
Advances in Radionuclides and Radiolabelled Peptides for Cancer Therapeutics

 ,
, 
 and
and
Abstract
:1. Introduction
2. Various Radionuclides for Theragnosis
3. Radiopharmaceuticals with Radiolabelled Peptides towards Cancer Therapy: Mechanistic Pathway and Biological Paraphernalia
3.1. Radiation Dosimetry
3.2. Localization Pathways
4. Fabrication of Amino Chains for Radiopharmaceutical Applications
5. Radiolabelled Peptides Used in Cancer Theragnosis
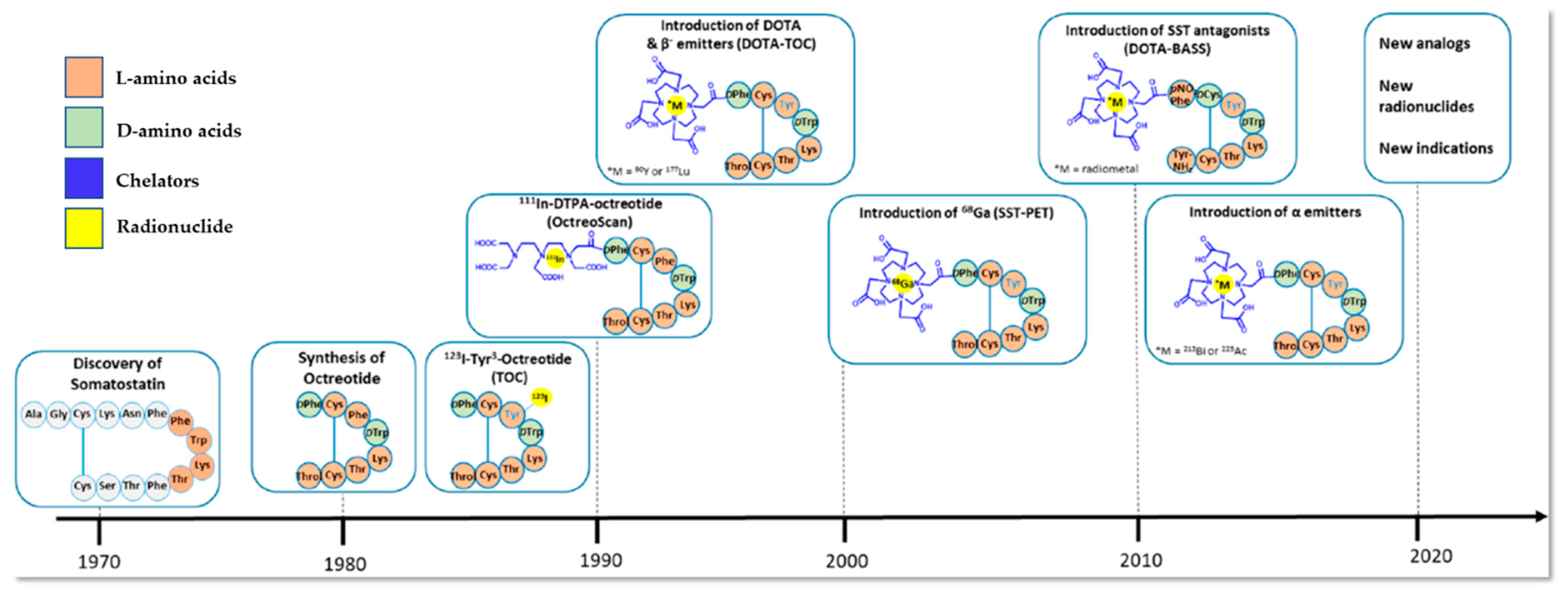
5.1. Somatostatin Receptor-Targeted Anticancer Therapy
5.2. CD13-Targeted Anticancer Therapy
6. Radiolabelled Peptides Translated into Clinical Trials
7. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simón, M.; Jørgensen, J.T.; Khare, H.A.; Christensen, C.; Nielsen, C.H.; Kjaer, A. Combination of [177Lu]Lu-DOTA-TATE Targeted Radionuclide Therapy and Photothermal Therapy as a Promising Approach for Cancer Treatment: In Vivo Studies in a Human Xenograft Mouse Model. Pharmaceutics 2022, 14, 1284. [Google Scholar] [CrossRef] [PubMed]
- Frantellizzi, V.; Verrina, V.; Raso, C.; Pontico, M.; Petronella, F.; Bertana, V.; Ballesio, A.; Marasso, S.L.; Miglietta, S.; Rosa, P.; et al. 99mTc-Labeled Keratin Gold-Nanoparticles in a Nephron-like Microfluidic Chip for Photo-Thermal Therapy Applications. Mater. Today Adv. 2022, 16, 100286. [Google Scholar] [CrossRef]
- Cheng, M.H.Y.; Overchuk, M.; Rajora, M.A.; Lou, J.W.H.; Chen, Y.; Pomper, M.G.; Chen, J.; Zheng, G. Targeted Theranostic 111 In/Lu-Nanotexaphyrin for SPECT Imaging and Photodynamic Therapy. Mol. Pharm. 2022, 19, 1803–1813. [Google Scholar] [CrossRef]
- Kumar, D.S.; Girija, A.R. Bionanotechnology in Cancer; Jenny Stanford Publishing: New York, NY, USA, 2022; ISBN 9780429422911. [Google Scholar]
- Ferreira, C.A.; Heidari, P.; Ataeinia, B.; Sinevici, N.; Sise, M.E.; Colvin, R.B.; Wehrenberg-Klee, E.; Mahmood, U. Non-Invasive Detection of Immunotherapy-Induced Adverse Events. Clin. Cancer Res. 2021, 27, 5353–5364. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Zhang, Y.; Wang, Z.; Sun, Y.; Shi, L.; Yu, Y.; Shi, J.; Hu, Z.; Wang, F. A Novel Peptide-Based Probe 99mTc-PEG6-RD-PDP2 for the Molecular Imaging of Tumor PD-L2 Expression. Chin. Chem. Lett. 2022, 33, 3497–3501. [Google Scholar] [CrossRef]
- Wen, X.; Zeng, X.; Liu, J.; Zhang, Y.; Shi, C.; Wu, X.; Zhuang, R.; Chen, X.; Zhang, X.; Guo, Z. Synergism of 64 Cu-Labeled RGD with Anti-PD-L1 Immunotherapy for the Long-Acting Antitumor Effect. Bioconjug. Chem. 2022, 33, 2170–2179. [Google Scholar] [CrossRef]
- He, Z.; Jia, H.; Zheng, M.; Wang, H.; Yang, W.; Gao, L.; Zhang, Z.; Xue, J.; Xu, B.; Yang, W.; et al. Trp2 Peptide-Assembled Nanoparticles with Intrinsically Self-Chelating 64 Cu Properties for PET Imaging Tracking and Dendritic Cell-Based Immunotherapy against Melanoma. ACS Appl. Bio Mater. 2021, 4, 5707–5716. [Google Scholar] [CrossRef]
- Wang, C.; Tian, Y.; Wu, B.; Cheng, W. Recent Progress Toward Imaging Application of Multifunction Sonosensitizers in Sonodynamic Therapy. Int. J. Nanomed. 2022, 17, 3511–3529. [Google Scholar] [CrossRef]
- Dhaini, B.; Kenzhebayeva, B.; Ben-Mihoub, A.; Gries, M.; Acherar, S.; Baros, F.; Thomas, N.; Daouk, J.; Schohn, H.; Hamieh, T.; et al. Peptide-Conjugated Nanoparticles for Targeted Photodynamic Therapy. Nanophotonics 2021, 10, 3089–3134. [Google Scholar] [CrossRef]
- Wang, H.; Wang, Z.; Chen, W.; Wang, W.; Shi, W.; Chen, J.; Hang, Y.; Song, J.; Xiao, X.; Dai, Z. Self-Assembly of Photosensitive and Radiotherapeutic Peptide for Combined Photodynamic-Radio Cancer Therapy with Intracellular Delivery of MiRNA-139-5p. Bioorg. Med. Chem. 2021, 44, 116305. [Google Scholar] [CrossRef]
- Ho, J.A.; Wang, L.-S.; Chuang, M.-C. Nanotheranostics—A Review of Recent Publications. Int. J. Nanomed. 2012, 7, 4679–4695. [Google Scholar] [CrossRef] [Green Version]
- Pan, T.; Mawlawi, O. PET/CT in Radiation Oncology. Med. Phys. 2008, 35, 4955–4966. [Google Scholar] [CrossRef] [Green Version]
- Guerra Liberal, F.D.C.; Tavares, A.A.S.; Tavares, J.M.R.S. Palliative Treatment of Metastatic Bone Pain with Radiopharmaceuticals: A Perspective beyond Strontium-89 and Samarium-153. Appl. Radiat. Isot. 2016, 110, 87–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzzini Calegaro, J.U.; de Podestá Haje, D.; Machado, J.; Sayago, M.; de Landa, D.C. Synovectomy Using Samarium-153 Hydroxyapatite in the Elbows and Ankles of Patients with Hemophilic Arthropathy. World J. Nucl. Med. 2018, 17, 6–11. [Google Scholar] [CrossRef]
- Kolesnikov-Gauthier, H.; Lemoine, N.; Tresch-Bruneel, E.; Olivier, A.; Oudoux, A.; Penel, N. Efficacy and Safety of 153Sm-EDTMP as Treatment of Painful Bone Metastasis: A Large Single-Center Study. Support. Care Cancer 2018, 26, 751–758. [Google Scholar] [CrossRef]
- Ma, H.; Li, F.; Shen, G.; Cai, H.; Liu, W.; Lan, T.; Yang, Y.; Yang, J.; Liao, J.; Liu, N. Synthesis and Preliminary Evaluation of 131 I-Labeled FAPI Tracers for Cancer Theranostics. Mol. Pharm. 2021, 18, 4179–4187. [Google Scholar] [CrossRef]
- Giannakenas, C.; Kalofonos, H.P.; Apostolopoulos, D.J.; Zarakovitis, J.; Kosmas, C.; Vassilakos, P.J. Preliminary Results of the Use of Re-186-HEDP for Palliation of Pain in Patients with Metastatic Bone Disease. Am. J. Clin. Oncol. Cancer Clin. Trials 2000, 23, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Klett, R.; Lange, U.; Haas, H.; Voth, M.; Pinkert, J. Radiosynoviorthesis of Medium-Sized Joints with Rhenium-186-Sulphide Colloid: A Review of the Literature. Rheumatology 2007, 46, 1531–1537. [Google Scholar] [CrossRef] [Green Version]
- Gomes Marin, J.F.; Nunes, R.F.; Coutinho, A.M.; Zaniboni, E.C.; Costa, L.B.; Barbosa, F.G.; Queiroz, M.A.; Cerri, G.G.; Buchpiguel, C.A. Theranostics in Nuclear Medicine: Emerging and Re-Emerging Integrated Imaging and Therapies in the Era of Precision Oncology. RadioGraphics 2020, 40, 1715–1740. [Google Scholar] [CrossRef] [PubMed]
- Arruebo, M.; Vilaboa, N.; Sáez-Gutierrez, B.; Lambea, J.; Tres, A.; Valladares, M.; González-Fernández, Á. Assessment of the Evolution of Cancer Treatment Therapies. Cancers 2011, 3, 3279–3330. [Google Scholar] [CrossRef] [Green Version]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; Rodriguez-Torres, M.d.P.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano Based Drug Delivery Systems: Recent Developments and Future Prospects. J. Nanobiotechnol. 2018, 16, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertz, S. Radioactive Iodine in the Study of Thyroid Physiology. J. Am. Med. Assoc. 1946, 131, 81. [Google Scholar] [CrossRef] [PubMed]
- Herrero Álvarez, N.; Bauer, D.; Hernández-Gil, J.; Lewis, J.S. Recent Advances in Radiometals for Combined Imaging and Therapy in Cancer. ChemMedChem 2021, 16, 2909–2941. [Google Scholar] [CrossRef] [PubMed]
- Roll, W.; Weckesser, M.; Seifert, R.; Bodei, L.; Rahbar, K. Imaging and Liquid Biopsy in the Prediction and Evaluation of Response to PRRT in Neuroendocrine Tumors: Implications for Patient Management. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4016–4027. [Google Scholar] [CrossRef]
- Ambrosini, V.; Kunikowska, J.; Baudin, E.; Bodei, L.; Bouvier, C.; Capdevila, J.; Cremonesi, M.; de Herder, W.W.; Dromain, C.; Falconi, M.; et al. Consensus on Molecular Imaging and Theranostics in Neuroendocrine Neoplasms. Eur. J. Cancer 2021, 146, 56–73. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Solnes, L.B.; Javadi, M.S.; Weich, A.; Gorin, M.A.; Pienta, K.J.; Higuchi, T.; Buck, A.K.; Pomper, M.G.; Rowe, S.P.; et al. SSTR-RADS Version 1.0 as a Reporting System for SSTR PET Imaging and Selection of Potential PRRT Candidates: A Proposed Standardization Framework. J. Nucl. Med. 2018, 59, 1085–1091. [Google Scholar] [CrossRef] [Green Version]
- Parghane, R.; Mitra, A.; Bannore, T.; Rakshit, S.; Banerjee, S.; Basu, S. Initial Clinical Evaluation of Indigenous 90Y-DOTATATE in Sequential Duo-PRRT Approach (177Lu-DOTATATE and 90Y-DOTATATE) in Neuroendocrine Tumors with Large Bulky Disease: Observation on Tolerability,90Y-DOTATATE Post- PRRT Imaging Characteristics (bremsstrahlung and PETCT) and early adverse effects. World J. Nucl. Med. 2021, 20, 73–81. [Google Scholar] [CrossRef]
- Ngam, P.I.; Tan, E.; Lim, G.; Yan, S.X. Improving Yittrium-90 PET Scan Image Quality through Optimized Reconstruction Algorithms. J. Nucl. Med. Technol. 2023, 51, 26–31. [Google Scholar] [CrossRef]
- Konuparamban, A.; Nautiyal, A.; Jha, A.; Srichandan, T.; Mithun, S.; RANGARAJAN, V. Feasibility and Reliability Assessment of Single Imaging Time-Point for Organ and Tumour Dosimetry Following 177Lu-DOTATATE PRRT. J. Nucl. Med. 2022, 63, 2817. [Google Scholar]
- Veenstra, E.B.; Brouwers, A.H.; de Groot, D.J.A.; Hofland, J.; Walenkamp, A.M.E.; Brabander, T.; Zandee, W.T.; Noordzij, W. Comparison of [18F]DOPA and [68Ga]DOTA-TOC as a PET Imaging Tracer before Peptide Receptor Radionuclide Therapy. Eur. J. Hybrid Imaging 2022, 6, 12. [Google Scholar] [CrossRef]
- Song, W.; Song, Y.; Li, Q.; Fan, C.; Lan, X.; Jiang, D. Advances in Aptamer-Based Nuclear Imaging. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2544–2559. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Bagni, O.; Nervi, C. Aptamer-Based Technology for Radionuclide Targeted Imaging and Therapy: A Promising Weapon against Cancer. Expert Rev. Med. Devices 2020, 17, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-B.; Banik, N.; Han, B.; Lee, D.-N.; Park, J. Peptide-Based Bioconjugates and Therapeutics for Targeted Anticancer Therapy. Pharmaceutics 2022, 14, 1378. [Google Scholar] [CrossRef]
- Wright, C.L.; Zhang, J.; Tweedle, M.F.; Knopp, M.V.; Hall, N.C. Theranostic Imaging of Yttrium-90. BioMed Res. Int. 2015, 2015, 481279. [Google Scholar] [CrossRef] [Green Version]
- Yong, K.; Milenic, D.; Baidoo, K.; Brechbiel, M. Mechanisms of Cell Killing Response from Low Linear Energy Transfer (LET) Radiation Originating from 177Lu Radioimmunotherapy Targeting Disseminated Intraperitoneal Tumor Xenografts. Int. J. Mol. Sci. 2016, 17, 736. [Google Scholar] [CrossRef] [Green Version]
- Kassis, A.I. Therapeutic Radionuclides: Biophysical and Radiobiologic Principles. Semin. Nucl. Med. 2008, 38, 358–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, S.A.; Hernandez, R.; Fonslet, J.; England, C.G.; Valdovinos, H.F.; Ellison, P.A.; Barnhart, T.E.; Elema, D.R.; Theuer, C.P.; Cai, W.; et al. Novel Preparation Methods of 52 Mn for ImmunoPET Imaging. Bioconjug. Chem. 2015, 26, 2118–2124. [Google Scholar] [CrossRef] [Green Version]
- McDevitt, M.R.; Sgouros, G.; Finn, R.D.; Humm, J.L.; Jurcic, J.G.; Larson, S.M.; Scheinberg, D.A. Radioimmunotherapy with Alpha-Emitting Nuclides. Eur. J. Nucl. Med. Mol. Imaging 1998, 25, 1341–1351. [Google Scholar] [CrossRef] [PubMed]
- McDevitt, M.R.; Ma, D.; Lai, L.T.; Simon, J.; Borchardt, P.; Frank, R.K.; Wu, K.; Pellegrini, V.; Curcio, M.J.; Miederer, M.; et al. Tumor Therapy with Targeted Atomic Nanogenerators. Science 2001, 294, 1537–1540. [Google Scholar] [CrossRef]
- Müller, C.; van der Meulen, N.P.; Benešová, M.; Schibli, R. Therapeutic Radiometals Beyond 177 Lu and 90 Y: Production and Application of Promising α-Particle, β-Particle, and Auger Electron Emitters. J. Nucl. Med. 2017, 58, 91S–96S. [Google Scholar] [CrossRef] [Green Version]
- Ling, S.W.; de Blois, E.; Hooijman, E.; van der Veldt, A.; Brabander, T. Advances in 177Lu-PSMA and 225Ac-PSMA Radionuclide Therapy for Metastatic Castration-Resistant Prostate Cancer. Pharmaceutics 2022, 14, 2166. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Chiaravalloti, A.; Schillaci, O.; Bagni, O. The Potential of PSMA-Targeted Alpha Therapy in the Management of Prostate Cancer. Expert Rev. Anticancer Ther. 2020, 20, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Stéen, E.J.L.; Edem, P.E.; Nørregaard, K.; Jørgensen, J.T.; Shalgunov, V.; Kjaer, A.; Herth, M.M. Pretargeting in Nuclear Imaging and Radionuclide Therapy: Improving Efficacy of Theranostics and Nanomedicines. Biomaterials 2018, 179, 209–245. [Google Scholar] [CrossRef] [PubMed]
- Li, G.-P. Avidin-Biotin System Pretargeting Radioimmunoimaging and Radioimmunotherapy and Its Application in Mouse Model of Human Colon Carcinoma. World J. Gastroenterol. 2005, 11, 6288. [Google Scholar] [CrossRef]
- Morgan, K.A.; de Veer, M.; Miles, L.A.; Kelderman, C.A.A.; McLean, C.A.; Masters, C.L.; Barnham, K.J.; White, J.M.; Paterson, B.M.; Donnelly, P.S. Pre-Targeting Amyloid-β with Antibodies for Potential Molecular Imaging of Alzheimer’s Disease. Chem. Commun. 2023, 59, 2243–2246. [Google Scholar] [CrossRef] [PubMed]
- Ku, A.; Facca, V.J.; Cai, Z.; Reilly, R.M. Auger Electrons for Cancer Therapy—A Review. EJNMMI Radiopharm. Chem. 2019, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, P.; Rimal, R.; Sahnoun, S.E.M.; Mottaghy, F.M.; Möller, M.; Morgenroth, A.; Singh, S. Radiolabeled Nanocarriers as Theranostics—Advancement from Peptides to Nanocarriers. Small 2022, 18, 2200673. [Google Scholar] [CrossRef] [PubMed]
- Stella, M.; Braat, A.J.A.T.; Lam, M.G.E.H.; de Jong, H.W.A.M.; van Rooij, R. Gamma Camera Characterization at High Holmium-166 Activity in Liver Radioembolization. EJNMMI Phys. 2021, 8, 22. [Google Scholar] [CrossRef]
- Klaassen, N.J.M.; Arntz, M.J.; Gil Arranja, A.; Roosen, J.; Nijsen, J.F.W. The Various Therapeutic Applications of the Medical Isotope Holmium-166: A Narrative Review. EJNMMI Radiopharm. Chem. 2019, 4, 19. [Google Scholar] [CrossRef] [Green Version]
- Breitz, H.B.; Wendt, R.E.; Stabin, M.S.; Shen, S.; Erwin, W.D.; Rajendran, J.G.; Eary, J.F.; Durack, L.; Delpassand, E.; Martin, W.; et al. 166Ho-DOTMP Radiation-Absorbed Dose Estimation for Skeletal Targeted Radiotherapy. J. Nucl. Med. 2006, 47, 534–542. [Google Scholar]
- Bayouth, J.E.; Macey, D.J.; Kasi, L.P.; Garlich, J.R.; McMillan, K.; Dimopoulos, M.A.; Champlin, R.E. Pharmacokinetics, Dosimetry and Toxicity of Holmium-166-DOTMP for Bone Marrow Ablation in Multiple Myeloma. J. Nucl. Med. 1995, 36, 730–737. [Google Scholar] [PubMed]
- Bahrami-Samani, A. Production, Quality Control and Pharmacokinetic Studies of 166Ho-EDTMP for Therapeutic Applications. Sci. Pharm. 2010, 78, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vente, M.A.D.; Hobbelink, M.G.G.; van het Schip, A.D.; Zonnenberg, B.A.; Nijsen, J.F.W. Radionuclide Liver Cancer Therapies: From Concept to Current Clinical Status. Anticancer Agents Med. Chem. 2007, 7, 441–459. [Google Scholar] [CrossRef]
- Vente, M.A.D.; de Wit, T.C.; van den Bosch, M.A.A.J.; Bult, W.; Seevinck, P.R.; Zonnenberg, B.A.; de Jong, H.W.A.M.; Krijger, G.C.; Bakker, C.J.G.; van het Schip, A.D.; et al. Holmium-166 Poly(L-Lactic Acid) Microsphere Radioembolisation of the Liver: Technical Aspects Studied in a Large Animal Model. Eur. Radiol. 2010, 20, 862–869. [Google Scholar] [CrossRef] [Green Version]
- Ha, E.J.; Gwak, H.-S.; Rhee, C.H.; Youn, S.M.; Choi, C.-W.; Cheon, G.J. Intracavitary Radiation Therapy for Recurrent Cystic Brain Tumors with Holmium-166-Chico: A Pilot Study. J. Korean Neurosurg. Soc. 2013, 54, 175. [Google Scholar] [CrossRef]
- Sohn, J.H.; Choi, H.J.; Lee, J.T.; Lee, J.D.; Kim, J.H.; Moon, Y.M.; Park, K.; Park, K.B.; Kim, E.; Yoo, N.C. Phase II Study of Transarterial Holmium-166-Chitosan Complex Treatment in Patients with a Single, Large Hepatocellular Carcinoma. Oncology 2009, 76, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bhusari, P.; Vatsa, R.; Singh, G.; Parmar, M.; Bal, A.; Dhawan, D.K.; Mittal, B.R.; Shukla, J. Development of Lu-177-Trastuzumab for Radioimmunotherapy of HER2 Expressing Breast Cancer and Its Feasibility Assessment in Breast Cancer Patients. Int. J. Cancer 2017, 140, 938–947. [Google Scholar] [CrossRef]
- Emmett, L.; Willowson, K.; Violet, J.; Shin, J.; Blanksby, A.; Lee, J. Lutetium 177 PSMA Radionuclide Therapy for Men with Prostate Cancer: A Review of the Current Literature and Discussion of Practical Aspects of Therapy. J. Med. Radiat. Sci. 2017, 64, 52–60. [Google Scholar] [CrossRef]
- Dash, A.; Knapp, F.F.; Pillai, M. Targeted Radionuclide Therapy—An Overview. Curr. Radiopharm. 2013, 6, 152–180. [Google Scholar] [CrossRef]
- Yeong, C.-H.; Cheng, M.; Ng, K.-H. Therapeutic Radionuclides in Nuclear Medicine: Current and Future Prospects. J. Zhejiang Univ. Sci. B 2014, 15, 845–863. [Google Scholar] [CrossRef] [Green Version]
- Sartor, O. Overview of Samarium Sm 153 Lexidronam in the Treatment of Painful Metastatic Bone Disease. Rev. Urol. 2004, 6 (Suppl. 10), S3–S12. [Google Scholar] [PubMed]
- Eary, J.F.; Collins, C.; Stabin, M.; Vernon, C.; Petersdorf, S.; Baker, M.; Hartnett, S.; Ferency, S.; Addison, S.J.; Appelbaum, F. Samarium-153-EDTMP Biodistribution and Dosimetry Estimation. J. Nucl. Med. 1993, 34, 1031–1036. [Google Scholar] [PubMed]
- Silberstein, E.B. Teletherapy and Radiopharmaceutical Therapy of Painful Bone Metastases. Semin. Nucl. Med. 2005, 35, 152–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Arienzo, M. Emission of Β+ Particles Via Internal Pair Production in the 0+–0+ Transition of 90Zr: Historical Background and Current Applications in Nuclear Medicine Imaging. Atoms 2013, 1, 2–12. [Google Scholar] [CrossRef]
- Kim, Y.-C.; Kim, Y.-H.; Uhm, S.-H.; Seo, Y.S.; Park, E.-K.; Oh, S.-Y.; Jeong, E.; Lee, S.; Choe, J.-G. Radiation Safety Issues in Y-90 Microsphere Selective Hepatic Radioembolization Therapy: Possible Radiation Exposure from the Patients. Nucl. Med. Mol. Imaging 2010, 44, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.K.T.; Kao, Y.H.; Too, C.W.; Chin, K.F.W.; Ng, D.C.E.; Chow, P.K.H. Yttrium-90 Hepatic Radioembolization: Clinical Review and Current Techniques in Interventional Radiology and Personalized Dosimetry. Br. J. Radiol. 2016, 89, 20150943. [Google Scholar] [CrossRef]
- Golfieri, R. SIR-Spheres Yttrium-90 Radioembolization for the Treatment of Unresectable Liver Cancers. Hepatic Oncol. 2014, 1, 265–283. [Google Scholar] [CrossRef] [Green Version]
- Van Thai, N.; Thinh, N.T.; Ky, T.D.; Bang, M.H.; Giang, D.T.; Ha, L.N.; Son, M.H.; Tien, D.D.; Lee, H.W. Efficacy and Safety of Selective Internal Radiation Therapy with Yttrium-90 for the Treatment of Unresectable Hepatocellular Carcinoma. BMC Gastroenterol. 2021, 21, 216. [Google Scholar] [CrossRef]
- Zeng, H.; Zhou, C.; Chen, X.; Hu, L.; Su, K.; Guo, L.; Han, Y. Comparison of the Efficacy and Safety of Selective Internal Radiotherapy and Sorafenib Alone or Combined for Hepatocellular Carcinoma: A Systematic Review and Bayesian Network Meta-Analysis. Clin. Exp. Med. 2023. [Google Scholar] [CrossRef]
- Lawless, S.; McMullin, M.F.; Cuthbert, R.; Houston, R. (32)P in the Treatment of Myeloproliferative Disorders. Ulst. Med. J. 2016, 85, 83–85. [Google Scholar]
- Giammarile, F.; Mognetti, T.; Resche, I. Bone Pain Palliation with Strontium-89 in Cancer Patients with Bone Metastases. Q. J. Nucl. Med. 2001, 45, 78–83. [Google Scholar]
- Singh, P.; Anil, G. Yttrium-90 Radioembolization of Liver Tumors: What Do the Images Tell Us? Cancer Imaging 2014, 13, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Dancey, J.E.; Shepherd, F.A.; Paul, K.; Sniderman, K.W.; Houle, S.; Gabrys, J.; Hendler, A.L.; Goin, J.E. Treatment of Nonresectable Hepatocellular Carcinoma with Intrahepatic 90Y-Microspheres. J. Nucl. Med. 2000, 41, 1673–1681. [Google Scholar]
- Jeyarajah, D.R.; Doyle, M.B.M.; Espat, N.J.; Hansen, P.D.; Iannitti, D.A.; Kim, J.; Thambi-Pillai, T.; Visser, B.C. Role of Yttrium-90 Selective Internal Radiation Therapy in the Treatment of Liver-Dominant Metastatic Colorectal Cancer: An Evidence-Based Expert Consensus Algorithm. J. Gastrointest. Oncol. 2020, 11, 443–460. [Google Scholar] [CrossRef]
- Braat, A.J.A.T.; Kwekkeboom, D.J.; Kam, B.L.R.; Teunissen, J.J.M.; de Herder, W.W.; Dreijerink, K.M.A.; van Rooij, R.; Krijger, G.C.; de Jong, H.W.A.M.; van den Bosch, M.A.A.J.; et al. Additional Hepatic 166Ho-Radioembolization in Patients with Neuroendocrine Tumours Treated with 177Lu-DOTATATE; a Single Center, Interventional, Non-Randomized, Non-Comparative, Open Label, Phase II Study (HEPAR PLUS Trial). BMC Gastroenterol. 2018, 18, 84. [Google Scholar] [CrossRef] [PubMed]
- van Roekel, C.; Bastiaannet, R.; Smits, M.L.J.; Bruijnen, R.C.; Braat, A.J.A.T.; de Jong, H.W.A.M.; Elias, S.G.; Lam, M.G.E.H. Dose–Effect Relationships of 166 Ho Radioembolization in Colorectal Cancer. J. Nucl. Med. 2021, 62, 272–279. [Google Scholar] [CrossRef]
- Kim, J.K.; Han, K.-H.; Lee, J.T.; Paik, Y.H.; Ahn, S.H.; Lee, J.D.; Lee, K.S.; Chon, C.Y.; Moon, Y.M. Long-Term Clinical Outcome of Phase IIb Clinical Trial of Percutaneous Injection with Holmium-166/Chitosan Complex (Milican) for the Treatment of Small Hepatocellular Carcinoma. Clin. Cancer Res. 2006, 12, 543–548. [Google Scholar] [CrossRef] [Green Version]
- Lo Bianco, G.; Lanza, E.; Provenzano, S.; Federico, M.; Papa, A.; Imani, F.; Shirkhany, G.; Laudicella, R.; Quartuccio, N. A Multimodal Clinical Approach for the Treatment of Bone Metastases in Solid Tumors. Anesthesiol. Pain Med. 2022, 12, e126333. [Google Scholar] [CrossRef]
- Rainone, P.; Riva, B.; Belloli, S.; Sudati, F.; Ripamonti, M.; Verderio, P.; Colombo, M.; Colzani, B.; Gilardi, M.C.; Moresco, R.M.; et al. Development of 99mTc-Radiolabeled Nanosilica for Targeted Detection of HER2-Positive Breast Cancer. Int. J. Nanomed. 2017, 12, 3447–3461. [Google Scholar] [CrossRef] [Green Version]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Dwivedi, S.N.; Bal, C. Radioligand Therapy With 177 Lu-PSMA for Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Meta-Analysis. Am. J. Roentgenol. 2019, 213, 275–285. [Google Scholar] [CrossRef]
- van der Doelen, M.J.; Kuppen, M.C.P.; Jonker, M.A.; Mehra, N.; Janssen, M.J.R.; van Oort, I.M.; Gerritsen, W.R. 223Ra Therapy in Patients with Advanced Castration-Resistant Prostate Cancer with Bone Metastases. Clin. Nucl. Med. 2018, 43, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagemann, U.B.; Wickstroem, K.; Hammer, S.; Bjerke, R.M.; Zitzmann-Kolbe, S.; Ryan, O.B.; Karlsson, J.; Scholz, A.; Hennekes, H.; Mumberg, D.; et al. Advances in Precision Oncology: Targeted Thorium-227 Conjugates as a New Modality in Targeted Alpha Therapy. Cancer Biother. Radiopharm. 2020, 35, 497–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manafi-Farid, R.; Masoumi, F.; Divband, G.; Saidi, B.; Ataeinia, B.; Hertel, F.; Schweighofer-Zwink, G.; Morgenroth, A.; Beheshti, M. Targeted Palliative Radionuclide Therapy for Metastatic Bone Pain. J. Clin. Med. 2020, 9, 2622. [Google Scholar] [CrossRef] [PubMed]
- Bäck, T.A.; Jennbacken, K.; Hagberg Thulin, M.; Lindegren, S.; Jensen, H.; Olafsen, T.; Yazaki, P.J.; Palm, S.; Albertsson, P.; Damber, J.-E.; et al. Targeted Alpha Therapy with Astatine-211-Labeled Anti-PSCA A11 Minibody Shows Antitumor Efficacy in Prostate Cancer Xenografts and Bone Microtumors. EJNMMI Res. 2020, 10, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byun, B.H.; Kim, M.H.; Han, Y.-H.; Jeong, H.-J. KSNM60 in Non-Thyroidal Radionuclide Therapy: Leaping into the Future. Nucl. Med. Mol. Imaging 2021, 55, 203–209. [Google Scholar] [CrossRef]
- Liepe, K. 188Re-HEDP Therapy in the Therapy of Painful Bone Metastases. World J. Nucl. Med. 2018, 17, 133–138. [Google Scholar] [CrossRef]
- Cayir, D.; Araz, M. Radioiodine Therapy of Malignant Thyroid Diseases. In Radionuclide Treatments; Intech Open: London, UK, 2017. [Google Scholar]
- Gill, M.R.; Menon, J.U.; Jarman, P.J.; Owen, J.; Skaripa-Koukelli, I.; Able, S.; Thomas, J.A.; Carlisle, R.; Vallis, K.A. 111 In-Labelled Polymeric Nanoparticles Incorporating a Ruthenium-Based Radiosensitizer for EGFR-Targeted Combination Therapy in Oesophageal Cancer Cells. Nanoscale 2018, 10, 10596–10608. [Google Scholar] [CrossRef] [Green Version]
- Kong, G.; Hicks, R.J. PRRT for Higher-Grade Neuroendocrine Neoplasms: What Is Still Acceptable? Curr. Opin. Pharmacol. 2022, 67, 102293. [Google Scholar] [CrossRef]
- Gudkov, S.; Shilyagina, N.; Vodeneev, V.; Zvyagin, A. Targeted Radionuclide Therapy of Human Tumors. Int. J. Mol. Sci. 2015, 17, 33. [Google Scholar] [CrossRef]
- Lee, S.J.; Park, H.J. Single Photon Emission Computed Tomography (SPECT) or Positron Emission Tomography (PET) Imaging for Radiotherapy Planning in Patients with Lung Cancer: A Meta-Analysis. Sci. Rep. 2020, 10, 14864. [Google Scholar] [CrossRef]
- Park, M.; Kim, M.; Yoo, J.; Jo, M. Validation of the Whole-Body Counting Measurement in a Radiation Emergency. Appl. Radiat. Isot. 2021, 168, 109476. [Google Scholar] [CrossRef] [PubMed]
- Tashima, H.; Yamaya, T. Compton Imaging for Medical Applications. Radiol. Phys. Technol. 2022, 15, 187–205. [Google Scholar] [CrossRef] [PubMed]
- Andreo, P. Monte Carlo Simulations in Radiotherapy Dosimetry. Radiat. Oncol. 2018, 13, 121. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.; Park, B.; Lee, S.-S.; Kim, J.-E.; Han, S.-S.; Huh, K.-H.; Yi, W.-J.; Heo, M.-S.; Choi, S.-C. Efficacy of the Monte Carlo Method and Dose Reduction Strategies in Paediatric Panoramic Radiography. Sci. Rep. 2019, 9, 9691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraro, S.; Battistoni, G.; Kraan, A.C. Challenges in Monte Carlo Simulations as Clinical and Research Tool in Particle Therapy: A Review. Front. Phys. 2020, 8, 567800. [Google Scholar] [CrossRef]
- Sánchez-Doblado, F.; Leal, A.; Perucha, M.; Arráns, R.; Núñez, L.; Roselló, J.V.; Sánchez-Nieto, B.; Carrasco, E.; Gonzalez, A.; Medrano, J.C.; et al. Monte Carlo Clinical Dosimetry. Rep. Pract. Oncol. Radiother. 2002, 7, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Snyder, W.S.; Fisher, H.L.; Ford, M.R.; Warner, G.G. Estimates of Absorbed Fractions for Monoenergetic Photon Sources Uniformly Distributed in Various Organs of a Heterogeneous Phantom. J. Nucl. Med. 1969, 10 (Suppl. S3), 7–52. [Google Scholar]
- Dieudonné, A.; Hobbs, R.F.; Bolch, W.E.; Sgouros, G.; Gardin, I. Fine-Resolution Voxel S Values for Constructing Absorbed Dose Distributions at Variable Voxel Size. J. Nucl. Med. 2010, 51, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Siegel, J.A.; Thomas, S.R.; Stubbs, J.B.; Stabin, M.G.; Hays, M.T.; Koral, K.F.; Robertson, J.S.; Howell, R.W.; Wessels, B.W.; Fisher, D.R.; et al. MIRD Pamphlet No. 16: Techniques for Quantitative Radiopharmaceutical Biodistribution Data Acquisition and Analysis for Use in Human Radiation Dose Estimates. J. Nucl. Med. 1999, 40, 37S–61S. [Google Scholar]
- Bolch, W.E.; Bouchet, L.G.; Robertson, J.S.; Wessels, B.W.; Siegel, J.A.; Howell, R.W.; Erdi, A.K.; Aydogan, B.; Costes, S.; Watson, E.E.; et al. MIRD Pamphlet No. 17: The Dosimetry of Nonuniform Activity Distributions--Radionuclide S Values at the Voxel Level. Medical Internal Radiation Dose Committee. J. Nucl. Med. 1999, 40, 11S–36S. [Google Scholar]
- Fernández, M.; Hänscheid, H.; Mauxion, T.; Bardiès, M.; Kletting, P.; Glatting, G.; Lassmann, M. A Fast Method for Rescaling Voxel S Values for Arbitrary Voxel Sizes in Targeted Radionuclide Therapy from a Single Monte Carlo Calculation. Med. Phys. 2013, 40, 082502. [Google Scholar] [CrossRef] [PubMed]
- Dieudonné, A.; Hobbs, R.F.; Lebtahi, R.; Maurel, F.; Baechler, S.; Wahl, R.L.; Boubaker, A.; Le Guludec, D.; Sgouros, G.; Gardin, I. Study of the Impact of Tissue Density Heterogeneities on 3-Dimensional Abdominal Dosimetry: Comparison Between Dose Kernel Convolution and Direct Monte Carlo Methods. J. Nucl. Med. 2013, 54, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeedzadeh, E.; Sarkar, S.; Abbaspour Tehrani-Fard, A.; Ay, M.R.; Khosravi, H.R.; Loudos, G. 3D Calculation of Absorbed Dose for 131I-Targeted Radiotherapy: A Monte Carlo Study. Radiat. Prot. Dosim. 2012, 150, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, M.; Chiesa, C.; Flux, G.; Bardiès, M. EANM Dosimetry Committee Guidance Document: Good Practice of Clinical Dosimetry Reporting. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 192–200. [Google Scholar] [CrossRef]
- Hippeläinen, E.; Tenhunen, M.; Sohlberg, A. Fast Voxel-Level Dosimetry for 177 Lu Labelled Peptide Treatments. Phys. Med. Biol. 2015, 60, 6685–6700. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, M.; Sjögreen-Gleisner, K. The Accuracy of Absorbed Dose Estimates in Tumours Determined by Quantitative SPECT: A Monte Carlo Study. Acta Oncol. 2011, 50, 981–989. [Google Scholar] [CrossRef]
- Sandström, M.; Garske, U.; Granberg, D.; Sundin, A.; Lundqvist, H. Individualized Dosimetry in Patients Undergoing Therapy with 177Lu-DOTA-D-Phe1-Tyr3-Octreotate. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 212–225. [Google Scholar] [CrossRef]
- Amaya, H. Diffusion Processes in Tumors: A Nuclear Medicine Approach. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2016; p. 080015. [Google Scholar]
- Rani, N.; Singh, B.; Kumar, N.; Singh, P.; Hazari, P.P.; Vyas, S.; Hooda, M.; Chitkara, A.; Shekhawat, A.S.; Gupta, S.K.; et al. [ 99m Tc]-Bis-Methionine-DTPA Single-Photon Emission Computed Tomography Impacting Glioma Management: A Sensitive Indicator for Postsurgical/Chemoradiotherapy Response Assessment. Cancer Biother. Radiopharm. 2021, 36, 568–578. [Google Scholar] [CrossRef]
- Verma, A.; Hesterman, J.Y.; Chazen, J.L.; Holt, R.; Connolly, P.; Horky, L.; Vallabhajosula, S.; Mozley, P.D. Intrathecal 99m Tc-DTPA Imaging of Molecular Passage from Lumbar Cerebrospinal Fluid to Brain and Periphery in Humans. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2020, 12, e12030. [Google Scholar] [CrossRef]
- Santra, A.; Sharma, P.; Kumar, R. Use of 99m-Technetium-Glucoheptonate as a Tracer for Brain Tumor Imaging: An Overview of Its Strengths and Pitfalls. Indian J. Nucl. Med. 2015, 30, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kung, H.F. New Technetium 99m-Labeled Brain Perfusion Imaging Agents. Semin. Nucl. Med. 1990, 20, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Wängler, C.; Wängler, B.; Lehner, S.; Elsner, A.; Todica, A.; Bartenstein, P.; Hacker, M.; Schirrmacher, R. A Universally Applicable 68 Ga-Labeling Technique for Proteins. J. Nucl. Med. 2011, 52, 586–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Efferth, T.; Langguth, P. Transport Processes of Radiopharmaceuticals and -Modulators. Radiat. Oncol. 2011, 6, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porubcin, S.; Rovnakova, A.; Zahornacky, O.; Jarcuska, P. Diagnostic Value of Radioisotope Cisternography Using 111In-DTPA in a Patient with Rhinorrhea and Purulent Meningitis. Medicina 2022, 58, 714. [Google Scholar] [CrossRef]
- Gandhi, S.; Babu, S.; Subramanyam, P.; Sundaram, P. Tc-99m Macro Aggregated Albumin Scintigraphy—Indications Other than Pulmonary Embolism: A Pictorial Essay. Indian J. Nucl. Med. 2013, 28, 152. [Google Scholar] [CrossRef] [Green Version]
- Czernin, J.; Satyamurthy, N.; Schiepers, C. Molecular Mechanisms of Bone 18 F-NaF Deposition. J. Nucl. Med. 2010, 51, 1826–1829. [Google Scholar] [CrossRef] [Green Version]
- Itoh, K. Comparison of Methods for Determination of Glomerular Filtration Rate: Tc-99m-DTPA Renography, Predicted Creatinine Clearance Method and Plasma Sample Method. Ann. Nucl. Med. 2003, 17, 561–565. [Google Scholar] [CrossRef]
- Holcman, K.; Rubiś, P.; Stępień, A.; Graczyk, K.; Podolec, P.; Kostkiewicz, M. The Diagnostic Value of 99mTc-HMPAO-Labelled White Blood Cell Scintigraphy and 18F-FDG PET/CT in Cardiac Device-Related Infective Endocarditis—A Systematic Review. J. Pers. Med. 2021, 11, 1016. [Google Scholar] [CrossRef]
- Witney, T.H.; Kettunen, M.I.; Day, S.E.; Hu, D.; Neves, A.A.; Gallagher, F.A.; Fulton, S.M.; Brindle, K.M. A Comparison between Radiolabeled Fluorodeoxyglucose Uptake and Hyperpolarized 13C-Labeled Pyruvate Utilization as Methods for Detecting Tumor Response to Treatment. Neoplasia 2009, 11, 574–582. [Google Scholar] [CrossRef] [Green Version]
- Wangler, B.; Schirrmacher, R.; Bartenstein, P.; Wangler, C. Chelating Agents and Their Use in Radiopharmaceutical Sciences. Mini-Rev. Med. Chem. 2011, 11, 968–983. [Google Scholar] [CrossRef]
- Okarvi, S.M. Recent Developments in 99Tcm-Labelled Peptide-Based Radiopharmaceuticals. Nucl. Med. Commun. 1999, 20, 1093–1112. [Google Scholar] [CrossRef] [PubMed]
- Dijkgraaf, I.; Agten, S.M.; Bauwens, M.; Hackeng, T.M. Strategies for Site-Specific Radiolabeling of Peptides and Proteins. In Radiopharmaceuticals—Current Research for Better Diagnosis and Therapy; IntechOpen: London, UK, 2022. [Google Scholar]
- Price, E.W.; Orvig, C. Matching Chelators to Radiometals for Radiopharmaceuticals. Chem. Soc. Rev. 2014, 43, 260–290. [Google Scholar] [CrossRef] [PubMed]
- Lozza, C.; Navarro-Teulon, I.; Pèlegrin, A.; Pouget, J.-P.; Vivès, E. Peptides in Receptor-Mediated Radiotherapy: From Design to the Clinical Application in Cancers. Front. Oncol. 2013, 3, 247. [Google Scholar] [CrossRef] [Green Version]
- Knapp, F.F.; Dash, A. Radiopharmaceuticals for Therapy; Springer: New Delhi, India, 2016; ISBN 978-81-322-2606-2. [Google Scholar]
- Bronstein, M.D. Acromegaly: Molecular Expression of Somatostatin Receptor Subtypes and Treatment Outcome. In Pituitary Today: Molecular, Physiological and Clinical Aspects; KARGER: Basel, Switzerland, 2006; pp. 129–134. [Google Scholar]
- de Herder, W.W.; Rehfeld, J.F.; Kidd, M.; Modlin, I.M. A Short History of Neuroendocrine Tumours and Their Peptide Hormones. Best Pract. Res. Clin. Endocrinol. Metab. 2016, 30, 3–17. [Google Scholar] [CrossRef]
- Bauer, W.; Briner, U.; Doepfner, W.; Haller, R.; Huguenin, R.; Marbach, P.; Petcher, T.J.; Pless, J. SMS 201–995: A Very Potent and Selective Octapeptide Analogue of Somatostatin with Prolonged Action. Life Sci. 1982, 31, 1133–1140. [Google Scholar] [CrossRef]
- Reubi, J.C.; Maurer, R. Autoradiographic Mapping of Somatostatin Receptors in the Rat Central Nervous System and Pituitary. Neuroscience 1985, 15, 1183–1193. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, S.W.; Reubi, J.C.; Bakker, W.H.; Krenning, E.P. Somatostatin Receptor Imaging with 123I-Tyr3-Octreotide. Z. Gastroenterol. 1990, 28 (Suppl. S2), 20–21. [Google Scholar]
- Bakker, W.H.; Albert, R.; Bruns, C.; Breeman, W.A.P.; Hofland, L.J.; Marbach, P.; Pless, J.; Pralet, D.; Stolz, B.; Koper, J.W.; et al. [111In-DTPA-D-Phe1]-Octreotide, a Potential Radiopharmaceutical for Imaging of Somatostatin Receptor-Positive Tumors: Synthesis, Radiolabeling and in Vitro Validation. Life Sci. 1991, 49, 1583–1591. [Google Scholar] [CrossRef]
- Krenning, E.P.; Kwekkeboom, D.J.; Bakker, W.H.; Breeman, W.A.P.; Kooij, P.P.M.; Oei, H.Y.; van Hagen, M.; Postema, P.T.E.; de Jong, M.; Reubi, J.C.; et al. Somatostatin Receptor Scintigraphy with [111In-DTPA-d-Phe1]- and [123I-Tyr3]-Octreotide: The Rotterdam Experience with More than 1000 Patients. Eur. J. Nucl. Med. 1993, 20, 716–731. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, M.; Kasi, A. Octreotide Scan; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Fani, M.; Mansi, R.; Nicolas, G.P.; Wild, D. Radiolabeled Somatostatin Analogs—A Continuously Evolving Class of Radiopharmaceuticals. Cancers 2022, 14, 1172. [Google Scholar] [CrossRef]
- Bushnell, D.L.; Menda, Y.; Madsen, M.T.; Link, B.K.; Kahn, D.; Truhlar, S.M.; Juweid, M.; Shannon, M.; Murguia, J.S. 99mTc-Depreotide Tumour Uptake in Patients with Non-Hodgkin’s Lymphoma. Nucl. Med. Commun. 2004, 25, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Behnammanesh, H.; Jokar, S.; Erfani, M.; Geramifar, P.; Sabzevari, O.; Amini, M.; Mazidi, S.M.; Hajiramezanali, M.; Beiki, D. Design, Preparation and Biological Evaluation of a 177Lu-Labeled Somatostatin Receptor Antagonist for Targeted Therapy of Neuroendocrine Tumors. Bioorg. Chem. 2020, 94, 103381. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Cheng, Y.; Zang, J.; Sui, H.; Wang, H.; Jacobson, O.; Zhu, Z.; Chen, X. Dose Escalation of an Evans Blue–Modified Radiolabeled Somatostatin Analog 177Lu-DOTA-EB-TATE in the Treatment of Metastatic Neuroendocrine Tumors. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, H.; Jacobson, O.; Cheng, Y.; Niu, G.; Li, F.; Bai, C.; Zhu, Z.; Chen, X. Safety, Pharmacokinetics, and Dosimetry of a Long-Acting Radiolabeled Somatostatin Analog 177 Lu-DOTA-EB-TATE in Patients with Advanced Metastatic Neuroendocrine Tumors. J. Nucl. Med. 2018, 59, 1699–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballal, S.; Yadav, M.P.; Bal, C.; Sahoo, R.K.; Tripathi, M. Broadening Horizons with 225Ac-DOTATATE Targeted Alpha Therapy for Gastroenteropancreatic Neuroendocrine Tumour Patients Stable or Refractory to 177Lu-DOTATATE PRRT: First Clinical Experience on the Efficacy and Safety. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 934–946. [Google Scholar] [CrossRef]
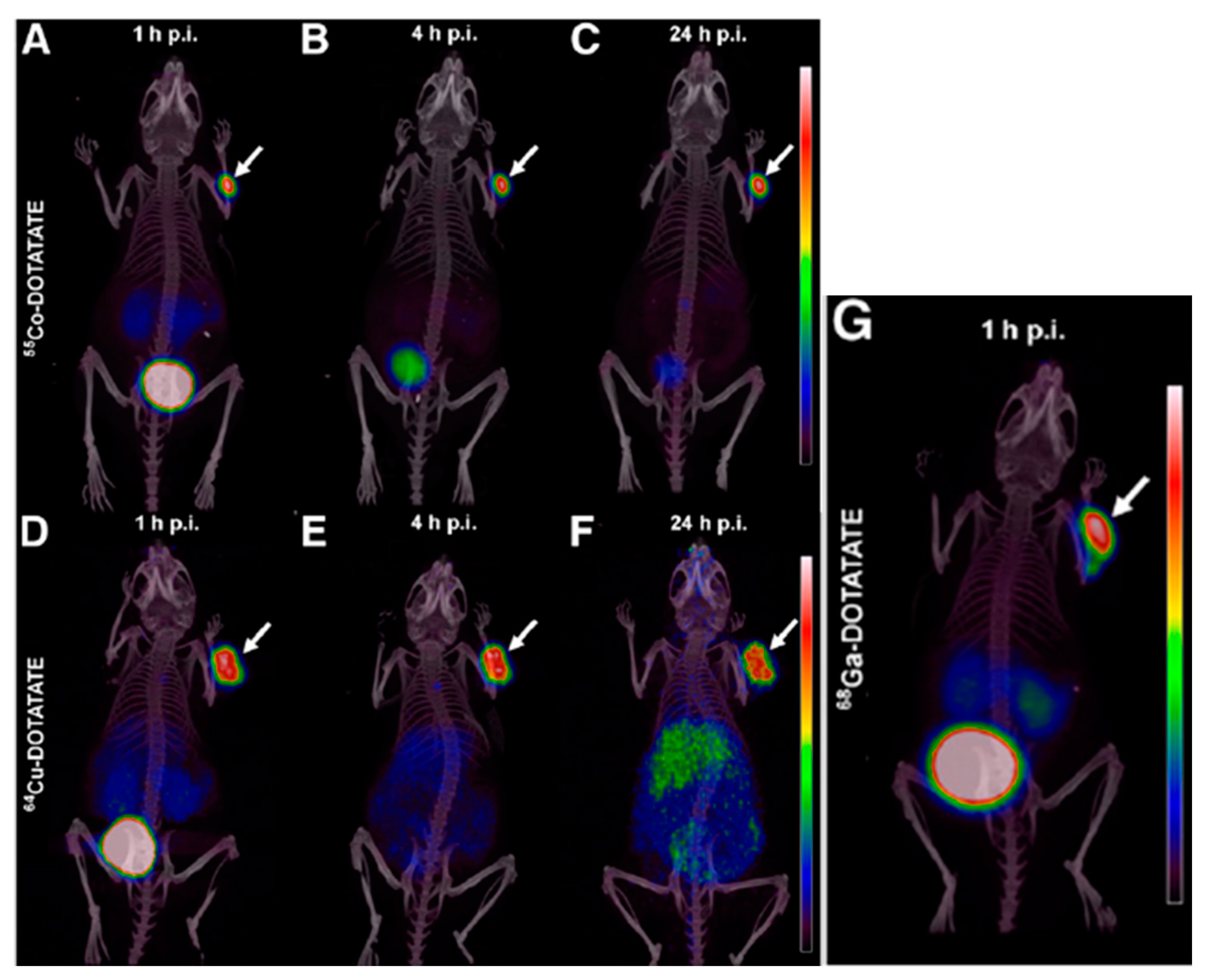
- Andersen, T.L.; Baun, C.; Olsen, B.B.; Dam, J.H.; Thisgaard, H. Improving Contrast and Detectability: Imaging with [55 Co]Co-DOTATATE in Comparison with [64 Cu]Cu-DOTATATE and [68 Ga]Ga-DOTATATE. J. Nucl. Med. 2020, 61, 228–233. [Google Scholar] [CrossRef] [Green Version]
- de Jong, M.; Breeman, W.A.P.; Bernard, B.F.; Bakker, W.H.; Visser, T.J.; Kooij, P.P.M.; van Gameren, A.; Krenning, E.P. Tumor Response After [90Y-DOTA0,Tyr3]Octreotide Radionuclide Therapy in a Transplantable Rat Tumor Model Is Dependent on Tumor Size. J. Nucl. Med. 2001, 42, 1841. [Google Scholar]
- Capello, A.; Krenning, E.P.; Breeman, W.A.P.; Bernard, B.F.; Konijnenberg, M.W.; de Jong, M. Tyr 3 -Octreotide and Tyr 3 -Octreotate Radiolabeled with 177 Lu or 90 Y: Peptide Receptor Radionuclide Therapy Results In Vitro. Cancer Biother. Radiopharm. 2003, 18, 761–768. [Google Scholar] [CrossRef]
- Zemczak, A.; Gut, P.; Pawlak, D.; Kołodziej, M.; Królicki, L.; Kos-Kudła, B.; Ruchała, M.; Kamiński, G.; Kunikowska, J. The Safety and Efficacy of the Repeated PRRT with [90Y]Y/[177Lu]Lu-DOTATATE in Patients with NET. Int. J. Endocrinol. 2021, 2021, 6615511. [Google Scholar] [CrossRef]
- Schaarschmidt, B.M.; Wildgruber, M.; Kloeckner, R.; Nie, J.; Steinle, V.; Braat, A.J.A.T.; Lohoefer, F.; Kim, H.S.; Lahner, H.; Weber, M.; et al. 90 Y Radioembolization in the Treatment of Neuroendocrine Neoplasms: Results of an International Multicenter Retrospective Study. J. Nucl. Med. 2022, 63, 679–685. [Google Scholar] [CrossRef]
- Bushnell, D.L.; Bodeker, K.L.; O’Dorisio, T.M.; Madsen, M.T.; Menda, Y.; Graves, S.; Zamba, G.K.D.; O’Dorisio, M.S. Addition of 131 I-MIBG to PRRT (90 Y-DOTATOC) for Personalized Treatment of Selected Patients with Neuroendocrine Tumors. J. Nucl. Med. 2021, 62, 1274–1277. [Google Scholar] [CrossRef] [PubMed]
- Cakir, M.; Dworakowska, D.; Grossman, A. Somatostatin Receptor Biology in Neuroendocrine and Pituitary Tumours: Part 1—Molecular Pathways. J. Cell. Mol. Med. 2010, 14, 2570–2584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogoza, O.; Megnis, K.; Kudrjavceva, M.; Gerina-Berzina, A.; Rovite, V. Role of Somatostatin Signalling in Neuroendocrine Tumours. Int. J. Mol. Sci. 2022, 23, 1447. [Google Scholar] [CrossRef]
- Alessandrini, L.; Ferrari, M.; Taboni, S.; Sbaraglia, M.; Franz, L.; Saccardo, T.; Del Forno, B.M.; Agugiaro, F.; Frigo, A.C.; Dei Tos, A.P.; et al. Tumor-Stroma Ratio, Neoangiogenesis and Prognosis in Laryngeal Carcinoma. A Pilot Study on Preoperative Biopsies and Matched Surgical Specimens. Oral Oncol. 2022, 132, 105982. [Google Scholar] [CrossRef] [PubMed]
- Mina-Osorio, P. The Moonlighting Enzyme CD13: Old and New Functions to Target. Trends Mol. Med. 2008, 14, 361–371. [Google Scholar] [CrossRef]
- Pasqualini, R.; Koivunen, E.; Kain, R.; Lahdenranta, J.; Sakamoto, M.; Stryhn, A.; Ashmun, R.A.; Shapiro, L.H.; Arap, W.; Ruoslahti, E. Aminopeptidase N Is a Receptor for Tumor-Homing Peptides and a Target for Inhibiting Angiogenesis. Cancer Res. 2000, 60, 722–727. [Google Scholar]
- Kis, A.; Dénes, N.; Szabó, J.P.; Arató, V.; Beke, L.; Matolay, O.; Enyedi, K.N.; Méhes, G.; Mező, G.; Bai, P.; et al. In Vivo Molecular Imaging of the Efficacy of Aminopeptidase N (APN/CD13) Receptor Inhibitor Treatment on Experimental Tumors Using 68Ga-NODAGA-c(NGR) Peptide. Biomed Res. Int. 2021, 2021, 6642973. [Google Scholar] [CrossRef]
- Israel, I.; Elflein, K.; Schirbel, A.; Chen, K.; Samnick, S. A Comparison of the Monomeric [68Ga]NODAGA-NGR and Dimeric [68Ga]NOTA-(NGR)2 as Aminopeptidase N Ligand for Positron Emission Tomography Imaging in Tumor-Bearing Mice. Eur. J. Pharm. Sci. 2021, 166, 105964. [Google Scholar] [CrossRef]
- Graziadio, A.; Zanda, M.; Frau, S.; Fleming, I.N.; Musolino, M.; Dall’Angelo, S.; Baldassarre, M.; Piras, M. NGR Tumor-Homing Peptides: Structural Requirements for Effective APN (CD13) Targeting. Bioconjug. Chem. 2016, 27, 1332–1340. [Google Scholar] [CrossRef] [Green Version]
- Gyuricza, B.; Szabó, J.P.; Arató, V.; Dénes, N.; Szűcs, Á.; Berta, K.; Kis, A.; Szücs, D.; Forgács, V.; Szikra, D.; et al. Synthesis of 68Ga-Labeled CNGR-Based Glycopeptides and In Vivo Evaluation by PET Imaging. Pharmaceutics 2021, 13, 2103. [Google Scholar] [CrossRef]
- Kis, A.; Dénes, N.; Szabó, J.P.; Arató, V.; Jószai, I.; Enyedi, K.N.; Lakatos, S.; Garai, I.; Mező, G.; Kertész, I.; et al. In Vivo Assessment of Aminopeptidase N (APN/CD13) Specificity of Different 68Ga-Labelled NGR Derivatives Using PET/MRI Imaging. Int. J. Pharm. 2020, 589, 119881. [Google Scholar] [CrossRef] [PubMed]
- Surowiak, P.; Drąg, M.; Materna, V.; Suchocki, S.; Grzywa, R.; Spaczyński, M.; Dietel, M.; Oleksyszyn, J.; Zabel, M.; Lage, H. Expression of Aminopeptidase N/CD13 in Human Ovarian Cancers. Int. J. Gynecol. Cancer 2006, 16, 1783–1788. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Zhang, Z.; Liu, K.; Ye, L.; Liang, Y.; Gu, W. Aminopeptidase N (CD13) Targeted MR and NIRF Dual-Modal Imaging of Ovarian Tumor Xenograft. Mater. Sci. Eng. C 2018, 93, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, J.; Zou, H.; Shen, Y.; Deng, S.; Wu, Y. Synthesis and Evaluation of 68 Ga-Labeled Dimeric CNGR Peptide for PET Imaging of CD13 Expression with Ovarian Cancer Xenograft. J. Cancer 2021, 12, 244–252. [Google Scholar] [CrossRef]
- Crowley, F.; Sterpi, M.; Buckley, C.; Margetich, L.; Handa, S.; Dovey, Z. A Review of the Pathophysiological Mechanisms Underlying Castration-Resistant Prostate Cancer. Res. Rep. Urol. 2021, 13, 457–472. [Google Scholar] [CrossRef]
- Cyrta, J.; Augspach, A.; De Filippo, M.R.; Prandi, D.; Thienger, P.; Benelli, M.; Cooley, V.; Bareja, R.; Wilkes, D.; Chae, S.-S.; et al. Role of Specialized Composition of SWI/SNF Complexes in Prostate Cancer Lineage Plasticity. Nat. Commun. 2020, 11, 5549. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Chen, Z.; Fu, F.; Li, F.; Zhu, Z.; Yang, Y.; Chen, X.; Jia, B.; Zheng, S.; Huang, C.; Miao, W. Comparison of [99mTc]3PRGD2 Imaging and [18F]FDG PET/CT in Breast Cancer and Expression of Integrin Avβ3 in Breast Cancer Vascular Endothelial Cells. Mol. Imaging Biol. 2018, 20, 846–856. [Google Scholar] [CrossRef]
- Zhao, Y.; Bachelier, R.; Treilleux, I.; Pujuguet, P.; Peyruchaud, O.; Baron, R.; Clément-Lacroix, P.; Clézardin, P. Tumor Avβ3 Integrin Is a Therapeutic Target for Breast Cancer Bone Metastases. Cancer Res. 2007, 67, 5821–5830. [Google Scholar] [CrossRef] [Green Version]
- Rolli, M.; Fransvea, E.; Pilch, J.; Saven, A.; Felding-Habermann, B. Activated Integrin Avβ3 Cooperates with Metalloproteinase MMP-9 in Regulating Migration of Metastatic Breast Cancer Cells. Proc. Natl. Acad. Sci. USA 2003, 100, 9482–9487. [Google Scholar] [CrossRef] [Green Version]
- Sloan, E.K.; Pouliot, N.; Stanley, K.L.; Chia, J.; Moseley, J.M.; Hards, D.K.; Anderson, R.L. Tumor-Specific Expression of Alphavbeta3 Integrin Promotes Spontaneous Metastasis of Breast Cancer to Bone. Breast Cancer Res. 2006, 8, R20. [Google Scholar] [CrossRef] [Green Version]
- Pauwels, E.; Cleeren, F.; Tshibangu, T.; Koole, M.; Serdons, K.; Dekervel, J.; Van Cutsem, E.; Verslype, C.; Van Laere, K.; Bormans, G.; et al. [18F]AlF-NOTA-Octreotide PET Imaging: Biodistribution, Dosimetry and First Comparison with [68Ga]Ga-DOTATATE in Neuroendocrine Tumour Patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 3033–3046. [Google Scholar] [CrossRef] [PubMed]
- Okarvi, S.M. Peptide-Based Radiopharmaceuticals: Future Tools for Diagnostic Imaging of Cancers and Other Diseases. Med. Res. Rev. 2004, 24, 357–397. [Google Scholar] [CrossRef]
- Kelkar, S.S.; Reineke, T.M. Theranostics: Combining Imaging and Therapy. Bioconjug. Chem. 2011, 22, 1879–1903. [Google Scholar] [CrossRef] [PubMed]
- Kumar, C.; Jayakumar, S.; Pandey, B.; Samuel, G.; Venkatesh, M. Cellular and Molecular Effects of Beta Radiation from I-131 on Human Tumor Cells a Comparison with Gamma Radiation. Curr. Radiopharm. 2014, 7, 138–143. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radionuclide | Half-Life | Therapeutic Decay | Daughter Nuclide | Clinical Application | Ref. |
|---|---|---|---|---|---|
| 32P | 14.26 days | β− | 32S | Myeloproliferative neoplasms | [71] |
| 89Sr | 50.53 days | β− | 89Y | Osseous (bony) metastases of bone cancer | [72] |
| 90Y | 64.10 h | β− | 90Zr | Liver tumours, primary hepatocellular carcinoma (HCC), and unresectable primary colorectal cancer | [73,74,75] |
| 166Ho | 26.76 h | β− | 166Er | NETs, colorectal cancer, small hepatocellular carcinoma (SCC) | [76,77,78] |
| 117mSn | 13.60 days | Isomeric transition | 117Sn | Bone metastases | [79] |
| 99mTc | 6.00 h | Isomeric transition | 99Tc | HER2-positive breast cancer | [80] |
| 177Lu | 6.6 days | β− | 177Hf | Metastatic castration-resistant prostate cancer | [81] |
| 223Ra | 11.4 days | α | 219Rn | Advanced prostate cancer with bone metastases | [82] |
| 227Th | 18.7 days | α | 223Ra | Haematological cancers, including CD22-positive B cell cancers and CD33-positive leukaemia | [83] |
| 153Sm | 46.2 h | β− | 153Eu | Metastatic bone disease | [84] |
| 211At | 7.2 h | α | 207Bi | Bone microtumours | [85] |
| 188Re | 16.9 h | β− | 188Os | Painful bone metastases Medullary carcinoma | [86,87] |
| 131I | 8.0 days | β− | 131Xe | Thyroid cancer | [88] |
| 111In | 2.80 days | Electron capture | 111Cd | Oesophageal cancer | [89] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chakraborty, K.; Mondal, J.; An, J.M.; Park, J.; Lee, Y.-K. Advances in Radionuclides and Radiolabelled Peptides for Cancer Therapeutics. Pharmaceutics 2023, 15, 971. https://doi.org/10.3390/pharmaceutics15030971
Chakraborty K, Mondal J, An JM, Park J, Lee Y-K. Advances in Radionuclides and Radiolabelled Peptides for Cancer Therapeutics. Pharmaceutics. 2023; 15(3):971. https://doi.org/10.3390/pharmaceutics15030971
Chicago/Turabian StyleChakraborty, Kushal, Jagannath Mondal, Jeong Man An, Jooho Park, and Yong-Kyu Lee. 2023. "Advances in Radionuclides and Radiolabelled Peptides for Cancer Therapeutics" Pharmaceutics 15, no. 3: 971. https://doi.org/10.3390/pharmaceutics15030971
APA StyleChakraborty, K., Mondal, J., An, J. M., Park, J., & Lee, Y. -K. (2023). Advances in Radionuclides and Radiolabelled Peptides for Cancer Therapeutics. Pharmaceutics, 15(3), 971. https://doi.org/10.3390/pharmaceutics15030971