
Formulation of a Gastroretentive In Situ Oral Gel Containing Metformin HCl Based on DoE


Abstract
:1. Introduction
2. Materials and Method
2.1. Materials
2.2. Methods
2.2.1. Preparation of Met HCl In Situ Oral Gel
2.2.2. In Vitro Dissolution Test of Met HCl In Situ Oral Gel
2.2.3. Floating Test of Met HCl In Situ Oral Gel
2.2.4. Physicochemical Characterization of Met HCl In Situ Oral Gel
2.2.5. Design of Experiments
3. Results and Discussion
3.1. Met HCl In Situ Oral Gel Formulation Containing Sod ALG and Calcium Carbonate: Formulation E1
3.1.1. Dissolution Study of Formulation E1
3.1.2. Floating Study of Formulation E1
3.1.3. Physicochemical Characteristics of Formulation E1
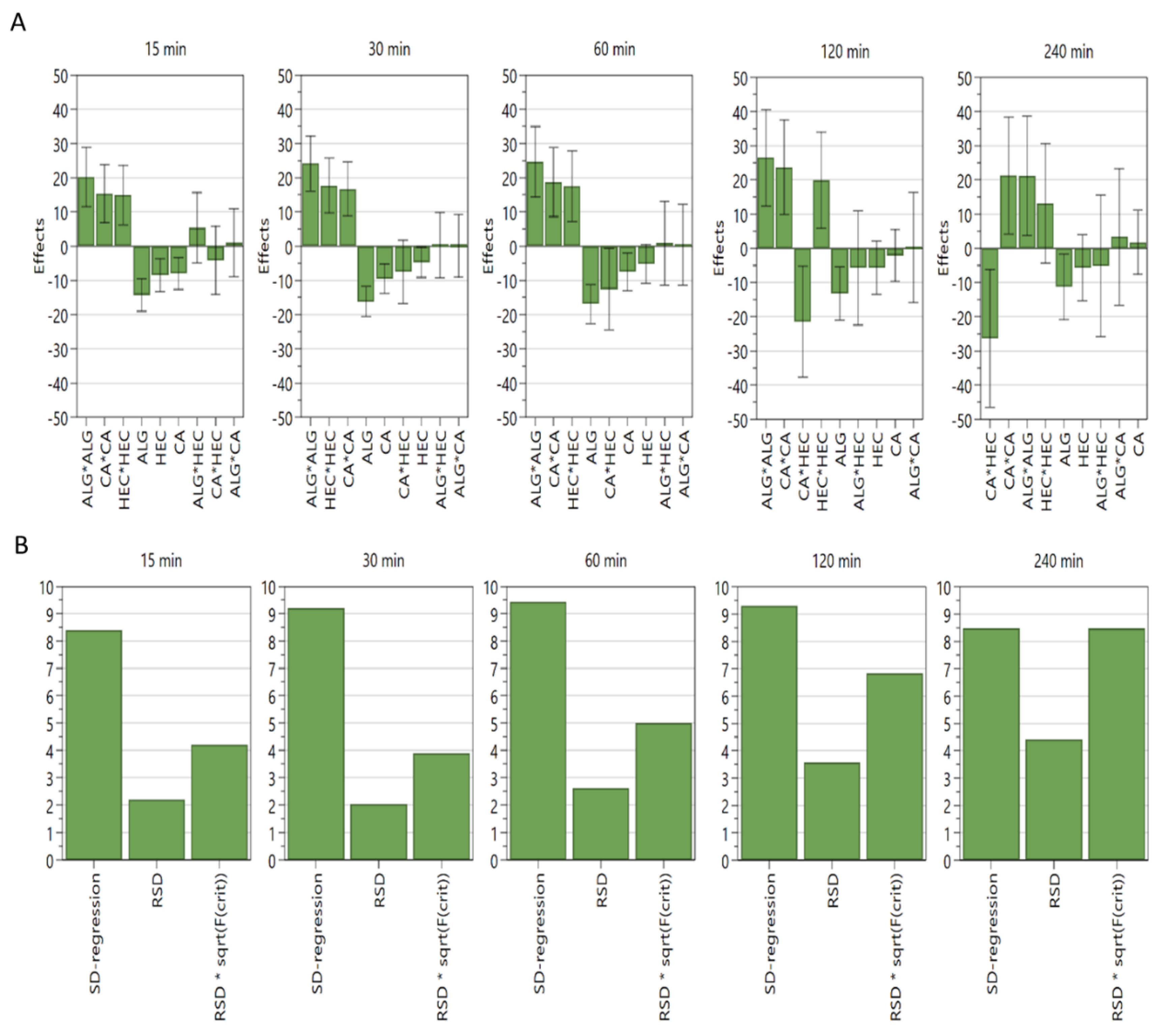
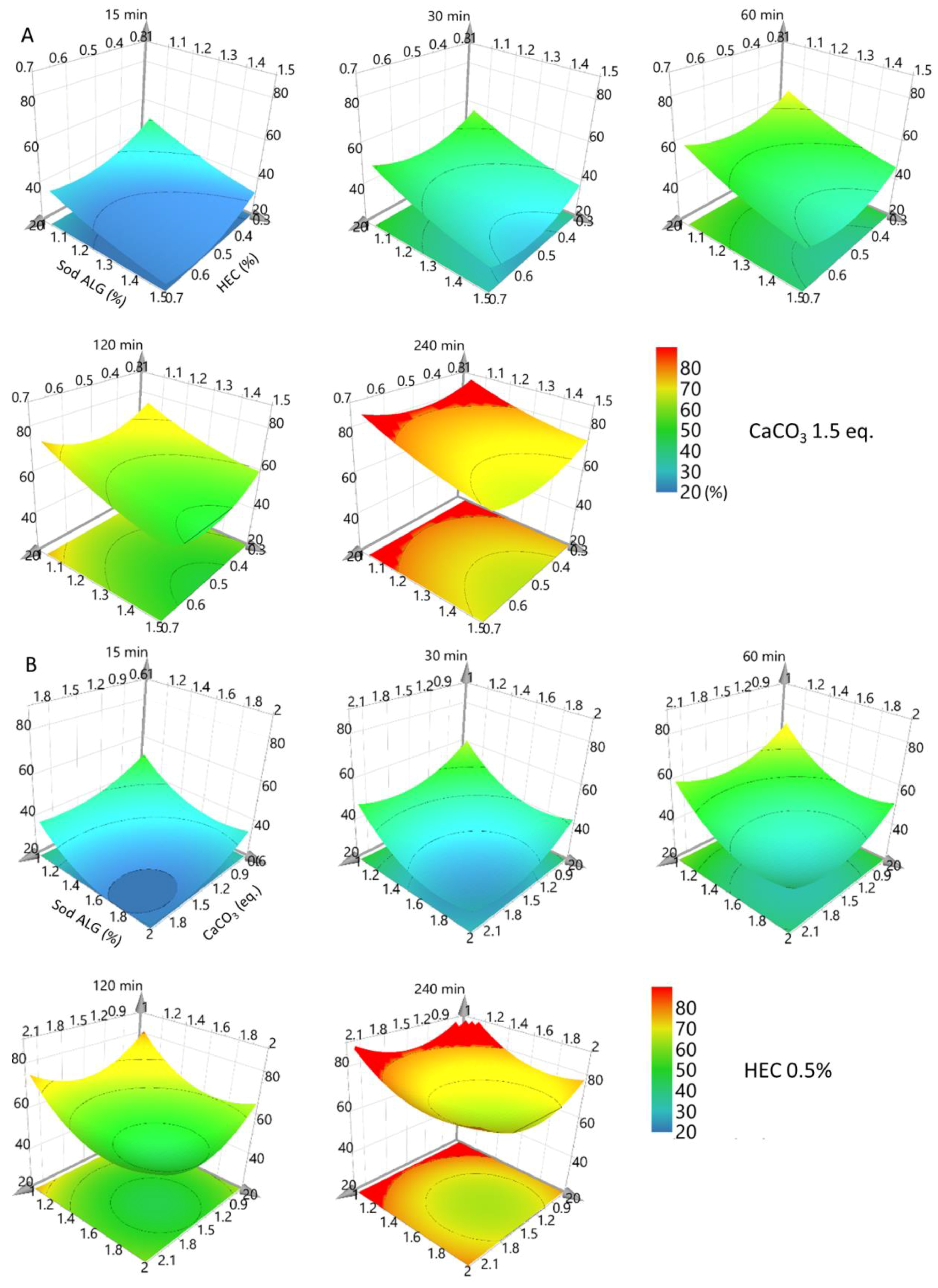
3.2. Met HCl In Situ Oral Gel Formulation Containing Sod ALG, Calcium Carbonate, and HEC: Formulation E2
3.2.1. Dissolution Study of Formulation E2
3.2.2. Floating Study of Formulation E2
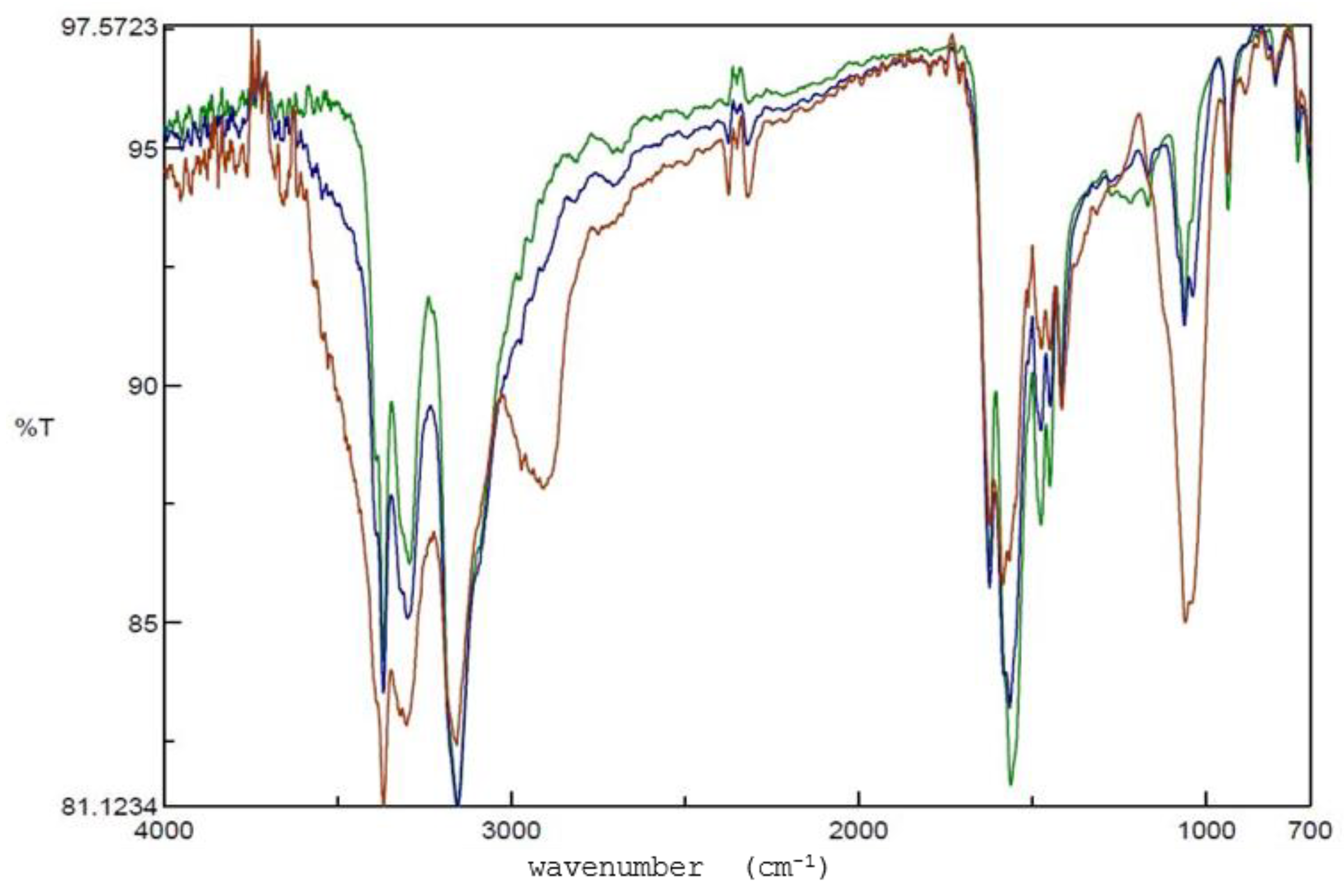
3.2.3. Physicochemical Characteristics of Formulation E2
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brusewitz, C.; Schendler, A.; Funke, A.; Wagner, T.; Lipp, R. Novel poloxamer-based nanoemulsions to enhance the intestinal absorption of active compounds. Int. J. Pharm. 2007, 329, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Bishnoi, R.S.; Shukla, A.K.; Jain, C.P. Techniques for Formulation of Nanoemulsion Drug Delivery System: A Review. Prev. Nutr. Food Sci. 2019, 24, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, J.; Siddiqui, H.H.; Badruddeen; Fareed, S.; Aqil, M. Nanomulsion as a carrier for efficient delivery of metformin. Curr. Drug Deliv. 2014, 11, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.H.; Du, Z.; Wang, G.N.; Chan, H.M.; Chang, Q.; Lai, L.C.; Chow, A.H.; Zheng, Y. Spray freeze drying with polyvinylpyrrolidone and sodium caprate for improved dissolution and oral bioavailability of oleanolic acid, a BCS Class IV compound. Int. J. Pharm. 2011, 404, 148–158. [Google Scholar] [CrossRef]
- Yadava, S. Formulation of metformin hydrochloride nanoparticles by using spray drying technique and in-vitro evaluation of sustained release with 32-level factorial design approach. Dry. Technol. 2016, 34, 916. [Google Scholar] [CrossRef]
- Pabla, D.; Akhlaghi, F.; Zia, H. Intestinal permeability enhancement of levothyroxine sodium by straight chain fatty acids studied in MDCK epithelial cell line. Eur. J. Pharm. Sci. 2010, 40, 466–472. [Google Scholar] [CrossRef]
- Kang, J.H.; Chun, M.H.; Cho, M.S.; Kwon, Y.B.; Choi, J.C.; Kim, D.W.; Park, C.W.; Park, E.S. Preparation and characterization of metformin hydrochloride controlled-release tablet using fatty acid coated granules. Drug Dev. Ind. Pharm. 2020, 46, 852–860. [Google Scholar] [CrossRef]
- Chitneni, M.; Peh, K.K.; Darwis, D.; Abdulkarim, M.; Abdullah, G.Z.; Qureshi, M.J. Intestinal permeability studies of sulpiride incorporated into self-microemulsifying drug delivery system (SMEDDS). Pak. J. Pharm. Sci. 2011, 24, 113–121. [Google Scholar]
- Oth, M.; Franz, M.; Timmermans, J.; Moes, A. The bilayer floating capsule: A stomach-directed drug delivery system for misoprostol. Pharm. Res. 1992, 9, 298–302. [Google Scholar] [CrossRef]
- Fabregas, J.L.; Claramunt, J.; Cucala, J.; Pous, R.; Siles, A. “In-Vitro” Testing of an Antacid Formulation with Prolonged Gastric Residence Time (Almagate Flot-Coat®). Drug Dev. Ind. Pharm. 1994, 20, 1199–1212. [Google Scholar] [CrossRef]
- Erni, W.; Held, K. The hydrodynamically balanced system: A novel principle of controlled drug release. Eur. Neurol. 1987, 27, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.; Stepensky, D.; Lavy, E.; Eyal, S.; Klausner, E.; Friedman, M. Pharmacokinetic and pharmacodynamic aspects of gastroretentive dosage forms. Int. J. Pharm. 2004, 277, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Graham, G.G.; Punt, J.; Arora, M.; Day, R.O.; Doogue, M.P.; Duong, J.K.; Furlong, T.J.; Greenfield, J.R.; Greenup, L.C.; Kirkpatrick, C.M.; et al. Clinical pharmacokinetics of metformin. Clin. Pharm. 2011, 50, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Menon, A.; Ritschel, W.A.; Sakr, A. Development and evaluation of a monolithic floating dosage form for furosemide. J. Pharm. Sci. 1994, 83, 239–245. [Google Scholar] [CrossRef]
- Ozdemir, N.; Ordu, S.; Ozkan, Y. Studies of floating dosage forms of furosemide: In vitro and in vivo evaluations of bilayer tablet formulations. Drug. Dev. Ind. Pharm. 2000, 26, 857–866. [Google Scholar] [CrossRef]
- Levy, G.; Jusko, W.J. Factors affecting the absorption of riboflavin in man. J. Pharm. Sci. 1966, 55, 285–289. [Google Scholar] [CrossRef]
- Matharu, R.S.; Sanghavi, N.M. Novel drug delivery system for captopril. Drug Dev. Ind. Pharm. 1992, 18, 1567–1574. [Google Scholar] [CrossRef]
- Sheth, P.R.; Tossounian, J. The Hydrodynamically Balanced System (Hbs™): A Novel Drug Delivery System for Oral Use. Drug Dev. Ind. Pharm. 1984, 10, 313–339. [Google Scholar] [CrossRef]
- Chen, G.L.; Hao, W.H. In vitro performance of floating sustained-release capsule of verapamil. Drug Dev. Ind. Pharm. 1998, 24, 1067–1072. [Google Scholar] [CrossRef]
- Streubel, A.; Siepmann, J.; Bodmeier, R. Gastroretentive drug delivery systems. Expert Opin. Drug Deliv. 2006, 3, 217–233. [Google Scholar] [CrossRef]
- Hauptstein, S.; Muller, C.; Dunnhaupt, S.; Laffleur, F.; Bernkop-Schnurch, A. Preactivated thiomers: Evaluation of gastroretentive minitablets. Int. J. Pharm. 2013, 456, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, J.; Gao, Y.; Zhu, J. Preparation and evaluation of glyceryl monooleate-coated hollow-bioadhesive microspheres for gastroretentive drug delivery. Int. J. Pharm. 2011, 413, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Narang, N. An updated review on: Floating drug delivery system (FDDS). Int. J. Appl. Pharm. 2011, 3, 1–7. [Google Scholar]
- Arnold, J.; Hunkeler, D. Gastro retention using polymer cocoons. Artif. Cells Nanomed. Biotechnol. 2015, 43, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Klausner, E.A.; Lavy, E.; Friedman, M.; Hoffman, A. Expandable gastroretentive dosage forms. J. Control. Release 2003, 90, 143–162. [Google Scholar] [CrossRef]
- Matharu, A.S.; Motto, M.G.; Patel, M.R.; Simonelli, A.P.; Dave, R.H. Evaluation of hydroxypropyl methylcellulose matrix systems as swellable gastro-retentive drug delivery systems (GRDDS). J. Pharm. Sci. 2011, 100, 150–163. [Google Scholar] [CrossRef]
- Vishal, P.; Jamdhade, A. Novel Strategy in Controlled Gastroretentive Drug Delivery: In-Situ Floating Gel. Int. J. Drug Deliv. 2014, 6, 230–243. [Google Scholar]
- Kim, B.; Byun, Y.; Lee, E.H. DoE-Based Design of a Simple but Efficient Preparation Method for a Non-Effervescent Gastro-Retentive Floating Tablet Containing Metformin HCl. Pharmaceutics 2021, 13, 1225. [Google Scholar] [CrossRef]
- Patel, D.M.; Patel, D.K.; Patel, C.N. Formulation and evaluation of floating oral in situ gelling system of amoxicillin. ISRN Pharm. 2011, 2011, 276250. [Google Scholar] [CrossRef]
- Zhao, J.; Sun, C.; Li, H.; Dong, X.; Zhang, X. Studies on the physicochemical properties, gelling behavior and drug release performance of agar/kappa-carrageenan mixed hydrogels. Int. J. Biol. Macromol. 2020, 154, 878–887. [Google Scholar] [CrossRef]
- Sharma, H.; Lahkar, S.; Nath, L. Extraction, Characterisation and Compatibility Study of Polysaccharides from Dillenia indica and Abelmoschus esculentus with Metformin Hydrochloride for Development of Drug Delivery System. Int. J. PharmTech Res. 2013, 5, 974–4304. [Google Scholar]
- Naveed, D.S.; Shafiq, A.; Khan, M.; Jamal, M.; Zafar, H.; Hashim, H.; Urooj, L. Diabetes & Metabolism Degradation Study of Available Brands of Metformin in Karachi Using UV Spectrophotometer. J. Diabetes Metab. 2014, 5, 1000328. [Google Scholar] [CrossRef]
- Alemón-Medina, R.; Coria-Jiménez, R.; Rivera, L.; Ramirez-Mendiola, B.; Garcia-Alvarez, R.; Juárez, H.; Chavez-Pacheco, J. Physicochemical and Microbiological Stabilities of a Sweetened and Calorie-Free Metformin Extemporaneous Formulation for Pediatrics. Lat. Am. J. Pharm. 2012, 31, 1253–1260. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Batch No. | Met HCl | Sod ALG | Calcium | Sodium | Water | Total |
|---|---|---|---|---|---|---|
| Carbonate | Bicarbonate | |||||
| E1-01 | 500 | 125 | 34 | 125 | 11,716 | 12,500 |
| E1-02 | 500 | 125 | 51 | 125 | 11,699 | 12,500 |
| E1-03 | 500 | 125 | 68 | 125 | 11,683 | 12,500 |
| E1-04 | 500 | 156 | 41 | 125 | 11,678 | 12,500 |
| E1-05 | 500 | 156 | 63 | 125 | 11,656 | 12,500 |
| E1-06 | 500 | 156 | 83 | 125 | 11,636 | 12,500 |
| E1-07 | 500 | 188 | 50 | 125 | 11,638 | 12,500 |
| E1-08 | 500 | 188 | 75 | 125 | 11,613 | 12,500 |
| E1-09 | 500 | 188 | 100 | 125 | 11,588 | 12,500 |
| Batch No. | Met HCl | Sod ALG | HEC | Calcium | Sodium | Water | Total |
|---|---|---|---|---|---|---|---|
| Carbonate | Bicarbonate | ||||||
| E2-01 | 500 | 125 | 38 | 33 | 125 | 11,679 | 12,500 |
| E2-02 | 500 | 188 | 38 | 50 | 125 | 11,600 | 12,500 |
| E2-03 | 500 | 125 | 63 | 33 | 125 | 11,654 | 12,500 |
| E2-04 | 500 | 188 | 63 | 50 | 125 | 11,575 | 12,500 |
| E2-05 | 500 | 125 | 38 | 67 | 125 | 11,646 | 12,500 |
| E2-06 | 500 | 188 | 38 | 100 | 125 | 11,550 | 12,500 |
| E2-07 | 500 | 125 | 63 | 67 | 125 | 11,621 | 12,500 |
| E2-08 | 500 | 188 | 63 | 100 | 125 | 11,525 | 12,500 |
| E2-09 | 500 | 104 | 50 | 41 | 125 | 11,680 | 12,500 |
| E2-10 | 500 | 209 | 50 | 84 | 125 | 11,533 | 12,500 |
| E2-11 | 500 | 156 | 29 | 63 | 125 | 11,627 | 12,500 |
| E2-12 | 500 | 156 | 71 | 63 | 125 | 11,585 | 12,500 |
| E2-13 | 500 | 156 | 50 | 26 | 125 | 11,643 | 12,500 |
| E2-14 | 500 | 156 | 50 | 93 | 125 | 11,576 | 12,500 |
| E2-15 | 500 | 156 | 50 | 63 | 125 | 11,606 | 12,500 |
| E2-16 | 500 | 156 | 50 | 63 | 125 | 11,606 | 12,500 |
| E2-17 | 500 | 156 | 50 | 63 | 125 | 11,606 | 12,500 |
| Batch No. | Coded Form | % Drug Released | |||||
|---|---|---|---|---|---|---|---|
| X1 | X2 | Y1 | Y2 | Y3 | Y4 | Y5 | |
| 15 min | 30 min | 60 min | 120 min | 240 min | |||
| E1-01 | −1 | −1 | 88.5 | 88.1 | 90.1 | 92.3 | 93.4 |
| E1-02 | −1 | 0 | 89.9 | 90.0 | 91.2 | 92.6 | 93.1 |
| E1-03 | −1 | 1 | 82.6 | 84.5 | 87.3 | 85.9 | 87.9 |
| E1-04 | 0 | −1 | 69.9 | 75.9 | 78.6 | 82.7 | 87.0 |
| E1-05 | 0 | 0 | 56.8 | 59.9 | 64.4 | 70.5 | 80.4 |
| E1-06 | 0 | 1 | 51.8 | 53.6 | 60.8 | 68.6 | 75.3 |
| E1-07 | 1 | −1 | 48.7 | 56.8 | 63.2 | 68.3 | 74.6 |
| E1-08 | 1 | 0 | 40.0 | 43.6 | 51.6 | 60.1 | 71.7 |
| E1-09 | 1 | 1 | 41.9 | 46.9 | 54.8 | 63.3 | 75.4 |
| coded values | actual values | ||||||
| Sod ALG (%) | CaCO3 (eq.) | ||||||
| −1 | 1.00 | 1.0 | |||||
| 0 | 1.25 | 1.5 | |||||
| 1 | 1.50 | 2.0 | |||||
| Batch No. | Coded Form | % Drug Released | ||||||
|---|---|---|---|---|---|---|---|---|
| X1 | X2 | X3 | Y1 | Y2 | Y3 | Y4 | Y5 | |
| Sod ALG | HEC | CaCO3 | 15 min | 30 min | 60 min | 120 min | 240 min | |
| E2-01 | −1 | −1 | −1 | 41.6 | 45.8 | 55.0 | 63.7 | 77.0 |
| E2-02 | 1 | −1 | −1 | 27.0 | 33.6 | 43.2 | 56.2 | 69.1 |
| E2-03 | −1 | 1 | −1 | 33.2 | 44.2 | 54.8 | 68.0 | 82.7 |
| E2-04 | 1 | 1 | −1 | 28.8 | 36.5 | 45.2 | 59.7 | 75.6 |
| E2-05 | −1 | −1 | 1 | 34.2 | 39.8 | 52.4 | 67.5 | 84.6 |
| E2-06 | 1 | −1 | 1 | 26.6 | 31.8 | 42.3 | 63.2 | 83.3 |
| E2-07 | −1 | 1 | 1 | 29.2 | 37.1 | 44.8 | 59.7 | 75.9 |
| E2-08 | 1 | 1 | 1 | 18.9 | 24.9 | 33.7 | 48.2 | 66.6 |
| E2-09 | −1.682 | 0 | 0 | 35.7 | 44.3 | 53.1 | 64.3 | 79.3 |
| E2-10 | 1.682 | 0 | 0 | 24.3 | 30.2 | 38.9 | 52.4 | 68.5 |
| E2-11 | 0 | −1.682 | 0 | 31.4 | 36.8 | 44.1 | 57.2 | 72.5 |
| E2-12 | 0 | 1.682 | 0 | 22.8 | 30.4 | 40.0 | 52.0 | 66.0 |
| E2-13 | 0 | 0 | −1.682 | 33.0 | 39.5 | 47.2 | 59.1 | 75.3 |
| E2-14 | 0 | 0 | 1.682 | 24.7 | 30.3 | 41.7 | 56.3 | 72.6 |
| E2-15 | 0 | 0 | 0 | 19.2 | 24.1 | 33.2 | 45.2 | 64.6 |
| E2-16 | 0 | 0 | 0 | 20.4 | 27.6 | 37.4 | 52.3 | 72.1 |
| E2-17 | 0 | 0 | 0 | 21.0 | 24.7 | 32.5 | 43.0 | 59.7 |
| coded values | actual values | |||||||
| (%) | (%) | (eq.) | ||||||
| −1.682 | 1.04 | 0.29 | 0.63 | |||||
| −1 | 1.25 | 0.38 | 1 | |||||
| 0 | 1.56 | 0.50 | 1.5 | |||||
| 1 | 1.88 | 0.63 | 2 | |||||
| 1.682 | 2.09 | 0.71 | 2.25 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.H.; Song, S.H.; Joo, S.H.; Park, G.H.; Weon, K.-Y. Formulation of a Gastroretentive In Situ Oral Gel Containing Metformin HCl Based on DoE. Pharmaceutics 2022, 14, 1777. https://doi.org/10.3390/pharmaceutics14091777
Kim JH, Song SH, Joo SH, Park GH, Weon K-Y. Formulation of a Gastroretentive In Situ Oral Gel Containing Metformin HCl Based on DoE. Pharmaceutics. 2022; 14(9):1777. https://doi.org/10.3390/pharmaceutics14091777
Chicago/Turabian StyleKim, Jong Hee, Seung Hyun Song, Sang Hoon Joo, Gyu Hwan Park, and Kwon-Yeon Weon. 2022. "Formulation of a Gastroretentive In Situ Oral Gel Containing Metformin HCl Based on DoE" Pharmaceutics 14, no. 9: 1777. https://doi.org/10.3390/pharmaceutics14091777
APA StyleKim, J. H., Song, S. H., Joo, S. H., Park, G. H., & Weon, K. -Y. (2022). Formulation of a Gastroretentive In Situ Oral Gel Containing Metformin HCl Based on DoE. Pharmaceutics, 14(9), 1777. https://doi.org/10.3390/pharmaceutics14091777