

Photodynamic Therapy, Photobiomodulation and Acetonide Triamcinolone 0.1% in the Treatment of Oral Lichen Planus: A Randomized Clinical Trial


 , , and
, , and 
Abstract
:1. Introduction
2. Material and Methods
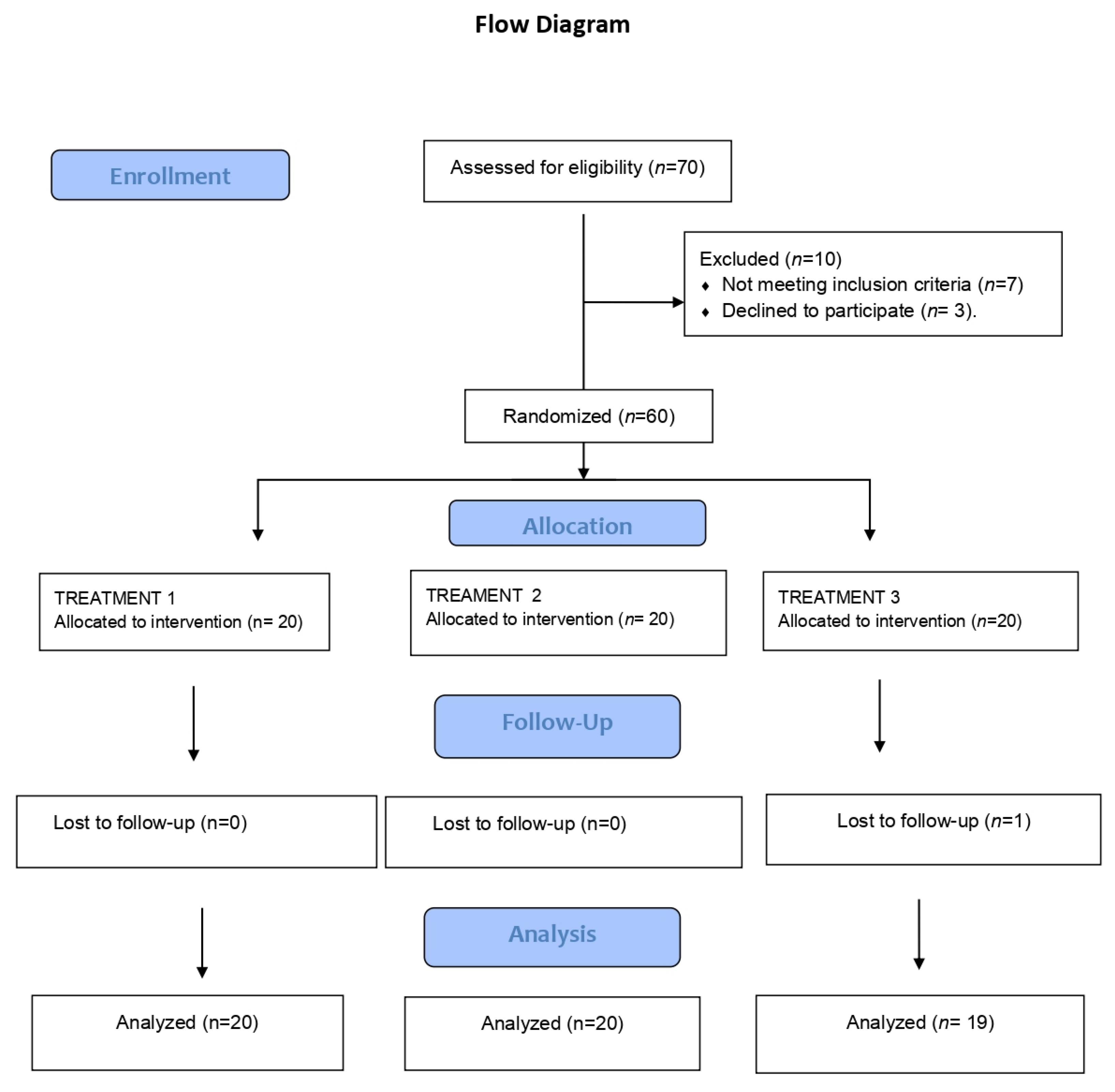
2.1. Study Population
2.2. Study Design
- -
- Group 1: Patients with OLP subjected to photodynamic therapy (Helbo® blue photosensitizer with low-power laser irradiation) applied once a week for 4 sessions, with orabase cream application three times a day at home.
- -
- Group 2: Patients with OLP subjected to low-power laser irradiation applied once a week for 4 sessions, with orabase cream application three times a day.
- -
- Group 3: Patients with OLP subjected to inactive laser application once a week for 4 sessions with triamcinolone acetonide orabase cream 0.1% applied three times a day.
2.3. Application of Laser Phototherapy
2.4. Study Variables
- -
- Visit 1 (day 1): Thongprasom + VAS + OHIP-14 + HAD + treatment according to group
- -
- Visits 2 (day 7), 3 (day 14), and 4 (day 21): VAS + laser + treatment according to group
- -
- Visit 5 (1 month after the last visit): follow-up period with Thongprasom + VAS + OHIP-14 + HAD
- -
- Visit 6 (3 months after the fourth visit): follow-up period with VAS + OHIP-14 + HAD
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carrozzo, M.; Porter, S.; Mercadante, V.; Fedele, S. Oral lichen planus: A disease or a spectrum of tissue reactions? Types, causes, diagnostic algorhythms, prognosis, management strategies. Periodontol. 2000 2019, 80, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Tang, X.; Zheng, X.; Ge, S.; Wen, H.; Lin, X.; Chen, Z.; Lu, L. Global Prevalence and Incidence Estimates of Oral Lichen Planus: A Systematic Review and Meta-analysis. JAMA Dermatol. 2020, 156, 172–181. [Google Scholar] [CrossRef] [PubMed]
- García-Pola, M.J.; González-Álvarez, L.; Garcia-Martin, J.M. Treatment of oral lichen planus. Systematic review and therapeutic guide. Med. Clin. (Barc.) 2017, 149, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Lodi, G.; Manfredi, M.; Mercadante, V.; Murphy, R.; Carrozzo, M. Interventions for treating oral lichen planus: Corticosteroid therapies. Cochrane Database Syst Rev. 2020, 2, CD001168. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, P.; De, D.; Handa, S.; Narang, T.; Saikia, U.N. A prospective observational study to compare efficacy of topical triamcinolone acetonide 0.1% oral paste, oral methotrexate, and a combination of topical triamcinolone acetonide 0.1% and oral methotrexate in moderate to severe oral lichen planus. Dermatol. Ther. 2018, 31, e12563. [Google Scholar] [CrossRef]
- Thongprasom, K.; Luangjarmekorn, L.; Sererat, T.; Taweesap, W. Relative efficacy of fluocinolone acetonide compared with triamcinolone acetonide in treatment of oral lichen planus. J. Oral Pathol. Med. 1992, 21, 456–458. [Google Scholar] [CrossRef]
- Akram, Z.; Javed, F.; Hosein, M.; Al-Qahtani, M.A.; Alshehri, F.; Alzahrani, A.I.; Vohra, F. Photodynamic therapy in the treatment of symptomatic oral lichen planus: A systematic review. Photodermatol. Photoimmunol. Photomed. 2018, 34, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Al-Maweri, S.A.; Ashraf, S.; Kalakonda, B.; Halboub, E.; Petro, W.; AlAizari, N.A. Efficacy of photodynamic therapy in the treatment of symptomatic oral lichen planus: A systematic review. J. Oral Pathol. Med. 2018, 47, 326–332. [Google Scholar] [CrossRef]
- Łukaszewska-Kuska, M.; Ślebioda, Z.; Dorocka-Bobkowska, B. The effectiveness of topical forms of dexamethasone in the treatment of oral lichen planus—A systematic review. Oral Dis. 2021, 28, 2063–2071. [Google Scholar] [CrossRef]
- He, Y.; Deng, J.; Zhao, Y.; Tao, H.; Dan, H.; Xu, H.; Chen, Q. Efficacy evaluation of photodynamic therapy for oral lichen planus: A systematic review and meta-analysis. BMC Oral Health 2020, 20, 302. [Google Scholar] [CrossRef]
- Sadaksharam, J.; Nayaki, K.P.; Panneer Selvam, N. Treatment of oral lichen planus with methylene blue mediated photodynamic therapy—A clinical study. Photodermatol. Photoimmunol. Photomed. 2012, 28, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, D.; Moussa, E.; Alnouaem, M. Evaluation of photodynamic therapy in treatment of oral erosive lichen planus in comparison with topically applied corticosteroids. Photodiagn. Photodyn. Ther. 2017, 19, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Mirza, S.; Rehman, N.; Alrahlah, A.; Alamri, W.R.; Vohra, F. Efficacy of photodynamic therapy or low level laser therapy against steroid therapy in the treatment of erosive-atrophic oral lichen planus. Photodiagnosis Photodyn. Ther. 2018, 21, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Sulewska, M.; Duraj, E.; Sobaniec, S.; Graczyk, A.; Milewski, R.; Wroblewska, M.; Pietruski, J.; Pietruska, M. A clinical evaluation of efficacy of photodynamic therapy in treatment of reticular oral lichen planus: A case series. Photodiagn. Photodyn. Ther. 2019, 25, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Jajarm, H.H.; Falaki, F.; Sanatkhani, M.; Ahmadzadeh, M.; Ahrari, F.; Shafaee, H. A comparative study of toluidine blue-mediated photodynamic therapy versus topical corticosteroids in the treatment of erosive-atrophic oral lichen planus: A randomized clinical controlled trial. Lasers Med. Sci. 2015, 30, 1475–1480. [Google Scholar] [CrossRef] [PubMed]
- Sobaniec, S.; Bernaczyk, P.; Pietruski, J.; Cholewa, M.; Skurska, A.; Dolińska, E.; Duraj, E.; Tokajuk, G.; Paniczko, A.; Olszewska, E.; et al. Clinical assessment of the efficacy of photodynamic therapy in the treatment of oral lichen planus. Lasers Med. Sci. 2013, 28, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Bakhtiari, S.; Mojahedi, S.M.; Azari-Marhabi, S.; Namdari, M.; Rankohi, Z.E. Comparing clinical effects of photodynamic therapy as a novel method with topical corticosteroid for treatment of oral lichen planus. Photodiagn. Photodyn. Ther. 2017, 20, 159–164. [Google Scholar] [CrossRef]
- Aghahosseini, F.; Arbabi-Kalati, F.; Fashtami, L.A.; Djavid, G.E.; Fateh, M.; Beitollahi, J.M. Methylene blue-mediated photodynamic therapy: A possible alternative treatment for oral lichen planus. Lasers Surg. Med. 2006, 38, 33–38. [Google Scholar] [CrossRef]
- Maloth, K.N.; Velpula, N.; Kodangal, S.; Sangmesh, M.; Vellamchetla, K.; Ugrappa, S.; Meka, N. Photodynamic Therapy—A Non-invasive Treatment Modality for Precancerous Lesions. J. Lasers Med. Sci. 2016, 7, 30–36. [Google Scholar] [CrossRef]
- Lavaee, F.; Shadmanpour, M. Comparison of the effect of photodynamic therapy and topical corticosteroid on oral lichen planus lesions. Oral Dis. 2019, 25, 1954–1963. [Google Scholar] [CrossRef]
- Saleh, W.; Tageldin, S.; Khashaba, E.; Darwish, M.; Elnagdy, S.; Khashaba, O. Could photodynamic therapy be utilized as a treatment modality for oral lichen planus? Photodiagn. Photodyn. Ther. 2020, 30, 101677. [Google Scholar] [CrossRef] [PubMed]
- Cosgarea, R.; Pollmann, R.; Sharif, J.; Schmidt, T.; Stein, R.; Bodea, A.; Auschill, T.; Sculean, A.; Eming, R.; Greene, B.; et al. Photodynamic therapy in oral lichen planus: A prospective case-controlled pilot study. Sci. Rep. 2020, 10, 1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jajarm, H.H.; Falaki, F.; Mahdavi, O. A comparative pilot study of low intensity laser versus topical corticosteroids in the treatment of erosive-atrophic oral lichen planus. Photomed. Laser Surg. 2011, 29, 421–425. [Google Scholar] [CrossRef] [PubMed]
- El Shenawy, H.M.; Eldin, A.M. A comparative evaluation of low-level laser and topical steroid therapies for the treatment of erosive atrophic lichen planus. Open Access Maced J. Med. Sci. 2015, 3, 462–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, E.P.; Cunha, K.R.L.; Abboud, C.S.; de Barros Gallo, C.; de Sousa Sobral, S.; de Fatima Teixeira da Silva, D.; Horliana, A.C.R.T.; Franco, A.L.; Rodrigues, M.F.S.D. Photobiomodulation is effective in oral lichen planus: A randomized, controlled, double-blind study. Oral Dis. 2021, 27, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Dillenburg, C.S.; Martins, M.A.; Munerato, M.C.; Marques, M.M.; Carrard, V.C.; Sant’Ana Filho, M.; Castilho, R.M.; Martins, M.D. Efficacy of laser phototherapy in comparison to topical clobetasol for the treatment of oral lichen planus: A randomized controlled trial. J. Biomed. Opt. 2014, 19, 068002. [Google Scholar] [CrossRef]
- van der Meij, E.H.; van der Waal, I. Lack of clinicopathologic correlation in the diagnosis of oral lichen planus based on the presently available diagnostic criteria and suggestions for modifications. J. Oral Pathol. Med. 2003, 32, 507–512. [Google Scholar] [CrossRef]
- Montero-Martin, J.; Bravo-Pérez, M.; Albaladejo-Martínez, A.; Hernández-Martin, L.A.; Rosel-Gallardo, E.M. Validation the Oral Health Impact Profile (OHIP-14sp) for adults in Spain. Med. Oral Patol. Oral Cir. Bucal 2009, 14. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Hesse, J.; Schmalfuss, A.; Kvaal, S.I. Photodynamic therapy of oral lichen planus. Photochem. Photobiol. Sci. 2020, 19, 1271–1279. [Google Scholar] [CrossRef]
- Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 348–364. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kędzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy—Mechanisms, photosensitizers and combinations. Biomed. Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef]
- Othman, N.A.; Shaker, O.G.; Elshenawy, H.M.; Abd-Elmoniem, W.; Eldin, A.M.; Fakhr, M.Y. The effect of diode laser and topical steroid on serum level of TNF-alpha in oral lichen planus patients. J. Clin. Exp. Dent. 2016, 8, e566–e570. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Khandelwal, S.; Sinha, N.; Kaswan, S.; Rahman, F.; Tipu, S. Treatment modalities of oral lichen planus: An update. J. Oral Diagn. 2016, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- López-Jornet, P.; Camacho-Alonso, F. Quality of life in patients with oral lichen planus. J. Eval. Clin. Pract. 2010, 16, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Adamo, D.; Ruoppo, E.; Leuci, S.; Aria, M.; Amato, M.; Mignogna, M.D. Sleep disturbances, anxiety and depression in patients with oral lichen planus: A case-control study. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 291–297. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Treatment | Test | p-Value | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| Age | 60.7 (9.7) | 63.5 (9.5) | 61.3 (11.1) | 57.2 (7.7) | F(2;56) = 2.16 | 0.125 |
| Gender | χ2(2) = 4.10 | 0.128 | ||||
| Male | 8 (13.6) | 1 (5.0) | 2 (10.0) | 5 (26.3) | ||
| Female | 51 (86.4) | 19 (95.0) | 18 (90.0) | 14 (73.7) | ||
| Smoking | χ2(4) = 8.52 | 0.074 | ||||
| Yes | 6 (10.2) | 1 (5.0) | 1 (5.0) | 4 (21.1) | ||
| Ex-smoker | 11 (18.6) | 7 (35.0) | 2 (10.0) | 2 (10.5) | ||
| Non-smoker | 41 (71.2) | 12 (60.0) | 17 (85.0) | 13 (68.4) | ||
| Alcohol | χ2(6) = 10.49 | 0.106 | ||||
| No | 37 (62.7) | 14 (70.0) | 15 (75.0) | 8 (42.1) | ||
| 1 glass/w | 14 (23.7) | 5 (25.0) | 4 (20.0) | 5 (26.3) | ||
| 2–3 glasses/w | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Social drinker | 8 (13.6) | 1 (5.0) | 1 (5.0) | 6 (31.6) | ||
| Duration of OLP (years) | 4 (3.4) | 4.8 (4.3) | 3.8 (3.4) | 2.5 (1.7) | F(2;56) = 2.26 | 0.114 |
| Location lesions | χ2(6) = 5.51 | 0.48 | ||||
| Others | 5 (8.5) | 2 (10.0) | 3 (15.0) | 0 (0.0) | ||
| Buccal mucosa | 33 (55.9) | 9 (45.0) | 10 (50.0) | 14 (73.7) | ||
| Gums | 15 (25.4) | 6 (30.0) | 5 (25.0) | 4 (21.1) | ||
| Tongue | 6 (10.2) | 3 (15.0) | 2 (10.0) | 1 (5.3) | ||
| CLINICAL LESIONS | χ2(4) = 2.447 | 0.654 | ||||
| Reticular | 25 (42.4) | 7 (35.0) | 10 (50.0) | 8 (42.1) | ||
| Atrophic | 20 (33.9) | 6 (30.0) | 7 (35.0) | 7 (36.8) | ||
| Erosive | 14 (23.7) | 7 (35.0) | 3 (15.0) | 4 (21.1) | ||
| Visit, Mean (SD) | Within-Subject Effects † | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | Visit | Treatment * Visit | |
| F(df); p-Value (η2) | F(df); p-Value (η2) | |||||||
| PAIN SCALE | F(5;275) = 46.14; p < 0.001 (0.456) | F(10;275) = 5.80; p < 0.001 (0.174) | ||||||
| Treat. 1 | 6.70 (3.44) | 5.65 (3.07) | 4.30 (2.83) | 2.80 (1.94) | 1.95 (1.79) | 2.05 (2.28) | ||
| Treat. 2 | 6.50 (2.86) | 5.50 (2.72) | 4.25 (2.71) | 3.25 (2.57) | 3.10 (2.17) | 3.20 (2.38) | ||
| Treat. 3 | 4.94 (3.02) | 4.17 (2.50) | 3.33 (2.06) | 2.83 (2.12) | 3.61 (2.93) | 4.06 (2.98) | ||
| Total | 6.09 (3.16) | 5.14 (2.81) | 3.98 (2.57) | 2.97 (2.20) | 2.86 (2.39) | 3.07 (2.64) | ||
| Visit | Difference in Means (p-Value) | ||
|---|---|---|---|
| Treatment 1 | Treatment 2 | Treatment 3 | |
| 1-2 | 1.05 (0.006) | 1.00 (0.011) | 0.77 (0.162) |
| 1-3 | 2.40 (<0.001) | 2.25 (<0.001) | 1.61 (0.029) |
| 1-4 | 3.90 (<0.001) | 3.25 (<0.001) | 2.11 (0.001) |
| 1-5 | 4.75 (<0.001) | 3.40 (<0.001) | 1.33 (0.272) |
| 1-6 | 4.65 (<0.001) | 3.30 (<0.001) | 0.88 (1) |
| 2-3 | 1.35 (0.012) | 1.25 (0.026) | 0.83 (0.632) |
| 2-4 | 2.85 (<0.001) | 2.25 (<0.001) | 1.33 (0.095) |
| 2-5 | 3.70 (<0.001) | 2.40 (0.001) | 0.55 (1) |
| 2-6 | 3.60 (<0.001) | 2.30 (0.009) | 0.11 (1) |
| 3-4 | 1.50 (<0.001) | 1.00 (0.044) | 0.5 (1) |
| 3-5 | 2.35 (<0.001) | 1.15 (0.047) | −0.2 (1) |
| 3-6 | 2.25 (0.001) | 1.05 (0.048) | −0.7 (1) |
| 4-5 | 0.85 (0.143) | 0.15 (1) | −0.7 (0.352) |
| 4-6 | 0.75 (1) | 0.05 (1) | −1.2 (0.223) |
| 5-6 | −0.1 (1) | −0.1 (1) | −0.4 (1) |
| Visit, Mean (SD) | Within-Subject Effects † | ||||
|---|---|---|---|---|---|
| Initial (1) | 1 Month (2) | 3 Months (3) | Visit | Treatment * visit | |
| F(df); p-Value (eta2) | F(df); p-Value (eta2) | ||||
| OHIP-14 | F(2;110) = 46.20; p < 0.001 (0.457) | F(4;110) = 2.53; p = 0.046 (0.088) | |||
| Treat. 1 | 18.05 (9.43) | 12.75 (7.17) | 9.10 (5.21) | ||
| Treat. 2 | 22.55 (9.12) | 17.50 (9.22) | 14.30 (7.95) | ||
| Treat. 3 | 25.94 (12.35) | 23.94 (12.26) | 22.06 (12.15) | ||
| Total | 22.05 (10.64) | 17.86 (10.54) | 14.91 (10.11) | ||
| Anxiety | F(2;110) = 25.75; p < 0.001 (0.319) | F(4;110) = 4.39; p = 0.002 (0.138) | |||
| Treat. 1 | 12.35 (3.79) | 9.05 (5.28) | 7.20 (4.23) | ||
| Treat. 2 | 12.55 (3.53) | 9.05 (2.56) | 6.60 (4.37) | ||
| Treat. 3 | 10.94 (3.40) | 11.06 (3.64) | 10.17 (3.37) | ||
| Total | 11.98 (3.59) | 9.67 (4.04) | 7.91 (4.25) | ||
| Depression | F(2;110) = 9.74; p < 0.001 (0.151) | F(4;110) = 0.67; p = 0.615 (0.024) | |||
| Treat. 1 | 4.85 (5.06) | 4.55 (4.92) | 4.25 (4.44) | ||
| Treat. 2 | 4.00 (2.36) | 3.70 (2.36) | 3.40 (2.23) | ||
| Treat. 3 | 6.00 (4.02) | 5.87 (3.43) | 5.33 (2.98) | ||
| Total | 4.91 (3.98) | 4.71 (3.75) | 4.33 (3.35) | ||
| Follow-Up | Difference in Means (p-Value) | ||
|---|---|---|---|
| Treat. 1 | Treat. 2 | Treat. 3 | |
| OHIP-14 Initial-1 month | 5.30 (<0.001) | 5.05 (<0.001) | 2 (0.363) |
| Initial-3 months | 8.95 (<0.001) | 8.25 (<0.001) | 3.88 (0.065) |
| 1 month-3 months | 3.65 (0.003) | 3.20 (0.01) | 1.88 (0.27) |
| Anxiety Initial-1 month | 3.30 (0.001) | 3.50 (<0.001) | −0.11 (1) |
| Initial-3 months | 5.15 (<0.001) | 5.95 (<0.001) | 0.77 (1) |
| 1 month-3 months | 1.85 (0.044) | 2.45 (0.029) | 0.88 (1) |
| Depression Initial-1 month | 0.3 (0.449) | 0.3 (0.449) | 0.13 (0.388) |
| Initial-3 months | 0.6 (0.385) | 0.6 (0.385) | 0.67 (0.119) |
| 1 month-3 months | 0.3 (0.95) | 0.3 (0.95) | 0.54 (0.303) |
| Visit | Difference in Means (p-Value) | ||
|---|---|---|---|
| Treat. 1 vs. Treat. 2 | Treat. 1 vs. Treat. 3 | Treat. 2 vs. Treat. 3 | |
| OHIP-14 Initial | −4.50 (0.521) | 7.89 (0.066) | −3.39 (0.948) |
| 1 month | −4.75 (0.379) | −11.19 (0.002) | −6.44 (0.135) |
| 3 Months | −5.20 (0.198) | −12.96 (<0.001) | −7.76 (0.026) |
| Anxiety Initial | −0.20 (1) | 1.41 (0.698) | 1.61 (0.521) |
| 1 month | 0.00 (1) | −2.01 (0.385) | −2.01 (0.385) |
| 3 months | 0.60 (1) | −2.97 (0.083) | −3.57 (0.026) |
| Depression Initial | 0.85 (1) | −1.15 (1) | −2.00 (0.38) |
| 1 month | 0.85 (1) | −1.12 (1) | −1.97 (0.331) |
| 3 months | 0.85 (1) | −0.58 (1) | −1.43 (0.582) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salinas-Gilabert, C.; Gómez García, F.; Galera Molero, F.; Pons-Fuster, E.; Vander Beken, S.; Lopez Jornet, P. Photodynamic Therapy, Photobiomodulation and Acetonide Triamcinolone 0.1% in the Treatment of Oral Lichen Planus: A Randomized Clinical Trial. Pharmaceutics 2023, 15, 30. https://doi.org/10.3390/pharmaceutics15010030
Salinas-Gilabert C, Gómez García F, Galera Molero F, Pons-Fuster E, Vander Beken S, Lopez Jornet P. Photodynamic Therapy, Photobiomodulation and Acetonide Triamcinolone 0.1% in the Treatment of Oral Lichen Planus: A Randomized Clinical Trial. Pharmaceutics. 2023; 15(1):30. https://doi.org/10.3390/pharmaceutics15010030
Chicago/Turabian StyleSalinas-Gilabert, Carmen, Francisco Gómez García, Fe Galera Molero, Eduardo Pons-Fuster, Seppe Vander Beken, and Pia Lopez Jornet. 2023. "Photodynamic Therapy, Photobiomodulation and Acetonide Triamcinolone 0.1% in the Treatment of Oral Lichen Planus: A Randomized Clinical Trial" Pharmaceutics 15, no. 1: 30. https://doi.org/10.3390/pharmaceutics15010030
APA StyleSalinas-Gilabert, C., Gómez García, F., Galera Molero, F., Pons-Fuster, E., Vander Beken, S., & Lopez Jornet, P. (2023). Photodynamic Therapy, Photobiomodulation and Acetonide Triamcinolone 0.1% in the Treatment of Oral Lichen Planus: A Randomized Clinical Trial. Pharmaceutics, 15(1), 30. https://doi.org/10.3390/pharmaceutics15010030