
Effect of Food on the Pediatric Dispersible Tablet Formulations of TRIUMEQ and DOVATO in Healthy Adult Participants

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Good Clinical Practice
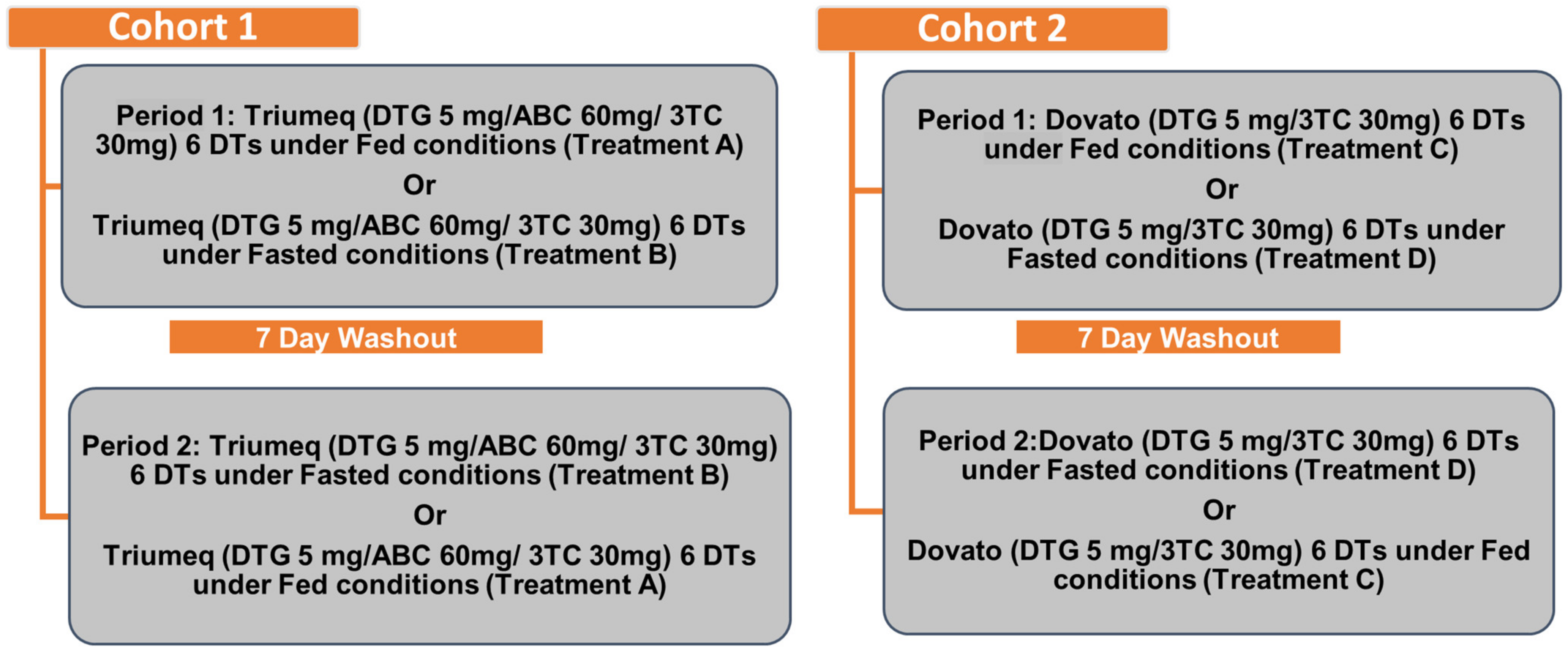
2.2. Study Design
2.3. PK Assessments
2.4. Safety Assessments
2.5. Palatability Assessments
3. Results
3.1. Participant Disposition and Demographics
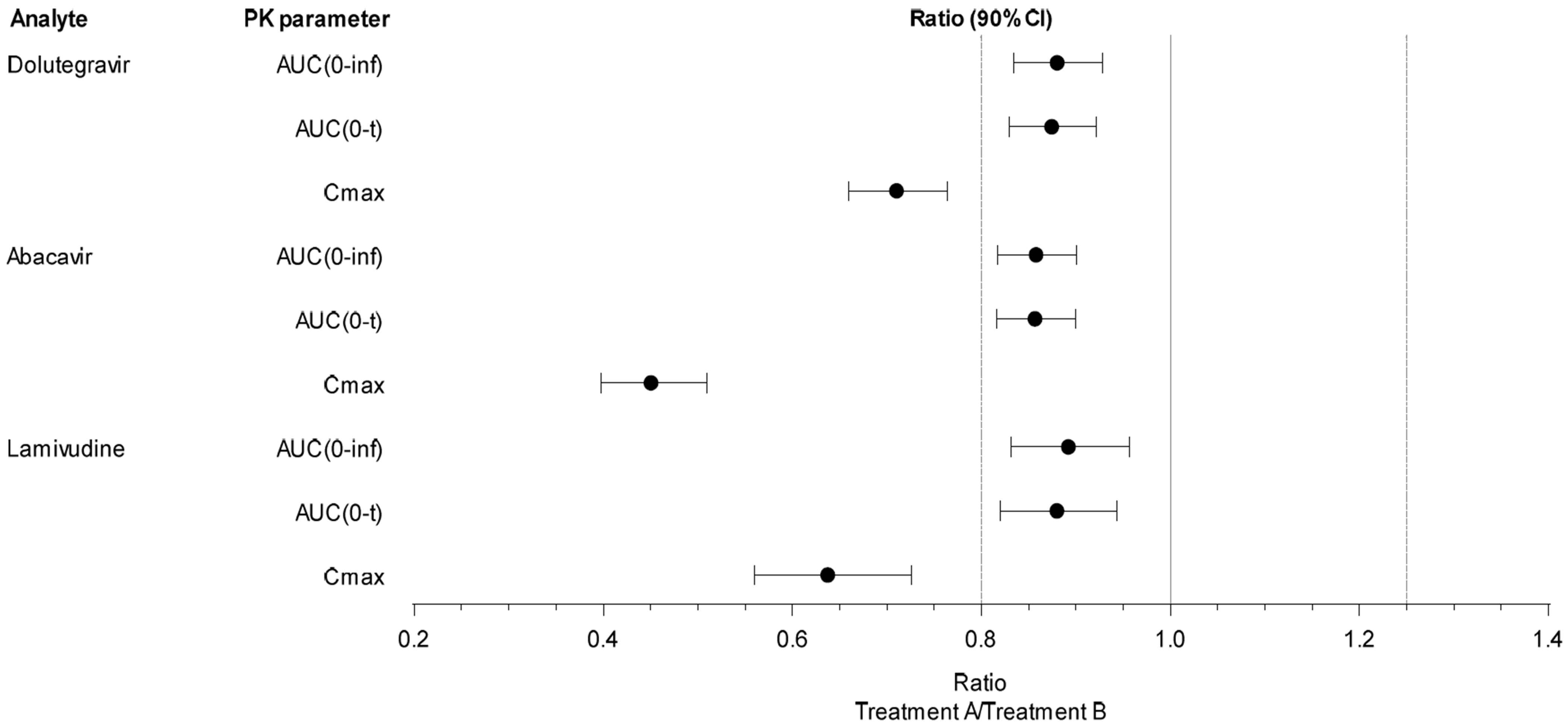
3.2. Cohort 1 Plasma PK Parameters of Dolutegravir, Abacavir, and Lamivudine
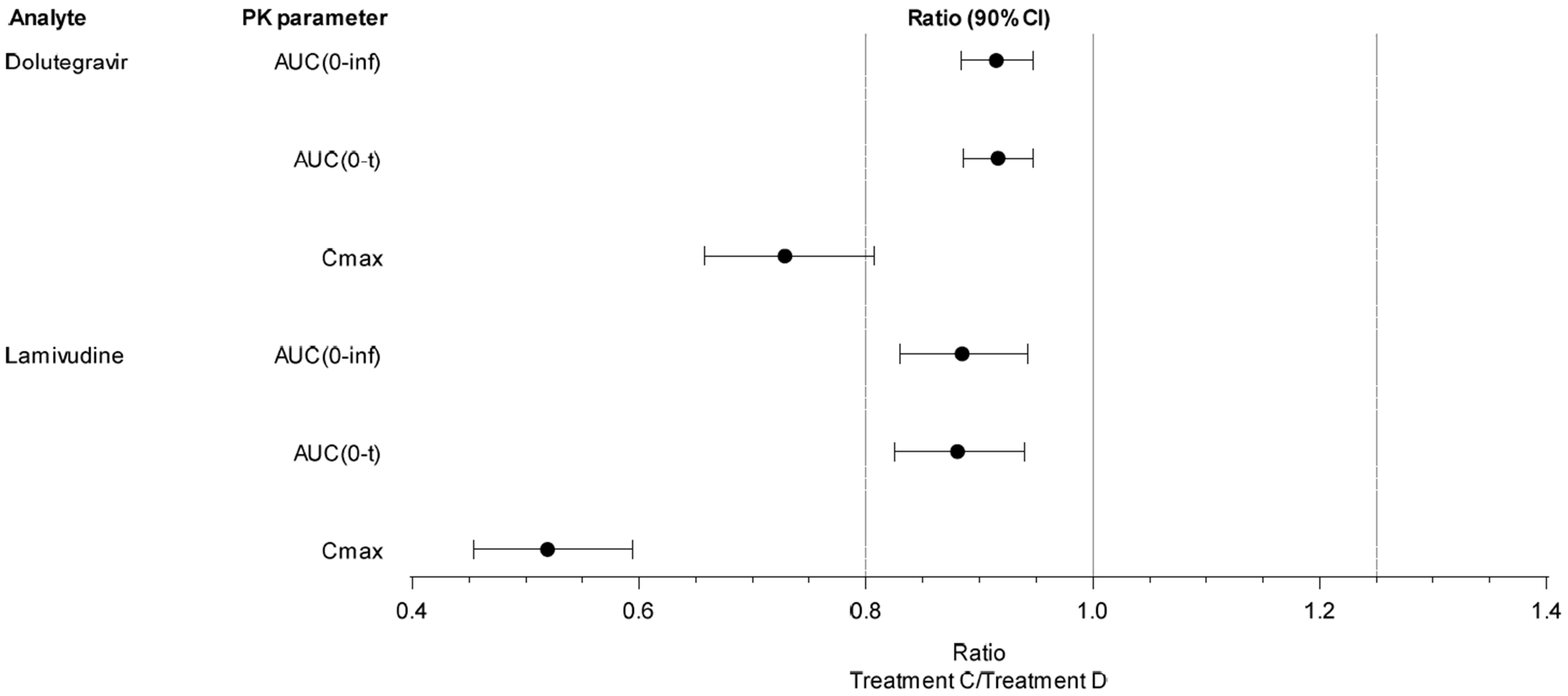
3.3. Cohort 2 Plasma PK Parameters of Dolutegravir and Lamivudine
3.4. Safety Results
3.5. Cohort 1
3.6. Cohort 2
3.7. Palatability Results
4. Discussion
4.1. Pharmacokinetics
4.1.1. Dolutegravir
4.1.2. Abacavir
4.1.3. Lamivudine
4.2. Safety and Tolerability
4.3. Palatability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV & AIDS Statistics—Fact Sheet; UNAIDS: Geneva, Switzerland, 2021. [Google Scholar]
- ViiV Healthcare. TRIUMEQ Tablets [Package Insert]; Food and Drug Adminstration: Silver Spring, MD, USA, 2014.
- ViiV Healthcare. DOVATO Tablets [Package Insert]; Food and Drug Adminstration: Silver Spring, MD, USA, 2019.
- US FDA. Guidance for Industry: Food-Effect Bioavailability and Fed Bioequivalence Studies. 2002. Available online: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidance/ucm070241.pdf (accessed on 3 February 2021).
- Weller, S.; Chen, S.; Borland, J.; Savina, P.; Wynne, B.; Piscitelli, S.C. Bioequivalence of a dolutegravir, abacavir, and lamivudine fixed-dose combination tablet and the effect of food. J. Acquir. Immune Defic. Syndr. 2014, 66, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, T.P.; Peddiraju, K.; Fu, C.; Bakshi, K.; Yu, S.; Zhang, Z.; Tenorio, A.R.; Spancake, C.; Joshi, S.; Wolstenholme, A.; et al. Bioequivalence and Food Effect Assessment of 2 Fixed-Dose Combination Formulations of Dolutegravir and Lamivudine. Clin. Pharmacol. Drug Dev. 2020, 9, 189–202. [Google Scholar] [CrossRef] [PubMed]
- Song, I.; Borland, J.; Chen, S.; Patel, P.; Wajima, T.; Peppercorn, A.; Piscitelli, S.C. Effect of food on the pharmacokinetics of the integrase inhibitor dolutegravir. Antimicrob. Agents Chemother. 2012, 56, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- ViiV Healthcare. TIVICAY Tablets [Package Insert]; Food and Drug Adminstration: Silver Spring, MD, USA, 2013.
- Singh, R.P.; Adkison, K.K.; Baker, M.; Parasrampuria, R.; Wolstenholme, A.; Davies, M.; Sewell, N.; Brothers, C.; Buchanan, A.M. Development of Dolutegravir Single-entity and Fixed-dose Combination Formulations for Children. Pediatr. Infect. Dis. J. 2022, 41, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Yuen, G.J.; Lou, Y.; Thompson, N.F.; Otto, V.R.; Allsup, T.L.; Mahony, W.B.; Hutman, H.W. Abacavir/lamivudine/zidovudine as a combined formulation tablet: Bioequivalence compared with each component administered concurrently and the effect of food on absorption. J. Clin. Pharmacol. 2001, 41, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Chittick, G.E.; Gillotin, C.; McDowell, J.A.; Lou, Y.; Edwards, K.D.; Prince, W.T.; Stein, D.S. Abacavir: Absolute bioavailability, bioequivalence of three oral formulations, and effect of food. Pharmacotherapy 1999, 19, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.N.; Sweet, D.E.; McDowell, J.A.; Symonds, W.; Lou, Y.; Hetherington, S.; LaFon, S. Safety and pharmacokinetics of abacavir (1592U89) following oral administration of escalating single doses in human immunodeficiency virus type 1-infected adults. Antimicrob. Agents Chemother. 1999, 43, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.H.; Shaw, S.; Laurent, A.L.; Lloyd, P.; Duncan, B.; Morris, D.M.; O’Mara, M.J.; Pakes, G.E. Lamivudine/zidovudine as a combined formulation tablet: Bioequivalence compared with lamivudine and zidovudine administered concurrently and the effect of food on absorption. J. Clin. Pharmacol. 1999, 39, 593–605. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Product Name | Drugs and Doses |
|---|---|
| TRIUMEQ FDC | 50 mg Dolutegravir/600 mg Abacavir/300 mg Lamivudine |
| TRIUMEQ DT FDC | 5 mg Dolutegravir/60 mg Abacavir/30 mg Lamivudine |
| DOVATO FDC | 50 mg Dolutegravir/300 mg Lamivudine |
| DOVATO DT FDC | 5 mg Dolutegravir/30 mg Lamivudine |
| Demographics | TRIUMEQ DT (Cohort 1) (N = 16) | DOVATO DT (Cohort 2) (N = 17) |
|---|---|---|
| Age in Years [Mean (SD)] | 34.9 (8.10) | 36.0 (8.07) |
| Sex [n (%)] | ||
| Female, potentially able to bear children | 6 (38) | 4 (24) |
| Male | 10 (63) | 13 (76) |
| BMI (kg/m2) [Mean (SD)] | 27.68 (1.909) | 26.78 (2.520) |
| Height (cm) [Mean (SD)] | 169.91 (12.780) | 172.57 (8.070) |
| Weight (kg) [Mean (SD)] | 80.21 (12.392) | 80.13 (11.760) |
| Ethnicity [n (%)] | ||
| Hispanic or Latino | 9 (56) | 7 (41) |
| Not Hispanic or Latino | 7 (44) | 10 (59) |
| Race [n (%)] | ||
| White—White/Caucasian/European Heritage | 9 (56) | 9 (53) |
| Black or African American | 5 (31) | 6 (35) |
| White—Arabic/North African Heritage | 1 (6) | 1 (6) |
| Multiple, Black or African American and White | 1 (6) | 0 |
| Asian—Central/South Asian Heritage | 0 | 1 (6) |
| Analyte: Dolutegravir | Analyte: Abacavir | Analyte: Lamivudine | ||||
|---|---|---|---|---|---|---|
| Parameter | Treatment A (N = 16) | Treatment B (N = 16) | Treatment A (N = 16) | Treatment B (N = 16) | Treatment A (N = 16) | Treatment B (N = 16) |
| Cmax (ng/mL) | ||||||
| Geometric Mean | 2359 | 3322 | 1837 | 4080 | 886.9 | 1392 |
| %CVb | 17.6 | 20.6 | 21.1 | 32.3 | 18.9 | 33.3 |
| AUC(0-inf) (h × ng/mL) a | ||||||
| Geometric Mean | 59,140 | 67,210 | 8565 | 9986 | 6508 | 7295 |
| %CVb | 25.7 | 24.0 | 24.9 | 28.8 | 19.9 | 23.4 |
| AUC(0-t) (h × ng/mL) | ||||||
| Geometric Mean | 55,770 | 63,790 | 8501 | 9923 | 6319 | 7182 |
| %CVb | 23.8 | 22.7 | 25.4 | 28.9 | 18.9 | 23.5 |
| AUC(0-24) (h × ng/mL) | ||||||
| Geometric Mean | 36,380 | 43870 | 8553 | 9980 | 5817 | 6707 |
| %CVb | 19.4 | 20.1 | 24.8 | 28.8 | 18.1 | 24.4 |
| Tmax (h) | ||||||
| Median | 5.000 | 1.250 | 2.750 | 0.500 | 3.500 | 1.508 |
| (Min, Max) | (3.00, 12.00) | (0.50, 4.00) | (0.50, 4.00) | (0.25, 1.50) | (2.00, 4.00) | (0.50, 3.50) |
| C24 (ng/mL) b | ||||||
| Geometric Mean | 958.6 | 996.3 | 4.833 | 3.814 | 23.40 | 21.74 |
| %CVb | 28.3 | 26.3 | 52.3 | 27.2 | 24.4 | 23.1 |
| Parameter | Treatment | N | n | Geometric LS Means | Ratio of Geometric LS Means (A/B) | 90% CI of the Ratio | Intra-Subject CV |
|---|---|---|---|---|---|---|---|
| Analyte: Dolutegravir | |||||||
| Cmax (ng/mL) | A | 16 | 16 | 2359 | 0.7102 | (0.6598, 0.7643) | 11.8 |
| B | 16 | 16 | 3322 | ||||
| AUC(0-inf) (h × ng/mL) | A | 16 | 16 | 59,140 | 0.8800 | (0.8344, 0.9282) | 8.6 |
| B | 16 | 16 | 67,210 | ||||
| AUC(0-t) (h × ng/mL) | A | 16 | 16 | 55,770 | 0.8744 | (0.8293, 0.9219) | 8.5 |
| B | 16 | 16 | 63,790 | ||||
| Analyte: Abacavir | |||||||
| Cmax (ng/mL) | A | 16 | 16 | 1837 | 0.4503 | (0.3976, 0.5100) | 20.2 |
| B | 16 | 16 | 4080 | ||||
| AUC(0-inf) (h × ng/mL) | A | 16 | 16 | 8565 | 0.8578 | (0.8168, 0.9007) | 7.9 |
| B | 16 | 16 | 9986 | ||||
| AUC(0-t) (h × ng/mL) | A | 16 | 16 | 8501 | 0.8567 | (0.8159, 0.8995) | 7.9 |
| B | 16 | 16 | 9923 | ||||
| Analyte: Lamivudine | |||||||
| Cmax (ng/mL) | A | 16 | 16 | 886.9 | 0.6373 | (0.5594, 0.7260) | 21.2 |
| B | 16 | 16 | 1392 | ||||
| AUC(0-inf) (h × ng/mL) | A | 16 | 15 | 6511 | 0.8919 | (0.8316, 0.9566) | 10.9 |
| B | 16 | 16 | 7300 | ||||
| AUC(0-t) (h × ng/mL) | A | 16 | 16 | 6319 | 0.8798 | (0.8202, 0.9438) | 11.3 |
| B | 16 | 16 | 7182 | ||||
| Analyte: Dolutegravir | Analyte: Lamivudine | |||
|---|---|---|---|---|
| Parameter | Treatment C (N = 17) | Treatment D (N = 16) | Treatment C (N = 17) | Treatment D (N = 16) |
| Cmax (ng/mL) | ||||
| Geometric Mean | 2331 | 3131 | 1084 | 2066 |
| %CVb | 15.4 | 19.8 | 18.6 | 28.6 |
| AUC(0-inf) (h × ng/mL) a | ||||
| Geometric Mean | 47,830 | 51,800 | 6975 | 7864 |
| %CVb | 24.2 | 24.3 | 10.1 | 13.9 |
| AUC(0-t) (h × ng/mL) | ||||
| Geometric Mean | 46,060 | 49,690 | 6799 | 7762 |
| %CVb | 22.2 | 22.0 | 10.5 | 14.0 |
| AUC(0-24) (h × ng/mL) | ||||
| Geometric Mean | 32,620 | 35,360 | 6339 | 7339 |
| %CVb | 19.2 | 15.6 | 10.7 | 14.9 |
| Tmax (h) | ||||
| Median | 4.000 | 0.875 | 3.000 | 0.750 |
| (Min, Max) | (3.50, 8.00) | (0.50, 3.50) | (0.75, 4.00) | (0.50, 1.00) |
| C24 (ng/mL) | ||||
| Geometric Mean | 764.7 | 715.4 | 22.56 | 20.38 |
| %CVb | 28.5 | 27.7 | 18.8 | 18.6 |
| Parameter | Treatment | N | n | Geometric LS Means | Ratio of Geometric LS Means (C/D) | 90% CI of the Ratio | Intra-Subject CV |
|---|---|---|---|---|---|---|---|
| Analyte: Dolutegravir | |||||||
| Cmax (ng/mL) | C | 17 | 17 | 2306 | 0.7284 | (0.6576, 0.8068) | 16.4 |
| D | 16 | 16 | 3166 | ||||
| AUC(0-inf) (h × ng/mL) | C | 17 | 16 | 47,610 | 0.9148 | (0.8834, 0.9472) | 5.6 |
| D | 16 | 16 | 52,040 | ||||
| AUC(0-t) (h × ng/mL) | C | 17 | 17 | 45,800 | 0.9163 | (0.8862, 0.9475) | 5.3 |
| D | 16 | 16 | 49,980 | ||||
| Analyte: Lamivudine | |||||||
| Cmax (ng/mL) | C | 17 | 17 | 1079 | 0.5191 | (0.4535, 0.5943) | 21.8 |
| D | 16 | 16 | 2078 | ||||
| AUC(0-inf) (h × ng/mL) | C | 17 | 16 | 6966 | 0.8847 | (0.8303, 0.9426) | 10.1 |
| D | 16 | 16 | 7874 | ||||
| AUC(0-t) (h × ng/mL) | C | 17 | 17 | 6816 | 0.8806 | (0.8251, 0.9398) | 10.4 |
| D | 16 | 16 | 7741 | ||||
| Treatment: TRIUMEQ DT | |||
|---|---|---|---|
| SOC Preferred Term, n (%) [Number of AEs Reported] | Treatment A (N = 16) | Treatment B (N = 16) | Total (N = 16) |
| Any AE | 1 (6) [1] | 3 (19) [4] | 4 (25) [5] |
| Gastrointestinal disorders, any AE | 1 (6) [1] | 2 (13) [2] | 3 (19) [3] |
| Abdominal discomfort | 1 (6) [1] | 0 | 1 (6) [1] |
| Angular cheilitis | 0 | 1 (6) [1] | 1 (6) [1] |
| Nausea | 0 | 1 (6) [1] | 1 (6) [1] |
| Nervous system disorders, any AE | 0 | 1 (6) [1] | 1 (6) [1] |
| Headache | 0 | 1 (6) [1] | 1 (6) [1] |
| Respiratory, thoracic, and mediastinal disorders, any AE | 0 | 1 (6) [1] | 1 (6) [1] |
| Oropharyngeal pain | 0 | 1 (6) [1] | 1 (6) [1] |
| Treatment: DOVATO DT | |||
| SOC Preferred Term, n (%) [number of AEs reported] | Treatment C (N = 17) | Treatment D (N = 16) | Total (N = 17) |
| Any AE | 1 (6) [1] | 1 (6) [1] | 1 * (6) [2] |
| Skin and subcutaneous tissue disorders, any AE | 1 (6) [1] | 1 (6) [1] | 1 (6) [2] |
| Dry skin | 0 | 1 (6) [1] | 1 (6) [1] |
| Skin irritation | 1 (6) [1] | 0 | 1 (6) [1] |
| TRIUMEQ DT (Cohort 1) | DOVATO DT (Cohort 2) | |||
|---|---|---|---|---|
| Palatability | Treatment A (N = 16) | Treatment B (N = 16) | Treatment C (N = 17) | Treatment D (N = 16) |
| 1-Very Poor | 3 (19%) | 4 (25%) | 0 | 0 |
| 2-Neutral/Acceptable | 13 (81%) | 10 (63%) | 8 (47%) | 6 (38%) |
| 3-Very Good | 0 | 2 (13%) | 9 (53%) | 10 (63%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandasana, H.; Marnoch, R.; McKenna, M.; Double, J.; Seal, C.; Bontempo, G.; Wolstenholme, A.; Buchanan, A. Effect of Food on the Pediatric Dispersible Tablet Formulations of TRIUMEQ and DOVATO in Healthy Adult Participants. Pharmaceutics 2023, 15, 1470. https://doi.org/10.3390/pharmaceutics15051470
Chandasana H, Marnoch R, McKenna M, Double J, Seal C, Bontempo G, Wolstenholme A, Buchanan A. Effect of Food on the Pediatric Dispersible Tablet Formulations of TRIUMEQ and DOVATO in Healthy Adult Participants. Pharmaceutics. 2023; 15(5):1470. https://doi.org/10.3390/pharmaceutics15051470
Chicago/Turabian StyleChandasana, Hardik, Ryan Marnoch, Michael McKenna, Julia Double, Ciara Seal, Gilda Bontempo, Allen Wolstenholme, and Ann Buchanan. 2023. "Effect of Food on the Pediatric Dispersible Tablet Formulations of TRIUMEQ and DOVATO in Healthy Adult Participants" Pharmaceutics 15, no. 5: 1470. https://doi.org/10.3390/pharmaceutics15051470
APA StyleChandasana, H., Marnoch, R., McKenna, M., Double, J., Seal, C., Bontempo, G., Wolstenholme, A., & Buchanan, A. (2023). Effect of Food on the Pediatric Dispersible Tablet Formulations of TRIUMEQ and DOVATO in Healthy Adult Participants. Pharmaceutics, 15(5), 1470. https://doi.org/10.3390/pharmaceutics15051470