
Cannabinoid-Based Ocular Therapies and Formulations

Abstract
:1. Introduction
2. Ocular Drug Delivery
Properties of Ocular Drug Delivery Nanosystems
3. Vehiculated Cannabinoids for Ocular Pathologies
3.1. Glaucoma
3.1.1. Therapeutic Potential of Cannabinoids on Glaucoma and Limitations of Conventional Formulations

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Targeted Disease | Cannabinoid | Formulation | Main Outcome | Reference |
|---|---|---|---|---|
| Glaucoma | Δ9-THC | Mineral oil | No reduction in IOP levels, side effects (burning sensation, tearing, lid swelling) | [72,80] |
| Tocrisolve® (commercial soybean oil emulsion (1:4 oil-in-water) stabilized by Pluronic-F68) | Sex-dependent IOP decrease; 28% IOP peak reduction persisting at least 8 h in male mice, persisting 4 h in female mice | [71] | ||
| THC-VHS, Δ9-THC | Tocrisolve® (commercial soybean oil emulsion (1:4 oil-in-water) stabilized by Pluronic-F68) | 36% IOP peak reduction for 2 h with Δ9-THC; 47% IOP peak reduction for 4 h with THC-VHS, resulting in IOP-modulating effect similar to commercial formulations but with shorter duration (2 h vs. 6 h) | [82] | |
| Δ8-THC | NEs (soybean oil, oleic acid, phospholipids, poloxamer, α-tocopherol, glycerin) | Marked and prolonged (over 8 h) decrease in IOP in normo- and hypertensive rabbits | [85] | |
| THC-VHS | NEs (sesame oil, polysorbate 80, poloxamer®188), alone and combined with a mucoadhesive agent (Carbopol®) | Higher and longer prolonged decrease in IOP vs. standard commercial treatments in New Zealand rabbits; high concentrations of polysorbate 80 led to diminished effect, attributed to THC entrapment in surfactant micelles decreasing permeation and release | [39] | |
| SLNs (Compritol 888 ATO, Pluronic F-68, polysorbate 80, glycerin) | Improved residence time and bioavailability; IOP peak decrease (31%) with longer prolonged effect (480 min) than standard commercial treatments (120 and 180 min of pilocarpine and timolol maleate, respectively) | [40] | ||
| CBD | Tocrisolve® (commercial soybean oil emulsion (1:4 oil-in-water) stabilized by Pluronic-F68) | IOP increase, prevention of THC IOP-decreasing effect | [71] | |
| NEs (sesame oil, polysorbate 80, poloxamer®188), alone and combined with a mucoadhesive agent (Carbopol®) | IOP peak reduction (19.9%) maintained for up to 300 min in normotensive rabbits | [38] | ||
| WIN55212-1 | 45% w/v 2-hydroxylpropyl-β-cyclodextrin in pH 7.4 adjusted saline | 31% IOP peak reduction within 1 h after single administration, maintained for 2 h | [66] | |
| CBGA | PEO/PLA NPs in an in situ gelling hyaluronic acid (HA) and methylcellulose (MC) hydrogel | 300-fold higher corneal penetration ex vivo in porcine whole eyes vs. CBGA in mineral oil, accounting for 0.015% of applied CBGA | [44] | |
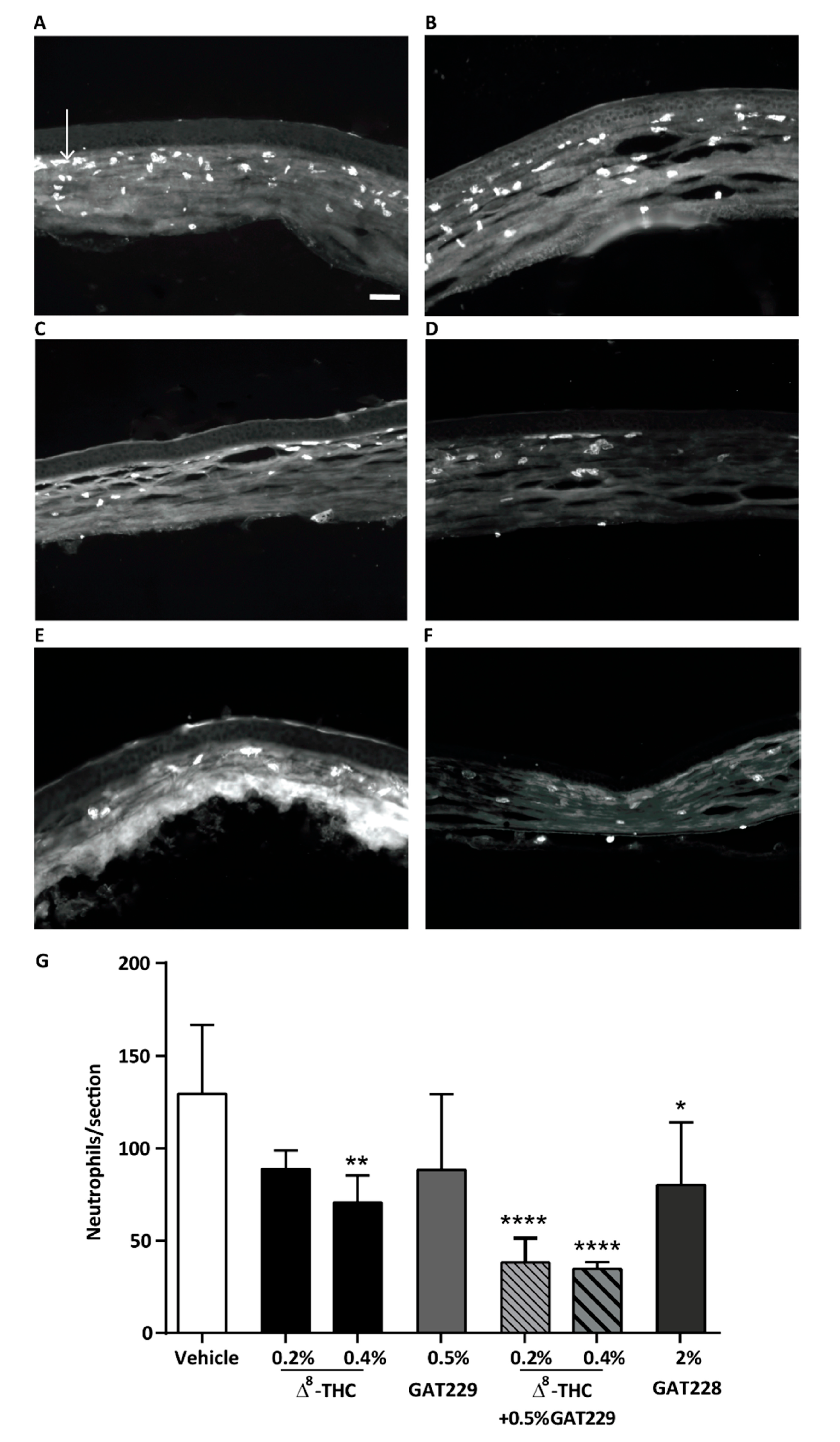
| Keratitis | Δ8-THC, CBD and HU-308 | Soybean oil | Reduced pain scores, neutrophil infiltration and inflammation | [86] |
| CB1 allosteric ligand GAT211 and enantiomers GAT228 and GAT229, Δ8-THC | Soybean oil with 2% DMSO and 4% Tween 20 | Reduced pain scores (GAT228), reduced corneal inflammation (GAT228 and GAT228 with Δ8-THC | [87] | |
| CBD | Mucoadhesive micelles of chitosan/poly(vinyl alcohol) and poly(methyl methacrylate) | Permeation through human cell corneal epithelium monolayer in vitro, up to 86% and 53% of applied CBD reaching the acceptor compartment in liquid–liquid and air–liquid exposition, respectively | [45] | |
| NEs (medium-chain triglycerides (MCT), polysorbate 80 and Solutol® HS 15), antioxidants propyl gallate or butylhydroxytoluene | Decrease in key inflammatory cytokines and IOP, not following a standard sigmoidal dose–response | [76] | ||
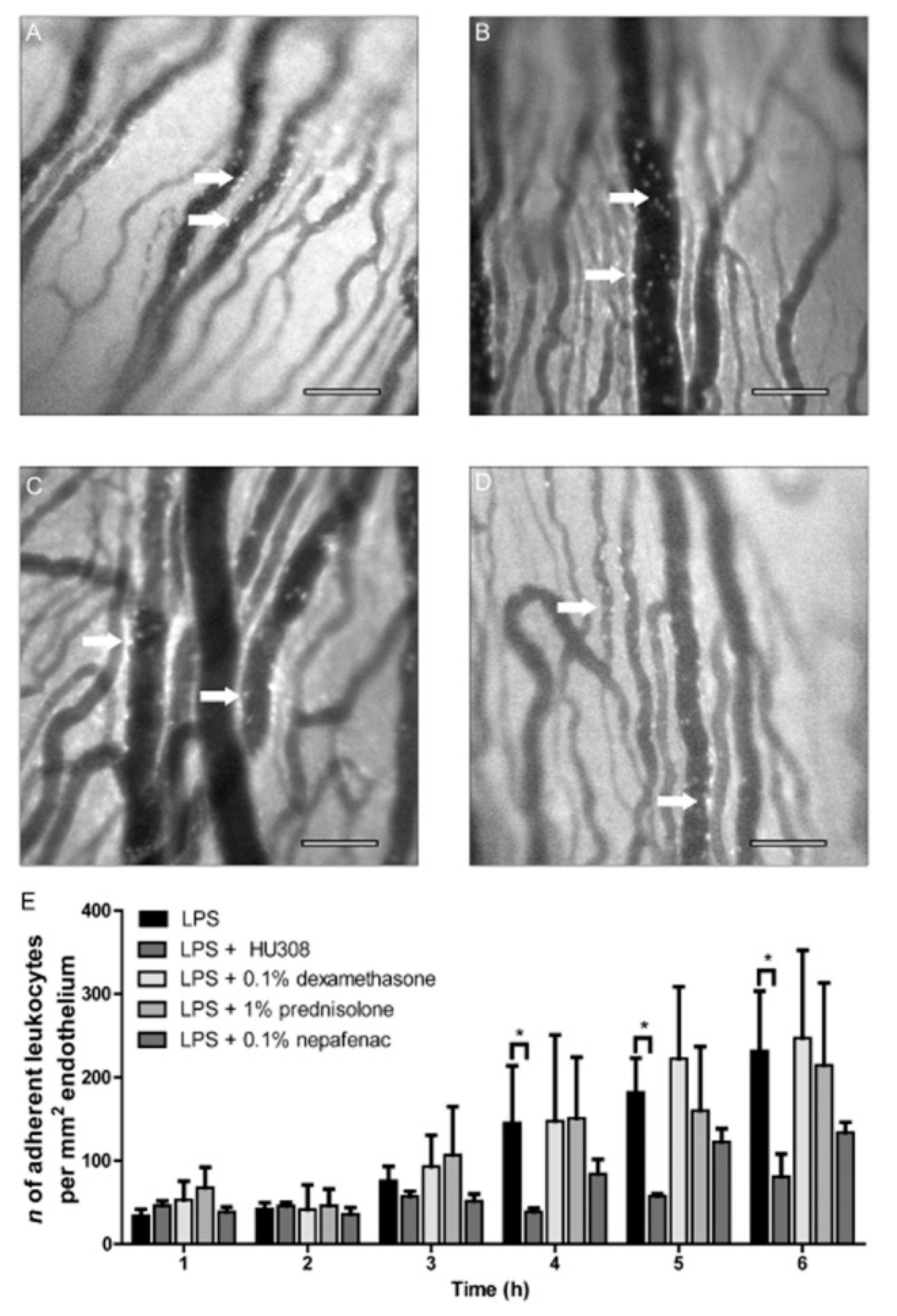
| Uveitis | HU308 | Tocrisolve® (commercial soybean oil emulsion (1:4 oil-in-water) stabilized by Pluronic-F68) | Reduced leukocyte levels in the iris microvasculature, decreased proinflammatory mediators, higher anti-inflammatory effects vs. reference compounds (nepafenac, dexamethasone, predinosolone) | [84,88] |
| RO6871304, RO6871085, HU910 | Tocrisolve® (commercial soybean oil emulsion (1:4 oil-in-water) stabilized by Pluronic-F68) | Attenuated leukocyte adhesion to the iris microvasculature | [89] | |
| Dry Eye Syndrome | Δ9-THC | 15% w/v DMSO and 10% w/v Cremophore EL in saline | Protected corneal nerve morphology, maintained corneal sensitivity, reduced infiltration of inflammatory CD4+ T cells | [90] |
| Δ8-THC, CBD, and HU-308 | Soybean oil | Antinociceptive and anti-inflammatory effects | [86,87] |
3.1.2. Recent Advances of Nanosystems in Enhancing Therapeutic Effects of Cannabinoids on Glaucoma
3.2. Keratitis
3.3. Uveitis
3.4. Dry Eye Syndrome
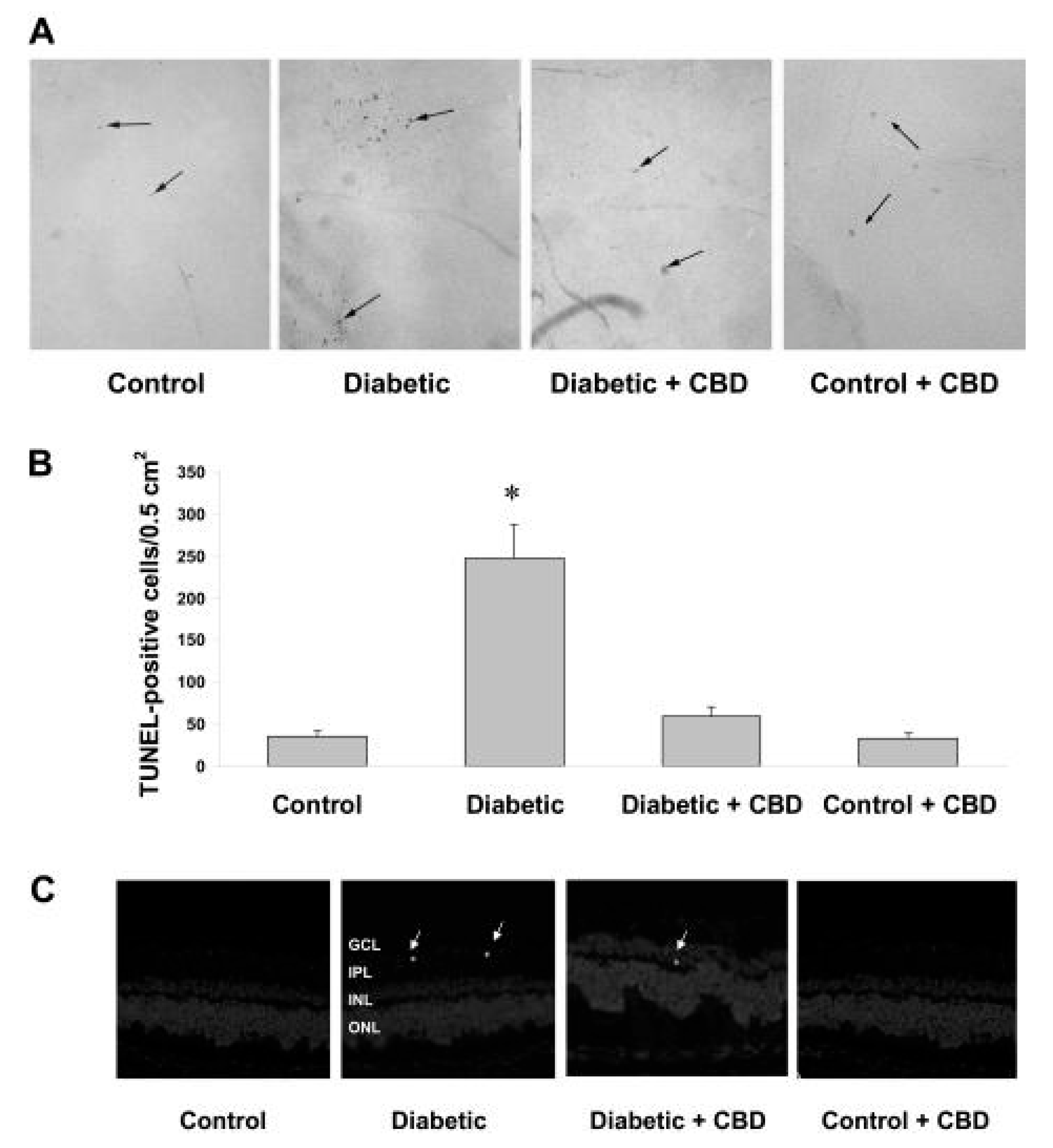
3.5. Diabetic Retinopathy
3.6. Ocular Damage Caused by Pseudomonas aeruginosa Biofilms in Contact Lenses
4. Other Cannabinoid Advanced Vehiculation Strategies and Considerations for Ocular Applications
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vasantha Rupasinghe, H.P.; Davis, A.; Kumar, S.K.; Murray, B.; Zheljazkov, V.D. Industrial Hemp (Cannabis Sativa Subsp. Sativa) as an Emerging Source for Value-Added Functional Food Ingredients and Nutraceuticals. Molecules 2020, 25, 4078. [Google Scholar] [CrossRef] [PubMed]
- Zuardi, A.W. History of Cannabis as a Medicine: A Review. Rev. Bras. Psiquiatr. 2006, 28, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Chandra, S.; Radwan, M.M.; Majumdar, C.G.; Church, J.C.; Freeman, T.P.; ElSohly, M.A. New Trends in Cannabis Potency in USA and Europe during the Last Decade (2008–2017). Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 5–15. [Google Scholar] [CrossRef]
- Razdan, C.K.; Razdan, R.K.; Prog, B.; Mechoulam, R.K.; Mechoulam, R.; Mccallum, R.; Burstein, N.K.; Archer, S.; Boyd, R.A.; Demarco, D.B.; et al. Marijuana, Chemistry, Pharmacology, Metabolism and Clinical Effects; Academic Press: Cambridge, MA, USA, 1981; Volume 46. [Google Scholar]
- Schlag, A.K.; Zafar, R.R.; Lynskey, M.T.; Athanasiou-Fragkouli, A.; Phillips, L.D.; Nutt, D.J. The Value of Real World Evidence: The Case of Medical Cannabis. Front. Psychiatry 2022, 13, 2489. [Google Scholar] [CrossRef]
- Modaresi, F.; Talachian, K. The Characteristics of Clinical Trials on Cannabis and Cannabinoids: A Review of Trials for Therapeutic or Drug Development Purposes. Pharmaceut. Med. 2022, 36, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.; Goodman, S.; Wadsworth, E.; Rynard, V.; Boudreau, C.; Hall, W. Evaluating the Impacts of Cannabis Legalization: The International Cannabis Policy Study. Int. J. Drug Policy 2020, 77, 102698. [Google Scholar] [CrossRef]
- Groce, E. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. J. Med. Regul. 2017, 104, 32. [Google Scholar] [CrossRef] [Green Version]
- Schussel, V.; Kenzo, L.; Santos, A.; Bueno, J.; Yoshimura, E.; de Oliveira Cruz Latorraca, C.; Pachito, D.V.; Riera, R. Cannabinoids for Nausea and Vomiting Related to Chemotherapy: Overview of Systematic Reviews. Phyther. Res. 2018, 32, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.N.; Mueller, M.; Sauls, R.S. Cannaboinoid Antiemetic Therapy; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Zaami, S.; Di Luca, A.; Di Luca, N.M.; Montanari Vergallo, G. Medical Use of Cannabis: Italian and European Legislation. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.; Cannas, C.; Rivetti, M.S.; Villa, C.; Rebesco, B. Innovative Clinical-Organizational Model to Ensure Appropriateness and Quality in the Management of Medical Cannabis: An Italian Regional Case. Healthcare 2021, 9, 1425. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Liu, J.; Liu, Z.; Zhou, H. Immune Modulating Nanoparticles for the Treatment of Ocular Diseases. J. Nanobiotechnol. 2022, 20, 496. [Google Scholar] [CrossRef] [PubMed]
- Dasram, M.H.; Walker, R.B.; Khamanga, S.M. Recent Advances in Endocannabinoid System Targeting for Improved Specificity: Strategic Approaches to Targeted Drug Delivery. Int. J. Mol. Sci. 2022, 23, 13223. [Google Scholar] [CrossRef]
- Aiello, F.; Afflitto, G.G.; Li, J.P.O.; Martucci, A.; Cesareo, M.; Nucci, C. Cannabineyeds: The Endocannabinoid System as a Regulator of the Ocular Surface Nociception, Inflammatory Response, Neovascularization and Wound Healing. J. Clin. Med. 2020, 9, 4036. [Google Scholar] [CrossRef]
- Wang, M.T.M.; Danesh-Meyer, H.V. Cannabinoids and the Eye. Surv. Ophthalmol. 2021, 66, 327–345. [Google Scholar] [CrossRef]
- Durán-Lobato, M.; Álvarez-Fuentes, J.; Fernández-Arévalo, M.; Martín-Banderas, L. Receptor-Targeted Nanoparticles Modulate Cannabinoid Anticancer Activity through Delayed Cell Internalization. Sci. Rep. 2022, 12, 1297. [Google Scholar] [CrossRef]
- Martín-Banderas, L.; Muñoz-Rubio, I.; Álvarez-Fuentes, J.; Durán-Lobato, M.; Arias, J.L.; Holgado, M.Á.; Fernández-Arévalo, M. Engineering of Δ9-Tetrahydrocannabinol Delivery Systems Based on Surface Modified-PLGA Nanoplatforms. Colloids Surf. B Biointerfaces 2014, 123, 114–122. [Google Scholar] [CrossRef]
- da Silva, A.; Lepetre-Mouelhi, S.; Couvreur, P. Micro- and Nanocarriers for Pain Alleviation. Adv. Drug Deliv. Rev. 2022, 187, 114359. [Google Scholar] [CrossRef] [PubMed]
- Bar-Hai, A.; Domb, A.J.; Hoffman, A. Strategies for Enhancing the Oral Bioavailability of Cannabinoids. Expert Opin. Drug Metab. Toxicol. 2022, 18, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Reimondez-Troitiño, S.; Csaba, N.; Alonso, M.J.; De La Fuente, M. Nanotherapies for the Treatment of Ocular Diseases. Eur. J. Pharm. Biopharm. 2015, 95, 279–293. [Google Scholar] [CrossRef]
- Durán-Lobato, M.; Niu, Z.; Alonso, M.J. Oral Delivery of Biologics for Precision Medicine. Adv. Mater. 2019, 32, e1901935. [Google Scholar] [CrossRef]
- Wood, R.W.; Li, V.H.K.; Kreuter, J.; Robinson, J.R. Ocular Disposition of Poly-Hexyl-2-Cyano[3-14C]Acrylate Nanoparticles in the Albino Rabbit. Int. J. Pharm. 1985, 23, 175–183. [Google Scholar] [CrossRef]
- Saraiva, S.M.; Castro-López, V.; Pañeda, C.; Alonso, M.J. Synthetic Nanocarriers for the Delivery of Polynucleotides to the Eye. Eur. J. Pharm. Sci. 2017, 103, 5–18. [Google Scholar] [CrossRef]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gote, V.; Ansong, M.; Pal, D. Prodrugs and Nanomicelles to Overcome Ocular Barriers for Drug Penetration. Expert Opin. Drug Metab. Toxicol. 2020, 16, 885–906. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, L.; Espina, M.; Severino, P.; Cano, A.; Ettcheto, M.; Camins, A.; García, M.L.; Souto, E.B.; Sánchez-López, E. Lipid Nanoparticles for the Posterior Eye Segment. Pharmaceutics 2022, 14, 90. [Google Scholar] [CrossRef] [PubMed]
- Durán-Lobato, M.; López-Estévez, A.M.; Cordeiro, A.S.; Dacoba, T.G.; Crecente-Campo, J.; Torres, D.; Alonso, M.J. Nanotechnologies for the Delivery of Biologicals: Historical Perspective and Current Landscape. Adv. Drug Deliv. Rev. 2021, 176, 113899. [Google Scholar] [CrossRef]
- Souto, E.B.; Dias-Ferreira, J.; López-Machado, A.; Ettcheto, M.; Cano, A.; Espuny, A.C.; Espina, M.; Garcia, M.L.; Sánchez-López, E. Advanced Formulation Approaches for Ocular Drug Delivery: State-of-the-Art and Recent Patents. Pharmaceutics 2019, 11, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandal, A.; Bisht, R.; Rupenthal, I.D.; Mitra, A.K. Polymeric Micelles for Ocular Drug Delivery: From Structural Frameworks to Recent Preclinical Studies. J. Control. Release 2017, 248, 96–116. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-López, E.; Espina, M.; Doktorovova, S.; Souto, E.B.; García, M.L. Lipid Nanoparticles (SLN, NLC): Overcoming the Anatomical and Physiological Barriers of the Eye—Part I—Barriers and Determining Factors in Ocular Delivery. Eur. J. Pharm. Biopharm. 2017, 110, 70–75. [Google Scholar] [CrossRef]
- Diebold, Y.; Calonge, M. Applications of Nanoparticles in Ophthalmology. Prog. Retin. Eye Res. 2010, 29, 596–609. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.; Spallarossa, A.; Tasso, B.; Villa, C.; Brullo, C. Nanotechnology for Pediatric Retinoblastoma Therapy. Pharmaceuticals 2022, 15, 1087. [Google Scholar] [CrossRef] [PubMed]
- Jumelle, C.; Gholizadeh, S.; Annabi, N.; Dana, R. Advances and Limitations of Drug Delivery Systems Formulated as Eye Drops. J. Control. Release 2020, 321, 1–22. [Google Scholar] [CrossRef]
- Allyn, M.M.; Luo, R.H.; Hellwarth, E.B.; Swindle-Reilly, K.E. Considerations for Polymers Used in Ocular Drug Delivery. Front. Med. 2022, 8, 2963. [Google Scholar] [CrossRef]
- Singh, M.; Bharadwaj, S.; Lee, K.E.; Kang, S.G. Therapeutic Nanoemulsions in Ophthalmic Drug Administration: Concept in Formulations and Characterization Techniques for Ocular Drug Delivery. J. Control. Release 2020, 328, 895–916. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y.; Meher, J.G.; Raval, K.; Khan, F.A.; Chaurasia, M.; Jain, N.K.; Chourasia, M.K. Nanoemulsion: Concepts, Development and Applications in Drug Delivery. J. Control. Release 2017, 252, 28–49. [Google Scholar] [CrossRef] [PubMed]
- Senapati, S.; Youssef, A.A.A.; Sweeney, C.; Cai, C.; Dudhipala, N.; Majumdar, S. Cannabidiol Loaded Topical Ophthalmic Nanoemulsion Lowers Intraocular Pressure in Normotensive Dutch-Belted Rabbits. Pharmaceutics 2022, 14, 2585. [Google Scholar] [CrossRef]
- Sweeney, C.; Dudhipala, N.; Thakkar, R.; Mehraj, T.; Marathe, S.; Gul, W.; El Sohly, M.A.; Murphy, B.; Majumdar, S. Effect of Surfactant Concentration and Sterilization Process on Intraocular Pressure–Lowering Activity of Δ9-Tetrahydrocannabinol-Valine-Hemisuccinate (NB1111) Nanoemulsions. Drug Deliv. Transl. Res. 2021, 11, 2096–2107. [Google Scholar] [CrossRef] [PubMed]
- Taskar, P.S.; Patil, A.; Lakhani, P.; Ashour, E.; Gul, W.; Elsohly, M.A.; Murphy, B.; Majumdar, S. Δ9-Tetrahydrocannabinol Derivative-Loaded Nanoformulation Lowers Intraocular Pressure in Normotensive Rabbits. Transl. Vis. Sci. Technol. 2019, 8, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, S.; Nair, A.B.; Shah, J.; Gupta, S.; Boddu, S.H.S.; Sreeharsha, N.; Joseph, A.; Shinu, P.; Morsy, M.A. Lipid Nanoparticles as a Promising Drug Delivery Carrier for Topical Ocular Therapy; An Overview on Recent Advances. Pharmaceutics 2022, 14, 533. [Google Scholar] [CrossRef]
- Mishra, V.; Bansal, K.K.; Verma, A.; Yadav, N.; Thakur, S.; Sudhakar, K.; Rosenholm, J.M. Solid Lipid Nanoparticles: Emerging Colloidal Nano Drug Delivery Systems. Pharmaceutics 2018, 10, 191. [Google Scholar] [CrossRef] [Green Version]
- Szczesniak, A.M.; Kelly, M.E.M.; Whynot, S.; Shek, P.N.; Hung, O. Ocular Hypotensive Effects of an Intratracheally Delivered Liposomal Δ9-Tetrahydrocannabinol Preparation in Rats. J. Ocul. Pharmacol. Ther. 2006, 22, 160–167. [Google Scholar] [CrossRef]
- Kabiri, M.; Kamal, S.H.; Pawar, S.V.; Roy, P.R.; Derakhshandeh, M.; Kumar, U.; Hatzikiriakos, S.G.; Hossain, S.; Yadav, V.G. A Stimulus-Responsive, in Situ-Forming, Nanoparticle-Laden Hydrogel for Ocular Drug Delivery. Drug Deliv. Transl. Res. 2018, 8, 484–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sosnik, A.; Shabo, R.B.; Halamish, H.M. Cannabidiol-Loaded Mixed Polymeric Micelles of Chitosan/Poly(Vinyl Alcohol) and Poly(Methyl Methacrylate) for Trans-Corneal Delivery. Pharmaceutics 2021, 13, 2142. [Google Scholar] [CrossRef] [PubMed]
- Kingman, S. Glaucoma Is Second Leading Cause of Blindness Globally. Bull. World Health Organ. 2004, 82, 887–888. [Google Scholar] [PubMed]
- Schmidl, D.; Schmetterer, L.; Garhöfer, G.; Popa-Cherecheanu, A. Pharmacotherapy of Glaucoma. J. Ocul. Pharmacol. Ther. 2015, 31, 63–77. [Google Scholar] [CrossRef] [Green Version]
- Foster, P.J.; Buhrmann, R.; Quigley, H.A.; Johnson, G.J. The Definition and Classification of Glaucoma in Prevalence Surveys. Br. J. Ophthalmol. 2002, 86, 238–242. [Google Scholar] [CrossRef] [Green Version]
- Luntz, M.H. Congenital, Infantile, and Juvenile Glaucoma. Ophthalmology 1979, 86, 793–802. [Google Scholar] [CrossRef]
- Badawi, A.H.; Al-Muhaylib, A.A.; Al Owaifeer, A.M.; Al-Essa, R.S.; Al-Shahwan, S.A. Primary Congenital Glaucoma: An Updated Review. Saudi J. Ophthalmol. 2019, 33, 382–388. [Google Scholar] [CrossRef]
- Coan, L.J.; Williams, B.M.; Krishna Adithya, V.; Upadhyaya, S.; Alkafri, A.; Czanner, S.; Venkatesh, R.; Willoughby, C.E.; Kavitha, S.; Czanner, G. Automatic Detection of Glaucoma via Fundus Imaging and Artificial Intelligence: A Review. Surv. Ophthalmol. 2022, 68, 17–41. [Google Scholar] [CrossRef]
- Mietzner, R.; Breunig, M. Causative Glaucoma Treatment: Promising Targets and Delivery Systems. Drug Discov. Today 2019, 24, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Bertaud, S.; Aragno, V.; Baudouin, C.; Labbé, A. Primary Open-Angle Glaucoma Young. Rev. Med. Interne 2019, 360, 445–452. [Google Scholar] [CrossRef]
- Storgaard, L.; Tran, T.L.; Freiberg, J.C.; Hauser, A.S.; Kolko, M. Glaucoma Clinical Research: Trends in Treatment Strategies and Drug Development. Front. Med. 2021, 8, 733080. [Google Scholar] [CrossRef]
- Quigley, H.A. Glaucoma. Lancet 2011, 377, 1367–1377. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Normal-Tension Glaucoma Study Group The Effectiveness of Intraocular Pressure Reduction in the Treatment of Normal-Tension Glaucoma. Am. J. Ophthalmol. 1998, 126, 498–505. [CrossRef] [PubMed]
- Hepler, R.S.; Frank, I.R. Marihuana Smoking and Intraocular Pressure. JAMA J. Am. Med. Assoc. 1971, 217, 1392. [Google Scholar] [CrossRef]
- Cohen, S. The 94-day Cannabis Study. Ann. N. Y. Acad. Sci. 1976, 282, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Merritt, J.C.; Crawford, W.J.; Alexander, P.C.; Anduze, A.L.; Gelbart, S.S. Effect of Marihuana on Intraocular and Blood Pressure in Glaucoma. Ophthalmology 1980, 87, 222–228. [Google Scholar] [CrossRef]
- Pagotto, U.; Marsicano, G.; Cota, D.; Lutz, B.; Pasquali, R. The Emerging Role of the Endocannabinoid System in Endocrine Regulation and Energy Balance. Endocr. Rev. 2006, 27, 73–100. [Google Scholar] [CrossRef]
- van der Horst, J.; Greenwood, I.A.; Jepps, T.A. Cyclic AMP-Dependent Regulation of Kv7 Voltage-Gated Potassium Channels. Front. Physiol. 2020, 11, 727. [Google Scholar] [CrossRef]
- Panchal, S.S.; Mehta, A.A.; Santani, D.D. Effect of Potassium Channel Openers in Acute and Chronic Models of Glaucoma. Taiwan J. Ophthalmol. 2016, 6, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Crandall, J.; Matragoon, S.; Khalifa, Y.M.; Borlongan, C.; Tsai, N.T.; Caldwell, R.B.; Liou, G.I. Neuroprotective and Intraocular Pressure-Lowering Effects of (-)Δ9-Tetrahydrocannabinol in a Rat Model of Glaucoma. Ophthalmic Res. 2007, 39, 69–75. [Google Scholar] [CrossRef]
- Liu, H.-F.; He, Y.; Jia, J.; Ji, M.-L.; Xi, J.-W. Clinical Study on Intravitreal Injection of Cannabinoid HU-211 for Optic Nerve Damage in Glaucoma Rats. Int. Eye Sci. 2014, 12, 1584–1586. [Google Scholar] [CrossRef]
- Pinar-Sueiro, S.; Zorrilla Hurtado, J.Á.; Veiga-Crespo, P.; Sharma, S.C.; Vecino, E. Neuroprotective Effects of Topical CB1 Agonist WIN 55212-2 on Retinal Ganglion Cells after Acute Rise in Intraocular Pressure Induced Ischemia in Rat. Exp. Eye Res. 2013, 110, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Porcella, A.; Maxia, C.; Gessa, G.L.; Pani, L. The Synthetic Cannabinoid WIN55212-2 Decreases the Intraocular Pressure in Human Glaucoma Resistant to Conventional Therapies. Eur. J. Neurosci. 2001, 13, 409–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, L.; Luong, V.; Gregson, A.; Baker, D.; Selwood, D.; Cordeiro, M.F. VSN16S, an Agonist of the Cannabinoid Receptor, Reduces IOP Profiles and Exhibits Neuroprotective Properties in a Rat Model of Glaucoma. Acta Ophthalmol. 2022, 100. [Google Scholar] [CrossRef]
- Tiedeman, J.S.; Shields, M.B.; Weber, P.A.; Crow, J.W.; Cocchetto, D.M.; Harris, W.A.; Howes, J.F. Effect of Synthetic Cannabinoids on Elevated Intraocular Pressure. Ophthalmology 1981, 88, 270–277. [Google Scholar] [CrossRef]
- Tomida, I.; Azuara-Blanco, A.; House, H.; Flint, M.; Pertwee, R.G.; Robson, P.J. Effect of Sublingual Application of Cannabinoids on Intraocular Pressure: A Pilot Study. J. Glaucoma 2006, 15, 349–353. [Google Scholar] [CrossRef]
- Thayer, A.; Murataeva, N.; Delcroix, V.; Wager-Miller, J.; Makarenkova, H.P.; Straiker, A. THC Regulates Tearing via Cannabinoid CB1 Receptors. Investig. Ophthalmol. Vis. Sci. 2020, 61, 48. [Google Scholar] [CrossRef]
- Miller, S.; Daily, L.; Leishman, E.; Bradshaw, H.; Straiker, A. ∆ 9 -Tetrahydrocannabinol and Cannabidiol Differentially Regulate Intraocular Pressure. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5904–5911. [Google Scholar] [CrossRef] [Green Version]
- Green, K.; Symonds, C.M.; Oliver, N.W.; Elijah, R.D. Intraocular Pressure Following Systemic Administration of Cannabinoids. Curr. Eye Res. 1982, 2, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Elsohly, M.A.; Harland, E.C.; Benigni, D.A.; Waller, C.W. Cannabinoids in Glaucoma II: The Effect of Different Cannabinoids on Intraocular Pressure of the Rabbit. Curr. Eye Res. 1984, 3, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.H.K.; Dacus, A.C. Central Nervous System and Peripheral Mechanisms in Ocular Hypotensive Effect of Cannabinoids. Arch. Ophthalmol. 1987, 105, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Green, K.; Wynn, H.; Bowman, K.A. A Comparison of Topical Cannabinoids on Intraocular Pressure. Exp. Eye Res. 1978, 27, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Rebibo, L.; Frušić-Zlotkin, M.; Ofri, R.; Nassar, T.; Benita, S. The Dose-Dependent Effect of a Stabilized Cannabidiol Nanoemulsion on Ocular Surface Inflammation and Intraocular Pressure. Int. J. Pharm. 2022, 617, 121627. [Google Scholar] [CrossRef] [PubMed]
- Latif, Z.; Garg, N. The Impact of Marijuana on the Cardiovascular System: A Review of the Most Common Cardiovascular Events Associated with Marijuana Use. J. Clin. Med. 2020, 9, 1925. [Google Scholar] [CrossRef]
- Pinar-Sueiro, S.; Rodríguez-Puertas, R.; Vecino, E. Cannabinoid Applications in Glaucoma. Arch. Soc. Esp. Oftalmol. 2011, 86, 16–23. [Google Scholar] [CrossRef]
- Cooler, P.; Gregg, J.M. Effect of Delta-9-Tetrahydrocannabinol on Intraocular Pressure in Humans. South. Med. J. 1976, 70, 77–87. [Google Scholar] [CrossRef]
- Jay, W.M.; Green, K. Multiple-Drop Study of Topically Applied 1% Δ9-Tetrahydrocannabinol in Human Eyes. Arch. Ophthalmol. 1983, 101, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Loftssona, T.; Järvinen, T. Cyclodextrins in Ophthalmic Drug Delivery. Adv. Drug Deliv. Rev. 1999, 36, 59–79. [Google Scholar] [CrossRef]
- Adelli, G.R.; Bhagav, P.; Taskar, P.; Hingorani, T.; Pettaway, S.; Gul, W.; ElSohly, M.A.; Repka, M.A.; Majumdar, S. Development of a ∆9-Tetrahydrocannabinol Amino Acid-Dicarboxylate Prodrug with Improved Ocular Bioavailability. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2167–2179. [Google Scholar] [CrossRef] [Green Version]
- Taskar, P.; Adelli, G.; Patil, A.; Lakhani, P.; Ashour, E.; Gul, W.; Elsohly, M.; Majumdar, S. Analog Derivatization of Cannabidiol for Improved Ocular Permeation. J. Ocul. Pharmacol. Ther. 2019, 35, 301–310. [Google Scholar] [CrossRef]
- Toguri, J.T.; Leishman, E.; Szczesniak, A.M.; Laprairie, R.B.; Oehler, O.; Straiker, A.J.; Kelly, M.E.M.; Bradshaw, H.B. Inflammation and CB 2 Signaling Drive Novel Changes in the Ocular Lipidome and Regulate Immune Cell Activity in the Eye. Prostaglandins Other Lipid Mediat. 2018, 139, 54–62. [Google Scholar] [CrossRef]
- Muchtar, S.; Almog, S.; Torracca, M.T.; Saettone, M.F.; Benita, S. A Submicron Emulsion as Ocular Vehicle for Delta-8-Tetrahydro-Cannabinol: Effect on Intraocular Pressure in Rabbits. Ophthalmic Res. 1992, 24, 142–149. [Google Scholar] [CrossRef]
- Thapa, D.; Cairns, E.A.; Szczesniak, A.M.; Toguri, J.T.; Caldwell, M.D.; Kelly, M.E.M. The Cannabinoids Δ8THC, CBD, and HU-308 Act via Distinct Receptors to Reduce Corneal Pain and Inflammation. Cannabis Cannabinoid Res. 2018, 3, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Thapa, D.; Cairns, E.A.; Szczesniak, A.M.; Kulkarni, P.M.; Straiker, A.J.; Thakur, G.A.; Kelly, M.E.M. Allosteric Cannabinoid Receptor 1 (CB1) Ligands Reduce Ocular Pain and Inflammation. Molecules 2020, 25, 417. [Google Scholar] [CrossRef] [Green Version]
- Toguri, J.T.; Lehmann, C.; Laprairie, R.B.; Szczesniak, A.M.; Zhou, J.; Denovan-Wright, E.M.; Kelly, M.E.M. Anti-Inflammatory Effects of Cannabinoid CB2 Receptor Activation in Endotoxin-Induced Uveitis. Br. J. Pharmacol. 2014, 171, 1448–1461. [Google Scholar] [CrossRef] [Green Version]
- Porter, R.F.; Szczesniak, A.-M.; Toguri, J.T.; Gebremeskel, S.; Johnston, B.; Lehmann, C.; Fingerle, J.; Rothenhäusler, B.; Perret, C.; Rogers-Evans, M.; et al. Selective Cannabinoid 2 Receptor Agonists as Potential Therapeutic Drugs for the Treatment of Endotoxin-Induced Uveitis. Molecules 2019, 24, 3338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, B.N.; Maass, M.; Musial, G.; Stern, M.E.; Gehlsen, U.; Steven, P. Topical Application of Cannabinoid-Ligands Ameliorates Experimental Dry-Eye Disease. Ocul. Surf. 2022, 23, 131–139. [Google Scholar] [CrossRef]
- Sweeney, C.; Dudhipala, N.; Thakkar, R.; Mehraj, T.; Marathe, S.; Gul, W.; ElSohly, M.A.; Murphy, B.; Majumdar, S. Impact of Mucoadhesive Agent Inclusion on the Intraocular Pressure Lowering Profile of Δ9-Tetrahydrocannabinol-Valine-Hemisuccinate Loaded Nanoemulsions in New Zealand White Rabbits. Int. J. Pharm. 2022, 616, 121564. [Google Scholar] [CrossRef] [PubMed]
- Balguri, S.P.; Adelli, G.R.; Majumdar, S. Topical Ophthalmic Lipid Nanoparticle Formulations (SLN, NLC) of Indomethacin for Delivery to the Posterior Segment Ocular Tissues. Eur. J. Pharm. Biopharm. 2016, 109, 224–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punyamurthula, N.S.; Adelli, G.R.; Gul, W.; Repka, M.A.; ElSohly, M.A.; Majumdar, S. Ocular Disposition of ∆8-Tetrahydrocannabinol from Various Topical Ophthalmic Formulations. AAPS PharmSciTech 2017, 18, 1936–1945. [Google Scholar] [CrossRef]
- Ting, D.S.J.; Ho, C.S.; Deshmukh, R.; Said, D.G.; Dua, H.S. Infectious Keratitis: An Update on Epidemiology, Causative Microorganisms, Risk Factors, and Antimicrobial Resistance. Eye 2021, 35, 1084–1101. [Google Scholar] [CrossRef]
- Wirta, D.; McLaurin, E.; Ousler, G.; Liu, J.; Kacmaz, R.O.; Grieco, J. Repository Corticotropin Injection (Acthar® Gel) for Refractory Severe Noninfectious Keratitis: Efficacy and Safety from a Phase 4, Multicenter, Open-Label Study. Ophthalmol. Ther. 2021, 10, 1077–1092. [Google Scholar] [CrossRef]
- Darlen Rodríguez Rivero, D.; Dra Silvia María López Hernández, I.; Yoanner Martín Perera, I.; Dra Eneida de la Caridad Pérez Candelaria, I.; Dra Karyna Castro Cárdenas, I.; Dra Lizet Sánchez Acosta, I.I.; Instituto Cubano de Oftalmología; Pando Ferrer, R.; Habana, L. Corneal Ulcers in Contact Lens Wearers. Rev. Cuba. Oftalmol. 2015, 28, 220–227. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, H.; Wang, Z.; Varadaraj, K.; Kumari, S.S.; Mergler, S.; Okada, Y.; Saika, S.; Kingsley, P.J.; Marnett, L.J.; et al. Cannabinoid Receptor 1 Suppresses Transient Receptor Potential Vanilloid 1-Induced Inflammatory Responses to Corneal Injury. Cell. Signal. 2013, 25, 501–511. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.; Daily, L.; Ploss, M.; Greig, I.; Ross, R.; Rayana, N.P.; Dai, J.; Sugali, C.K.; Mao, W.; Straiker, A. Evidence That Cannabinoid CB1 Receptors Regulate Intraocular Pressure via Two Opposing Mechanisms. Exp. Eye Res. 2020, 200, 108241. [Google Scholar] [CrossRef]
- McCannel, C.A.; Holland, G.N.; Helm, C.J.; Cornell, P.J.; Winston, J.V.; Rimmer, T.G.; Astorino, A.; Chang, A.M.; Cornell, P.J.; Davidorf, B.S.; et al. Causes of Uveitis in the General Practice of Ophthalmology. Am. J. Ophthalmol. 1996, 121, 35–46. [Google Scholar] [CrossRef]
- Calvo Hernández, L.M.; Bautista Salinas, R.M.; Cervera Segura, R.; Suárez Cabrera, M. Uveitis: A Challenge for Internist. An. Med. Interna 2008, 25, 141–148. [Google Scholar] [PubMed] [Green Version]
- González, M.M.; Solano, M.M.; Porco, T.C.; Oldenburg, C.E.; Acharya, N.R.; Lin, S.C.; Chan, M.F. Epidemiology of Uveitis in a US Population-Based Study. J. Ophthalmic Inflamm. Infect. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.R.; Jabs, D.A.; Briceland, D.J.; Holland, G.N. Education in the Ophthalmic Discipline of Uveitis. Am. J. Ophthalmol. 2008, 146, 799–801. [Google Scholar] [CrossRef]
- Lehoang, P. The Gold Standard of Noninfectious Uveitis: Corticosteroids. Dev. Ophthalmol. 2012, 51, 7–28. [Google Scholar] [CrossRef]
- Gómez-Gómez, A.; Loza, E.; Rosario, M.P.; Espinosa, G.; de Morales, J.M.G.R.; Herrera, J.M.; Muñoz-Fernández, S.; Rodríguez-Rodríguez, L.; Cordero-Coma, M. Efficacy and Safety of Immunomodulatory Drugs in Patients with Non-Infectious Intermediate and Posterior Uveitis, Panuveitis and Macular Edema: A Systematic Literature Review. Semin. Arthritis Rheum. 2020, 50, 1299–1306. [Google Scholar] [CrossRef]
- Couret, C.; Servant, M.; Lebranchu, P.; Hamidou, M.; Weber, M. Efficacy and Safety of Interferon Alpha 2A and Pegylated Interferon Alpha 2A in Inflammatory Macular Edema. Ocul. Immunol. Inflamm. 2020, 28, 329–336. [Google Scholar] [CrossRef]
- Biester, S.; Deuter, C.; Michels, H.; Haefner, R.; Kuemmerle-Deschner, J.; Doycheva, D.; Zierhut, M. Adalimumab in the Therapy of Uveitis in Childhood. Br. J. Ophthalmol. 2007, 91, 319–324. [Google Scholar] [CrossRef] [PubMed]
- HUMIRA: Non-Infectious Uveitis Treatment. Available online: https://www.humira.com/uveitis/non-infectious-uv-treatment (accessed on 15 January 2023).
- Toguri, J.T.; Caldwell, M.; Kelly, M.E.M. Turning down the Thermostat: Modulating the Endocannabinoid System in Ocular Inflammation and Pain. Front. Pharmacol. 2016, 7, 304. [Google Scholar] [CrossRef] [Green Version]
- Ben-David, G.; Nisgav, Y.; Weinberger, Y.; Kramer, M. Cannabinoid 2 (CB2) Receptor Upregulation in Experimental Autoimmune Uveitis (EAU). Investig. Ophthalmol. Vis. Sci. 2022, 63, 2227-A0523. [Google Scholar]
- Xu, H.; Cheng, C.L.; Chen, M.; Manivannan, A.; Cabay, L.; Pertwee, R.G.; Coutts, A.; Forrester, J.V. Anti-Inflammatory Property of the Cannabinoid Receptor-2-Selective Agonist JWH-133 in a Rodent Model of Autoimmune Uveoretinitis. J. Leukoc. Biol. 2007, 82, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Szczesniak, A.M.; Porter, R.F.; Toguri, J.T.; Borowska-Fielding, J.; Gebremeskel, S.; Siwakoti, A.; Johnston, B.; Lehmann, C.; Kelly, M.E.M. Cannabinoid 2 Receptor Is a Novel Anti-Inflammatory Target in Experimental Proliferative Vitreoretinopathy. Neuropharmacology 2017, 113, 627–638. [Google Scholar] [CrossRef]
- Messmer, E.M. Pathophysiology of Dry Eye Disease and Novel Therapeutic Targets. Exp. Eye Res. 2022, 217, 108944. [Google Scholar] [CrossRef] [PubMed]
- Benitez-Del-Castillo, J.M.; Moreno-Montañés, J.; Jiménez-Alfaro, I.; Muñoz-Negrete, F.J.; Turman, K.; Palumaa, K.; Sádaba, B.; González, M.V.; Ruz, V.; Vargas, B.; et al. Safety and Efficacy Clinical Trials for SYL1001, a Novel Short Interfering RNA for the Treatment of Dry Eye Disease. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6447–6454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsubota, K.; Pflugfelder, S.C.; Liu, Z.; Baudouin, C.; Kim, H.M.; Messmer, E.M.; Kruse, F.; Liang, L.; Carreno-Galeano, J.T.; Rolando, M.; et al. Defining Dry Eye from a Clinical Perspective. Int. J. Mol. Sci. 2020, 21, 9271. [Google Scholar] [CrossRef] [PubMed]
- McDowell, T.S.; Wang, Z.Y.; Singh, R.; Bjorling, D. CB1 Cannabinoid Receptor Agonist Prevents NGF-Induced Sensitization of TRPV1 in Sensory Neurons. Neurosci. Lett. 2013, 551, 34–38. [Google Scholar] [CrossRef] [Green Version]
- El-Remessy, A.B.; Al-Shabrawey, M.; Khalifa, Y.; Tsai, N.T.; Caldwell, R.B.; Liou, G.I. Neuroprotective and Blood-Retinal Barrier-Preserving Effects of Cannabidiol in Experimental Diabetes. Am. J. Pathol. 2006, 168, 235–244. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, S.H.; Schwartz, S.S. Diabetic Retinopathy–An Underdiagnosed and Undertreated Inflammatory, Neuro-Vascular Complication of Diabetes. Front. Endocrinol. 2019, 10, 843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teo, Z.L.; Tham, Y.-C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-Analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef]
- Yau, J.W.Y.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Global Prevalence and Major Risk Factors of Diabetic Retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, M.P.; Lent-Schochet, D.; Lo, T.; Yiu, G. Emerging Concepts in the Treatment of Diabetic Retinopathy. Curr. Diab. Rep. 2019, 19, 137. [Google Scholar] [CrossRef] [PubMed]
- El-Remessy, A.B.; Khalil, I.E.; Matragoon, S.; Abou-Mohamed, G.; Tsai, N.J.; Roon, P.; Caldwell, R.B.; Caldwell, R.W.; Green, K.; Liou, G.I. Neuroprotective Effect of(-)Δ9-Tetrahydrocannabinol and Cannabidiol in N-Methyl-D-Aspartate-Induced Retinal Neurotoxicity: Involvement of Peroxynitrite. Am. J. Pathol. 2003, 163, 1997–2008. [Google Scholar] [CrossRef] [PubMed]
- Jamal, M.; Ahmad, W.; Andleeb, S.; Jalil, F.; Imran, M.; Nawaz, M.A.; Hussain, T.; Ali, M.; Rafiq, M.; Kamil, M.A. Bacterial Biofilm and Associated Infections. J. Chinese Med. Assoc. 2018, 81, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Urwin, L.; Okurowska, K.; Crowther, G.; Roy, S.; Garg, P.; Karunakaran, E.; MacNeil, S.; Partridge, L.J.; Green, L.R.; Monk, P.N. Corneal Infection Models: Tools to Investigate the Role of Biofilms in Bacterial Keratitis. Cells 2020, 9, 2450. [Google Scholar] [CrossRef]
- Saraswathi, P.; Beuerman, R.W. Corneal Biofilms: From Planktonic to Microcolony Formation in an Experimental Keratitis Infection with Pseudomonas aeruginosa. Ocul. Surf. 2015, 13, 331–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rybtke, M.; Hultqvist, L.D.; Givskov, M.; Tolker-Nielsen, T. Pseudomonas aeruginosa Biofilm Infections: Community Structure, Antimicrobial Tolerance and Immune Response. J. Mol. Biol. 2015, 427, 3628–3645. [Google Scholar] [CrossRef] [PubMed]
- El-Ganiny, A.M.; Shaker, G.H.; Aboelazm, A.A.; El-Dash, H.A. Prevention of Bacterial Biofilm Formation on Soft Contact Lenses Using Natural Compounds. J. Ophthalmic Inflamm. Infect. 2017, 7, 1–7. [Google Scholar] [CrossRef]
- Bispo, P.J.M.; Haas, W.; Gilmore, M.S. Biofilms in Infections of the Eye. Pathogens 2015, 4, 111–136. [Google Scholar] [CrossRef] [PubMed]
- Schofs, L.; Sparo, M.D.; Sánchez Bruni, S.F. The Antimicrobial Effect behind Cannabis Sativa. Pharmacol. Res. Perspect. 2021, 9, e00761. [Google Scholar] [CrossRef]
- Di Onofrio, V.; Gesuele, R.; Maione, A.; Liguori, G.; Liguori, R.; Guida, M.; Nigro, R.; Galdiero, E. Prevention of Pseudomonas aeruginosa Biofilm Formation on Soft Contact Lenses by Allium Sativum Fermented Extract (BGE) and Cannabinol Oil Extract (CBD). Antibiotics 2019, 8, 258. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Fuentes, J.; Martín-Banderas, L.; Muñoz-Rubio, I.; Holgado, M.A.; Fernández-Arévalo, M. Development and Validation of an RP-HPLC Method for CB13 Evaluation in Several PLGA Nanoparticle Systems. Sci. World J. 2012, 2012, 737526. [Google Scholar] [CrossRef] [Green Version]
- Berrocoso, E.; Rey-Brea, R.; Fernández-Arévalo, M.; Micó, J.A.; Martín-Banderas, L. Single Oral Dose of Cannabinoid Derivate Loaded PLGA Nanocarriers Relieves Neuropathic Pain for Eleven Days. Nanomed. Nanotechnol. Biol. Med. 2017, 13, 2623–2632. [Google Scholar] [CrossRef] [PubMed]
- El-Hammadi, M.M.; Small-Howard, A.L.; Jansen, C.; Fernández-Arévalo, M.; Turner, H.; Martín-Banderas, L. Potential Use for Chronic Pain: Poly(Ethylene Glycol)-Poly(Lactic-Co-Glycolic Acid) Nanoparticles Enhance the Effects of Cannabis-Based Terpenes on Calcium Influx in TRPV1-Expressing Cells. Int. J. Pharm. 2022, 616, 121524. [Google Scholar] [CrossRef] [PubMed]
- Durán-Lobato, M.; Martín-Banderas, L.; Gonçalves, L.M.D.; Fernández-Arévalo, M.; Almeida, A.J. Comparative Study of Chitosan- and PEG-Coated Lipid and PLGA Nanoparticles as Oral Delivery Systems for Cannabinoids. J. Nanopart. Res. 2015, 17, 1–17. [Google Scholar] [CrossRef]
- He, X.; Zhu, Y.; Wang, M.; Jing, G.; Zhu, R.; Wang, S. Antidepressant Effects of Curcumin and HU-211 Coencapsulated Solid Lipid Nanoparticles against Corticosterone-Induced Cellular and Animal Models of Major Depression. Int. J. Nanomed. 2016, 17, 4975–4990. [Google Scholar] [CrossRef] [Green Version]
- He, X.L.; Yang, L.; Wang, Z.J.; Huang, R.Q.; Zhu, R.R.; Cheng, L.M. Solid Lipid Nanoparticles Loading with Curcumin and Dexanabinol to Treat Major Depressive Disorder. Neural Regen. Res. 2021, 16, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Matarazzo, A.P.; Elisei, L.M.S.; Carvalho, F.C.; Bonfílio, R.; Ruela, A.L.M.; Galdino, G.; Pereira, G.R. Mucoadhesive Nanostructured Lipid Carriers as a Cannabidiol Nasal Delivery System for the Treatment of Neuropathic Pain. Eur. J. Pharm. Sci. 2021, 159, 105698. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Rizwanullah, M.; Mir, S.R.; Akhtar, M.S.; Amin, S. Development of Cannabidiol Nanoemulsion for Direct Nose to Brain Delivery: Statistical Optimization, in Vitro and in Vivo Evaluation. Biomed. Mater. 2022, 17, 065009. [Google Scholar] [CrossRef]
- Linsell, O.; Brownjohn, P.W.; Nehoff, H.; Greish, K.; Ashton, J.C. Effect of Styrene Maleic Acid WIN55,212-2 Micelles on Neuropathic Pain in a Rat Model. J. Drug Target. 2015, 23, 353–359. [Google Scholar] [CrossRef]
- Greish, K.; Mathur, A.; Al Zahrani, R.; Elkaissi, S.; Al Jishi, M.; Nazzal, O.; Taha, S.; Pittalà, V.; Taurin, S. Synthetic Cannabinoids Nano-Micelles for the Management of Triple Negative Breast Cancer. J. Control. Release 2018, 291, 184–195. [Google Scholar] [CrossRef]
- Rao, Y.; Li, R.; Liu, S.; Meng, L.; Wu, Q.; Yuan, Q.; Liang, H.; Qin, M. Enhanced Bioavailability and Biosafety of Cannabidiol Nanomicelles for Effective Anti-Inflammatory Therapy. Particuology 2022, 69, 1–9. [Google Scholar] [CrossRef]
- Park, C.; Zuo, J.; Somayaji, V.; Lee, B.J.; Löbenberg, R. Development of a Novel Cannabinoid-Loaded Microemulsion towards an Improved Stability and Transdermal Delivery. Int. J. Pharm. 2021, 604, 120766. [Google Scholar] [CrossRef]
- Lodzki, M.; Godin, B.; Rakou, L.; Mechoulam, R.; Gallily, R.; Touitou, E. Cannabidiol—Transdermal Delivery and Anti-Inflammatory Effect in a Murine Model. J. Control. Release 2003, 93, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Sharkawy, A.; Silva, A.M.; Rodrigues, F.; Barreiro, F.; Rodrigues, A. Pickering Emulsions Stabilized with Chitosan/Collagen Peptides Nanoparticles as Green Topical Delivery Vehicles for Cannabidiol (CBD). Colloids Surf. A Physicochem. Eng. Asp. 2021, 631, 127677. [Google Scholar] [CrossRef]
- Xie, J.; Xiao, D.; Zhao, J.; Hu, N.; Bao, Q.; Jiang, L.; Yu, L. Mesoporous Silica Particles as a Multifunctional Delivery System for Pain Relief in Experimental Neuropathy. Adv. Healthc. Mater. 2016, 5, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Hassanzadeh, P.; Arbabi, E.; Atyabi, F.; Dinarvand, R. Application of Carbon Nanotubes as the Carriers of the Cannabinoid, 2-Arachidonoylglycerol: Towards a Novel Treatment Strategy in Colitis. Life Sci. 2017, 179, 66–72. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saraiva, S.M.; Martín-Banderas, L.; Durán-Lobato, M. Cannabinoid-Based Ocular Therapies and Formulations. Pharmaceutics 2023, 15, 1077. https://doi.org/10.3390/pharmaceutics15041077
Saraiva SM, Martín-Banderas L, Durán-Lobato M. Cannabinoid-Based Ocular Therapies and Formulations. Pharmaceutics. 2023; 15(4):1077. https://doi.org/10.3390/pharmaceutics15041077
Chicago/Turabian StyleSaraiva, Sofia M., Lucía Martín-Banderas, and Matilde Durán-Lobato. 2023. "Cannabinoid-Based Ocular Therapies and Formulations" Pharmaceutics 15, no. 4: 1077. https://doi.org/10.3390/pharmaceutics15041077
APA StyleSaraiva, S. M., Martín-Banderas, L., & Durán-Lobato, M. (2023). Cannabinoid-Based Ocular Therapies and Formulations. Pharmaceutics, 15(4), 1077. https://doi.org/10.3390/pharmaceutics15041077