
Development of an Oral Liquid Formulation of Nicardipine Hydrochloride Compounded with Simple Excipients for the Treatment of Pediatric Hypertension
 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Analytical Method
2.2.1. Chromatographic Conditions
2.2.2. Sample Preparation
2.3. Retrospective Analysis of Patients Treated with Nicardipine 2 mg/mL Oral Formulation
2.4. Pre-Formulation
2.4.1. Excipients
2.4.2. Efficacy of Antimicrobial Preservation
2.5. Characterization of the Final Formulation
2.5.1. Light Microscopy
2.5.2. Uniformity of Content
2.6. Stability Study
2.6.1. Chemical Stability
2.6.2. Physical Stability
2.6.3. Microbiological Study
- Method validation
- 2.
- Microbiological stability
2.7. Uniformity and Accuracy of Delivered Doses from Multidose Bottles
2.8. Data Analysis
3. Results
3.1. Retrospective Analysis of Patients Treated with Nicardipine Hydrochloride 2 mg/mL Oral Formulation
3.2. Pre-Formulation
3.2.1. Selection of Excipients
3.2.2. Efficacy of Antimicrobial Preservation
3.2.3. Final Formulation
3.3. Characterization of the Final Formulation
3.3.1. Light Microscopy
3.3.2. Uniformity of Content
3.4. Stability Study
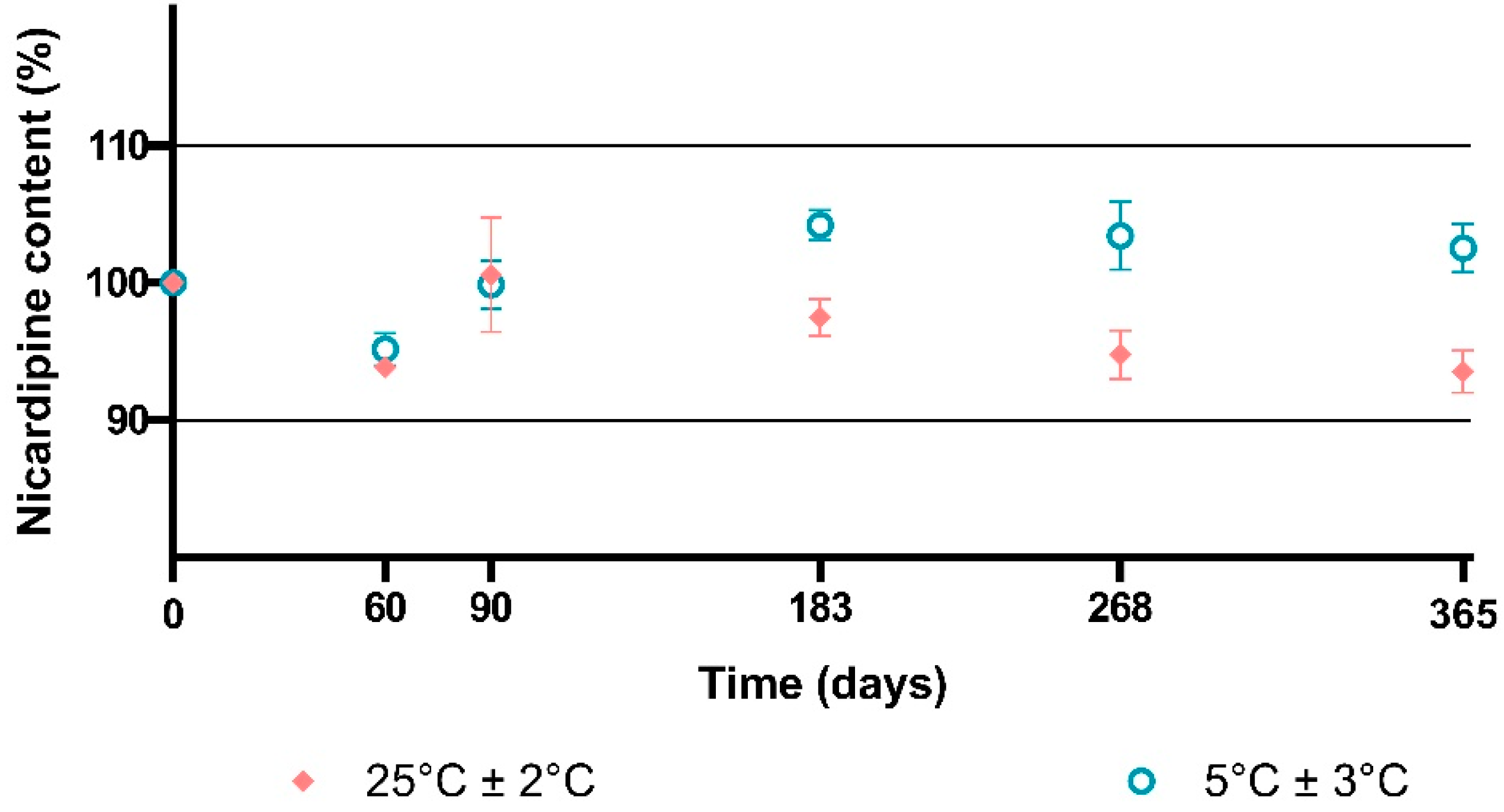
3.4.1. Chemical Stability
- Long-term storage conditions
- 2.
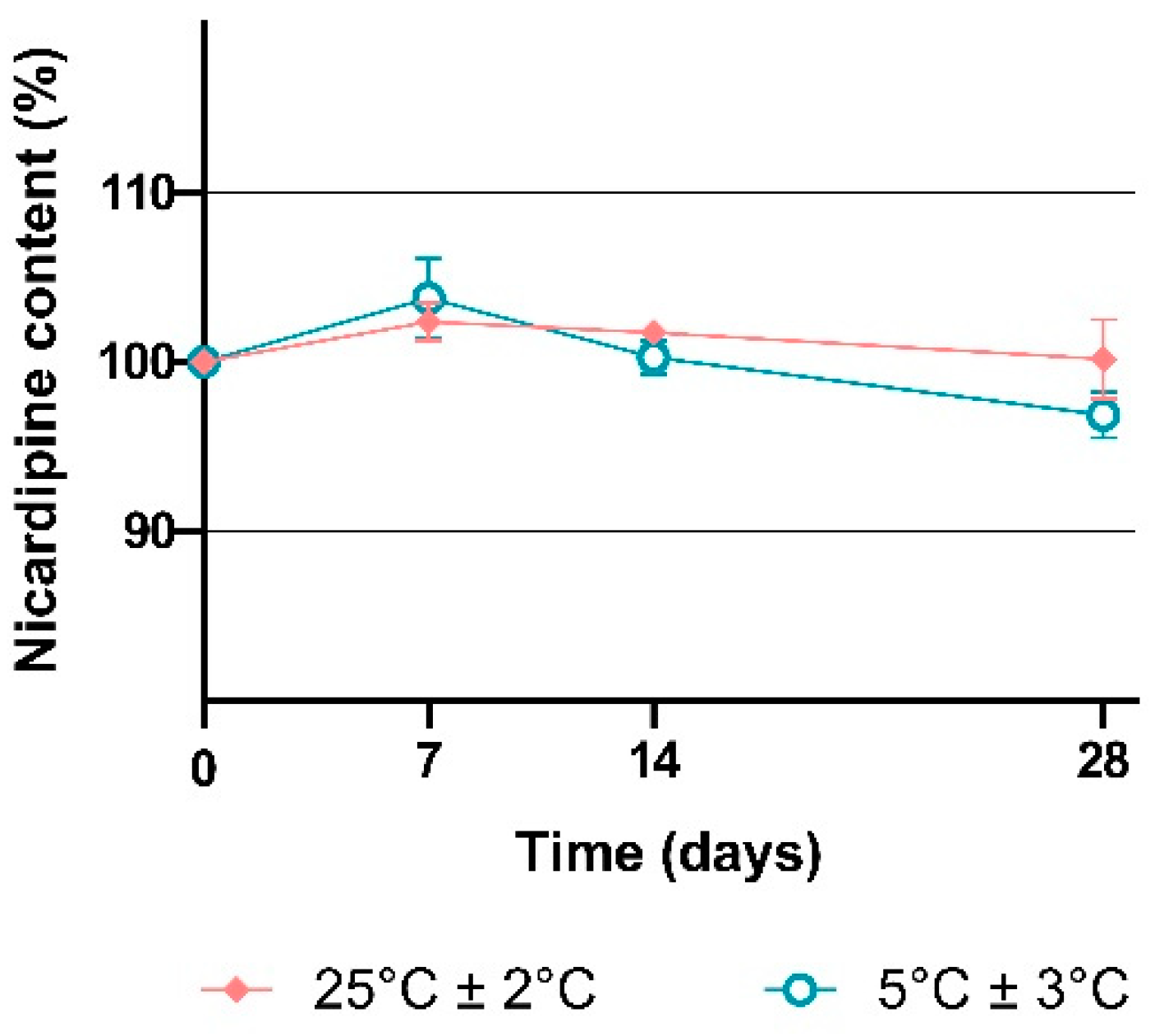
- In-use conditions
3.4.2. Physical Stability
3.4.3. Microbiological Study
3.5. Uniformity and Accuracy of Delivered Doses from Multidose Bottles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- del Moral-Sanchez, J.-M.; Gonzalez-Alvarez, I.; Gonzalez-Alvarez, M.; Navarro-Ruiz, A.; Bermejo, M. Availability of Authorizations from EMA and FDA for Age-Appropriate Medicines Contained in the WHO Essential Medicines List for Children 2019. Pharmaceutics 2020, 12, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Riet-Nales, D.A.; de Jager, K.E.; Schobben, A.F.; Egberts, T.C.; Rademaker, C.M. The Availability and Age-Appropriateness of Medicines Authorized for Children in the Netherlands. Br. J. Clin. Pharm. 2011, 72, 465–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, C. Pediatric Hypertension. Prim. Care Clin. Off. Pract. 2021, 48, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.S.; Samuel, J.P.; Samuels, J.A. Prevalence of Hypertension in Children. Hypertension 2019, 73, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.T.; Kaelber, D.C.; Baker-Smith, C.M.; Blowey, D.; Carroll, A.E.; Daniels, S.R.; de Ferranti, S.D.; Dionne, J.M.; Falkner, B.; Flinn, S.K.; et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics 2017, 140, e20171904. [Google Scholar] [CrossRef] [Green Version]
- Polli, J.E.; Yu, L.X.; Mehta, M.U.; Amidon, G.L.; Zhao, H.; Lesko, L.J.; Chen, M.-L.; Lee, V.H.L.; Shah, V.P.; Conner, D.P.; et al. Biopharmaceutics Classification System: The Scientific Basis for Biowaiver Extensions. Pharm. Res. 2002, 19, 921–925. [Google Scholar] [CrossRef] [Green Version]
- Maurin, M.B.; Rowe, S.M.; Koval, C.A.; Hussain, M.A. Solubilization of Nicardipine Hydrochloride via Complexation and Salt Formation. J. Pharm. Sci. 1994, 83, 1418–1420. [Google Scholar] [CrossRef]
- Pouton, C.W. Formulation of Poorly Water-Soluble Drugs for Oral Administration: Physicochemical and Physiological Issues and the Lipid Formulation Classification System. Eur. J. Pharm. Sci. 2006, 29, 278–287. [Google Scholar] [CrossRef]
- André, J.-L. Hypertension artérielle chez l’enfant et l’adolescent. EMC Cardiol. Angéiologie 2005, 2, 478–490. [Google Scholar] [CrossRef]
- Ernest, T.B.; Elder, D.P.; Martini, L.G.; Roberts, M.; Ford, J.L. Developing Paediatric Medicines: Identifying the Needs and Recognizing the Challenges. J. Pharm. Pharm. 2007, 59, 1043–1055. [Google Scholar] [CrossRef]
- Salunke, S.; Clapham, D.; Agrawal, A.; Hughes, K.; Nunn, T. Best Practices for Selection of Excipients for Paediatrics—Workshop Reflection. Eur. J. Pharm. Biopharm. 2021, 160, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Zupanets, K.O.; Shebeko, S.K.; Ratushna, K.L.; Katilov, O.V. Cumulative Risks of Excipients in Pediatric Phytomucolytic Syrups: The Implications for Pharmacy Practice. Sci. Pharm. 2021, 89, 32. [Google Scholar] [CrossRef]
- Rouaz, K.; Chiclana-Rodríguez, B.; Nardi-Ricart, A.; Suñé-Pou, M.; Mercadé-Frutos, D.; Suñé-Negre, J.M.; Pérez-Lozano, P.; García-Montoya, E. Excipients in the Paediatric Population: A Review. Pharmaceutics 2021, 13, 387. [Google Scholar] [CrossRef]
- Belayneh, A.; Tadese, E.; Molla, F. Safety and Biopharmaceutical Challenges of Excipients in Off-Label Pediatric Formulations. Int. J. Gen. Med. 2020, 13, 1051–1066. [Google Scholar] [CrossRef] [PubMed]
- Fuss, D.; Gondé, H.; Lamoureux, F.; Pereira, T.; Colnot, M.; Buchbinder, N.; Coquard, A.; Varin, R.; Hervouët, C. Stability Study of a Compounded Oral Solution of Nicardipine for the Treatment of Hypertension in Children. Eur. J. Pharm. Sci. 2021, 160, 105738. [Google Scholar] [CrossRef]
- Schrier, L.; Hadjipanayis, A.; Stiris, T.; Ross-Russell, R.I.; Valiulis, A.; Turner, M.A.; Zhao, W.; De Cock, P.; de Wildt, S.N.; Allegaert, K.; et al. Off-Label Use of Medicines in Neonates, Infants, Children, and Adolescents: A Joint Policy Statement by the European Academy of Paediatrics and the European Society for Developmental Perinatal and Pediatric Pharmacology. Eur. J. Pediatr. 2020, 179, 839–847. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Reflection Paper: Formulations of Choice for the Paediatric Population. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-formulations-choice-paediatric-population_en.pdf (accessed on 15 January 2023).
- Lajoinie, A.; Henin, E.; Nguyen, K.A.; Malik, S.; Mimouni, Y.; Sapori, J.M.; Bréant, V.; Cochat, P.; Kassai, B. Oral Drug Dosage Forms Administered to Hospitalized Children: Analysis of 117,665 Oral Administrations in a French Paediatric Hospital over a 1-Year Period. Int. J. Pharm. 2016, 500, 336–344. [Google Scholar] [CrossRef]
- Moreira, M.; Sarraguça, M. How Can Oral Paediatric Formulations Be Improved? A Challenge for the XXI Century. Int. J. Pharm. 2020, 590, 119905. [Google Scholar] [CrossRef] [PubMed]
- Malkawi, W.A.; AlRafayah, E.; AlHazabreh, M.; AbuLaila, S.; Al-Ghananeem, A.M. Formulation Challenges and Strategies to Develop Pediatric Dosage Forms. Children 2022, 9, 488. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Gervase, M.A.; Evans, J.; Deville, R.; Dong, X. The Stability of Quetiapine Oral Suspension Compounded from Commercially Available Tablets. PLoS ONE 2021, 16, e0255963. [Google Scholar] [CrossRef]
- Hinterlang, M.; Sebti, M.; Cotteret, C.; Vidal, F.; Neven, B.; Cisternino, S.; Schlatter, J. Physicochemical Stability Study of Oral Suspension Containing Ruxolitinib in Children with Steroid-Refractory Acute Graft-Versus-Host Disease. Sci. World J. 2022, 2022, 1931118. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-S.; Lin, S.-C.; Hsieh, Y.-T.; Liu, L.-Y.; Lin, C.-H.; Shen, L.-J.; Huang, C.-F. Formulation and Stability of an Extemporaneously Compounded Propafenone Hydrochloride Oral Suspension for Children with Arrhythmia. Eur. J. Hosp. Pharm. 2022, 29, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Walsh, A.; Ziegler, B.; Lingertat-Walsh, K.; Law, S.; Walker, S.E. Stability of Extemporaneously Compounded Nadolol 10-Mg/ML Suspension in Oral Mix in Glass and Plastic Bottles and Plastic Syringes. Int. J. Pharm. Compd. 2021, 25, 163–168. [Google Scholar] [PubMed]
- Bonnaure, A.-C.; Bellay, R.; Rault, P.; Lester, M.-A.; Boivin, P.-N. Physicochemical Stability of 5 Mg/ML Pediatric Prednisone Oral Suspension in Syrspend® SF PH4. Pharm. Technol. Hosp. Pharm. 2018, 3, 49–57. [Google Scholar] [CrossRef] [Green Version]
- van der Vossen, A.C.; van der Velde, I.; Smeets, O.S.N.M.; Postma, D.J.; Vermes, A.; Koch, B.C.P.; Vulto, A.G.; Hanff, L.M. Design and Stability Study of an Oral Solution of Amlodipine Besylate for Pediatric Patients. Eur. J. Pharm. Sci. 2016, 92, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Santoveña, A.; Suárez-González, J.; Martín-Rodríguez, C.; Fariña, J.B. Formulation Design of Oral Pediatric Acetazolamide Suspension: Dose Uniformity and Physico-Chemical Stability Study. Pharm. Dev. Technol. 2017, 22, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Kriegel, C.; Festag, M.; Kishore, R.S.K.; Roethlisberger, D.; Schmitt, G. Pediatric Safety of Polysorbates in Drug Formulations. Children 2020, 7, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee for Medicinal Products for Human Use (CHMP). Information for the Package Leaflet Regarding Polysorbates Used as Excipients in Medicinal Products for Human Use; European Medicines Agency: Amsterdam, The Netherlands, 2018; pp. 1–42. [Google Scholar]
- Mennella, J.A.; Beauchamp, G.K. Optimizing Oral Medications for Children. Clin. Ther. 2008, 30, 2120–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forestell, C.A. Flavor Perception and Preference Development in Human Infants. Ann. Nutr. Metab. 2017, 70 (Suppl. S3), 17–25. Available online: https://www.karger.com/Article/FullText/478759 (accessed on 12 January 2023). [CrossRef] [Green Version]
- Walsh, J.; Cram, A.; Woertz, K.; Breitkreutz, J.; Winzenburg, G.; Turner, R.; Tuleu, C. European Formulation Initiative Playing Hide and Seek with Poorly Tasting Paediatric Medicines: Do Not Forget the Excipients. Adv. Drug Deliv. Rev. 2014, 73, 14–33. [Google Scholar] [CrossRef]
- Nellis, G.; Metsvaht, T.; Varendi, H.; Toompere, K.; Lass, J.; Mesek, I.; Nunn, A.J.; Turner, M.A.; Lutsar, I. Potentially Harmful Excipients in Neonatal Medicines: A Pan-European Observational Study. Arch. Dis. Child. 2015, 100, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Nowak, K.; Ratajczak–Wrona, W.; Górska, M.; Jabłońska, E. Parabens and Their Effects on the Endocrine System. Mol. Cell. Endocrinol. 2018, 474, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Rowe, R.C.; Sheskey, P.; Quinn, M. Handbook of Pharmaceutical Excipients; Pharmaceutical Press: London, UK, 2009. [Google Scholar]
- Bledsoe, S.; Oschman, A.; Hampson, K.; Hoebing, W.; Pabst, D. Transition to ENFit Enteral Devices: Special Challenges for Pediatric Institutions. Am. J. Health-Syst. Pharm. 2016, 73, 1781–1783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litman, R.S.; Smith, V.I.; Mainland, P. New Solutions to Reduce Wrong Route Medication Errors. Paediatr. Anaesth. 2018, 28, 8–12. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 32 | |
|---|---|---|
| Age (years) (median [IQR]) | 4.5 [2.8–7] | |
| Sex ratio (M/F) | 1.7 | |
| Patient care units | Pediatric hematology/oncology | 78.1% (n = 25) |
| Pediatric intensive care unit | 9.4% (n = 3) | |
| Pediatric department | 6.3% (n = 2) | |
| Pediatric surgery department | 6.3% (n = 2) | |
| Number of administrations per day (mean ± sd) | 2.8 ± 0.3 | |
| Dose per administration (mg) (median, [IQR]) | 8.2 [4–10] | |
| Formulations | Polysorbate 80 | Simple Syrup | Sterile Water | Thickening Agent | Sweetening Agent | Citric Acid/Sodium Citrate | Flavor | Results |
|---|---|---|---|---|---|---|---|---|
| F1 | 1% | To 50 mL | - | - | - | - | - |
|
| F2 | 1% | 50% | To 50 mL | - | - | - | - |
|
| F3 | - | - | To 50 mL | CMC 0.5% or 0.1% | - | - | - |
|
| F4 | - | - | To 50 mL | HPMC 0.5% | - | - | - |
|
| F5 | - | - | To 50 mL | HPMC 0.25% | - | - | - |
|
| F6 | - | - | To 50 mL | HPMC 0.25% | Sorbitol 20% or 70% | - | - |
|
| F7 | - | - | To 50 mL | HPMC 0.25% | Sodium saccharin 0.075–0.1% | - | - |
|
| F8 | - | - | To 50 mL | HPMC 0.25% | Sodium saccharin 0.1% | 0.1%/0.1% | - |
|
| F9 | 1% | - | To 50 mL | HPMC 0.25% | Sodium saccharin 0.1% | 0.1%/0.1% | - |
|
| F10 | 0.75% | - | To 50 mL | HPMC 0.25% | Sodium saccharin 0.1% | 0.1%/0.1% | - |
|
| F11 | 0.5% | - | To 50 mL | HPMC 0.25% | Sodium saccharin 0.1% | 0.1%/0.1% | - |
|
| F12 | 0.75% | - | To 50 mL | HPMC 0.25% | Sodium saccharin 0.15% | 0.1%/0.1% | - |
|
| F13 | 0.75% | - | To 50 mL | HPMC 0.25% | Sodium saccharin 0.1% | 0.1%/0.1% | 3 to 10 drops (strawberry and/or raspberry) |
|
| F14 | 0.75% | 38% | To 50 mL | HPMC 0.25% | Sodium saccharin 0.1% | 0.1%/0.1% | 4 drops (strawberry) |
|
| Microorganisms | Potassium Sorbate | Concentration (CFU/mL) | ||
|---|---|---|---|---|
| Day 0 | Day 14 | Day 28 | ||
| Staphylococcus aureus | 0.2% | 1.3 × 105 | 0 | 0 |
| 0.3% | 2.4 × 105 | 0 | 0 | |
| Escherichia coli | 0.2% | 1.6 × 105 | 0 | 0 |
| 0.3% | 2.3 × 105 | 0 | 0 | |
| Pseudomonas aeruginosa | 0.2% | 2.0 × 105 | 0 | 0 |
| 0.3% | 6.9 × 105 | 0 | 0 | |
| Candida albicans | 0.2% | 1.1 × 105 | 0 | 0 |
| 0.3% | 1.1 × 105 | 0 | 0 | |
| Aspergillus brasiliensis | 0.2% | 0.4 × 105 | 0 | 0 |
| 0.3% | 1.0 × 105 | 0 | 0 | |
| Components | Quantities |
|---|---|
| Nicardipine hydrochloride | 2 g |
| Polysorbate 80 | 7.5 g |
| Hydroxypropylmethylcellulose | 2.5 g |
| Potassium sorbate | 2 g |
| Sodium saccharin | 1 g |
| Citric acid | 1 g |
| Sodium citrate | 1 g |
| Simple syrup | 380 g |
| Strawberry flavor | 80 drops |
| Sterile water | To 1000 mL |
| Days | Storage Temperature | pH | Osmolality (mOsm/kg) |
|---|---|---|---|
| 0 | 25 ± 2 °C | 4.84 (±0) | 1165 (±40) |
| 5 ± 3 °C | 4.84 (±0.01) | 1152 (±28) | |
| 7 | 25 ± 2 °C | 4.77 (±0) | 1164 (±21) |
| 5 ± 3 °C | 4.83 (±0.01) | 1144 (±17) | |
| 14 | 25 ± 2 °C | 4.84 (±0) | 1160 (±21) |
| 5 ± 3 °C | 4.86 (±0) | 1131 (±15) | |
| 28 | 25 ± 2 °C | 4.85 (±0.01) | 1159 (±20) |
| 5 ± 3 °C | 4.86 (±0.01) | 1139 (±27) | |
| 60 | 25 ± 2 °C | 4.88 (±0) | 1145 (±42) |
| 5 ± 3 °C | 4.90 (±0.01) | 1133 (±17) | |
| 90 | 25 ± 2 °C | 4.91 (±0.01) | 1166 (±22) |
| 5 ± 3 °C | 4.93 (±0.01) | 1155 (±14) | |
| 183 | 25 ± 2 °C | 4.84 (±0.01) | 1165 (±8) |
| 5 ± 3 °C | 4.88 (±0.01) | 1156 (±10) | |
| 268 | 25 ± 2 °C | 4.87 (±0.01) | 1172 (±5) |
| 5 ± 3 °C | 4.89 (±0) | 1156 (±11) | |
| 365 | 25 ± 2 °C | 4.89 (±0.01) | 1179 (±7) |
| 5 ± 3 °C | 4.92 (±0) | 1153 (±10) |
| Individual Doses | Luer-Lock Syringe with Adapter(g) | Luer Syringe with Adapter (g) | Syringe for Oral Use without Adapter (g) | Syringe for Oral Use with Adapter (g) |
|---|---|---|---|---|
| 1 | 4.38 | 4.41 | 4.57 | 4.43 |
| 2 | 4.39 | 4.41 | 4.61 | 4.39 |
| 3 | 4.40 | 4.40 | 4.59 | 4.44 |
| 4 | 4.40 | 4.39 | 4.63 | 4.42 |
| 5 | 4.41 | 4.41 | 4.62 | 4.46 |
| 6 | 4.40 | 4.38 | 4.61 | 4.42 |
| 7 | 4.40 | 4.40 | 4.59 | 4.41 |
| 8 | 4.41 | 4.40 | 4.60 | 4.40 |
| 9 | 4.41 | 4.40 | 4.58 | 4.42 |
| 10 | 4.41 | 4.41 | 4.62 | 4.41 |
| 11 | 4.39 | 4.40 | 4.61 | 4.40 |
| 12 | 4.41 | 4.40 | 4.59 | 4.41 |
| 13 | 4.40 | 4.39 | 4.58 | 4.44 |
| 14 | 4.40 | 4.40 | 4.58 | 4.40 |
| 15 | 4.41 | 4.40 | 4.64 | 4.41 |
| 16 | 4.41 | 4.41 | 4.59 | 4.41 |
| 17 | 4.39 | 4.39 | 4.66 | 4.42 |
| 18 | 4.40 | 4.41 | 4.68 | 4.41 |
| 19 | 4.40 | 4.41 | 4.73 | 4.39 |
| 20 | 4.40 | 4.40 | 4.65 | 4.43 |
| Average | 4.40 | 4.40 | 4.62 | 4.42 |
| 10% deviation | [3.96–4.84] | [3.96–4.84] | [4.15–5.08] | [3.97–4.86] |
| 20% deviation | [3.52–5.28] | [3.52–5.28] | [3.69–5.54] | [3.53–5.30] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavelier, M.; Gondé, H.; Costa, D.; Lamoureux, F.; Pereira, T.; Buchbinder, N.; Varin, R.; Hervouët, C. Development of an Oral Liquid Formulation of Nicardipine Hydrochloride Compounded with Simple Excipients for the Treatment of Pediatric Hypertension. Pharmaceutics 2023, 15, 446. https://doi.org/10.3390/pharmaceutics15020446
Cavelier M, Gondé H, Costa D, Lamoureux F, Pereira T, Buchbinder N, Varin R, Hervouët C. Development of an Oral Liquid Formulation of Nicardipine Hydrochloride Compounded with Simple Excipients for the Treatment of Pediatric Hypertension. Pharmaceutics. 2023; 15(2):446. https://doi.org/10.3390/pharmaceutics15020446
Chicago/Turabian StyleCavelier, Marine, Henri Gondé, Damien Costa, Fabien Lamoureux, Tony Pereira, Nimrod Buchbinder, Rémi Varin, and Charles Hervouët. 2023. "Development of an Oral Liquid Formulation of Nicardipine Hydrochloride Compounded with Simple Excipients for the Treatment of Pediatric Hypertension" Pharmaceutics 15, no. 2: 446. https://doi.org/10.3390/pharmaceutics15020446
APA StyleCavelier, M., Gondé, H., Costa, D., Lamoureux, F., Pereira, T., Buchbinder, N., Varin, R., & Hervouët, C. (2023). Development of an Oral Liquid Formulation of Nicardipine Hydrochloride Compounded with Simple Excipients for the Treatment of Pediatric Hypertension. Pharmaceutics, 15(2), 446. https://doi.org/10.3390/pharmaceutics15020446