 137, 209–216. [Google Scholar] [CrossRef]
- López, C.; de Vries, A.; Marrink, S. Molecular mechanism of cyclodextrin mediated cholesterol extraction. PLoS Comput. Biol. 2011, 7, e1002020. [Google Scholar] [CrossRef] [Green Version]
- Maulvi, F.A.; Soni, T.G.; Shah, D.O. A review on therapeutic contact lenses for ocular drug delivery. Drug Deliv. 2016, 23, 3017–3026. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Conway, A.; Chauhan, A. Extended delivery of ophthalmic drugs by silicone hydrogel contact lenses. Biomaterials 2008, 29, 2259–2269. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, X.; Sun, F. Cyclodextrin-containing hydrogels for contact lenses as a platform for drug incorporation and release. Acta Biomaterialia 2010, 6, 486–493. [Google Scholar] [CrossRef]
- Yang, L.; Wang, C.; Li, L.; Zhu, F.; Ren, X.; Huang, Q.; Cheng, Y.; Li, Y. Bioinspired integration of naturally occurring molecules towards universal and smart antibacterial coatings. Adv. Funct. Mater. 2021, 32, 2108749. [Google Scholar] [CrossRef]
- Shobana, C.S.; Mythili, A.; Homa, M.; Galgóczy, L.; Priya, R.; Singh, Y.B.; Panneerselvam, K.; Vágvölgyi, C.; Kredics, L.; Narendran, V.; et al. In vitro susceptibility of filamentous fungi from mycotic keratitis to azole drugs. J. Mycol. Med. 2015, 25, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.S.; Al-Hatmi, A.M.; Shobana, C.S.; van Diepeningen, A.D.; Kredics, L.; Vágvölgyi, C.; Homa, M.; Meis, J.F.; de Hoog, G.S.; Narendran, V.; et al. Antifungal susceptibility and phylogeny of opportunistic members of the genus fusarium causing human keratomycosis in South India. Med. Mycol. 2016, 4, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manikandan, P.; Varga, J.; Kocsubé, S.; Anita, R.; Revathi, R.; Németh, T.M.; Narendran, V.; Vágvölgyi, C.; Panneer Selvam, K.; Shobana, C.S.; et al. Epidemiology of Aspergillus keratitis at a tertiary care eye hospital in South India and antifungal susceptibilities of the causative agents. Mycoses 2013, 56, 26–33. [Google Scholar] [CrossRef]
- Morgan, S.R.; Pilia, N.; Hewitt, M.; Lewis, P.N.; Morrison, P.; Kelly, S.L.; Parker, J.E.; Whitaker, D.; Quantock, A.J.; Heard, C.M.; et al. Controlled in vitro delivery of voriconazole and diclofenac to the cornea using contact lenses for the treatment of Acanthamoeba keratitis. Int. J. Pharm. 2020, 579, 119102. [Google Scholar] [CrossRef]
- Arora, I.; Kulshrestha, O.P.; Upadhaya, S. Treatment of fungal corneal ulcers with econazole. Indian J. Ophthalmol. 1983, 31 (Suppl. 7), 1019–1021. [Google Scholar] [PubMed]
- Galarreta, D.J.; Tuft, S.J.; Ramsay, A.; Dart, J.K. Fungal keratitis in London: Microbiological and clinical evaluation. Cornea 2007, 26, 1082–1086. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.S.; Fung, S.S.; Macleod, D.; Dart, J.K.; Tuft, S.J.; Burton, M.J. Altered patterns of fungal keratitis at a london ophthalmic referral hospital: An eight-year retrospective observational study. Am. J. Ophthalmol. 2016, 168, 227–236. [Google Scholar] [CrossRef] [Green Version]
- Berry, M.; Gurung, A.; Easty, D.L. Toxicity of antibiotics and antifungals on cultured human corneal cells: Effect of mixing, exposure and concentration. Eye 1995, 9, 110–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelkader, H.; Fathalla, Z.; Moharram, H.; Ali, T.F.; Pierscionek, B. Cyclodextrin enhances corneal tolerability and reduces ocular toxicity caused by diclofenac. Oxid. Med. Cell. Longev. 2018, 2018, 5260976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, T.; Xhonneux, B.; Mesens, J.; Borgers, M. Beta-cyclodextrins as vehicles in eye-drop formulations: An evaluation of their effects on rabbit corneal epithelium. Lens Eye Toxic. Res. 1990, 7, 459–468. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| g/mL CD | M HP-α-CD | Room Temperature | 37 °C | M HP-β-CD | Room Temperature | 37 °C | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| μg/mL Econazole | M Econazole | M CD/M Econazole | μg/mL Econazole | M Econazole | M CD/M Econazole | μg/mL Econazole | M Econazole | M CD/M Econazole | μg/mL Econazole | M Econazole | M CD/M Econazole | |||
| 0 | 0 | 38.03 | 2.33 × 10−4 | - | 91.35 | 4.11 × 10−4 | - | 0 | 88.73 | 2.33 × 10−4 | - | 156.91 | 4.11 × 10−4 | - |
| 0.0033 | 2.80 × 10−3 | 185.29 | 4.85 × 10−4 | 5.77 | 280.18 | 7.34 × 10−4 | 3.81 | 2.40 × 10−3 | 119.77 | 3.14 × 10−4 | 7.64 | 268.09 | 7.02 × 10−4 | 3.42 |
| 0.0066 | 5.59 × 10−3 | 268.14 | 7.49 × 10−4 | 7.46 | 384.02 | 1.00 × 10−3 | 5.59 | 4.80 × 10−3 | 192.33 | 5.04 × 10−4 | 9.52 | 386.43 | 1.01 × 10−3 | 4.75 |
| 0.0165 | 8.47 × 10−3 | 497.65 | 1.30 × 10−3 | 6.51 | 638.27 | 1.67 × 10−3 | 5.07 | 1.82 × 10−2 | 378.73 | 9.92 × 10−4 | 18.37 | 668.76 | 1.75 × 10−3 | 10.4 |
| 0.033 | 2.79 × 10−2 | 800.65 | 2.10 × 10−3 | 13.29 | 1038.51 | 2.72 × 10−3 | 10.36 | 2.40 × 10−2 | 547.47 | 1.43 × 10−3 | 16.78 | 950.05 | 2.49 × 10−3 | 9.64 |
| 0.05 | 4.24 × 10−2 | 1010.17 | 2.65 × 10−3 | 16.00 | 1155.01 | 3.30 × 10−3 | 12.85 | 3.64 × 10−2 | 657.45 | 1.72 × 10−3 | 21.16 | 1062.3 | 2.78 × 10−3 | 13.09 |
| 0.066 | 5.59 × 10−2 | 1199.41 | 3.14 × 10−3 | 17.80 | 1438.15 | 3.77 × 10−3 | 14.83 | 4.80 × 10−2 | 755.42 | 2.03 × 10−3 | 23.65 | 1200.61 | 3.14 × 10−3 | 15.29 |
| 0.0825 | 6.99 × 10−2 | 1383.41 | 3.62 × 10−3 | 19.31 | 1689.42 | 4.43 × 10−3 | 15.78 | 6.00 × 10−2 | 762 | 2.00 × 10−3 | 30.00 | 1343.19 | 3.52 × 10−3 | 17.05 |
| 0.1 | 8.47 × 10−2 | 1561.05 | 4.09 × 10−3 | 20.71 | 1794.04 | 4.70 × 10−3 | 18.02 | 7.27 × 10−2 | 831.69 | 2.18 × 10−3 | 33.35 | 1398.24 | 3.66 × 10−3 | 19.86 |
| 0.1155 | 9.79 × 10−2 | 1673.3 | 4.38 × 10−3 | 22.35 | 2116.84 | 5.54 × 10−3 | 17.67 | 8.40 × 10−2 | 861.6 | 2.26 × 10−3 | 33.17 | 1479.49 | 3.88 × 10−3 | 21.65 |
| 0.132 | 1.19 × 10−1 | 1769.13 | 4.63 × 10−3 | 25.70 | 2293.58 | 6.00 × 10−3 | 19.83 | 9.60 × 10−2 | 908.56 | 2.37 × 10−3 | 40.51 | 1584.94 | 4.15 × 10−3 | 23.13 |
| Fungal Strain | Fusarium semitectum | Fusarium solani | Scolecobasidium tshawytschae | Bipolaris hawaiiensis |
|---|---|---|---|---|
| Mean MIC [econazole], μg/mL | 141 | 141 | 283 | 283 |
| [Econazole] required in cornea (MIC×0.19), μg | 26.79 | 26.79 | 53.77 | 53.77 |
| [Econazole] in cornea, @ 6h; econazole only eyedrop | 21.66 ± 2.36 | 21.66 ± 2.36 | 21.66 ± 2.36 | 21.66 ± 2.36 |
| Factor, [econazole] delivered/MIC×0.19 | ×0.81 | ×0.81 | ×0.40 | ×0.40 |
| [Econazole] in cornea, @ 6h; econazole contact lens | 90.88 ± 9.75 | 90.88 ± 9.75 | 90.88 ± 9.75 | 90.88 ± 9.75 |
| Factor, [econazole] delivered/MIC×0.19 | ×3.39 | ×3.39 | ×1.69 | ×1.69 |
| [Econazole] in cornea, @ 6h; econazole + HP-β-CD eyedrop | 60.57 ± 11.47 | 60.57 ± 11.47 | 60.57 ± 11.47 | 60.57 ± 11.47 |
| Factor, [econazole] delivered/MIC×0.19 | ×2.26 | ×2.26 | ×1.13 | ×1.13 |
| [Econazole] in cornea, @ 6h; econazole + HP-β-CD contact lens | 160.17 ± 23.63 | 160.17 ± 23.63 | 160.17 ± 23.63 | 160.17 ± 23.63 |
| Factor, [econazole] delivered/MIC×0.19 | ×5.98 | ×5.98 | ×2.98 | ×2.98 |
| [Econazole] in cornea, @ 6h; econazole + HP-α-CD eyedrop | 87.65 ± 8.74 | 87.65 ± 8.74 | 87.65 ± 8.74 | 87.65 ± 8.74 |
| Factor, [econazole] delivered/MIC×0.19 | ×3.27 | ×3.27 | ×1.63 | ×1.63 |
| [Econazole] in cornea, @ 6h; econazole + HP-α-CD contact lens | 200.8 ± 9.6 | 200.8 ± 9.6 | 200.8 ± 9.6 | 200.8 ± 9.6 |
| Factor, [econazole] delivered/MIC×0.19 | ×7.5 | ×7.5 | ×3.73 | ×3.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, A.; Fallon, M.; Celiksoy, V.; Ferla, S.; Varricchio, C.; Whitaker, D.; Quantock, A.J.; Heard, C.M. A Composite System Based upon Hydroxypropyl Cyclodextrins and Soft Hydrogel Contact Lenses for the Delivery of Therapeutic Doses of Econazole to the Cornea, In Vitro. Pharmaceutics 2022, 14, 1631. https://doi.org/10.3390/pharmaceutics14081631
Wong A, Fallon M, Celiksoy V, Ferla S, Varricchio C, Whitaker D, Quantock AJ, Heard CM. A Composite System Based upon Hydroxypropyl Cyclodextrins and Soft Hydrogel Contact Lenses for the Delivery of Therapeutic Doses of Econazole to the Cornea, In Vitro. Pharmaceutics. 2022; 14(8):1631. https://doi.org/10.3390/pharmaceutics14081631
Chicago/Turabian StyleWong, Anepmete, Melissa Fallon, Vildan Celiksoy, Salvatore Ferla, Carmine Varricchio, David Whitaker, Andrew J. Quantock, and Charles M. Heard. 2022. "A Composite System Based upon Hydroxypropyl Cyclodextrins and Soft Hydrogel Contact Lenses for the Delivery of Therapeutic Doses of Econazole to the Cornea, In Vitro" Pharmaceutics 14, no. 8: 1631. https://doi.org/10.3390/pharmaceutics14081631
APA StyleWong, A., Fallon, M., Celiksoy, V., Ferla, S., Varricchio, C., Whitaker, D., Quantock, A. J., & Heard, C. M. (2022). A Composite System Based upon Hydroxypropyl Cyclodextrins and Soft Hydrogel Contact Lenses for the Delivery of Therapeutic Doses of Econazole to the Cornea, In Vitro. Pharmaceutics, 14(8), 1631. https://doi.org/10.3390/pharmaceutics14081631