
Optimization of a Quantitative Anti-Drug Antibodies against Infliximab Assay with the Liquid Chromatography-Tandem Mass Spectrometry: A Method Validation Study and Future Perspectives

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Preparation of Standards, Internal Standard and Quality Controls
2.3. Instrumentation and Chromatographic Conditions
2.4. F(ab’)2 Production
2.5. Sample Preparation
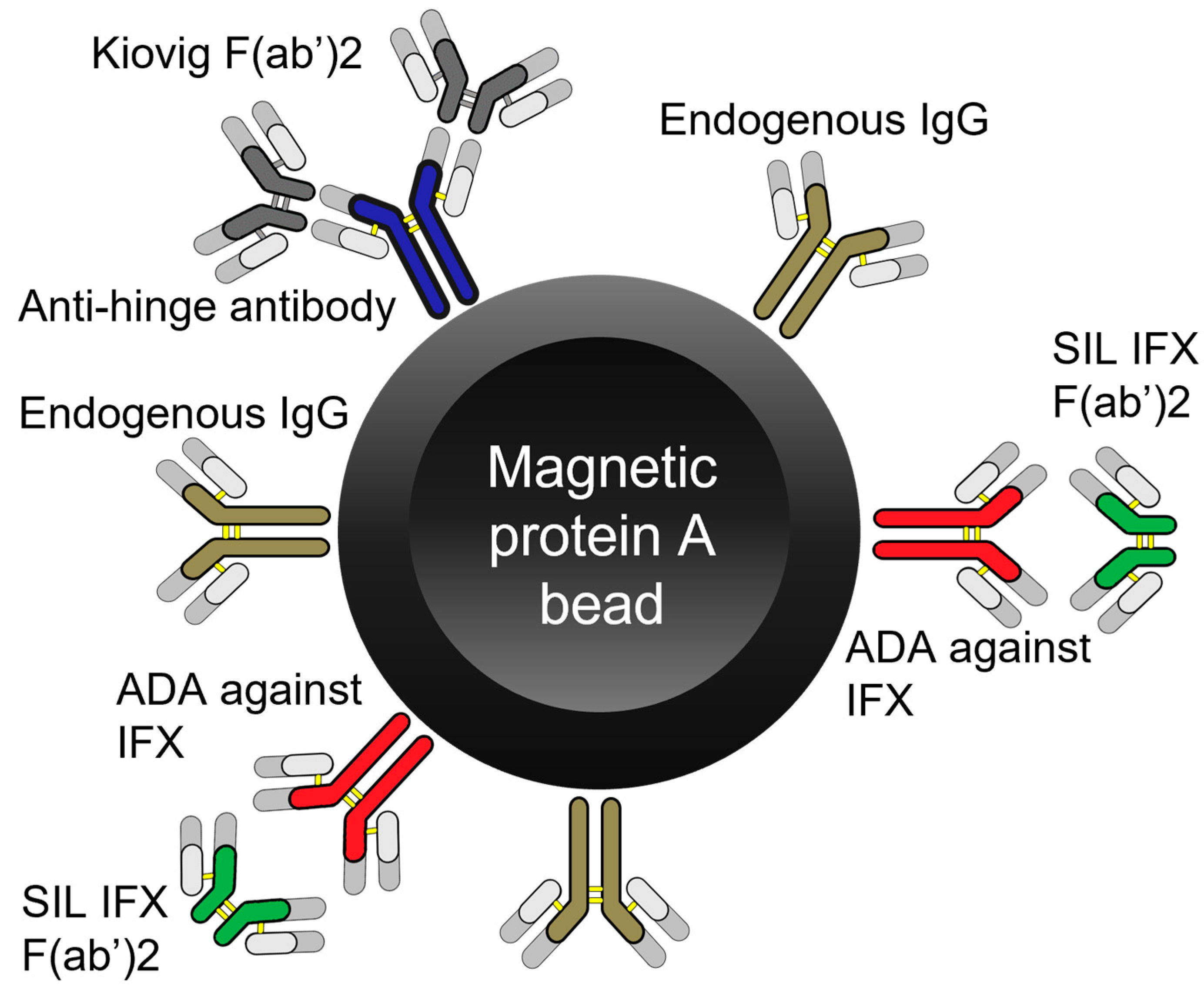
2.6. Magnetic Beads
2.7. Aspecific Interaction
2.8. Validation
2.9. RIA Method for Binding Antibodies
2.10. Patient Samples and Statistical Analysis
3. Results
3.1. Internal Validation Results
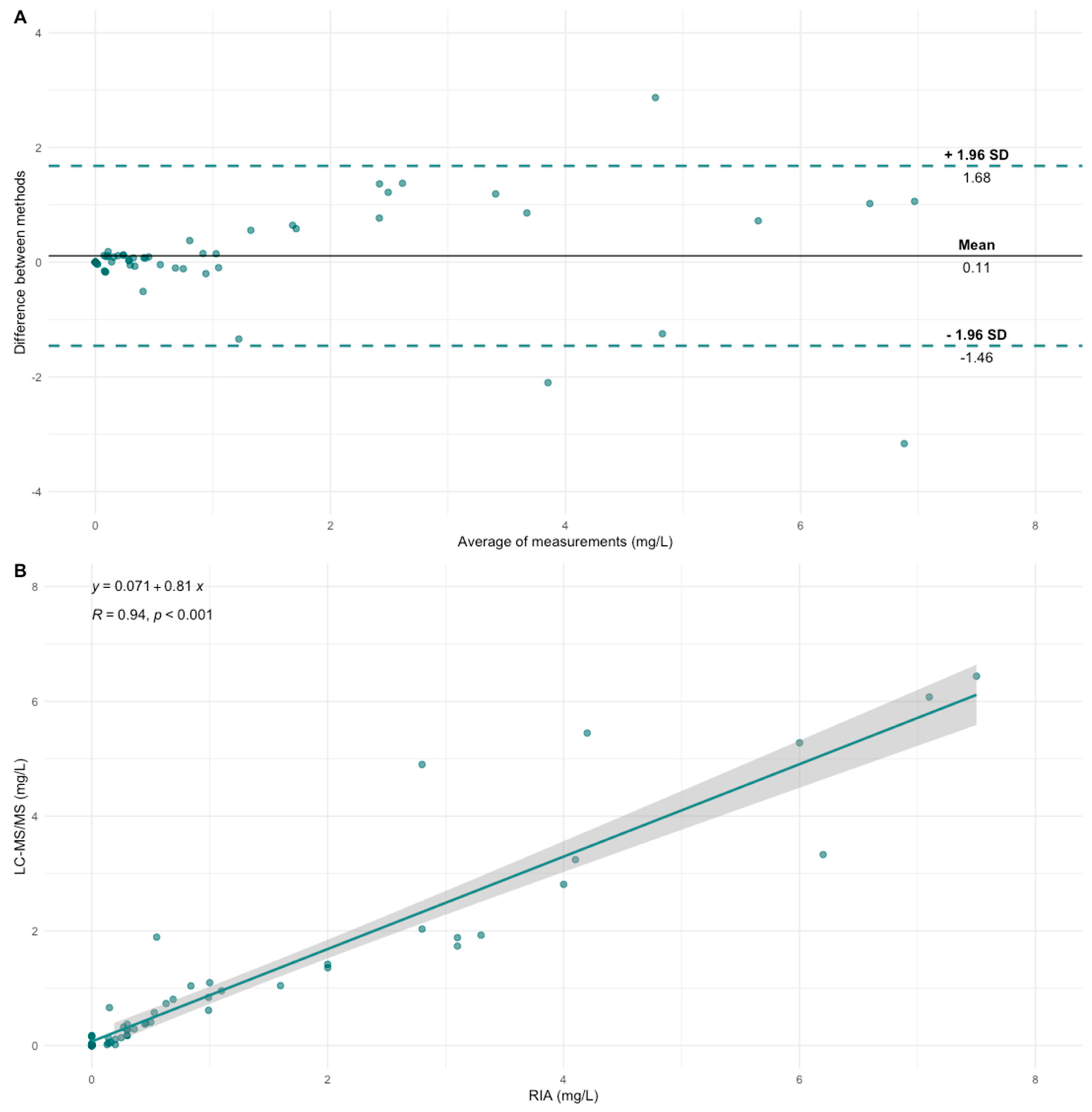
3.2. Cross-Validation
3.3. Magnetic Beads
3.4. Aspecific Interaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Syversen, S.W.; Goll, G.L.; Jørgensen, K.K.; Sandanger, Ø.; Sexton, J.; Olsen, I.C.; Gehin, J.E.; Warren, D.J.; Brun, M.K.; Klaasen, R.A.; et al. Effect of Therapeutic Drug Monitoring vs Standard Therapy during Infliximab Induction on Disease Remission in Patients with Chronic Immune-Mediated Inflammatory Diseases: A Randomized Clinical Trial. JAMA—J. Am. Med. Assoc. 2021, 325, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- Syversen, S.W.; Jørgensen, K.K.; Goll, G.L.; Brun, M.K.; Sandanger, Ø.; Bjørlykke, K.H.; Sexton, J.; Olsen, I.C.; Gehin, J.E.; Warren, D.J.; et al. Effect of Therapeutic Drug Monitoring vs Standard Therapy during Maintenance Infliximab Therapy on Disease Control in Patients with Immune-Mediated Inflammatory Diseases: A Randomized Clinical Trial. JAMA—J. Am. Med. Assoc. 2021, 326, 2375–2384. [Google Scholar] [CrossRef] [PubMed]
- Marquez-Megias, S.; Nalda-Molina, R.; Sanz-Valero, J.; Más-Serrano, P.; Diaz-Gonzalez, M.; Candela-Boix, M.R.; Ramon-Lopez, A. Cost-Effectiveness of Therapeutic Drug Monitoring of Anti-TNF Therapy in Inflammatory Bowel Disease: A Systematic Review. Pharmaceutics 2022, 14, 1009. [Google Scholar] [CrossRef] [PubMed]
- Krishna, M.; Nadler, S.G. Immunogenicity to Biotherapeutics—The Role of Anti-Drug Immune Complexes. Front. Immunol. 2016, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Baert, F.; Noman, M.; Vermeire, S.; van Assche, G.; d’Haens, G.; Carbonez, A.; Rutgeerts, P. Influence of Immunogenicity on the Long-Term Efficacy of Infliximab in Crohn’s Disease. N. Engl. J. Med. 2003, 348, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Nanda, K.S.; Cheifetz, A.S.; Moss, A.C. Impact of Antibodies to Infliximab on Clinical Outcomes and Serum Infliximab Levels in Patients With Inflammatory Bowel Disease (IBD): A Meta-Analysis. Am. J. Gastroenterol. 2013, 108, 40–47. [Google Scholar] [CrossRef] [PubMed]
- vande Casteele, N. Assays for Measurement of TNF Antagonists in Practice. Frontline Gastroenterol. 2017, 8, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Clarke, W.T.; Vande Casteele, N.; Germansky, K.A.; Feuerstein, J.D.; Melmed, G.Y.; Siegel, C.A.; Irving, P.M.; Cheifetz, A.S. Comparison of Assays for Therapeutic Monitoring of Infliximab and Adalimumab in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2021, 19, 839–841.e2. [Google Scholar] [CrossRef]
- Vande Casteele, N.; Buurman, D.J.; Sturkenboom, M.G.G.G.; Kleibeuker, J.H.; Vermeire, S.; Rispens, T.; Van Der Kleij, D.; Gils, A.; Dijkstra, G.; Vande Casteele, N.; et al. Detection of Infliximab Levels and Anti-Infliximab Antibodies: A Comparison of Three Different Assays. Aliment. Pharmacol. Ther. 2012, 36, 765. [Google Scholar] [CrossRef]
- el Amrani, M.; Donners, A.A.M.M.; Hack, C.E.; Huitema, A.D.R.R.; van Maarseveen, E.M. Six-Step Workflow for the Quantification of Therapeutic Monoclonal Antibodies in Biological Matrices with Liquid Chromatography Mass Spectrometry—A Tutorial. Anal. Chim. Acta 2019, 1080, 22–34. [Google Scholar] [CrossRef]
- el Amrani, M.; Göbel, C.; Egas, A.C.; Nierkens, S.; Hack, C.E.; Huitema, A.D.R.; van Maarseveen, E.M. Quantification of Neutralizing Anti-Drug Antibodies and Their Neutralizing Capacity Using Competitive Displacement and Tandem Mass Spectrometry: Infliximab as Proof of Principle. J. Transl. Autoimmun. 2019, 1, 100004. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Afif, W.; Drobne, D.; Dubinsky, M.C.; Ferrante, M.; Irving, P.M.; Kamperidis, N.; Kobayashi, T.; Kotze, P.G.; Lambert, J.; et al. Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease: Unmet Needs and Future Perspectives. Lancet Gastroenterol. Hepatol. 2022, 7, 171–185. [Google Scholar] [CrossRef] [PubMed]
- Myler, H.; Pedras-Vasconcelos, J.; Phillips, K.; Hottenstein, C.S.; Chamberlain, P.; Devanaryan, V.; Gleason, C.; Goodman, J.; Manning, M.S.; Purushothama, S.; et al. Anti-Drug Antibody Validation Testing and Reporting Harmonization. AAPS J. 2022, 24, 4. [Google Scholar] [CrossRef] [PubMed]
- Genovis, A.B.S. FragITTM Kit. Available online: https://www.genovis.com/smartenzymes/antibody-digestion/fabricator/ (accessed on 1 May 2023).
- Promega Corporation Technical Manual: MagneTM Protein A Beads and MagneTM Protein G Beads for Antibody Purification. Available online: https://www.promega.com (accessed on 1 May 2023).
- Rispens, T.; de Vrieze, H.; de Groot, E.; Wouters, D.; Stapel, S.; Wolbink, G.J.; Aarden, L.A. Antibodies to Constant Domains of Therapeutic Monoclonal Antibodies: Anti-Hinge Antibodies in Immunogenicity Testing. J. Immunol. Methods 2012, 375, 93–99. [Google Scholar] [CrossRef]
- EMEA/CHMP/EWP/192217/2009; European Medicines Agency Committee for Medicinal Products for Human Use (CHMP) Guideline on Bioanalytical Method Validation. European Medicines Agency: London, UK, 2011; 44, pp. 1–23.
- European Medicines Agency Committee for Medicinal Products for Human Use (CHMP). Guideline on Immunogenicity Assessment of Therapeutic Proteins; CHMP: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Food and Drug Administration Center for Drug Evaluation and Research (CDER). Immunogenicity Testing of Therapeutic Protein Products—Developing and Validating Assays for Anti-Drug Antibody Detection Guidance for Industry; CDER: Silver Spring, MD, USA, 2019. [Google Scholar]
- Wolbink, G.J.; Vis, M.; Lems, W.; Voskuyl, A.E.; de Groot, E.; Nurmohamed, M.T.; Stapel, S.; Tak, P.P.; Aarden, L.; Dijkmans, B. Development of Antiinfliximab Antibodies and Relationship to Clinical Response in Patients with Rheumatoid Arthritis. Arthritis Rheum. 2006, 54, 711–715. [Google Scholar] [CrossRef]
- Afonso, J.; Lopes, S.; Gonçalves, R.; Caldeira, P.; Lago, P.; Tavares De Sousa, H.; Ramos, J.; Gonçalves, A.R.; Ministro, P.; Rosa, I.; et al. Detection of Anti-Infliximab Antibodies Is Impacted by Antibody Titer, Infliximab Level and IgG4 Antibodies: A Systematic Comparison of Three Different Assays. Ther. Adv. Gastroenterol. 2016, 9, 781–794. [Google Scholar] [CrossRef]
- Van den Abbeele, A.D.; Aaranson, R.A.; Daher, S.; Taube, R.A.; Adelstein, S.J.; Kassis, A.I. Antigen-Binding Site Protection during Radiolabeling Leads to a Higher Immunoreactive Fraction. J. Nucl. Med. 1991, 32, 116–122. [Google Scholar]
- Ovacik, M.; Lin, K. Tutorial on Monoclonal Antibody Pharmacokinetics and Its Considerations in Early Development. Clin. Transl. Sci. 2018, 11, 540–552. [Google Scholar] [CrossRef]
- Van Schie, K.A.; Hart, M.H.; De Groot, E.R.; Kruithof, S.; Aarden, L.A.; Wolbink, G.J.; Rispens, T. The Antibody Response against Human and Chimeric Anti-TNF Therapeutic Antibodies Primarily Targets the TNF Binding Region. Ann. Rheum. Dis. 2015, 74, 311–314. [Google Scholar] [CrossRef]
- Weisshof, R.; Ungar, B.; Blatt, A.; Dahan, A.; Pressman, S.; Waterman, M.; Kopylov, U.; Ben-Horin, S.; Chowers, Y. Anti-Infliximab Antibodies with Neutralizing Capacity in Patients with Inflammatory Bowel Disease: Distinct Clinical Implications Revealed by a Novel Assay. Inflamm. Bowel Dis. 2016, 22, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Paolicelli, D.; D’Onghia, M.; Pellegrini, F.; Direnzo, V.; Iaffaldano, P.; Lavolpe, V.; Trojano, M. The Impact of Neutralizing Antibodies on the Risk of Disease Worsening in Interferon β–Treated Relapsing Multiple Sclerosis: A 5 Year Post-Marketing Study. J. Neurol. 2013, 260, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- vande Casteele, N.; Gils, A.; Singh, S.; Ohrmund, L.; Hauenstein, S.; Rutgeerts, P.; Vermeire, S.; Casteele, N.; vande Gils, A.; Singh, S.; et al. Antibody Response to Infliximab and Its Impact on Pharmacokinetics Can Be Transient. Am. J. Gastroenterol. 2013, 108, 962–971. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Lee, Y.; Choe, B.-H.; Kang, B. Factors Associated with the Immunogenicity of Anti-Tumor Necrosis Factor Agents in Pediatric Patients with Inflammatory Bowel Disease. Gut Liver 2021, 15, 588–598. [Google Scholar] [CrossRef]
- Steenholdt, C. Transient and Persistent Antibodies against TNF-Inhibitors in IBD. Am. J. Gastroenterol. 2015, 110, 1623–1624. [Google Scholar] [CrossRef]
- Ungar, B.; Chowers, Y.; Yavzori, M.; Picard, O.; Fudim, E.; Har-Noy, O.; Kopylov, U.; Eliakim, R.; Ben-Horin, S. The Temporal Evolution of Antidrug Antibodies in Patients with Inflammatory Bowel Disease Treated with Infliximab. Gut 2014, 63, 1258–1264. [Google Scholar] [CrossRef]
- Patton, A.; Mullenix, M.C.; Swanson, S.J.; Koren, E. An Acid Dissociation Bridging ELISA for Detection of Antibodies Directed against Therapeutic Proteins in the Presence of Antigen. J. Immunol. Methods 2005, 304, 189–195. [Google Scholar] [CrossRef]
- Kharlamova, N.; Hermanrud, C.; Dunn, N.; Ryner, M.; Hambardzumyan, K.; Vivar Pomiano, N.; Marits, P.; Gjertsson, I.; Saevarsdottir, S.; Pullerits, R.; et al. Drug Tolerant Anti-Drug Antibody Assay for Infliximab Treatment in Clinical Practice Identifies Positive Cases Earlier. Front. Immunol. 2020, 11, 1365. [Google Scholar] [CrossRef]
- Vande Casteele, N.; Abreu, M.T.; Flier, S.; Papamichael, K.; Rieder, F.; Silverberg, M.S.; Khanna, R.; Okada, L.; Yang, L.; Jain, A.; et al. Patients With Low Drug Levels or Antibodies to a Prior Anti–Tumor Necrosis Factor Are More Likely to Develop Antibodies to a Subsequent Anti–Tumor Necrosis Factor. Clin. Gastroenterol. Hepatol. 2022, 20, 465–467.e2. [Google Scholar] [CrossRef]
- Frederiksen, M.T.; Ainsworth, M.A.; Brynskov, J.; Thomsen, O.Ø.O.; Bendtzen, K.; Steenholdt, C. Antibodies against Infliximab Are Associated with de Novo Development of Antibodies to Adalimumab and Therapeutic Failure in Infliximab-to-Adalimumab Switchers with IBD. Inflamm. Bowel Dis. 2014, 20, 1714–1721. [Google Scholar] [CrossRef]
- Papamichael, K.; Vande Casteele, N.; Abraham, B.P.; Ritter, T.; Jain, A.; Cheifetz, A.S. Prior Antibodies to Infliximab or Adalimumab Are Related to Immunogenicity to Vedolizumab in Patients with Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2022, 11, S1542–S3565. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Mizuno, T.; Colman, R.; Hyams, J.; Noe, J.D.; Boyle, B.; Tsai, Y.; Dong, M.; Jackson, K.; Punt, N.; et al. Real-World Infliximab Pharmacokinetic Study Informs an Electronic Health Record-Embedded Dashboard to Guide Precision Dosing in Children with Crohn’s Disease. Clin. Pharmacol. Ther. 2021, 109, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Chen, L. Current Status of Anti-Drug Antibody Analysis Using Immunocapture-Liquid Chromatography/Mass Spectrometry. J. Appl. Bioanal. 2018, 4, 74–80. [Google Scholar] [CrossRef]
- Qin, Q.; Gong, L. Current Analytical Strategies for Antibody–Drug Conjugates in Biomatrices. Molecules 2022, 27, 6299. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Peptide Sequence | Used as | Precursor (m/z) | Product (m/z) | Product Ion | Charge | CE a (V) | CV b (V) |
|---|---|---|---|---|---|---|---|
| YASESMSGIPSR[13C6,15N4] | Quantifier | 647.80 | 844.42 | y8 | 1+ | 25 | 35 |
| YASESMSGIPSR | IS | 642.80 | 834.41 | y8 | 1+ | 25 | 35 |
| ASQFVGSSIHWYQQR[13C6,15N4] | Qualifier | 601.96 | 759.38 | y12 | 2+ | 17 | 35 |
| ASQFVGSSIHWYQQR | IS | 598.63 | 754.38 | y12 | 2+ | 17 | 35 |
| SINSATHYAESVK[13C6,15N2] | Qualifier | 472.24 | 607.80 | y11 | 2+ | 13 | 35 |
| SINSATHYAESVK | IS | 469.57 | 603.79 | y11 | 2+ | 13 | 35 |
| Precision (% CV) | Accuracy (% bias) | |||
|---|---|---|---|---|
| QC | Within-Run | Between-Run | Overall | Overall |
| LLOQ | 12.3 | 7.8 | 14.6 | 14.8 |
| Low | 7.4 | 2.1 | 7.7 | −0.4 |
| Med | 6.3 | 0 | 6.3 | 7.4 |
| High | 5.9 | 3.1 | 6.7 | 7.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smeijsters, E.H.; van der Elst, K.C.M.; Visch, A.; Göbel, C.; Loeff, F.C.; Rispens, T.; Huitema, A.D.R.; van Luin, M.; El Amrani, M. Optimization of a Quantitative Anti-Drug Antibodies against Infliximab Assay with the Liquid Chromatography-Tandem Mass Spectrometry: A Method Validation Study and Future Perspectives. Pharmaceutics 2023, 15, 1477. https://doi.org/10.3390/pharmaceutics15051477
Smeijsters EH, van der Elst KCM, Visch A, Göbel C, Loeff FC, Rispens T, Huitema ADR, van Luin M, El Amrani M. Optimization of a Quantitative Anti-Drug Antibodies against Infliximab Assay with the Liquid Chromatography-Tandem Mass Spectrometry: A Method Validation Study and Future Perspectives. Pharmaceutics. 2023; 15(5):1477. https://doi.org/10.3390/pharmaceutics15051477
Chicago/Turabian StyleSmeijsters, Erin H., Kim C. M. van der Elst, Amy Visch, Camiel Göbel, Floris C. Loeff, Theo Rispens, Alwin D. R. Huitema, Matthijs van Luin, and Mohsin El Amrani. 2023. "Optimization of a Quantitative Anti-Drug Antibodies against Infliximab Assay with the Liquid Chromatography-Tandem Mass Spectrometry: A Method Validation Study and Future Perspectives" Pharmaceutics 15, no. 5: 1477. https://doi.org/10.3390/pharmaceutics15051477
APA StyleSmeijsters, E. H., van der Elst, K. C. M., Visch, A., Göbel, C., Loeff, F. C., Rispens, T., Huitema, A. D. R., van Luin, M., & El Amrani, M. (2023). Optimization of a Quantitative Anti-Drug Antibodies against Infliximab Assay with the Liquid Chromatography-Tandem Mass Spectrometry: A Method Validation Study and Future Perspectives. Pharmaceutics, 15(5), 1477. https://doi.org/10.3390/pharmaceutics15051477