


Microneedle-Mediated Transdermal Delivery of Biopharmaceuticals


Abstract
:
1. Introduction
1.1. Skin Structure
1.2. Transdermal Drug Delivery
1.3. Microneedle Technology


1.4. Introduction of Biopharmaceuticals
1.5. Current Status of Biopharmaceuticals
1.6. Conventional Parenteral Administration
1.7. Transdermal Delivery of Biopharmaceuticals
1.8. Microneedles for Biopharmaceutical Delivery
1.9. Stability of Biopharmaceuticals in Microneedles
2. Microneedle Types for Biopharmaceutical Delivery
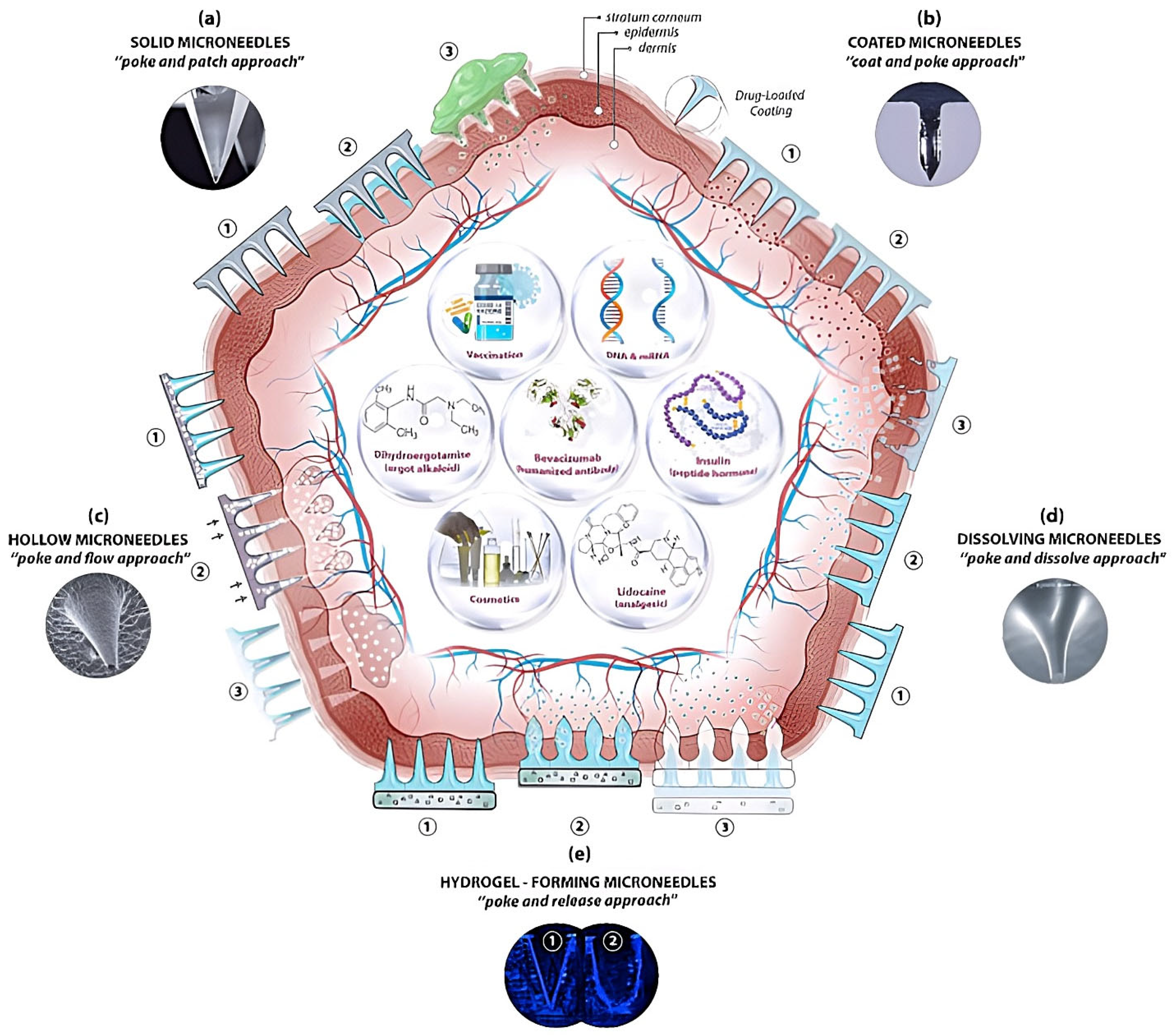
2.1. Solid Microneedles
2.2. Coated Microneedles
2.3. Hollow Microneedles
2.4. Dissolving Microneedles
2.5. Swelling Microneedles
3. Clinical Trials of Microneedles for Biopharmaceutical Delivery
4. Safety and Acceptability of Microneedles
4.1. Safety of Microneedles
4.2. Acceptability of Microneedles
5. Manufacturing and Regulatory Issues
5.1. Manufacturing Issues
5.2. Regulatory Issues
6. Conclusions
7. Future of Microneedles
Funding
Conflicts of Interest
Abbreviations
| bFGF | Basic fibroblast growth factor |
| BSA | Bovine serum albumin |
| CDC | Centers for Disease Control and Prevention |
| CMC | Chemistry, manufacturing, and controls |
| FDA | Food and Drug Administration |
| FITC | Fluorescein isothiocyanate |
| hMTS | Hollow microstructured transdermal system |
| ICH | International Conference on Harmonization |
| IgG | Immunoglobulin G |
| MN | Microneedle |
| MW | Molecular weight |
| PLA | Polylactic acid |
| PLGA | Poly Lactic-co-Glycolic Acid |
| PTH | Parathyroid hormone |
| PVA | Polyvinyl alcohol |
| rhGH | Recombinant human growth hormone |
| sMTS | Solid microstructured transdermal system |
| UV | Ultraviolet |
| VAS | Visual analog scale |
References
- Boer, M.; Duchnik, E.; Maleszka, R.; Marchlewicz, M. Structural and Biophysical Characteristics of Human Skin in Maintaining Proper Epidermal Barrier Function. Adv. Dermatol. Allergol. 2016, 33, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kolarsick, P.A.J.; Kolarsick, M.A.; Goodwin, C. Anatomy and Physiology of the Skin. J. Dermatol. Nurses Assoc. 2011, 3, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Roberts, M.S.; Cheruvu, H.S.; Mangion, S.E.; Alinaghi, A.; Benson, H.A.E.; Mohammed, Y.; Holmes, A.; van der Hoek, J.; Pastore, M.; Grice, J.E. Topical Drug Delivery: History, Percutaneous Absorption, and Product Development. Adv. Drug Deliv. Rev. 2021, 177, 113929. [Google Scholar] [CrossRef] [PubMed]
- Ingrole, R.S.; Azizoglu, E.; Dul, M.; Birchall, J.C.; Gill, H.S.; Prausnitz, M.R. Trends of Microneedle Technology in the Scientific Literature, Patents, Clinical Trials and Internet Activity. Biomaterials 2021, 267, 120491. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Alle, M.; Chakraborty, C.; Kim, J.-C. Strategies for Transdermal Drug Delivery against Bone Disorders: A Preclinical and Clinical Update. J. Control. Release 2021, 336, 375–395. [Google Scholar] [CrossRef] [PubMed]
- Zaid Alkilani, A.; McCrudden, M.T.; Donnelly, R.F. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the Stratum Corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, R.F.; Singh, T.R.R.; Larrañeta, E.; McCrudden, M.T. Microneedles for Drug and Vaccine Delivery and Patient Monitoring; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Ramadon, D.; McCrudden, M.T.C.; Courtenay, A.J.; Donnelly, R.F. Enhancement Strategies for Transdermal Drug Delivery Systems: Current Trends and Applications. Drug Deliv. Transl. Res. 2022, 12, 758–791. [Google Scholar] [CrossRef]
- Bajaj, S.; Whiteman, A.; Brandner, B. Transdermal Drug Delivery in Pain Management. Contin. Educ. Anaesth. Crit. Care Pain 2011, 11, 39–43. [Google Scholar] [CrossRef] [Green Version]
- Frampton, J.E. Rotigotine Transdermal Patch: A Review in Parkinson’s Disease. CNS Drugs 2019, 33, 707–718. [Google Scholar] [CrossRef]
- Pastore, M.N.; Kalia, Y.N.; Horstmann, M.; Roberts, M.S. Transdermal Patches: History, Development and Pharmacology. Br. J. Pharmacol. 2015, 172, 2179–2209. [Google Scholar] [CrossRef]
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. Available online: https://www.accessdata.fda.gov/ (accessed on 25 December 2022).
- Haque, T.; Talukder, M.M.U. Chemical Enhancer: A Simplistic Way to Modulate Barrier Function of the Stratum Corneum. Adv. Pharm. Bull. 2018, 8, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Alexander, A.; Dwivedi, S.; Giri, T.K.; Saraf, S.; Saraf, S.; Tripathi, D.K. Approaches for Breaking the Barriers of Drug Permeation through Transdermal Drug Delivery. J. Control. Release 2012, 164, 26–40. [Google Scholar] [CrossRef]
- Gazerani, P.; Arendt-Nielsen, L. Cutaneous Vasomotor Reactions in Response to Controlled Heat Applied on Various Body Regions of Healthy Humans: Evaluation of Time Course and Application Parameters. Int. J. Physiol. Pathophysiol. Pharmacol. 2011, 3, 202–209. [Google Scholar]
- Singh, I.; Morris, A.P. Performance of Transdermal Therapeutic Systems: Effects of Biological Factors. Int. J. Pharm. Investig. 2011, 1, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Bhoyar, N.; Giri, T.K.; Tripathi, D.K.; Alexander, A. Others Recent Advances in Novel Drug Delivery System through Gels: Review. J. Pharm. Allied Health Sci. 2012, 2, 21. [Google Scholar]
- Sachdeva, V.; K Banga, A. Microneedles and Their Applications. Recent Pat. Drug Deliv. Formul. 2011, 5, 95–132. [Google Scholar] [CrossRef]
- Akhtar, N.; Singh, V.; Yusuf, M.; Khan, R.A. Non-Invasive Drug Delivery Technology: Development and Current Status of Transdermal Drug Delivery Devices, Techniques and Biomedical Applications. Biomed. Eng. 2020, 65, 243–272. [Google Scholar] [CrossRef] [Green Version]
- Pires, L.R.; Vinayakumar, K.B.; Turos, M.; Miguel, V.; Gaspar, J. A Perspective on Microneedle-Based Drug Delivery and Diagnostics in Paediatrics. J. Pers. Med. 2019, 9, 49. [Google Scholar] [CrossRef] [Green Version]
- Ruby, P.K.; Pathak, S.M.; Aggarwal, D. Critical Attributes of Transdermal Drug Delivery System (TDDS)—A Generic Product Development Review. Drug Dev. Ind. Pharm. 2014, 40, 1421–1428. [Google Scholar] [CrossRef]
- Brogden, N.K.; Milewski, M.; Ghosh, P.; Hardi, L.; Crofford, L.J.; Stinchcomb, A.L. Diclofenac Delays Micropore Closure Following Microneedle Treatment in Human Subjects. J. Control. Release 2012, 163, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Kalluri, H.; Banga, A.K. Formation and Closure of Microchannels in Skin Following Microporation. Pharm. Res. 2011, 28, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Zaid Alkilani, A.; Nimrawi, S.; Al-Nemrawi, N.K.; Nasereddin, J. Microneedle-Assisted Transdermal Delivery of Amlodipine Besylate Loaded Nanoparticles. Drug Dev. Ind. Pharm. 2022, 48, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, Y.; Holmes, A.; Kwok, P.C.L.; Kumeria, T.; Namjoshi, S.; Imran, M.; Matteucci, L.; Ali, M.; Tai, W.; Benson, H.A. Advances and Future Perspectives in Epithelial Drug Delivery. Adv. Drug Deliv. Rev. 2022, 186. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Cheng, L.; Wu, Q.; Li, Y.; Ran, L.; Wang, W.; Huang, K.; Zhu, R.; Xue, S.; Zhou, C.; et al. A Modified Hyaluronic Acid-Based Dissolving Microneedle Loaded With Daphnetin Improved the Treatment of Psoriasis. Front. Bioeng. Biotechnol. 2022, 10, 900274. [Google Scholar] [CrossRef]
- Makvandi, P.; Jamaledin, R.; Chen, G.; Baghbantaraghdari, Z.; Zare, E.N.; Di Natale, C.; Onesto, V.; Vecchione, R.; Lee, J.; Tay, F.R.; et al. Stimuli-Responsive Transdermal Microneedle Patches. Mater. Today 2021, 47, 206–222. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, H.; Wang, Z.; Shiu, C.Y.A.; Gu, Z. Microneedle Array Patches Integrated with Nanoparticles for Therapy and Diagnosis. Small Struct. 2021, 2, 2000097. [Google Scholar] [CrossRef]
- Makvandi, P.; Kirkby, M.; Hutton, A.R.; Shabani, M.; Yiu, C.K.; Baghbantaraghdari, Z.; Jamaledin, R.; Carlotti, M.; Mazzolai, B.; Mattoli, V. Engineering Microneedle Patches for Improved Penetration: Analysis, Skin Models and Factors Affecting Needle Insertion. Nano-Micro Lett. 2021, 13, 1–41. [Google Scholar] [CrossRef]
- Yang, Y.; Song, W.; Wang, N.; Ren, Y.; Liu, H. Tip-Concentrated Microneedle Patch Delivering Everolimus for Therapy of Multiple Sclerosis. Biomater. Adv. 2022, 135, 212729. [Google Scholar] [CrossRef]
- Donnelly, R.F.; Raj Singh, T.R.; Woolfson, A.D. Microneedle-Based Drug Delivery Systems: Microfabrication, Drug Delivery, and Safety. Drug Deliv. 2010, 17, 187–207. [Google Scholar] [CrossRef] [Green Version]
- van der Maaden, K.; Jiskoot, W.; Bouwstra, J. Microneedle Technologies for (Trans)Dermal Drug and Vaccine Delivery. J. Control. Release 2012, 161, 645–655. [Google Scholar] [CrossRef]
- Tuan-Mahmood, T.-M.; McCrudden, M.T.; Torrisi, B.M.; McAlister, E.; Garland, M.J.; Singh, T.R.R.; Donnelly, R.F. Microneedles for Intradermal and Transdermal Drug Delivery. Eur. J. Pharm. Sci. 2013, 50, 623–637. [Google Scholar] [CrossRef] [Green Version]
- Pierre, M.B.R.; Rossetti, F.C. Microneedle-Based Drug Delivery Systems for Transdermal Route. Curr. Drug Targets 2014, 15, 281–291. [Google Scholar] [CrossRef]
- Yadav, P.R.; Han, T.; Olatunji, O.; Pattanayek, S.K.; Das, D.B. Mathematical Modelling, Simulation and Optimisation of Microneedles for Transdermal Drug Delivery: Trends and Progress. Pharmaceutics 2020, 12, 693. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Nguyen, T.T.D.; Van Vo, G. Advances of Microneedles in Hormone Delivery. Biomed. Pharmacother. 2022, 145, 112393. [Google Scholar] [CrossRef]
- Ali, M.; Namjoshi, S.; Benson, H.A.E.; Kumeria, T.; Mohammed, Y. Skin Biomechanics: Breaking the Dermal Barriers with Microneedles. Nano TransMed 2022, 1, e9130002. [Google Scholar] [CrossRef]
- Kearney, M.-C.; Caffarel-Salvador, E.; Fallows, S.J.; McCarthy, H.O.; Donnelly, R.F. Microneedle-Mediated Delivery of Donepezil: Potential for Improved Treatment Options in Alzheimer’s Disease. Eur. J. Pharm. Biopharm. 2016, 103, 43–50. [Google Scholar] [CrossRef] [Green Version]
- McCrudden, M.T.C.; Alkilani, A.Z.; McCrudden, C.M.; McAlister, E.; McCarthy, H.O.; Woolfson, A.D.; Donnelly, R.F. Design and Physicochemical Characterisation of Novel Dissolving Polymeric Microneedle Arrays for Transdermal Delivery of High Dose, Low Molecular Weight Drugs. J. Control. Release 2014, 180, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Wang, L.; Yu, H.; Li, C.; Feng, J.; Haq, F.; Khan, A.; Khan, R.U. Preparation, Properties and Challenges of the Microneedles-Based Insulin Delivery System. J. Control. Release 2018, 288, 173–188. [Google Scholar] [CrossRef]
- Liu, T.; Chen, M.; Fu, J.; Sun, Y.; Lu, C.; Quan, G.; Pan, X.; Wu, C. Recent Advances in Microneedles-Mediated Transdermal Delivery of Protein and Peptide Drugs. Acta Pharm. Sin. B 2021, 11, 2326–2343. [Google Scholar] [CrossRef]
- Stinson, J.A.; Boopathy, A.V.; Cieslewicz, B.M.; Zhang, Y.; Hartman, N.W.; Miller, D.P.; Dirckx, M.; Hurst, B.L.; Tarbet, E.B.; Kluge, J.A. Enhancing Influenza Vaccine Immunogenicity and Efficacy through Infection Mimicry Using Silk Microneedles. Vaccine 2021, 39, 5410–5421. [Google Scholar] [CrossRef]
- Yin, Y.; Su, W.; Zhang, J.; Huang, W.; Li, X.; Ma, H.; Tan, M.; Song, H.; Cao, G.; Yu, S. Separable Microneedle Patch to Protect and Deliver DNA Nanovaccines against COVID-19. ACS Nano 2021, 15, 14347–14359. [Google Scholar] [CrossRef]
- Choi, S.Y.; Kwon, H.J.; Ahn, G.R.; Ko, E.J.; Yoo, K.H.; Kim, B.J.; Lee, C.; Kim, D. Hyaluronic Acid Microneedle Patch for the Improvement of Crow’s Feet Wrinkles. Dermatol. Ther. 2017, 30, e12546. [Google Scholar] [CrossRef]
- Mohammed, Y.H.; Yamada, M.; Lin, L.L.; Grice, J.E.; Roberts, M.S.; Raphael, A.P.; Benson, H.A.E.; Prow, T.W. Microneedle Enhanced Delivery of Cosmeceutically Relevant Peptides in Human Skin. PLoS ONE 2014, 9, e101956. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Park, J.; Chu, G.S.; Kim, K.S.; Sung, J.H.; Kim, B. Transdermal Delivery of Cosmetic Ingredients Using Dissolving Polymer Microneedle Arrays. Biotechnol. Bioprocess Eng. 2015, 20, 543–549. [Google Scholar] [CrossRef]
- Niu, L.; Chu, L.Y.; Burton, S.A.; Hansen, K.J.; Panyam, J. Intradermal Delivery of Vaccine Nanoparticles Using Hollow Microneedle Array Generates Enhanced and Balanced Immune Response. J. Control. Release 2019, 294, 268–278. [Google Scholar] [CrossRef]
- Peng, K.; Vora, L.K.; Tekko, I.A.; Permana, A.D.; Domínguez-Robles, J.; Ramadon, D.; Chambers, P.; McCarthy, H.O.; Larrañeta, E.; Donnelly, R.F. Dissolving Microneedle Patches Loaded with Amphotericin B Microparticles for Localised and Sustained Intradermal Delivery: Potential for Enhanced Treatment of Cutaneous Fungal Infections. J. Control. Release 2021, 339, 361–380. [Google Scholar] [CrossRef]
- Zhang, D.; Das, D.B.; Rielly, C.D. An Experimental Study of Microneedle-Assisted Microparticle Delivery. J. Pharm. Sci. 2013, 102, 3632–3644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, G.A.; Picece, V.C.T.M.; Ou, B.S.; Luo, W.; Pulendran, B.; Appel, E.A. Designing Spatial and Temporal Control of Vaccine Responses. Nat. Rev. Mater. 2022, 7, 174–195. [Google Scholar] [CrossRef] [PubMed]
- Saha, I.; Rai, V.K. Hyaluronic Acid Based Microneedle Array: Recent Applications in Drug Delivery and Cosmetology. Carbohydr. Polym. 2021, 267, 118168. [Google Scholar] [CrossRef]
- Kuwentrai, C.; Yu, J.; Rong, L.; Zhang, B.-Z.; Hu, Y.-F.; Gong, H.-R.; Dou, Y.; Deng, J.; Huang, J.-D.; Xu, C. Intradermal Delivery of Receptor-Binding Domain of SARS-CoV-2 Spike Protein with Dissolvable Microneedles to Induce Humoral and Cellular Responses in Mice. Bioeng. Transl. Med. 2021, 6, e10202. [Google Scholar] [CrossRef]
- Ali, M.; Namjoshi, S.; Benson, H.A.; Mohammed, Y.; Kumeria, T. Dissolvable Polymer Microneedles for Drug Delivery and Diagnostics. J. Control. Release 2022, 347, 561–589. [Google Scholar] [CrossRef]
- Naveen, N.R.; Goudanavar, P.S.; Ramesh, B.; Kumar, G.K. Prospection of Fabrication Techniques and Material Selection of Microneedles for Transdermal Drug Delivery: An Update on Clinical Trials. Mater. Today Proc. 2022, 69, 187–192. [Google Scholar]
- Rajput, A.; Kulkarni, M.; Deshmukh, P.; Pingale, P.; Garkal, A.; Gandhi, S.; Butani, S. A Key Role by Polymers in Microneedle Technology: A New Era. Drug Dev. Ind. Pharm. 2022, 47, 1713–1732. [Google Scholar] [CrossRef]
- Dabholkar, N.; Gorantla, S.; Waghule, T.; Rapalli, V.K.; Kothuru, A.; Goel, S.; Singhvi, G. Biodegradable Microneedles Fabricated with Carbohydrates and Proteins: Revolutionary Approach for Transdermal Drug Delivery. Int. J. Biol. Macromol. 2021, 170, 602–621. [Google Scholar] [CrossRef]
- Zhou, P.; Zhao, S.; Huang, C.; Qu, Y.; Zhang, C. Bletilla Striata Polysaccharide Microneedle for Effective Transdermal Administration of Model Protein Antigen. Int. J. Biol. Macromol. 2022, 205, 511–519. [Google Scholar] [CrossRef]
- Damiri, F.; Kommineni, N.; Ebhodaghe, S.O.; Bulusu, R.; Jyothi, V.G.S.; Sayed, A.A.; Awaji, A.A.; Germoush, M.O.; Al-Malky, H.S.; Nasrullah, M.Z. Microneedle-Based Natural Polysaccharide for Drug Delivery Systems (DDS): Progress and Challenges. Pharmaceuticals 2022, 15, 190. [Google Scholar] [CrossRef]
- Dharadhar, S.; Majumdar, A.; Dhoble, S.; Patravale, V. Microneedles for Transdermal Drug Delivery: A Systematic Review. Drug Dev. Ind. Pharm. 2019, 45, 188–201. [Google Scholar] [CrossRef]
- Permana, A.D.; Anjani, Q.K.; Sartini; Utomo, E.; Volpe-Zanutto, F.; Paredes, A.J.; Evary, Y.M.; Mardikasari, S.A.; Pratama, M.R.; Tuany, I.N.; et al. Selective Delivery of Silver Nanoparticles for Improved Treatment of Biofilm Skin Infection Using Bacteria-Responsive Microparticles Loaded into Dissolving Microneedles. Mater. Sci. Eng. C 2021, 120, 111786. [Google Scholar] [CrossRef]
- Caudill, C.; Perry, J.L.; Iliadis, K.; Tessema, A.T.; Lee, B.J.; Mecham, B.S.; Tian, S.; DeSimone, J.M. Transdermal Vaccination via 3D-Printed Microneedles Induces Potent Humoral and Cellular Immunity. Proc. Natl. Acad. Sci. USA 2021, 118, e2102595118. [Google Scholar] [CrossRef]
- Economidou, S.N.; Pissinato Pere, C.P.; Okereke, M.; Douroumis, D. Optimisation of Design and Manufacturing Parameters of 3D Printed Solid Microneedles for Improved Strength, Sharpness, and Drug Delivery. Micromachines 2021, 12, 117. [Google Scholar] [CrossRef]
- Chen, Z.; Wu, H.; Zhao, S.; Chen, X.; Wei, T.; Peng, H.; Chen, Z. 3D-Printed Integrated Ultrasonic Microneedle Array for Rapid Transdermal Drug Delivery. Mol. Pharm. 2022, 19, 3314–3322. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.X.; Bozorg, B.D.; Kim, Y.; Wieber, A.; Birk, G.; Lubda, D.; Banga, A.K. Poly (Vinyl Alcohol) Microneedles: Fabrication, Characterization, and Application for Transdermal Drug Delivery of Doxorubicin. Eur. J. Pharm. Biopharm. 2018, 129, 88–103. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.X.; Banga, A.K. Delivery of Methotrexate and Characterization of Skin Treated by Fabricated PLGA Microneedles and Fractional Ablative Laser. Pharm. Res. 2018, 35, 1–20. [Google Scholar] [CrossRef]
- Brogden, N.K.; Banks, S.L.; Crofford, L.J.; Stinchcomb, A.L. Diclofenac Enables Unprecedented Week-Long Microneedle-Enhanced Delivery of a Skin Impermeable Medication in Humans. Pharm. Res. 2013, 30, 1947–1955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, J.; Gill, H.S.; Andrews, S.N.; Prausnitz, M.R. Kinetics of Skin Resealing after Insertion of Microneedles in Human Subjects. J. Control. Release 2011, 154, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Haridass, I.N.; Wei, J.C.; Mohammed, Y.H.; Crichton, M.L.; Anderson, C.D.; Henricson, J.; Sanchez, W.Y.; Meliga, S.C.; Grice, J.E.; Benson, H.A. Cellular Metabolism and Pore Lifetime of Human Skin Following Microprojection Array Mediation. J. Control. Release 2019, 306, 59–68. [Google Scholar]
- Avcil, M.; Çelik, A. Microneedles in Drug Delivery: Progress and Challenges. Micromachines 2021, 12, 1321. [Google Scholar] [CrossRef]
- Chen, M.-C.; Huang, S.-F.; Lai, K.-Y.; Ling, M.-H. Fully Embeddable Chitosan Microneedles as a Sustained Release Depot for Intradermal Vaccination. Biomaterials 2013, 34, 3077–3086. [Google Scholar] [CrossRef]
- Han, Y.; Gao, Z.; Chen, L.; Kang, L.; Huang, W.; Jin, M.; Wang, Q.; Bae, Y.H. Multifunctional Oral Delivery Systems for Enhanced Bioavailability of Therapeutic Peptides/Proteins. Acta Pharm. Sin. B 2019, 9, 902–922. [Google Scholar]
- Katikaneni, S. Transdermal Delivery of Biopharmaceuticals: Dream or Reality? Ther. Deliv. 2015, 6, 1109–1116. [Google Scholar] [CrossRef]
- Mitragotri, S.; Burke, P.A.; Langer, R. Overcoming the Challenges in Administering Biopharmaceuticals: Formulation and Delivery Strategies. Nat. Rev. Drug Discov. 2014, 13, 655–672. [Google Scholar] [CrossRef] [Green Version]
- Herwadkar, A.; Banga, A.K. Transdermal Delivery of Peptides and Proteins. In Peptide and Protein Delivery; Elsevier: Amsterdam, The Netherlands, 2011; pp. 69–86. [Google Scholar]
- Yan, M.; Du, J.; Gu, Z.; Liang, M.; Hu, Y.; Zhang, W.; Priceman, S.; Wu, L.; Zhou, Z.H.; Liu, Z. A Novel Intracellular Protein Delivery Platform Based on Single-Protein Nanocapsules. Nat. Nanotechnol. 2010, 5, 48–53. [Google Scholar] [CrossRef]
- Agyei, D.; Ahmed, I.; Akram, Z.; MN Iqbal, H.; K Danquah, M. Protein and Peptide Biopharmaceuticals: An Overview. Protein Pept. Lett. 2017, 24, 94–101. [Google Scholar] [CrossRef]
- Jain, D.; Mahammad, S.S.; Singh, P.P.; Kodipyaka, R. A Review on Parenteral Delivery of Peptides and Proteins. Drug Dev. Ind. Pharm. 2019, 45, 1403–1420. [Google Scholar] [CrossRef]
- Ye, Y.; Yu, J.; Wen, D.; Kahkoska, A.R.; Gu, Z. Polymeric Microneedles for Transdermal Protein Delivery. Adv. Drug Deliv. Rev. 2018, 127, 106–118. [Google Scholar] [CrossRef]
- Riley, R.S.; June, C.H.; Langer, R.; Mitchell, M.J. Delivery Technologies for Cancer Immunotherapy. Nat. Rev. Drug Discov. 2019, 18, 175–196. [Google Scholar] [CrossRef]
- Kinch, M.S. An Overview of FDA-Approved Biologics Medicines. Drug Discov. Today 2015, 20, 393–398. [Google Scholar] [CrossRef]
- Kirkby, M.; Hutton, A.R.; Donnelly, R.F. Microneedle Mediated Transdermal Delivery of Protein, Peptide and Antibody Based Therapeutics: Current Status and Future Considerations. Pharm. Res. 2020, 37, 1–18. [Google Scholar] [CrossRef]
- Ibraheem, D.; Elaissari, A.; Fessi, H. Administration Strategies for Proteins and Peptides. Int. J. Pharm. 2014, 477, 578–589. [Google Scholar] [CrossRef]
- Chaulagain, B.; Jain, A.; Tiwari, A.; Verma, A.; Jain, S.K. Passive Delivery of Protein Drugs through Transdermal Route. Artif. Cells Nanomed. Biotechnol. 2018, 46, 472–487. [Google Scholar] [CrossRef] [Green Version]
- Asfour, M.H. Advanced Trends in Protein and Peptide Drug Delivery: A Special Emphasis on Aquasomes and Microneedles Techniques. Drug Deliv. Transl. Res. 2021, 11, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.O.; Fathe, K.R.; Brunaugh, A.; Ferrati, S.; Li, S.; Montenegro-Nicolini, M.; Mousavikhamene, Z.; McConville, J.T.; Prausnitz, M.R.; Smyth, H.D. Challenges and Future Prospects for the Delivery of Biologics: Oral Mucosal, Pulmonary, and Transdermal Routes. AAPS J. 2017, 19, 652–668. [Google Scholar] [CrossRef] [PubMed]
- Ye, M.; Kim, S.; Park, K. Issues in Long-Term Protein Delivery Using Biodegradable Microparticles. J. Control. Release 2010, 146, 241–260. [Google Scholar] [CrossRef] [PubMed]
- Bruno, B.J.; Miller, G.D.; Lim, C.S. Basics and Recent Advances in Peptide and Protein Drug Delivery. Ther. Deliv. 2013, 4, 1443–1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawat, A.; Burgess, D.J. Parenteral Delivery of Peptides and Proteins. In Biodrug Delivery Systems; CRC Press: Boca Raton, FL, USA, 2016; pp. 66–84. [Google Scholar]
- Patel, A.; Cholkar, K.; Mitra, A.K. Recent Developments in Protein and Peptide Parenteral Delivery Approaches. Ther. Deliv. 2014, 5, 337–365. [Google Scholar] [CrossRef]
- Lopes, A.M.; Apolinário, A.C.; Valenzuela-Oses, J.K.; Costa, J.S.; Pessoa, A.; Barbosa, L.R. Nanostructures for Protein Drug Delivery. Biomater. Sci. 2016, 4, 205–218. [Google Scholar]
- Zhang, L.; Dong, Z.; Liu, W.; Wu, X.; He, H.; Lu, Y.; Wu, W.; Qi, J. Novel Pharmaceutical Strategies for Enhancing Skin Penetration of Biomacromolecules. Pharmaceuticals 2022, 15, 877. [Google Scholar] [CrossRef]
- Blattner, C.M.; Coman, G.; Blickenstaff, N.R.; Maibach, H.I. Percutaneous Absorption of Water in Skin: A Review. Rev. Environ. Health 2014, 29, 175–180. [Google Scholar] [CrossRef]
- Depelsenaire, A.C.; Witham, K.; Veitch, M.; Wells, J.W.; Anderson, C.D.; Lickliter, J.D.; Rockman, S.; Bodle, J.; Treasure, P.; Hickling, J. Cellular Responses at the Application Site of a High-Density Microarray Patch Delivering an Influenza Vaccine in a Randomized, Controlled Phase I Clinical Trial. PLoS ONE 2021, 16, e0255282. [Google Scholar] [CrossRef]
- Ng, H.-I.; Tuong, Z.K.; Fernando, G.J.P.; Depelsenaire, A.C.I.; Meliga, S.C.; Frazer, I.H.; Kendall, M.A.F. Microprojection Arrays Applied to Skin Generate Mechanical Stress, Induce an Inflammatory Transcriptome and Cell Death, and Improve Vaccine-Induced Immune Responses. Npj Vaccines 2019, 4, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Rouphael, N.G.; Paine, M.; Mosley, R.; Henry, S.; McAllister, D.V.; Kalluri, H.; Pewin, W.; Frew, P.M.; Yu, T.; Thornburg, N.J. The Safety, Immunogenicity, and Acceptability of Inactivated Influenza Vaccine Delivered by Microneedle Patch (TIV-MNP 2015): A Randomised, Partly Blinded, Placebo-Controlled, Phase 1 Trial. Lancet 2017, 390, 649–658. [Google Scholar] [CrossRef]
- Khan, S.; Minhas, M.U.; Singh Thakur, R.R.; Aqeel, M.T. Microneedles Assisted Controlled and Improved Transdermal Delivery of High Molecular Drugs via in Situ Forming Depot Thermoresponsive Poloxamers Gels in Skin Microchannels. Drug Dev. Ind. Pharm. 2022, 48, 265–278. [Google Scholar] [CrossRef]
- Aich, K.; Singh, T.; Dang, S. Advances in Microneedle-Based Transdermal Delivery for Drugs and Peptides. Drug Deliv. Transl. Res. 2022, 12, 1556–1568. [Google Scholar] [CrossRef]
- Chandrasekhar, S.; Iyer, L.K.; Panchal, J.P.; Topp, E.M.; Cannon, J.B.; Ranade, V.V. Microarrays and Microneedle Arrays for Delivery of Peptides, Proteins, Vaccines and Other Applications. Expert Opin. Drug Deliv. 2013, 10, 1155–1170. [Google Scholar] [CrossRef]
- Peña-Juárez, M.; Guadarrama-Escobar, O.R.; Escobar-Chávez, J.J. Transdermal Delivery Systems for Biomolecules. J. Pharm. Innov. 2021, 17, 319–332. [Google Scholar] [CrossRef]
- Lee, J.W.; Choi, S.-O.; Felner, E.I.; Prausnitz, M.R. Dissolving Microneedle Patch for Transdermal Delivery of Human Growth Hormone. Small 2011, 7, 531–539. [Google Scholar] [CrossRef]
- Yu, J.; Zhang, Y.; Ye, Y.; DiSanto, R.; Sun, W.; Ranson, D.; Ligler, F.S.; Buse, J.B.; Gu, Z. Microneedle-Array Patches Loaded with Hypoxia-Sensitive Vesicles Provide Fast Glucose-Responsive Insulin Delivery. Proc. Natl. Acad. Sci. USA 2015, 112, 8260–8265. [Google Scholar] [CrossRef] [Green Version]
- Bao, C.; Li, Z.; Liang, S.; Hu, Y.; Wang, X.; Fang, B.; Wang, P.; Chen, S.; Li, Y. Microneedle Patch Delivery of Capsaicin-Containing α-Lactalbumin Nanomicelles to Adipocytes Achieves Potent Anti-Obesity Effects. Adv. Funct. Mater. 2021, 31, 2011130. [Google Scholar] [CrossRef]
- Chen, M.; Yang, D.; Sun, Y.; Liu, T.; Wang, W.; Fu, J.; Wang, Q.; Bai, X.; Quan, G.; Pan, X.; et al. In Situ Self-Assembly Nanomicelle Microneedles for Enhanced Photoimmunotherapy via Autophagy Regulation Strategy. ACS Nano 2021, 15, 3387–3401. [Google Scholar] [CrossRef]
- Wang, Y.; Cheng, S.; Hu, W.; Lin, X.; Cao, C.; Zou, S.; Tong, Z.; Jiang, G.; Kong, X. Polymer-Grafted Hollow Mesoporous Silica Nanoparticles Integrated with Microneedle Patches for Glucose-Responsive Drug Delivery. Front. Mater. Sci. 2021, 15, 98–112. [Google Scholar] [CrossRef]
- Oh, S.J.; Jung, J.H. Sustainable Drug Release Using Nanoparticle Encapsulated Microneedles. Chem. Asian J. 2022, 17, e202200333. [Google Scholar] [CrossRef] [PubMed]
- Salwa; Chevala, N.T.; Jitta, S.R.; Marques, S.M.; Vaz, V.M.; Kumar, L. Polymeric Microneedles for Transdermal Delivery of Nanoparticles: Frontiers of Formulation, Sterility and Stability Aspects. J. Drug Deliv. Sci. Technol. 2021, 65, 102711. [Google Scholar] [CrossRef]
- Chen, W.; Tian, R.; Xu, C.; Yung, B.C.; Wang, G.; Liu, Y.; Ni, Q.; Zhang, F.; Zhou, Z.; Wang, J. Microneedle-Array Patches Loaded with Dual Mineralized Protein/Peptide Particles for Type 2 Diabetes Therapy. Nat. Commun. 2017, 8, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.-C.; Park, J.-H.; Prausnitz, M.R. Microneedles for Drug and Vaccine Delivery. Adv. Drug Deliv. Rev. 2012, 64, 1547–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo, R.; Jiang, T.; Di, J.; Tai, W.; Gu, Z. Emerging Micro-and Nanotechnology Based Synthetic Approaches for Insulin Delivery. Chem. Soc. Rev. 2014, 43, 3595–3629. [Google Scholar] [CrossRef]
- Waghule, T.; Singhvi, G.; Dubey, S.K.; Pandey, M.M.; Gupta, G.; Singh, M.; Dua, K. Microneedles: A Smart Approach and Increasing Potential for Transdermal Drug Delivery System. Biomed. Pharmacother. 2019, 109, 1249–1258. [Google Scholar] [CrossRef]
- Li, G.; Badkar, A.; Nema, S.; Kolli, C.S.; Banga, A.K. In Vitro Transdermal Delivery of Therapeutic Antibodies Using Maltose Microneedles. Int. J. Pharm. 2009, 368, 109–115. [Google Scholar] [CrossRef]
- Rejinold, N.S.; Shin, J.-H.; Seok, H.Y.; Kim, Y.-C. Biomedical Applications of Microneedles in Therapeutics: Recent Advancements and Implications in Drug Delivery. Expert Opin. Drug Deliv. 2016, 13, 109–131. [Google Scholar] [CrossRef]
- He, X.; Sun, J.; Zhuang, J.; Xu, H.; Liu, Y.; Wu, D. Microneedle System for Transdermal Drug and Vaccine Delivery: Devices, Safety, and Prospects. Dose-Response 2019, 17, 1559325819878585. [Google Scholar] [CrossRef] [Green Version]
- Larrañeta, E.; Lutton, R.E.M.; Woolfson, A.D.; Donnelly, R.F. Microneedle Arrays as Transdermal and Intradermal Drug Delivery Systems: Materials Science, Manufacture and Commercial Development. Mater. Sci. Eng. R Rep. 2016, 104, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Pastor, Y.; Larrañeta, E.; Erhard, Á.; Quincoces, G.; Peñuelas, I.; Irache, J.M.; Donnelly, R.; Gamazo, C. Dissolving Microneedles for Intradermal Vaccination against Shigellosis. Vaccines 2019, 7, 159. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.-J.; Vines, J.B.; Park, H.; Lee, S.-H. Microneedles: A Versatile Strategy for Transdermal Delivery of Biological Molecules. Int. J. Biol. Macromol. 2018, 110, 30–38. [Google Scholar] [CrossRef]
- Jamaledin, R.; Di Natale, C.; Onesto, V.; Taraghdari, Z.B.; Zare, E.N.; Makvandi, P.; Vecchione, R.; Netti, P.A. Progress in Microneedle-Mediated Protein Delivery. J. Clin. Med. 2020, 9, 542. [Google Scholar] [CrossRef] [Green Version]
- Di Natale, C.; La Manna, S.; Malfitano, A.M.; Di Somma, S.; Florio, D.; Scognamiglio, P.L.; Novellino, E.; Netti, P.A.; Marasco, D. Structural Insights into Amyloid Structures of the C-Terminal Region of Nucleophosmin 1 in Type A Mutation of Acute Myeloid Leukemia. Biochim. Biophys. Acta BBA-Proteins Proteom. 2019, 1867, 637–644. [Google Scholar] [CrossRef]
- Cobo, I.; Li, M.; Sumerlin, B.S.; Perrier, S. Smart Hybrid Materials by Conjugation of Responsive Polymers to Biomacromolecules. Nat. Mater. 2015, 14, 143–159. [Google Scholar] [CrossRef]
- Karimi, M.; Sahandi Zangabad, P.; Baghaee-Ravari, S.; Ghazadeh, M.; Mirshekari, H.; Hamblin, M.R. Smart Nanostructures for Cargo Delivery: Uncaging and Activating by Light. J. Am. Chem. Soc. 2017, 139, 4584–4610. [Google Scholar] [CrossRef]
- Singh, S.K.; Afonina, N.; Awwad, M.; Bechtold-Peters, K.; Blue, J.T.; Chou, D.; Cromwell, M.; Krause, H.-J.; Mahler, H.-C.; Meyer, B.K.; et al. An Industry Perspective on the Monitoring of Subvisible Particles as a Quality Attribute for Protein Therapeutics. J. Pharm. Sci. 2010, 99, 3302–3321. [Google Scholar] [CrossRef]
- Migalska, K.; Morrow, D.I.J.; Garland, M.J.; Thakur, R.; Woolfson, A.D.; Donnelly, R.F. Laser-Engineered Dissolving Microneedle Arrays for Transdermal Macromolecular Drug Delivery. Pharm. Res. 2011, 28, 1919–1930. [Google Scholar] [CrossRef]
- Mistilis, M.J.; Bommarius, A.S.; Prausnitz, M.R. Development of a Thermostable Microneedle Patch for Influenza Vaccination. J. Pharm. Sci. 2015, 104, 740–749. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Rewatkar, P.; Wang, R.; Hasnain, S.Z.; Popat, A.; Kumeria, T. Nanocarriers for Oral Delivery of Biologics: Small Carriers for Big Payloads. Trends Pharmacol. Sci. 2021, 42, 957–972. [Google Scholar] [CrossRef]
- Donnelly, R.F.; Majithiya, R.; Singh, T.R.R.; Morrow, D.I.J.; Garland, M.J.; Demir, Y.K.; Migalska, K.; Ryan, E.; Gillen, D.; Scott, C.J.; et al. Design, Optimization and Characterisation of Polymeric Microneedle Arrays Prepared by a Novel Laser-Based Micromoulding Technique. Pharm. Res. 2011, 28, 41–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukushima, K.; Ise, A.; Morita, H.; Hasegawa, R.; Ito, Y.; Sugioka, N.; Takada, K. Two-Layered Dissolving Microneedles for Percutaneous Delivery of Peptide/Protein Drugs in Rats. Pharm. Res. 2011, 28, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.P.; Koutsonanos, D.G.; Del Pilar Martin, M.; Lee, J.W.; Zarnitsyn, V.; Choi, S.-O.; Murthy, N.; Compans, R.W.; Skountzou, I.; Prausnitz, M.R. Dissolving Polymer Microneedle Patches for Influenza Vaccination. Nat. Med. 2010, 16, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Battisti, M.; Vecchione, R.; Casale, C.; Pennacchio, F.A.; Lettera, V.; Jamaledin, R.; Profeta, M.; Di Natale, C.; Imparato, G.; Urciuolo, F. Non-Invasive Production of Multi-Compartmental Biodegradable Polymer Microneedles for Controlled Intradermal Drug Release of Labile Molecules. Front. Bioeng. Biotechnol. 2019, 7, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, E.Y.; Lee, J.; Kim, B.J.; Joo, K.I.; Kim, K.H.; Lim, G.; Cha, H.J. Bio-Inspired Swellable Hydrogel-Forming Double-Layered Adhesive Microneedle Protein Patch for Regenerative Internal/External Surgical Closure. Biomaterials 2019, 222, 119439. [Google Scholar] [CrossRef]
- Liu, S.; Zhang, S.; Duan, Y.; Niu, Y.; Gu, H.; Zhao, Z.; Zhang, S.; Yang, Y.; Wang, X.; Gao, Y. Transcutaneous Immunization of Recombinant Staphylococcal Enterotoxin B Protein Using a Dissolving Microneedle Provides Potent Protection against Lethal Enterotoxin Challenge. Vaccine 2019, 37, 3810–3819. [Google Scholar] [CrossRef]
- Ito, Y.; Hagiwara, E.; Saeki, A.; Sugioka, N.; Takada, K. Feasibility of Microneedles for Percutaneous Absorption of Insulin. Eur. J. Pharm. Sci. 2006, 29, 82–88. [Google Scholar] [CrossRef]
- Ling, M.-H.; Chen, M.-C. Dissolving Polymer Microneedle Patches for Rapid and Efficient Transdermal Delivery of Insulin to Diabetic Rats. Acta Biomater. 2013, 9, 8952–8961. [Google Scholar] [CrossRef]
- Kochhar, J.S.; Zou, S.; Chan, S.Y.; Kang, L. Protein Encapsulation in Polymeric Microneedles by Photolithography. Int. J. Nanomed. 2012, 7, 3143–3154. [Google Scholar] [CrossRef] [Green Version]
- Kochhar, J.S.; Goh, W.J.; Chan, S.Y.; Kang, L. A Simple Method of Microneedle Array Fabrication for Transdermal Drug Delivery. Drug Dev. Ind. Pharm. 2013, 39, 299–309. [Google Scholar] [CrossRef]
- Mönkäre, J.; Reza Nejadnik, M.; Baccouche, K.; Romeijn, S.; Jiskoot, W.; Bouwstra, J.A. IgG-Loaded Hyaluronan-Based Dissolving Microneedles for Intradermal Protein Delivery. J. Control. Release 2015, 218, 53–62. [Google Scholar] [CrossRef]
- Hiraishi, Y.; Nakagawa, T.; Quan, Y.-S.; Kamiyama, F.; Hirobe, S.; Okada, N.; Nakagawa, S. Performance and Characteristics Evaluation of a Sodium Hyaluronate-Based Microneedle Patch for a Transcutaneous Drug Delivery System. Int. J. Pharm. 2013, 441, 570–579. [Google Scholar] [CrossRef]
- Park, J.-H.; Allen, M.G.; Prausnitz, M.R. Polymer Microneedles for Controlled-Release Drug Delivery. Pharm. Res. 2006, 23, 1008–1019. [Google Scholar] [CrossRef]
- Lee, J.W.; Park, J.-H.; Prausnitz, M.R. Dissolving Microneedles for Transdermal Drug Delivery. Biomaterials 2008, 29, 2113–2124. [Google Scholar] [CrossRef] [Green Version]
- Ameri, M.; Daddona, P.E.; Maa, Y.-F. Demonstrated Solid-State Stability of Parathyroid Hormone PTH (1–34) Coated on a Novel Transdermal Microprojection Delivery System. Pharm. Res. 2009, 26, 2454–2463. [Google Scholar] [CrossRef]
- Gomaa, Y.; Kolluru, C.; Milewski, M.; Lee, D.; Zhang, J.; Saklatvala, R.; Prausnitz, M.R. Development of a Thermostable Oxytocin Microneedle Patch. J. Control. Release 2021, 337, 81–89. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Banga, A.K. Fabrication, Characterization and Application of Sugar Microneedles for Transdermal Drug Delivery. Ther. Deliv. 2017, 8, 249–264. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Banga, A.K. Enhanced Skin Delivery of Vismodegib by Microneedle Treatment. Drug Deliv. Transl. Res. 2015, 5, 407–423. [Google Scholar] [CrossRef]
- Cheung, K.; Han, T.; Das, D.B. Effect of Force of Microneedle Insertion on the Permeability of Insulin in Skin. J. Diabetes Sci. Technol. 2014, 8, 444–452. [Google Scholar] [CrossRef] [Green Version]
- Yan, G.; Warner, K.S.; Zhang, J.; Sharma, S.; Gale, B.K. Evaluation Needle Length and Density of Microneedle Arrays in the Pretreatment of Skin for Transdermal Drug Delivery. Int. J. Pharm. 2010, 391, 7–12. [Google Scholar] [CrossRef]
- Kumar, A.; Li, X.; Sandoval, M.A.; Rodriguez, B.L.; Sloat, B.R.; Cui, Z. Permeation of Antigen Protein-Conjugated Nanoparticles and Live Bacteria through Microneedle-Treated Mouse Skin. Int. J. Nanomed. 2011, 6, 1253–1264. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Badkar, A.; Kalluri, H.; Banga, A.K. Microchannels Created by Sugar and Metal Microneedles: Characterization by Microscopy, Macromolecular Flux and Other Techniques. J. Pharm. Sci. 2010, 99, 1931–1941. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Qiu, Y.; Gao, Y. Enhanced Delivery of Hydrophilic Peptides in Vitro by Transdermal Microneedle Pretreatment. Acta Pharm. Sin. B 2014, 4, 100–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Gao, Y.; Qin, G.; Zhang, S.; Qiu, Y.; Li, F.; Xu, B. Sustained Release of Insulin through Skin by Intradermal Microdelivery System. Biomed. Microdevices 2010, 12, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.Y.; Zhang, J.N.; Chen, B.Z.; Wang, Q.L.; Guo, X.D. A Solid Polymer Microneedle Patch Pretreatment Enhances the Permeation of Drug Molecules into the Skin. RSC Adv. 2017, 7, 15408–15415. [Google Scholar] [CrossRef] [Green Version]
- Martanto, W.; Davis, S.P.; Holiday, N.R.; Wang, J.; Gill, H.S.; Prausnitz, M.R. Transdermal Delivery of Insulin Using Microneedles in Vivo. Pharm. Res. 2004, 21, 947–952. [Google Scholar] [CrossRef]
- Qiu, Y.; Qin, G.; Zhang, S.; Wu, Y.; Xu, B.; Gao, Y. Novel Lyophilized Hydrogel Patches for Convenient and Effective Administration of Microneedle-Mediated Insulin Delivery. Int. J. Pharm. 2012, 437, 51–56. [Google Scholar] [CrossRef]
- Chen, X.; Kask, A.S.; Crichton, M.L.; McNeilly, C.; Yukiko, S.; Dong, L.; Marshak, J.O.; Jarrahian, C.; Fernando, G.J.; Chen, D. Improved DNA Vaccination by Skin-Targeted Delivery Using Dry-Coated Densely-Packed Microprojection Arrays. J. Control. Release 2010, 148, 327–333. [Google Scholar] [CrossRef]
- Ma, Y.; Gill, H.S. Coating Solid Dispersions on Microneedles via a Molten Dip-Coating Method: Development and in Vitro Evaluation for Transdermal Delivery of a Water-Insoluble Drug. J. Pharm. Sci. 2014, 103, 3621–3630. [Google Scholar] [CrossRef] [Green Version]
- Ameri, M.; Kadkhodayan, M.; Nguyen, J.; Bravo, J.A.; Su, R.; Chan, K.; Samiee, A.; Daddona, P.E. Human Growth Hormone Delivery with a Microneedle Transdermal System: Preclinical Formulation, Stability, Delivery and PK of Therapeutically Relevant Doses. Pharmaceutics 2014, 6, 220–234. [Google Scholar] [CrossRef] [Green Version]
- Kusamori, K.; Katsumi, H.; Sakai, R.; Hayashi, R.; Hirai, Y.; Tanaka, Y.; Hitomi, K.; Quan, Y.; Kamiyama, F.; Yamada, K. Development of a Drug-Coated Microneedle Array and Its Application for Transdermal Delivery of Interferon Alpha. Biofabrication 2016, 8, 015006. [Google Scholar] [CrossRef]
- Caudill, C.L.; Perry, J.L.; Tian, S.; Luft, J.C.; DeSimone, J.M. Spatially Controlled Coating of Continuous Liquid Interface Production Microneedles for Transdermal Protein Delivery. J. Control. Release 2018, 284, 122–132. [Google Scholar] [CrossRef]
- Daddona, P.E.; Matriano, J.A.; Mandema, J.; Maa, Y.-F. Parathyroid Hormone (1-34)-Coated Microneedle Patch System: Clinical Pharmacokinetics and Pharmacodynamics for Treatment of Osteoporosis. Pharm. Res. 2011, 28, 159–165. [Google Scholar] [CrossRef]
- Kapoor, Y.; Milewski, M.; Dick, L.; Zhang, J.; Bothe, J.R.; Gehrt, M.; Manser, K.; Nissley, B.; Petrescu, I.; Johnson, P. Coated Microneedles for Transdermal Delivery of a Potent Pharmaceutical Peptide. Biomed. Microdevices 2020, 22, 7. [Google Scholar] [CrossRef]
- Peters, E.E.; Ameri, M.; Wang, X.; Maa, Y.-F.; Daddona, P.E. Erythropoietin-Coated ZP-Microneedle Transdermal System: Preclinical Formulation, Stability, and Delivery. Pharm. Res. 2012, 29, 1618–1626. [Google Scholar] [CrossRef]
- Ross, S.; Scoutaris, N.; Lamprou, D.; Mallinson, D.; Douroumis, D. Inkjet Printing of Insulin Microneedles for Transdermal Delivery. Drug Deliv. Transl. Res. 2015, 5, 451–461. [Google Scholar] [CrossRef]
- Saurer, E.M.; Flessner, R.M.; Sullivan, S.P.; Prausnitz, M.R.; Lynn, D.M. Layer-by-Layer Assembly of DNA-and Protein-Containing Films on Microneedles for Drug Delivery to the Skin. Biomacromolecules 2010, 11, 3136–3143. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Coulman, S.A.; Hanna, S.J.; Wong, F.S.; Dayan, C.M.; Birchall, J.C. Formulation of Hydrophobic Peptides for Skin Delivery via Coated Microneedles. J. Control. Release 2017, 265, 2–13. [Google Scholar] [CrossRef]
- Li, S.; Li, W.; Prausnitz, M. Individually Coated Microneedles for Co-Delivery of Multiple Compounds with Different Properties. Drug Deliv. Transl. Res. 2018, 8, 1043–1052. [Google Scholar] [CrossRef]
- Sathyan, G.; Sun, Y.N.; Weyers, R.; Daddona, P.; Staehr, P.; Gupta, S. Macroflux® Desmopressin Transdermal Delivery System: Pharmacokinetics and Pharmacodynamic Evaluation in Healthy Volunteers. AAPS J. 2004, 6, 665. [Google Scholar]
- Shrestha, P.; Stoeber, B. Fluid Absorption by Skin Tissue during Intradermal Injections through Hollow Microneedles. Sci. Rep. 2018, 8, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terashima, S.; Tatsukawa, C.; Takahashi, T.; Suzuki, M.; Aoyagi, S. Fabrication of Hyaluronic Acid Hollow Microneedle Array. Jpn. J. Appl. Phys. 2020, 59, SIIJ03. [Google Scholar] [CrossRef]
- Harvey, A.J.; Kaestner, S.A.; Sutter, D.E.; Harvey, N.G.; Mikszta, J.A.; Pettis, R.J. Microneedle-Based Intradermal Delivery Enables Rapid Lymphatic Uptake and Distribution of Protein Drugs. Pharm. Res. 2011, 28, 107–116. [Google Scholar] [CrossRef] [PubMed]
- McVey, E.; Hirsch, L.; Sutter, D.E.; Kapitza, C.; Dellweg, S.; Clair, J.; Rebrin, K.; Judge, K.; Pettis, R.J. Pharmacokinetics and Postprandial Glycemic Excursions Following Insulin Lispro Delivered by Intradermal Microneedle or Subcutaneous Infusion. J. Diabetes Sci. Technol. 2012, 6, 743–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, J.; Felner, E.I.; Prausnitz, M.R. Rapid Pharmacokinetics of Intradermal Insulin Administered Using Microneedles in Type 1 Diabetes Subjects. Diabetes Technol. Ther. 2011, 13, 451–456. [Google Scholar] [CrossRef] [Green Version]
- McAllister, D.V.; Wang, P.M.; Davis, S.P.; Park, J.-H.; Canatella, P.J.; Allen, M.G.; Prausnitz, M.R. Microfabricated Needles for Transdermal Delivery of Macromolecules and Nanoparticles: Fabrication Methods and Transport Studies. Proc. Natl. Acad. Sci. USA 2003, 100, 13755–13760. [Google Scholar] [CrossRef] [Green Version]
- Xenikakis, I.; Tsongas, K.; Tzimtzimis, E.K.; Katsamenis, O.L.; Demiri, E.; Zacharis, C.K.; Georgiou, D.; Kalogianni, E.P.; Tzetzis, D.; Fatouros, D.G. Transdermal Delivery of Insulin across Human Skin in Vitro with 3D Printed Hollow Microneedles. J. Drug Deliv. Sci. Technol. 2022, 67, 102891. [Google Scholar] [CrossRef]
- Torrisi, B.M.; Zarnitsyn, V.; Prausnitz, M.R.; Anstey, A.; Gateley, C.; Birchall, J.C.; Coulman, S.A. Pocketed Microneedles for Rapid Delivery of a Liquid-State Botulinum Toxin A Formulation into Human Skin. J. Control. Release 2013, 165, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Golombek, S.; Pilz, M.; Steinle, H.; Kochba, E.; Levin, Y.; Lunter, D.; Schlensak, C.; Wendel, H.P.; Avci-Adali, M. Intradermal Delivery of Synthetic MRNA Using Hollow Microneedles for Efficient and Rapid Production of Exogenous Proteins in Skin. Mol. Ther.-Nucleic Acids 2018, 11, 382–392. [Google Scholar] [CrossRef] [Green Version]
- Valla, V. Therapeutics of Diabetes Mellitus: Focus on Insulin Analogues and Insulin Pumps. Exp. Diabetes Res. 2010, 2010, 178372. [Google Scholar] [CrossRef] [Green Version]
- Burton, S.A.; Ng, C.-Y.; Simmers, R.; Moeckly, C.; Brandwein, D.; Gilbert, T.; Johnson, N.; Brown, K.; Alston, T.; Prochnow, G.; et al. Rapid Intradermal Delivery of Liquid Formulations Using a Hollow Microstructured Array. Pharm. Res. 2011, 28, 31–40. [Google Scholar] [CrossRef] [Green Version]
- An, M.; Liu, H. Dissolving Microneedle Arrays for Transdermal Delivery of Amphiphilic Vaccines. Small 2017, 13, 1700164. [Google Scholar] [CrossRef]
- Hong, X.; Wei, L.; Wu, F.; Wu, Z.; Chen, L.; Liu, Z.; Yuan, W. Dissolving and Biodegradable Microneedle Technologies for Transdermal Sustained Delivery of Drug and Vaccine. Drug Des. Devel. Ther. 2013, 7, 945–952. [Google Scholar] [CrossRef] [Green Version]
- Tran, K.; Gavitt, T.D.; Farrell, N.J.; Curry, E.J.; Mara, A.B.; Patel, A.; Brown, L.; Kilpatrick, S.; Piotrowska, R.; Mishra, N. Transdermal Microneedles for the Programmable Burst Release of Multiple Vaccine Payloads. Nat. Biomed. Eng. 2021, 5, 998–1007. [Google Scholar] [CrossRef]
- Lopez-Ramirez, M.A.; Kupor, D.; Marchiori, L.; Soto, F.; Rueda, R.; Reynoso, M.; Narra, L.R.; Chakravarthy, K.; Wang, J. Combinatorial Microneedle Patch with Tunable Release Kinetics and Dual Fast-Deep/Sustained Release Capabilities. J. Mater. Chem. B 2021, 9, 2189–2199. [Google Scholar] [CrossRef]
- Amani, H.; Shahbazi, M.-A.; D’Amico, C.; Fontana, F.; Abbaszadeh, S.; Santos, H.A. Microneedles for Painless Transdermal Immunotherapeutic Applications. J. Control. Release 2021, 330, 185–217. [Google Scholar] [CrossRef]
- Dardano, P.; De Martino, S.; Battisti, M.; Miranda, B.; Rea, I.; De Stefano, L. One-Shot Fabrication of Polymeric Hollow Microneedles by Standard Photolithography. Polymers 2021, 13, 520. [Google Scholar] [CrossRef]
- Chang, H.; Chew, S.W.T.; Zheng, M.; Lio, D.C.S.; Wiraja, C.; Mei, Y.; Ning, X.; Cui, M.; Than, A.; Shi, P.; et al. Cryomicroneedles for Transdermal Cell Delivery. Nat. Biomed. Eng. 2021, 5, 1008–1018. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, H.; Hu, T.; Xu, C.; Jiang, L.; Shrike Zhang, Y.; Xie, M. Recent Advances of Microneedles Used towards Stimuli-Responsive Drug Delivery, Disease Theranostics, and Bioinspired Applications. Chem. Eng. J. 2021, 426, 130561. [Google Scholar] [CrossRef]
- Vora, L.K.; Moffatt, K.; Tekko, I.A.; Paredes, A.J.; Volpe-Zanutto, F.; Mishra, D.; Peng, K.; Raj Singh Thakur, R.; Donnelly, R.F. Microneedle Array Systems for Long-Acting Drug Delivery. Eur. J. Pharm. Biopharm. 2021, 159, 44–76. [Google Scholar] [CrossRef]
- Ohn, J.; Jang, M.; Kang, B.M.; Yang, H.; Hong, J.T.; Kim, K.H.; Kwon, O.; Jung, H. Dissolving Candlelit Microneedle for Chronic Inflammatory Skin Diseases. Adv. Sci. 2021, 8, 2004873. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Lee, C.Y.; Jung, H. Dissolving Microneedles for Transdermal Drug Administration Prepared by Stepwise Controlled Drawing of Maltose. Biomaterials 2011, 32, 3134–3140. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-C.; Ling, M.-H.; Lai, K.-Y.; Pramudityo, E. Chitosan Microneedle Patches for Sustained Transdermal Delivery of Macromolecules. Biomacromolecules 2012, 13, 4022–4031. [Google Scholar] [CrossRef] [PubMed]
- Yi, X.; Wang, C.; Yu, X.; Su, W.; Yuan, Z. Chitosan/Zinc Nitrate Microneedles for Bacterial Biofilm Eradication. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 911–920. [Google Scholar] [CrossRef]
- Chu, L.Y.; Choi, S.-O.; Prausnitz, M.R. Fabrication of Dissolving Polymer Microneedles for Controlled Drug Encapsulation and Delivery: Bubble and Pedestal Microneedle Designs. J. Pharm. Sci. 2010, 99, 4228–4238. [Google Scholar] [CrossRef]
- Moga, K.A.; Bickford, L.R.; Geil, R.D.; Dunn, S.S.; Pandya, A.A.; Wang, Y.; Fain, J.H.; Archuleta, C.F.; O’Neill, A.T.; Desimone, J.M. Rapidly-Dissolvable Microneedle Patches via a Highly Scalable and Reproducible Soft Lithography Approach. Adv. Mater. 2013, 25, 5060–5066. [Google Scholar] [CrossRef]
- Fukushima, K.; Yamazaki, T.; Hasegawa, R.; Ito, Y.; Sugioka, N.; Takada, K. Pharmacokinetic and Pharmacodynamic Evaluation of Insulin Dissolving Microneedles in Dogs. Diabetes Technol. Ther. 2010, 12, 465–474. [Google Scholar] [CrossRef]
- Ito, Y.; Yamazaki, T.; Sugioka, N.; Takada, K. Self-Dissolving Micropile Array Tips for Percutaneous Administration of Insulin. J. Mater. Sci. Mater. Med. 2010, 21, 835–841. [Google Scholar] [CrossRef]
- Shen, D.; Yu, H.; Wang, L.; Chen, X.; Feng, J.; Zhang, Q.; Xiong, W.; Pan, J.; Han, Y.; Liu, X. Biodegradable Phenylboronic Acid-Modified ε-Polylysine for Glucose-Responsive Insulin Delivery via Transdermal Microneedles. J. Mater. Chem. B 2021, 9, 6017–6028. [Google Scholar] [CrossRef]
- Zhang, Y.; Wu, M.; Tan, D.; Liu, Q.; Xia, R.; Chen, M.; Liu, Y.; Xue, L.; Lei, Y. A Dissolving and Glucose-Responsive Insulin-Releasing Microneedle Patch for Type 1 Diabetes Therapy. J. Mater. Chem. B 2021, 9, 648–657. [Google Scholar] [CrossRef]
- Chen, M.-C.; Ling, M.-H.; Kusuma, S.J. Poly-γ-Glutamic Acid Microneedles with a Supporting Structure Design as a Potential Tool for Transdermal Delivery of Insulin. Acta Biomater. 2015, 24, 106–116. [Google Scholar] [CrossRef]
- Kim, J.D.; Kim, M.; Yang, H.; Lee, K.; Jung, H. Droplet-Born Air Blowing: Novel Dissolving Microneedle Fabrication. J. Control. Release 2013, 170, 430–436. [Google Scholar] [CrossRef]
- Yang, C.; Sheng, T.; Hou, W.; Zhang, J.; Cheng, L.; Wang, H.; Liu, W.; Wang, S.; Yu, X.; Zhang, Y. Glucose-Responsive Microneedle Patch for Closed-Loop Dual-Hormone Delivery in Mice and Pigs. Sci. Adv. 2022, 8, eadd3197. [Google Scholar] [CrossRef]
- Demir, B.; Rosselle, L.; Voronova, A.; Pagneux, Q.; Quenon, A.; Gmyr, V.; Jary, D.; Hennuyer, N.; Staels, B.; Hubert, T. Innovative Transdermal Delivery of Insulin Using Gelatin Methacrylate-Based Microneedle Patches in Mice and Mini-Pigs. Nanoscale Horiz. 2022, 7, 174–184. [Google Scholar] [CrossRef]
- Jeong, H.-R.; Kim, J.-Y.; Kim, S.-N.; Park, J.-H. Local Dermal Delivery of Cyclosporin A, a Hydrophobic and High Molecular Weight Drug, Using Dissolving Microneedles. Eur. J. Pharm. Biopharm. 2018, 127, 237–243. [Google Scholar] [CrossRef]
- Liu, S.; Jin, M.; Quan, Y.; Kamiyama, F.; Kusamori, K.; Katsumi, H.; Sakane, T.; Yamamoto, A. Transdermal Delivery of Relatively High Molecular Weight Drugs Using Novel Self-Dissolving Microneedle Arrays Fabricated from Hyaluronic Acid and Their Characteristics and Safety after Application to the Skin. Eur. J. Pharm. Biopharm. 2014, 86, 267–276. [Google Scholar] [CrossRef]
- Chen, J.; Qiu, Y.; Zhang, S.; Gao, Y. Dissolving Microneedle-Based Intradermal Delivery of Interferon-α-2b. Drug Dev. Ind. Pharm. 2016, 42, 890–896. [Google Scholar] [CrossRef]
- Dillon, C.; Hughes, H.; O’Reilly, N.J.; McLoughlin, P. Formulation and Characterisation of Dissolving Microneedles for the Transdermal Delivery of Therapeutic Peptides. Int. J. Pharm. 2017, 526, 125–136. [Google Scholar] [CrossRef]
- Fakhraei Lahiji, S.; Jang, Y.; Huh, I.; Yang, H.; Jang, M.; Jung, H. Exendin-4–Encapsulated Dissolving Microneedle Arrays for Efficient Treatment of Type 2 Diabetes. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Lahiji, S.F.; Jang, Y.; Ma, Y.; Dangol, M.; Yang, H.; Jang, M.; Jung, H. Effects of Dissolving Microneedle Fabrication Parameters on the Activity of Encapsulated Lysozyme. Eur. J. Pharm. Sci. 2018, 117, 290–296. [Google Scholar] [CrossRef]
- Vora, L.K.; Courtenay, A.J.; Tekko, I.A.; Larrañeta, E.; Donnelly, R.F. Pullulan-Based Dissolving Microneedle Arrays for Enhanced Transdermal Delivery of Small and Large Biomolecules. Int. J. Biol. Macromol. 2020, 146, 290–298. [Google Scholar] [CrossRef] [PubMed]
- GhavamiNejad, A.; Li, J.; Lu, B.; Zhou, L.; Lam, L.; Giacca, A.; Wu, X.Y. Glucose-Responsive Composite Microneedle Patch for Hypoglycemia-Triggered Delivery of Native Glucagon. Adv. Mater. 2019, 31, 1901051. [Google Scholar] [CrossRef] [PubMed]
- Naito, C.; Katsumi, H.; Suzuki, T.; Quan, Y.; Kamiyama, F.; Sakane, T.; Yamamoto, A. Self-Dissolving Microneedle Arrays for Transdermal Absorption Enhancement of Human Parathyroid Hormone (1-34). Pharmaceutics 2018, 10, 215. [Google Scholar] [CrossRef] [Green Version]
- Chi, J.; Zhang, X.; Chen, C.; Shao, C.; Zhao, Y.; Wang, Y. Antibacterial and Angiogenic Chitosan Microneedle Array Patch for Promoting Wound Healing. Bioact. Mater. 2020, 5, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Murano, H.; Hamasaki, N.; Fukushima, K.; Takada, K. Incidence of Low Bioavailability of Leuprolide Acetate after Percutaneous Administration to Rats by Dissolving Microneedles. Int. J. Pharm. 2011, 407, 126–131. [Google Scholar] [CrossRef]
- Fakhraei Lahiji, S.; Kim, Y.; Kang, G.; Kim, S.; Lee, S.; Jung, H. Tissue Interlocking Dissolving Microneedles for Accurate and Efficient Transdermal Delivery of Biomolecules. Sci. Rep. 2019, 9, 7886. [Google Scholar] [CrossRef] [Green Version]
- Yao, Z.; Xue, T.; Xiong, H.; Cai, C.; Liu, X.; Wu, F.; Liu, S.; Fan, C. Promotion of Collagen Deposition during Skin Healing through Smad3/MTOR Pathway by Parathyroid Hormone-Loaded Microneedle. Mater. Sci. Eng. C 2021, 119, 111446. [Google Scholar] [CrossRef]
- Chen, Y.; Yu, W.; Qian, X.; Li, X.; Wang, Y.; Ji, J. Dissolving Microneedles with a Biphasic Release of Antibacterial Agent and Growth Factor to Promote Wound Healing. Biomater. Sci. 2022, 10, 2409–2416. [Google Scholar] [CrossRef]
- Sim, J.; Kang, G.; Yang, H.; Jang, M.; Kim, Y.; Ahn, H.; Kim, M.; Jung, H. Development of Clinical Weekly-Dose Teriparatide Acetate Encapsulated Dissolving Microneedle Patch for Efficient Treatment of Osteoporosis. Polymers 2022, 14, 4027. [Google Scholar] [CrossRef]
- GhavamiNejad, A.; Lu, B.; Samarikhalaj, M.; Liu, J.F.; Mirzaie, S.; Pereira, S.; Zhou, L.; Giacca, A.; Wu, X.Y. Transdermal Delivery of a Somatostatin Receptor Type 2 Antagonist Using Microneedle Patch Technology for Hypoglycemia Prevention. Drug Deliv. Transl. Res. 2022, 12, 792–804. [Google Scholar] [CrossRef]
- Hu, W.; Peng, T.; Huang, Y.; Ren, T.; Chen, H.; Chen, Y.; Feng, D.; Wu, C.; Pan, X. Hyaluronidase-Powered Microneedles for Significantly Enhanced Transdermal Delivery Efficiency. J. Control. Release 2023, 353, 380–390. [Google Scholar] [CrossRef]
- Panda, A.; Sharma, P.K.; McCann, T.; Bloomekatz, J.; Repka, M.A.; Murthy, S.N. Fabrication and Development of Controlled Release PLGA Microneedles for Macromolecular Delivery Using FITC-Dextran as Model Molecule. J. Drug Deliv. Sci. Technol. 2022, 68, 102712. [Google Scholar] [CrossRef]
- Men, Z.; Lu, X.; He, T.; Wu, M.; Su, T.; Shen, T. Microneedle Patch-Assisted Transdermal Administration of Recombinant Hirudin for the Treatment of Thrombotic Diseases. Int. J. Pharm. 2022, 612, 121332. [Google Scholar] [CrossRef]
- Don, T.-M.; Chen, M.; Lee, I.-C.; Huang, Y.-C. Preparation and Characterization of Fast Dissolving Ulvan Microneedles for Transdermal Drug Delivery System. Int. J. Biol. Macromol. 2022, 207, 90–99. [Google Scholar] [CrossRef]
- Abe, H.; Matsui, Y.; Kimura, N.; Nishizawa, M. Biodegradable Porous Microneedles for an Electric Skin Patch. Macromol. Mater. Eng. 2021, 306, 2100171. [Google Scholar] [CrossRef]
- Kusama, S.; Sato, K.; Matsui, Y.; Kimura, N.; Abe, H.; Yoshida, S.; Nishizawa, M. Transdermal Electroosmotic Flow Generated by a Porous Microneedle Array Patch. Nat. Commun. 2021, 12, 658. [Google Scholar] [CrossRef]
- Gholami, S.; Zarkesh, I.; Ghanian, M.-H.; Hajizadeh-Saffar, E.; Hassan-Aghaei, F.; Mohebi, M.-M.; Baharvand, H. Dynamically Capped Hierarchically Porous Microneedles Enable Post-Fabrication Loading and Self-Regulated Transdermal Delivery of Insulin. Chem. Eng. J. 2021, 421, 127823. [Google Scholar] [CrossRef]
- Tabassum, N.; Alba, M.; Yan, L.; Voelcker, N.H. Porous Silicon Microneedles for Enhanced Transdermal Drug Delivery. Adv. Ther. 2022, 2200156. [Google Scholar] [CrossRef]
- Lee, Y.; Li, W.; Tang, J.; Schwendeman, S.P.; Prausnitz, M.R. Immediate Detachment of Microneedles by Interfacial Fracture for Sustained Delivery of a Contraceptive Hormone in the Skin. J. Control. Release 2021, 337, 676–685. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, G.; Cai, L.; Wang, Y.; Sun, L.; Zhao, Y. Bioinspired Pagoda-like Microneedle Patches with Strong Fixation and Hemostasis Capabilities. Chem. Eng. J. 2021, 414, 128905. [Google Scholar] [CrossRef]
- Jung, J.H.; Jin, S.G. Microneedle for Transdermal Drug Delivery: Current Trends and Fabrication. J. Pharm. Investig. 2021, 51, 503–517. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Liu, Q.; Wang, X.; Gao, N.; Li, X.; Chen, H.; Mei, L.; Zeng, X. Actively Separated Microneedle Patch for Sustained-Release of Growth Hormone to Treat Growth Hormone Deficiency. Acta Pharm. Sin. B 2022, in press. [Google Scholar] [CrossRef]
- Li, J.Y.; Feng, Y.H.; He, Y.T.; Hu, L.F.; Liang, L.; Zhao, Z.Q.; Chen, B.Z.; Guo, X.D. Thermosensitive Hydrogel Microneedles for Controlled Transdermal Drug Delivery. Acta Biomater. 2022, 153, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.G.; White, L.R.; Estrela, P.; Leese, H.S. Hydrogel-Forming Microneedles: Current Advancements and Future Trends. Macromol. Biosci. 2021, 21, 2000307. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.F.; McCrudden, M.T.; Alkilani, A.Z.; Larrañeta, E.; McAlister, E.; Courtenay, A.J.; Kearney, M.-C.; Singh, T.R.R.; McCarthy, H.O.; Kett, V.L.; et al. Hydrogel-Forming Microneedles Prepared from “Super Swelling” Polymers Combined with Lyophilised Wafers for Transdermal Drug Delivery. PLoS ONE 2014, 9, e111547. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.F.; Singh, T.R.R.; Garland, M.J.; Migalska, K.; Majithiya, R.; McCrudden, C.M.; Kole, P.L.; Mahmood, T.M.T.; McCarthy, H.O.; Woolfson, A.D. Hydrogel-Forming Microneedle Arrays for Enhanced Transdermal Drug Delivery. Adv. Funct. Mater. 2012, 22, 4879–4890. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Yeo, D.C.; Wiraja, C.; Tey, H.L.; Mrksich, M.; Xu, C. Peptide Delivery with Poly (Ethylene Glycol) Diacrylate Microneedles through Swelling Effect. Bioeng. Transl. Med. 2017, 2, 258–267. [Google Scholar] [CrossRef]
- Seong, K.-Y.; Seo, M.-S.; Hwang, D.Y.; O’Cearbhaill, E.D.; Sreenan, S.; Karp, J.M.; Yang, S.Y. A Self-Adherent, Bullet-Shaped Microneedle Patch for Controlled Transdermal Delivery of Insulin. J. Control. Release 2017, 265, 48–56. [Google Scholar] [CrossRef]
- Courtenay, A.J.; McCrudden, M.T.; McAvoy, K.J.; McCarthy, H.O.; Donnelly, R.F. Microneedle-Mediated Transdermal Delivery of Bevacizumab. Mol. Pharm. 2018, 15, 3545–3556. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.; Liu, Y.; Qi, Z.; Tao, X.; Kundu, S.C.; Lu, S. Sustained Release of Insulin from Silk Microneedles. J. Drug Deliv. Sci. Technol. 2022, 74, 103611. [Google Scholar] [CrossRef]
- Cosman, F.; Lane, N.E.; Bolognese, M.A.; Zanchetta, J.R.; Garcia-Hernandez, P.A.; Sees, K.; Matriano, J.A.; Gaumer, K.; Daddona, P.E. Effect of Transdermal Teriparatide Administration on Bone Mineral Density in Postmenopausal Women. J. Clin. Endocrinol. Metab. 2010, 95, 151–158. [Google Scholar] [CrossRef]
- Pettis, R.J.; Ginsberg, B.; Hirsch, L.; Sutter, D.; Keith, S.; McVey, E.; Harvey, N.G.; Hompesch, M.; Nosek, L.; Kapitza, C.; et al. Intradermal Microneedle Delivery of Insulin Lispro Achieves Faster Insulin Absorption and Insulin Action than Subcutaneous Injection. Diabetes Technol. Ther. 2011, 13, 435–442. [Google Scholar] [CrossRef]
- Pettis, R.J.; Hirsch, L.; Kapitza, C.; Nosek, L.; Hövelmann, U.; Kurth, H.-J.; Sutter, D.E.; Harvey, N.G.; Heinemann, L. Microneedle-Based Intradermal versus Subcutaneous Administration of Regular Human Insulin or Insulin Lispro: Pharmacokinetics and Postprandial Glycemic Excursions in Patients with Type 1 Diabetes. Diabetes Technol. Ther. 2011, 13, 443–450. [Google Scholar] [CrossRef]
- Norman, J.J.; Brown, M.R.; Raviele, N.A.; Prausnitz, M.R.; Felner, E.I. Faster Pharmacokinetics and Increased Patient Acceptance of Intradermal Insulin Delivery Using a Single Hollow Microneedle in Children and Adolescents with Type 1 Diabetes. Pediatr. Diabetes 2013, 14, 459–465. [Google Scholar] [CrossRef]
- Ghosh, T.K. Dermal Drug Delivery: From Innovation to Production; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- Li, W.-Z.; Huo, M.-R.; Zhou, J.-P.; Zhou, Y.-Q.; Hao, B.-H.; Liu, T.; Zhang, Y. Super-Short Solid Silicon Microneedles for Transdermal Drug Delivery Applications. Int. J. Pharm. 2010, 389, 122–129. [Google Scholar] [CrossRef]
- Donnelly, R.F.; Singh, T.R.R.; Alkilani, A.Z.; McCrudden, M.T.C.; O’Neill, S.; O’Mahony, C.; Armstrong, K.; McLoone, N.; Kole, P.; Woolfson, A.D. Hydrogel-Forming Microneedle Arrays Exhibit Antimicrobial Properties: Potential for Enhanced Patient Safety. Int. J. Pharm. 2013, 451, 76–91. [Google Scholar] [CrossRef] [Green Version]
- Baek, C.; Han, M.; Min, J.; Prausnitz, M.R.; Park, J.-H.; Park, J.H. Local Transdermal Delivery of Phenylephrine to the Anal Sphincter Muscle Using Microneedles. J. Control. Release 2011, 154, 138–147. [Google Scholar] [CrossRef]
- Bariya, S.H.; Gohel, M.C.; Mehta, T.A.; Sharma, O.P. Microneedles: An Emerging Transdermal Drug Delivery System. J. Pharm. Pharmacol. 2012, 64, 11–29. [Google Scholar] [CrossRef]
- Quinn, H.L.; Larrañeta, E.; Donnelly, R.F. Dissolving Microneedles: Safety Considerations and Future Perspectives. Ther. Deliv. 2016, 7, 283–285. [Google Scholar] [CrossRef]
- Bediz, B.; Korkmaz, E.; Khilwani, R.; Donahue, C.; Erdos, G.; Falo, L.D.; Ozdoganlar, O.B. Dissolvable Microneedle Arrays for Intradermal Delivery of Biologics: Fabrication and Application. Pharm. Res. 2014, 31, 117–135. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-H.; Prausnitz, M.R. Analysis of Mechanical Failure of Polymer Microneedles by Axial Force. J. Korean Phys. Soc. 2010, 56, 1223. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.-R.; Lee, H.-S.; Choi, I.-J.; Park, J.-H. Considerations in the Use of Microneedles: Pain, Convenience, Anxiety and Safety. J. Drug Target. 2017, 25, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Kettwich, S.C.; Sibbitt, W.L.; Brandt, J.R.; Johnson, C.R.; Wong, C.S.; Bankhurst, A.D. Needle Phobia and Stress-Reducing Medical Devices in Pediatric and Adult Chemotherapy Patients. J. Pediatr. Oncol. Nurs. 2007, 24, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Caffarel-Salvador, E.; Tuan-Mahmood, T.-M.; McElnay, J.C.; McCarthy, H.O.; Mooney, K.; Woolfson, A.D.; Donnelly, R.F. Potential of Hydrogel-Forming and Dissolving Microneedles for Use in Paediatric Populations. Int. J. Pharm. 2015, 489, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Chege, M.; McConville, A.; Davis, J. Microneedle Drug Delivery Systems: Appraising Opportunities for Improving Safety and Assessing Areas of Concern. J. Chem. Health Saf. 2017, 24, 6–14. [Google Scholar] [CrossRef]
- Marshall, S.; Sahm, L.J.; Moore, A.C. Microneedle Technology for Immunisation: Perception, Acceptability and Suitability for Paediatric Use. Vaccine 2016, 34, 723–734. [Google Scholar] [CrossRef]
- Sezgin, B.; Ozel, B.; Bulam, H.; Guney, K.; Tuncer, S.; Cenetoglu, S. The Effect of Microneedle Thickness on Pain During Minimally Invasive Facial Procedures: A Clinical Study. Aesthetic Surg. J. Am. Soc. Aesthetic Plast. Surg. 2014, 34, 757–765. [Google Scholar] [CrossRef]
- Donnelly, R.F.; Mooney, K.; Caffarel-Salvador, E.; Torrisi, B.M.; Eltayib, E.; McElnay, J.C. Microneedle-Mediated Minimally Invasive Patient Monitoring. Ther. Drug Monit. 2014, 36, 10–17. [Google Scholar] [CrossRef]
- Birchall, J.C.; Clemo, R.; Anstey, A.; John, D.N. Microneedles in Clinical Practice–an Exploratory Study into the Opinions of Healthcare Professionals and the Public. Pharm. Res. 2011, 28, 95–106. [Google Scholar] [CrossRef]
- Lee, B.Y.; Bartsch, S.M.; Mvundura, M.; Jarrahian, C.; Zapf, K.M.; Marinan, K.; Wateska, A.R.; Snyder, B.; Swaminathan, S.; Jacoby, E. An Economic Model Assessing the Value of Microneedle Patch Delivery of the Seasonal Influenza Vaccine. Vaccine 2015, 33, 4727–4736. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, R.F.; Moffatt, K.; Alkilani, A.Z.; Vicente-Pérez, E.M.; Barry, J.; McCrudden, M.T.C.; Woolfson, A.D. Hydrogel-Forming Microneedle Arrays Can Be Effectively Inserted in Skin by Self-Application: A Pilot Study Centred on Pharmacist Intervention and a Patient Information Leaflet. Pharm. Res. 2014, 31, 1989–1999. [Google Scholar] [CrossRef]
- Norman, J.J.; Arya, J.M.; McClain, M.A.; Frew, P.M.; Meltzer, M.I.; Prausnitz, M.R. Microneedle Patches: Usability and Acceptability for Self-Vaccination against Influenza. Vaccine 2014, 32, 1856–1862. [Google Scholar] [CrossRef] [Green Version]
- Caffarel-Salvador, E.; Donnelly, R.F. Transdermal Drug Delivery Mediated by Microneedle Arrays: Innovations and Barriers to Success. Curr. Pharm. Des. 2016, 22, 1105–1117. [Google Scholar] [CrossRef]
- Cai, B.; Xia, W.; Bredenberg, S.; Li, H.; Engqvist, H. Bioceramic Microneedles with Flexible and Self-Swelling Substrate. Eur. J. Pharm. Biopharm. 2015, 94, 404–410. [Google Scholar] [CrossRef]
- McCrudden, M.T.C.; Alkilani, A.Z.; Courtenay, A.J.; McCrudden, C.M.; McCloskey, B.; Walker, C.; Alshraiedeh, N.; Lutton, R.E.M.; Gilmore, B.F.; Woolfson, A.D.; et al. Considerations in the Sterile Manufacture of Polymeric Microneedle Arrays. Drug Deliv. Transl. Res. 2015, 5, 3–14. [Google Scholar] [CrossRef]
- Lutton, R.E.M.; Moore, J.; Larrañeta, E.; Ligett, S.; Woolfson, A.D.; Donnelly, R.F. Microneedle Characterisation: The Need for Universal Acceptance Criteria and GMP Specifications When Moving towards Commercialisation. Drug Deliv. Transl. Res. 2015, 5, 313–331. [Google Scholar] [CrossRef] [Green Version]
- Norman, J.J.; Strasinger, C. Scientific Considerations for Microneedle Drug Products: Product Development, Manufacturing, and Quality Control. In Proceedings of the The 4th International Conference on Microneedles, London, UK, 23 May 2016. [Google Scholar]
- Donnelly, R.F.; Woolfson, A.D. Patient Safety and beyond: What Should We Expect from Microneedle Arrays in the Transdermal Delivery Arena? Ther. Deliv. 2014, 5, 653–662. [Google Scholar] [CrossRef]
- McAlister, E.; Kearney, M.-C.; Martin, E.L.; Donnelly, R.F. From the Laboratory to the End-User: A Primary Packaging Study for Microneedle Patches Containing Amoxicillin Sodium. Drug Deliv. Transl. Res. 2021, 11, 2169–2185. [Google Scholar] [CrossRef]
- Indermun, S.; Luttge, R.; Choonara, Y.E.; Kumar, P.; du Toit, L.C.; Modi, G.; Pillay, V. Current Advances in the Fabrication of Microneedles for Transdermal Delivery. J. Control. Release 2014, 185, 130–138. [Google Scholar] [CrossRef]
- Cahill, E.M.; O’Cearbhaill, E.D. Toward Biofunctional Microneedles for Stimulus Responsive Drug Delivery. Bioconjug. Chem. 2015, 26, 1289–1296. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor Types | Factors | Degradation | Microneedle Types |
|---|---|---|---|
| Drug–device interface | Needle bore, material properties, surface morphology, drug formulation | Aggregation, adsorption, unfolding | Hollow, coated, and solid microneedles |
| Drug concentration | Coating and molding formulation | Aggregation | Coated, dissolving, and swelling microneedles |
| Elevated temperature | Material polymerization, transition temperature, drying process | Aggregation, chemical degradation, unfolding | Coated and dissolving microneedles |
| Metal catalysis | Formulation ingredients, microneedle materials | Aggregation, oxidation | Hollow and solid metal microneedles |
| Air exposure | Storage conditions | Aggregation, adsorption, oxidation, unfolding | Coated, dissolving, swelling, and solid microneedles |
| pH | Composition and properties of coating and molding formulation | Aggregation, chemical degradation, unfolding | Coated, dissolving, swelling, and solid microneedles |
| Microneedle Types | Microneedle Processes for Drug Delivery | Advantages | Disadvantages |
|---|---|---|---|
| Solid microneedles | “Poke and patch” technique Microneedle fabrication Preparation of drug formulation Characterization of microneedles Characterization of drug formulation Skin insertion of microneedles Removal of solid microneedles Characterization of microchannels Application of drug formulation on microneedle-treated area Drug permeation study | Mechanically robust microneedlesMicroneedles could be fabricated in harsh conditions and from various materials Simple production Versatile drug formulations Delivery of large doses Use for molecules with high and low potency Possibility of sustained drug delivery | Significant effects of pore closure Complicated two-step application Possible error of misalignment of microneedle treatment and formulation application sites Biosafety risk of microneedle fracture in skin tissue Sharp waste disposal Risk of disease transmission Risk of microneedle reuse Significant drug loss/waste (low fraction of drug delivered) No accurate dosing Thermolabile drugs in liquid or semisolid formulations require cold-chain storage and transportation Slow drug release by diffusion Long wearing time Separate packages for microneedles and formulation |
| Hollow microneedles | “Poke and flow” technique Microneedle fabrication Preparation of drug formulation Characterization of microneedles Characterization of drug formulation Skin insertion of microneedles Injection of drug formulation Characterization of microchannels Drug permeation study | Simple one-step application Microneedles could be fabricated in harsh conditions Convenient production by downscaling hypodermic needlesDelivery of large and accurate doses Controlled rate of drug delivery Use for molecules with high and low potency No requirement for drug reformulation High delivery efficiency | Fabricated from only strong materials to ensure the microneedle robustness Limited microneedle designs Biosafety risk of fracture of weak microneedles in skin tissue Possible bore clogging Possible drug leakage Extended wearing time Risk of microneedle reuse Risk of disease transmission Complex two-component device: microneedles and drug reservoir Drug formulation limited to low-viscosity solution Sharp waste disposal Thermolabile drugs in liquid formulation require cold-chain storage and transportation |
| Coated microneedles | “Coat and poke” technique Fabrication of solid microneedles Preparation of coating formulation Characterization of solid microneedles Characterization of coating formulation Coating drug formulation onto microneedles’ surface Dissolution of coated layer and drug release kinetics Skin insertion of microneedles Characterization of microchannels Drug permeation study | Simple one-step application Improved drug stability in solid form Versatile polymers for coating formulation No requirement for cold-chain storage and transportation Mechanically robust microneedlesNo risk of microneedle reuse Rapid dissolution, fast drug release Short wearing time Precise dosing High delivery efficiency Single product package | Controlled, mild production environment Limited drug-coating quantity and delivery dose Suitable for highly potent molecules Sharp waste disposal Risk of disease transmission Risk of drug dislocation on microneedle array Coating layer affects needle sharpness and skin penetration efficiency Requirement for drug reformulation |
| Dissolving microneedles | “Poke and release” technique Preparation of drug-loaded polymeric formulation Characterization of polymeric formulation Fabrication of drug-loaded microneedles Characterization of dissolving microneedles Dissolution of microneedles and drug release kinetics Skin insertion of microneedles Characterization of microchannels Drug permeation study | Simple one-step application Improved drug stability in solid form No requirement for cold-chain storage and transportation No risk of microneedle reuse No risk of disease transmission No sharp waste Short wearing time Microneedle dissolution depends on formulation and materials Possibility of bolus or sustained drug release and delivery Minimal drug loss during fabrication and application Precise dosing High delivery efficiency Single product package | Limited range of materials with sufficient mechanical strength, biocompatibility, and biodegradability Limited drug-loading quantity and delivery dose Suitable for highly potent molecules Drug payload affects microneedles’ mechanical strength and sharpness Requirement for drug reformulation |
| Swelling microneedles | “Poke and swell” technique Fabrication of swelling microneedles Preparation of drug formulation Characterization of swelling microneedles Characterization of drug formulation Drug release kinetics from the reservoir Skin insertion of drug-reservoir-assembled swelling microneedles Characterization of microchannels Drug permeation study | Simple one-step application Improved drug stability in solid form No requirement for cold-chain storage and transportation No risk of microneedle reuse No risk of disease transmission No sharp waste No biosafety risk Delivery of large doses Microneedles’ mechanical strength and sharpness unaffected by the drug payload Use for molecules with high and low potency Single product package | Limited range of swelling materials Requirement for drug reformulation Low delivery efficiency, low fraction of drug delivered No accurate dosing Slow drug release by diffusion Long wearing time |
| NCT No. | Clinical Trial | Condition and Diseases | Drug and Device | Phase | Location | Status |
|---|---|---|---|---|---|---|
| NCT00837512 | Insulin delivery using microneedles in type 1 diabetes | Type 1 diabetes mellitus | Device: hollow microneedle (1 mm) Device: subcutaneous (SC) insulin catheter | II, III | Emory University (USA) | Completed |
| NCT02837094 | Enhanced Epidermal Antigen-Specific Immunotherapy Trial-1 (EE-ASI-1) | Type 1 diabetes | Drug: C19-A3 GNP (MicronJet 600) | I | Cardiff University | Unknown |
| NCT02329457 | VZV Vaccine for Hematopoietic Stem Cell Transplantation (VZIDST) | Varicella Zoster infection | Biological: Zostavax | II, III | The University of Hong Kong | Completed |
| NCT03274674 | Use of Injectable-Platelet-Rich-Fibrin (I-PRF) to Thicken Gingival Phenotype | Periodontoclasiagingiva; injury condition blood clot gingiva disorder | Other: I-PRF | NA | Bezmialem Vakif University (Turkey) | Completed |
| NCT00602914 | A pilot study to assess the safety, PK, and PD of insulin injected via MicronJet or conventional needles | Diabetes mellitus | Device: MicronJet Device: conventional needle (NanoPass microneedle) | Early Phase I | NanoPass Technologies Ltd. | Completed |
| NCT02459938 | Safety and Efficacy of ZP-Glucagon to Injectable Glucagon for Hypoglycemia | Hypoglycemia | Solid/metal (drug-coated titanium microneedles) Zosano microneedle patch | I | Nucleus Network (Australia) | Completed |
| NCT00489918 | Dose-ranging study—Macroflux parathyroid hormone (PTH) in postmenopausal women with osteoporosis | Osteoporosis | Drug: Teriparatide (Zosano Pharma) | II | Zosano Pharma Corporation | Completed |
| NCT02478879 | A study to determine the patient preference between Zosano Pharma parathyroid hormone (ZP-PTH) patch and the Forteo pen | Postmenopausal osteoporosis | Coated titanium (ZP-PTH microneedle patch) | I | Covance Daytona Beach Clinical Research Unit (USA) | Completed |
| NCT01674621 | Phase 2 study of BA058 (Abaloparatide) transdermal delivery in postmenopausal women with osteoporosis | Postmenopausal osteoporosis | Drug: BA058 placebo Drug: BA058 TD (50, 100, 150 µg) Drug: BA058 injection (80 µg) (TD: coated 3M microstructured transdermal system (MTS), 250 µm, 316 microprojections) | II | Radius Health, Inc. | Completed |
| NCT03607903 | Adalimumab microneedles in healthy volunteers | Pain injection site | Biological: Adalimumab ID or SC Biological: Adalimumab SC Other: saline ID or SC (3M hMTS, 1500 µm, 12 needles) | I, II | Centre for Human Drug Research (Netherlands) | Completed |
| NCT03054480 | Fractional Micro-Needle Radiofrequency and I Botulinum Toxin A for Primary Axillary Hyperhidrosis | Primary axillary hyperhidrosis | Device: fractional microneedle radiofrequency Drug: botulinum toxin type A | NA | Thep Chalermchai, Mae Fah Luang, University Hospital | Completed |
| NCT03126786 | Suprachoroidal CLS-TA With Intravitreal Aflibercept Versus Aflibercept Alone in Subject with Diabetic Macular Edema | Diabetic macular edema | IVT aflibercept, Sham SC, SC CLS-TA | II | Clearside Biomedical, Inc. | Completed |
| NCT03203174 | The use of microneedles with topical botulinum toxin for the treatment of palmar hyperhidrosis | Hyperhidrosis | Solid (Sham microneedle) Botulinum toxin type A | I | University of California, Davis | Completed |
| NCT01684956 | Pharmacokinetic comparison of intradermal versus subcutaneous insulin and glucagon delivery in type 1 diabetes | Type 1 diabetes | Hollow (MicronJet™) | II | Massachusetts General Hospital (USA) | Unknown |
| NCT01557907 | Multi-day (three) in-patient evaluation of intradermal versus subcutaneous basal and bolus insulin infusion | Diabetes | Hollow (BD research catheter) | I/II | Profil Institut fur Stoffwechselfforschung GmbH (Germany) | Completed |
| NCT01120444 | Study on the effects on blood glucose following intradermal and subcutaneous dosing of insulin in diabetic patients | Diabetes | Hollow (BD research catheter) | I/II | Profil Institute of Clinical Research (Germany) | Completed |
| NCT01061216 | Pharmacokinetics/dynamics of basal (continuous) insulin infusion administered either intradermally or subcutaneously | Diabetes Mellitus, Type 1/2 | Hollow (BD research catheter) | I/II | Profil Institut fur Stoffwechselfforschung GmbH (Germany) | Completed |
| NCT00553488 | Feasibility Study of the Effect of Intra-Dermal Insulin Injection on Blood Glucose Levels After Eating | Diabetes mellitus, type 1 | BD research catheter (34G × 1.5 mm needle) Insulin | II | Profil Institut fur Stoffwechselfforschung GmbH (Germany) | Completed |
| NCT01518478 | Atopic Dermatitis Research Network (ADRN) Influenza Vaccine Pilot | Atopic dermatitis | Fluzone® intradermal | I | National Institute of Allergy and Infectious Diseases (USA) | Completed |
| NCT01737710 | Atopic Dermatitis Research Network (ADRN) Influenza Vaccine Study | Atopic dermatitis | Fluzone® intradermal vaccine Fluzone® (intramuscular) vaccine | I | National Institute of Allergy and Infectious Diseases (USA) | Completed |
| NCT04064411 | Efficacy and Safety of Abaloparatide-Solid Microstructured Transdermal System in Postmenopausal Women With Osteoporosis | Postmenopausal osteoporosis | Abaloparatide solid microstructured transdermal system; abaloparatide-SC | III | Radius Health, Inc. | Completed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, H.X.; Nguyen, C.N. Microneedle-Mediated Transdermal Delivery of Biopharmaceuticals. Pharmaceutics 2023, 15, 277. https://doi.org/10.3390/pharmaceutics15010277
Nguyen HX, Nguyen CN. Microneedle-Mediated Transdermal Delivery of Biopharmaceuticals. Pharmaceutics. 2023; 15(1):277. https://doi.org/10.3390/pharmaceutics15010277
Chicago/Turabian StyleNguyen, Hiep X., and Chien N. Nguyen. 2023. "Microneedle-Mediated Transdermal Delivery of Biopharmaceuticals" Pharmaceutics 15, no. 1: 277. https://doi.org/10.3390/pharmaceutics15010277
APA StyleNguyen, H. X., & Nguyen, C. N. (2023). Microneedle-Mediated Transdermal Delivery of Biopharmaceuticals. Pharmaceutics, 15(1), 277. https://doi.org/10.3390/pharmaceutics15010277