
Polymer-Drug Anti-Thrombogenic and Hemocompatible Coatings as Surface Modifications




Abstract
:1. Introduction
2. Blood Interactions with Biomaterials
3. Medical Devices
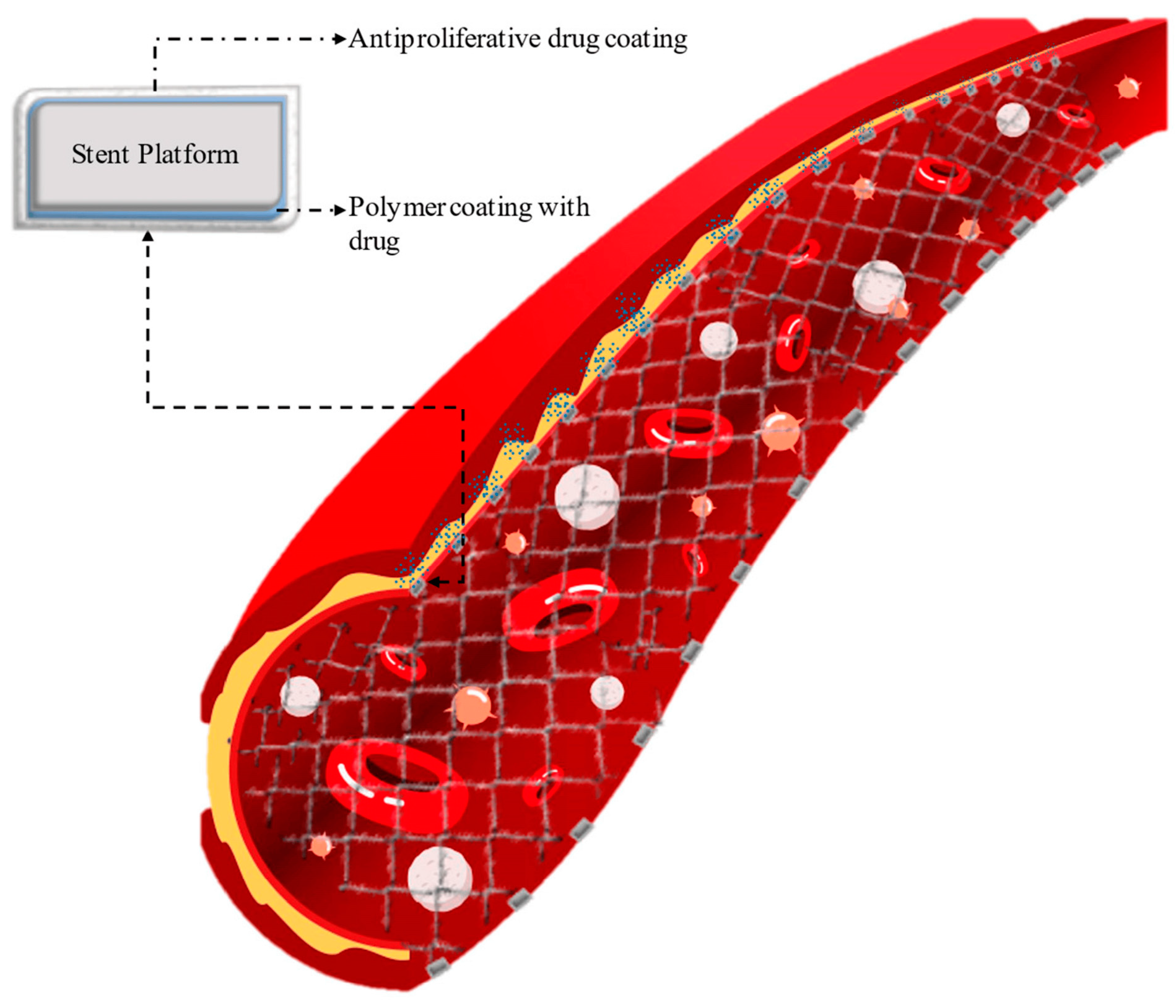
3.1. Stents and Catheters
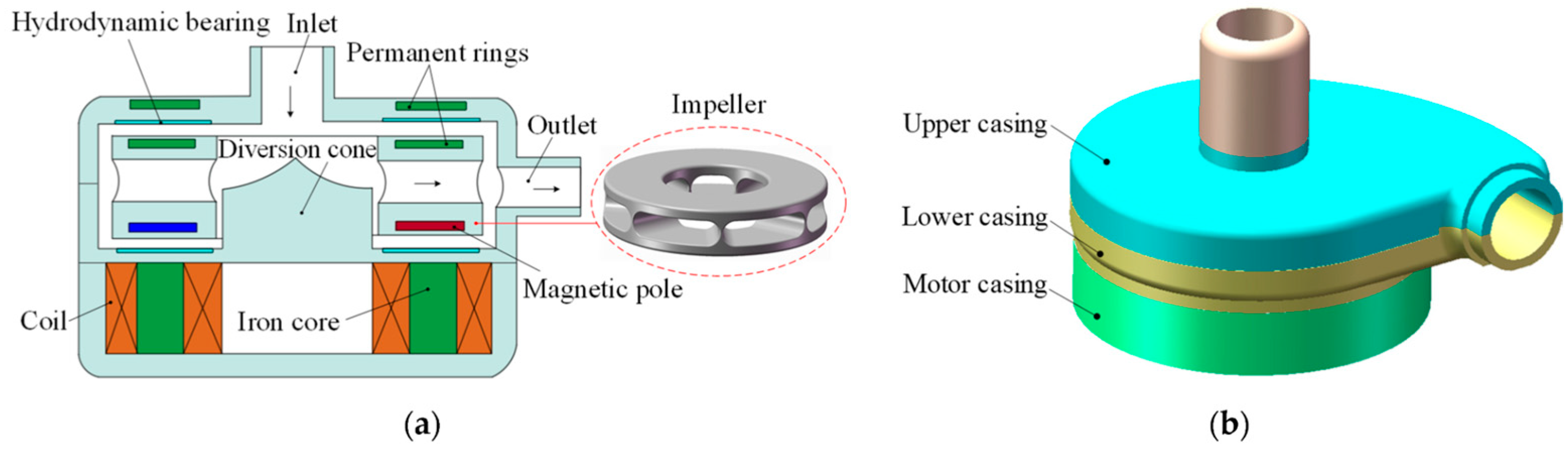
3.2. Blood Pumps and Heart Valves
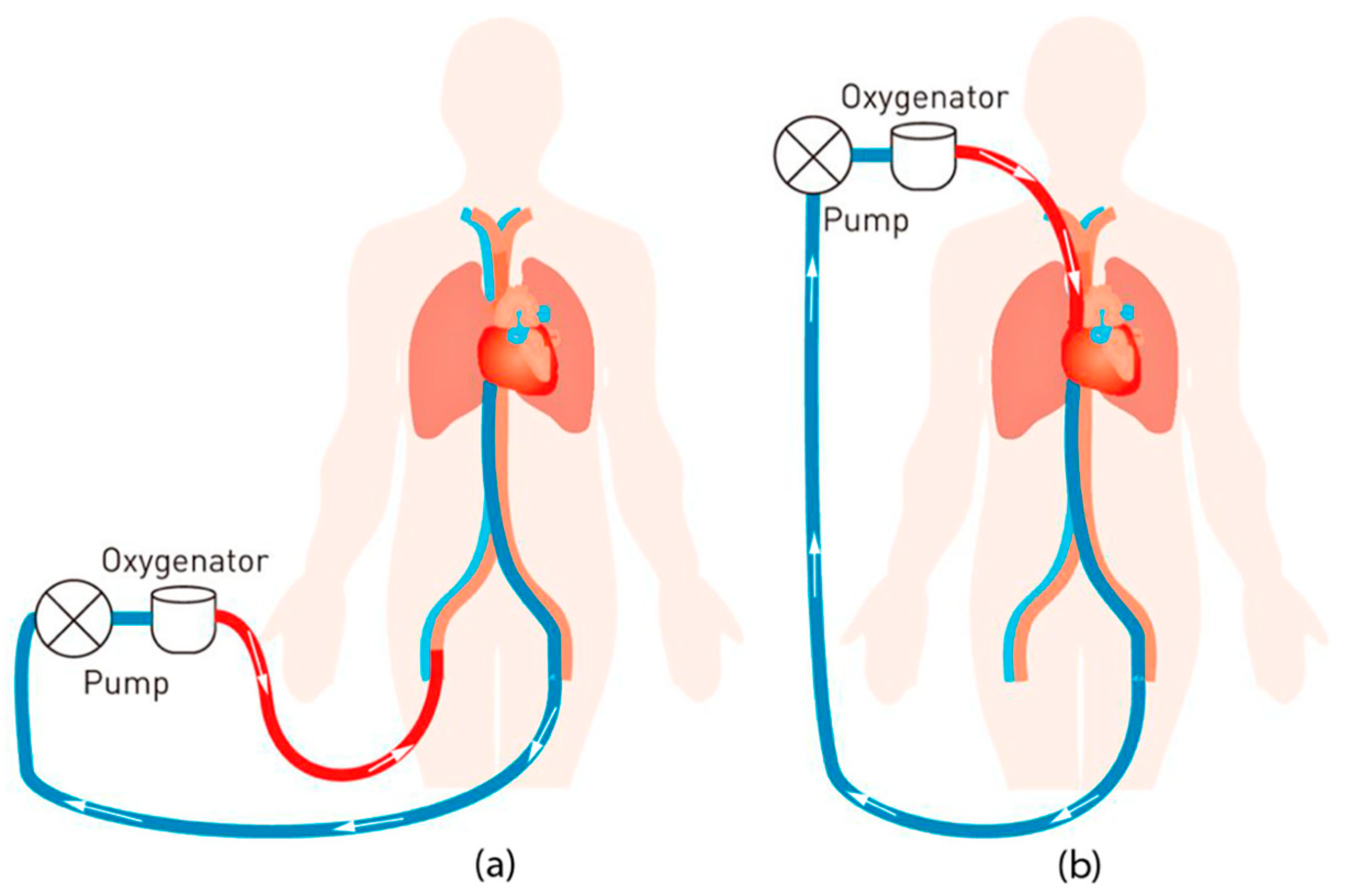
3.3. Artificial Lungs and Extracorporeal Membrane Oxygenation
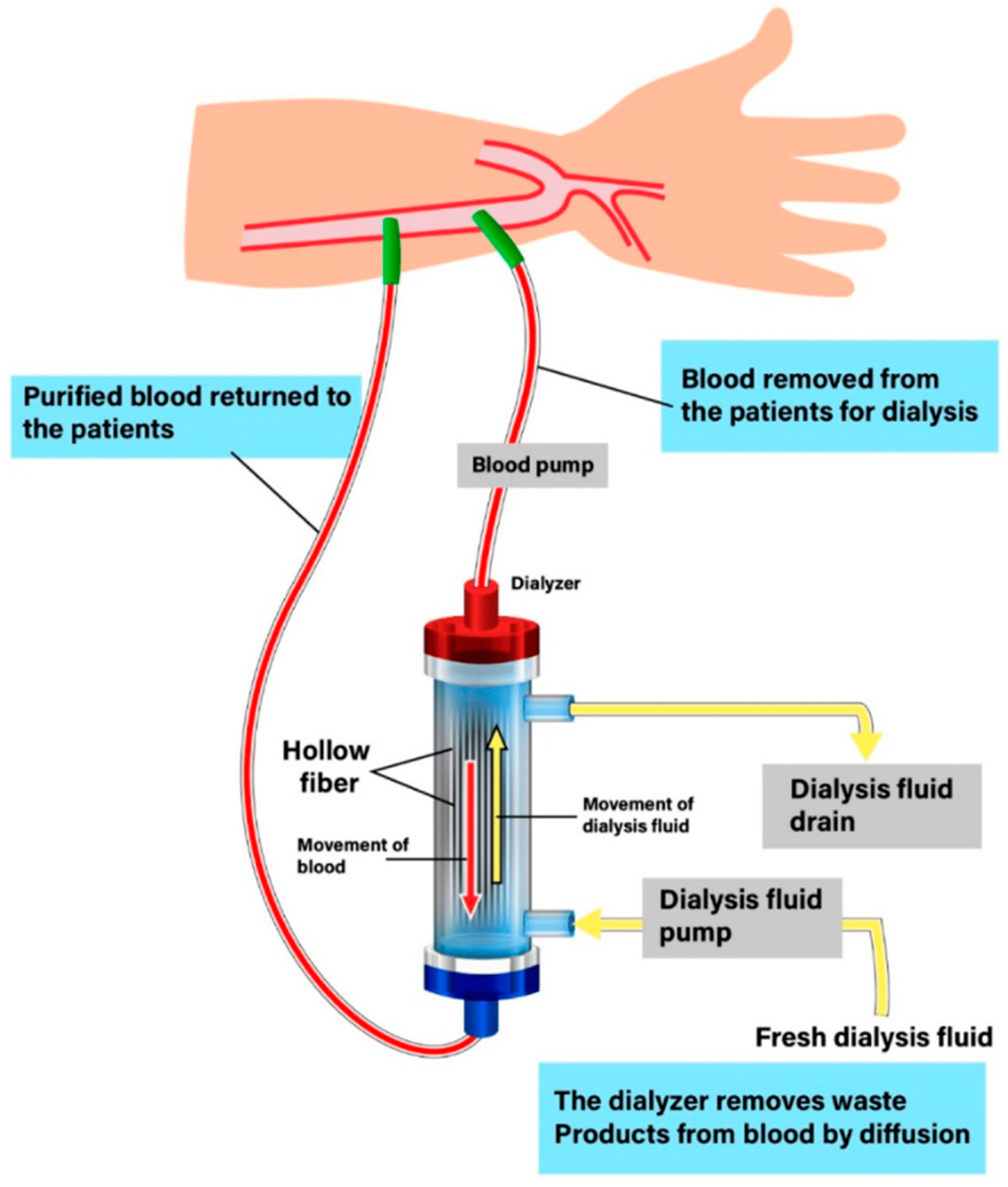
3.4. Hemodialysis Membranes
4. Final Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Scafa Udriște, A.; Niculescu, A.G.; Grumezescu, A.M.; Bădilă, E. Cardiovascular stents: A review of past, current, and emerging devices. Materials 2021, 14, 2498. [Google Scholar] [CrossRef]
- Weber, M.; Steinle, H.; Golombek, S.; Hann, L.; Schlensak, C.; Wendel, H.P.; Avci-Adali, M. Blood-contacting biomaterials: In vitro evaluation of the hemocompatibility. Front. Bioeng. Biotechnol. 2018, 6, 99. [Google Scholar] [CrossRef]
- Nathanael, A.J.; Oh, T.H. Biopolymer coatings for biomedical applications. Polymers 2020, 12, 3061. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yang, L.; Liao, Y.; Yu, H.; Liang, Z.; Zhang, B.; Lan, X.; Luo, R.; Wang, Y. Superhydrophilic versus normal polydopamine coating: A superior and robust platform for synergistic antibacterial and antithrombotic properties. J. Chem. Eng. 2020, 402, 126196. [Google Scholar] [CrossRef]
- Liechty, W.B.; Kryscio, D.R.; Slaughter, B.V.; Peppas, N.A. Polymers for drug delivery systems. Annu. Rev. Chem. Biomol. Eng. 2010, 1, 149–173. [Google Scholar] [CrossRef] [PubMed]
- Gu, B.; Burgess, D.J. Polymeric materials in drug delivery. In Natural and Synthetic Biomedical Polymers; Kumbar, S.G., Laurencin, C.T., Deng, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; Chapter 20; pp. 333–349. [Google Scholar] [CrossRef]
- Vroman, L.; Adams, A.L. Identification of rapid changes at plasma-solid interfaces. J. Biomed. Mater. Res. 1969, 3, 43–67. [Google Scholar] [CrossRef] [PubMed]
- Jaffer, I.H.; Weitz, J.I. The blood compatibility challenge. Part 1: Blood-contacting medical devices: The scope of the problem. Acta Biomater. 2019, 94, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Vroman, L.; Adams, A.L.; Fischer, G.C.; Munoz, P.C. Interaction of high molecular weight kininogen, factor XII, and fibrinogen in plasma at interfaces. Blood 1980, 55, 156–159. [Google Scholar] [CrossRef]
- Schmaier, A.H. The contact activation and kallikrein/kinin systems: Pathophysiologic and physiologic activities. J. Thromb. Haemost. 2016, 14, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Bournazos, S.; Ravetch, J.V. Diversification of IgG effector functions. Int. Immunol. 2017, 29, 303–310. [Google Scholar] [CrossRef]
- Janeway, C.A., Jr.; Travers, P.; Walport, M.; Shlomchik, M. Immunobiology: The Immune System in Health and Disease, 5th ed.; Garland Science: New York, NY, USA, 2001. [Google Scholar]
- Morgan, B.P. The complement system: An overview. Methods Mol. Biol. 2000, 150, 1–13. [Google Scholar] [CrossRef]
- Ricklin, D.; Reis, E.S.; Lambris, J.D. Complement in disease: A defence system turning offensive. Nat. Rev. Nephrol. 2016, 12, 383–401. [Google Scholar] [CrossRef]
- Schraufstatter, I.U.; Trieu, K.; Sikora, L.; Sriramarao, P.; DiScipio, R. Complement C3a and C5a induce different signal transduction cascades in endothelial cells. J. Immunol. 2002, 169, 2102–2110. [Google Scholar] [CrossRef] [PubMed]
- Dole, V.S.; Bergmeier, W.; Mitchell, H.A.; Eichenberger, S.C.; Wagner, D.D. Activated platelets induce Weibel-Palade-body secretion and leukocyte rolling in vivo: Role of P-selectin. Blood 2005, 106, 2334–2339. [Google Scholar] [CrossRef]
- Hoffman, M.; Monroe, D.M. A cell-based model of hemostasis. Thromb. Haemost. 2001, 85, 958–965. [Google Scholar] [PubMed]
- Kawanami, D.; Matoba, K.; Kanazawa, Y.; Ishizawa, S.; Yokota, T.; Utsunomiya, K. Thrombin induces MCP-1 expression through Rho-kinase and subsequent p38MAPK/NF-kB signaling pathway activation in vascular endothelial cells. Biochem. Biophys. Res. Commun. 2011, 411, 798–803. [Google Scholar] [CrossRef]
- Burzynski, L.C.; Humphry, M.; Pyrillou, K.; Wiggins, K.A.; Chan, J.N.E.; Figg, N.; Kitt, L.L.; Summers, C.; Tatham, K.C.; Martin, P.B.; et al. The coagulation and immune systems are directly linked through the activation of interleukin-1α by thrombin. Immunity 2019, 50, 1033–1042. [Google Scholar] [CrossRef]
- Podgórska, K.; Derkacz, A.; Szahidewicz-Krupska, E.; Jasiczek, J.; Dobrowolski, P.; Radziwon-Balicka, A.; Skomro, R.; Szuba, A.; Mazur, G.; Doroszko, A. Effect of regular aerobic activity in young healthy athletes on profile of endothelial function and platelet activity. BioMed Res. Int. 2017, 2017, 8715909. [Google Scholar] [CrossRef]
- White, J. Platelet structural physiology: The ultrastructure of adhesion, secretion, and aggregation in arterial thrombosis. Cardiovasc. Clin. 1987, 18, 13–33. [Google Scholar] [PubMed]
- Sadler, J.E. Biochemistry and genetics of von willebrand factor. Annu. Rev. Biochem. 1998, 67, 395–424. [Google Scholar] [CrossRef]
- Clemetson, K.J.; Clemetson, J.M. Platelet collagen receptors. Thromb. Haemost. 2001, 86, 189–197. [Google Scholar] [CrossRef]
- Chen, J.; Lopez, J.A. Interactions of platelets with subendothelium and endothelium. Microcirculation 2005, 12, 235–246. [Google Scholar] [CrossRef]
- Rivera, J.; Lozano, M.L.; Navarro-Núñez, L.; Vicente, V. Platelet receptors and signaling in the dynamics of thrombus formation. Haematologica 2009, 94, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, P.E.; McEver, R.P.; Shuman, M.A.; Jacques, Y.V.; Bainton, D.F. A platelet alpha-granule membrane protein (GMP-140) is expressed on the plasma membrane after activation. J. Cell Biol. 1985, 101, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Larsen, E.; Celi, A.; Gilbert, G.E.; Furie, B.C.; Erban, J.K.; Bonfanti, R.; Wagner, D.D.; Furie, B. PADGEM protein: A receptor that mediates the interaction of activated platelets with neutrophils and monocytes. Cell 1989, 59, 305–312. [Google Scholar] [CrossRef]
- Amirkhosravi, A.; Amaya, M.; Siddiqui, F.; Biggerstaff, J.P.; Meyer, T.V.; Francis, J.L. Blockade of GpIIb/IIIa inhibits the release of vascular endothelial growth factor (VEGF) from tumor cell-activated platelets and experimental metastasis. Platelets 1999, 10, 285–292. [Google Scholar] [CrossRef]
- Jurasz, P.; Alonso, D.; Castro-Blanco, S.; Murad, F.; Radomski, M.W. Generation and role of angiostatin in human platelets. Blood 2003, 102, 3217–3223. [Google Scholar] [CrossRef] [PubMed]
- Jurasz, P.; Santos-Martinez, M.J.; Radomska, A.; Radomski, M.W. Generation of platelet angiostatin mediated by urokinase plasminogen activator: Effects on angiogenesis. J. Thromb. Haemost. 2006, 4, 1095–1106. [Google Scholar] [CrossRef]
- Fullard, J. The role of the platelet glycoprotein IIb/IIIa in thrombosis and haemostasis. Curr. Pharm. Des. 2004, 10, 1567–1576. [Google Scholar] [CrossRef]
- Tsoi, M.F.; Cheung, C.L.; Cheung, T.T.; Wong, I.C.; Kumana, C.R.; Tse, H.F.; Cheung, B.M. Duration of dual antiplatelet therapy after drug-eluting stent implantation: Meta-analysis of large randomised controlled trials. Sci. Rep. 2015, 5, 13204. [Google Scholar] [CrossRef]
- Ode Boni, B.; Lamboni, L.; Souho, T.; Gauthier, M.; Yang, G. Immunomodulation and cellular response to biomaterials: The orverriding role of neutrophils in healing. Mater. Horiz. 2019, 6, 1122–1137. [Google Scholar] [CrossRef]
- Jokinen, V.; Kankuri, E.; Hoshian, S.; Franssila, S.; Ras, R.H.A. Superhydrophobic blood repellent surfaces. Adv. Mater. 2018, 30, 1705104. [Google Scholar] [CrossRef] [PubMed]
- Christo, S.N.; Diener, K.R.; Bachhuka, A.; Vasilev, K.; Hayball, J.D. Innate immunity and biomaterials at the nexus: Friends or foes. BioMed. Res. Int. 2015, 2015, 342304. [Google Scholar] [CrossRef] [PubMed]
- Barrantes, A.; Wengenroth, J.; Arnebrant, T.; Haugen, H.J. Poly-L-lysine/heparin multilayer coatings prevent blood protein adsorption. J. Colloid Interface Sci. 2017, 485, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Gott, V.L.; Whiffen, J.D.; Dutton, R.C. Heparin bonding on colloidal graphite surfaces. Science 1963, 142, 1297–1298. [Google Scholar] [CrossRef] [PubMed]
- Gerzer, R.; Karrenbrock, B.; Siess, W.; Heim, J.M. Direct comparison of the effects of nitroprusside, SIN 1, and various nitrates on platelet aggregation and soluble guanylate cyclase activity. Thromb. Res. 1988, 52, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Radziwon-Balicka, A.; Lesyk, G.; Back, V.; Fong, T.; Loredo-Calderon, E.L.; Dong, B.; El-Sikhry, H.; El-Sherbeni, A.A.; El-Kadi, A.; Ogg, S.; et al. Differential eNOS-signalling by platelet subpopulations regulates adhesion and aggregation. Cardiovasc Res. 2017, 113, 1719–1731. [Google Scholar] [CrossRef]
- Chen, L.Y.; Mehta, J.L. Further evidence of the presence of constitutive and inducible nitric oxide synthase isoforms in human platelets. J. Cardiovasc. Pharmacol. 1996, 27, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Radomski, M.W.; Palmer, R.M.; Moncada, S. The role of nitric oxide and cGMP in platelet adhesion to vascular endothelium. Biochem. Biophys. Res. Commun. 1987, 148, 1482–1489. [Google Scholar] [CrossRef]
- Lee, C.H.; Chang, S.H.; Lin, Y.H.; Liu, S.J.; Wang, C.J.; Hsu, M.Y.; Hung, K.C.; Yeh, Y.H.; Chen, W.J.; Hsieh, I.C.; et al. Acceleration of re-endothelialization and inhibition of neointimal formation using hybrid biodegradable nanofibrous rosuvastatin-loaded stents. Biomaterials 2014, 35, 4417–4427. [Google Scholar] [CrossRef]
- Sperling, C.; Salchert, K.; Streller, U.; Werner, C. Covalently immobilized thrombomodulin inhibits coagulation and complement activation of artificial surfaces in vitro. Biomaterials 2004, 25, 5101–5113. [Google Scholar] [CrossRef] [PubMed]
- McClung, W.G.; Clapper, D.L.; Hu, S.P.; Brash, J.L. Adsorption of plasminogen from human plasma to lysine-containing surfaces. J. Biomed. Mater. Res. 2000, 49, 409–414. [Google Scholar] [CrossRef]
- Liu, Q.; Li, D.; Zhan, W.; Luan, Y.; Du, H.; Liu, X.; Brash, J.L.; Chen, H. Surfaces having dual affinity for plasminogen and tissue plasminogen activator: In situ plasmin generation and clot lysis. J. Mater. Chem. B Mater. Biol. Med. 2015, 3, 6939–6944. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.R.; Garren, M.R.S.; Handa, H.; Batchinsky, A.I. Toward an artificial endothelium: Development of blood-compatible surfaces for extracorporeal life support. J. Trauma. Acute Care Surg. 2020, 89, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Lock, A.; Cornish, J.; Musson, D.S. The role of in vitro immune response assessment for biomaterials. J. Funct. Biomater. 2019, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Dondossola, E.; Holzapfel, B.M.; Alexander, S.; Filippini, S.; Hutmacher, D.W.; Friedl, P. Examination of the foreign body response to biomaterials by nonlinear intravital microscopy. Nat. Biomed Eng. 2016, 1, 0007. [Google Scholar] [CrossRef] [PubMed]
- Kizhakkedathu, J.N.; Conway, E.M. Biomaterial and cellular implants: Foreign surfaces where immunity and coagulation meet. Blood. 2022, 139, 1987–1998. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics 2012 update. J. Am. Heart Assoc. 2012, 125, e2–e220. [Google Scholar] [CrossRef]
- Jensen, L.O.; Christiansen, E.H. Are drug-eluting stents safer than bare-metal stents? Lancet 2019, 393, 2472–2474. [Google Scholar] [CrossRef]
- Raikar, A.S.; Priya, S.; Bhilegaonkar, S.P.; Somnache, S.N.; Kalaskar, D.M. Surface engineering of bioactive coatings for improved stent hemocompatibility: A comprehensive review. Materials 2023, 16, 6940. [Google Scholar] [CrossRef]
- O’Brien, B.J.; Stinson, J.S.; Larsen, S.R.; Eppihimer, M.J.; Carroll, W.M. A platinum-chromium steel for cardiovascular stents. Biomaterials 2010, 31, 3755–3761. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Jiao, L.; Pang, S.; Yan, P.; Wang, X.; Qiu, T. The development of design and manufacture techniques for bioresorbable coronary artery stents. Micromachines 2021, 12, 990. [Google Scholar] [CrossRef] [PubMed]
- Koźlik, M.; Harpula, J.; Chuchra, P.J.; Nowak, M.; Wojakowski, W.; Gąsior, P. Drug-eluting stents: Technical and clinical progress. Biomimetics 2023, 8, 72. [Google Scholar] [CrossRef] [PubMed]
- McQueen, A.; Escuer, J.; Schmidt, A.F.; Aggarwal, A.; Kennedy, S.; McCormick, C.; Oldroyd, K.; McGinty, S. An intricate interplay between stent drug dose and release rate dictates arterial restenosis. J. Control. Release 2022, 349, 992–1008. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.Y.; Chen, C.-C.; Wang, C.-Y.; Chang, S.-H.; Hsieh, M.-J.; Lee, C.-H.; Wu, V.C.-C.; Hsieh, I.-C. The development of coronary artery stents: From bare-metal to bio-resorbable types. Metals 2016, 6, 168. [Google Scholar] [CrossRef]
- Rodriguez-Granillo, A.; Rubilar, B.; Rodriguez-Granillo, G.; Rodriguez, A.E. Advantages and disadvantages of biodegradable platforms in drug eluting stents. World J. Cardiol. 2011, 3, 84–92. [Google Scholar] [CrossRef]
- Akinapelli, A.; Chen, J.P.; Roy, K.; Donnelly, J.; Dawkins, K.; Huibregtse, B.; Hou, D. Current state of bioabsorbable polymer-coated drug-eluting stents. Curr. Cardiol. Rev. 2017, 13, 139–154. [Google Scholar] [CrossRef]
- Babos, G.; Rydz, J.; Kawalec, M.; Klim, M.; Fodor-Kardos, A.; Trif, L.; Feczkó, T. Poly(3-hydroxybutyrate)-based nanoparticles for sorafenib and doxorubicin anticancer drug delivery. Int. J. Mol. Sci. 2020, 21, 7312. [Google Scholar] [CrossRef]
- Itoh, T.; Otake, H.; Kimura, T.; Tsukiyama, Y.; Kikuchi, T.; Okubo, M.; Hayashi, T.; Okamura, T.; Kuramitsu, S.; Morita, T.; et al. A serial optical frequency-domain imaging study of early and late vascular responses to bioresorbable-polymer sirolimus-eluting stents for the treatment of acute myocardial infarction and stable coronary artery disease patients: Results of the MECHANISM-U. Cardiovasc. Interv. Ther. 2022, 37, 281–292. [Google Scholar] [CrossRef]
- Garg, S.; Serruys, P.W. Coronary stents: Current status. J. Am. Coll. Cardiol. 2010, 56, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Bravo Baptista, S. The third generation of drug-eluting stents: Reassuring data while we wait for the next one. Rev. Port. Cardiol. 2021, 40, 77–80. [Google Scholar] [CrossRef]
- Hassan, S.; Ali, M.N.; Ghafoor, B. Evolutionary perspective of drug eluting stents: From thick polymer to polymer free approach. J. Cardiothorac. Surg. 2022, 17, 65. [Google Scholar] [CrossRef]
- Polimeni, A.; Sorrentino, S.; Spaccarotella, C.; Mongiardo, A.; Sabatino, J.; De Rosa, S.; Gori, T.; Indolfi, C. Stent thrombosis after percutaneous coronary. Interv. Cardiol. Clin. 2020, 38, 639–647. [Google Scholar] [CrossRef]
- Opálková Šišková, A.; Bučková, M.; Kroneková, Z.; Kleinová, A.; Nagy, Š.; Rydz, J.; Opálek, A.; Sláviková, M.; Eckstein Andicsová, A. The drug-loaded electrospun poly(ε-caprolactone) mats for therapeutic application. Nanomaterials 2021, 11, 922. [Google Scholar] [CrossRef] [PubMed]
- Rocher, L.; Cameron, J.; Barr, J.; Dillon, B.; Lennon, A.B.; Menary, G.H. Linking processing, microstructure and mechanical properties of expanded PLLA tubes for bioresorbable stent applications. Eur. Polym. J. 2023, 195, 112205. [Google Scholar] [CrossRef]
- Torki, M.M.; Hassanajili, S.; Jalisi, M.M. Design optimizations of PLA stent structure by FEM and investigating its function in a simulated plaque artery. Math. Comput. Simul. 2019, 169, 103–116. [Google Scholar] [CrossRef]
- Musioł, M.; Jurczyk, S.; Kwiecień, M.; Smola-Dmochowska, A.; Domański, M.; Janeczek, H.; Włodarczyk, J.; Klim, M.; Rydz, J.; Kawalec, M.; et al. The impact of shape memory test on degradation profile of a bioresorbable polymer. J. Mech. Behav. Biomed. Mater. 2018, 81, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Yiqing, G.; Tian, Y.; Cheng, J.; Zhao, G. Preparation and evaluation of PDLLA/sirolimus coatings on fully bioabsorbable drug-eluting stents. In ICBET ‘18: Proceedings of the 2018 8th International Conference on Biomedical Engineering and Technology, New York, NY, USA, 23–25 April 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 65–70. [Google Scholar] [CrossRef]
- Xu, W.; Sasaki, M.; Niidome, T. Sirolimus release from biodegradable polymers for coronary stent application: A review. Pharmaceutics 2022, 14, 492. [Google Scholar] [CrossRef] [PubMed]
- Wulf, K.; Goblet, M.; Raggl, S.; Teske, M.; Eickner, T.; Lenarz, T.; Grabow, N.; Paasche, G. PLLA Coating of active implants for dual drug release. Molecules 2022, 27, 1417. [Google Scholar] [CrossRef]
- Lih, E.; Jung, J.W.; Joung, Y.K.; Ahn, D.J.; Han, D.K. Synergistic effect of anti-platelet and anti-inflammation of drug-coated Co-Cr substrates for prevention of initial in-stent restenosis. Colloids Surf B Biointerfaces 2016, 140, 353–360. [Google Scholar] [CrossRef]
- Matsuda, Y.; Ashikaga, T.; Sasaoka, T.; Hatano, Y.; Umemoto, T.; Lee, T.; Yonetsu, T.; Maejima, Y.; Sasano, T. Comparison of neointimal response between durable-polymer everolimus-eluting stent and bioabsorbable-polymer everolimus-eluting stent for severely calcified lesions requiring rotational atherectomy. Int. Heart J. 2020, 61, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Li, J.; Deng, D.; Wu, G.; Zhou, M.; Zhao, G.; Ni, Z. Improved mechanical properties of poly(L-lactic acid) stent coated by poly(D,L-lactic acid) and poly(L-lactic-co-glycolic acid) biopolymer blend. Polym. Adv. Technol. 2022, 33, 1109–1115. [Google Scholar] [CrossRef]
- Guerra, A.J.; Ciurana, J. 3D-printed bioabsordable polycaprolactone stent: The effect of process parameters on its physical features. Mater. Des. 2018, 13, 430–437. [Google Scholar] [CrossRef]
- Zhao, J.; Mo, Z.; Guo, F.; Shi, D.; Han, Q.Q.; Liu, Q. Drug loaded nanoparticle coating on totally bioresorbable PLLA stents to prevent in-stent restenosis. J. Biomed. Mater. Res.–B Appl. Biomater. 2017, 106, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.M.; Amaro, A.M.; Piedade, A.P. 3D printing of polymeric bioresorbable stents: A strategy to improve both cellular compatibility and mechanical properties. Polymers 2022, 14, 1099. [Google Scholar] [CrossRef]
- Ormiston, J.A.; Serruys, P.W.S. Bioabsorbable coronary stents. Circ. Cardiovasc. Interv. 2009, 2, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Jo, H.H.; Lim, K.S.; Lim, D.; Lee, S.; Lee, J.H.; Kim, W.D.; Jeong, M.H.; Lim, J.Y.; Kwon, I.K.; et al. Heparin coating on 3D printed poly (L-lactic acid) biodegradable cardiovascular stent via mild surface modification approach for coronary artery implantation. Chem. Eng. J. 2019, 378, 122116. [Google Scholar] [CrossRef]
- Pan, K.; Zhang, W.; Shi, H.; Dai, M.; Wei, W.; Liu, X.; Li, X. Zinc Ion-crosslinked polycarbonate/heparin composite coatings for biodegradable Zn-alloy stent applications. Colloids Surf. B 2022, 218, 112725. [Google Scholar] [CrossRef]
- Dai, S.; Gao, Y.; Duan, L. Recent advances in hydrogel coatings for urinary catheters. J. Appl. Polym. Sci. 2023, 140, 53701. [Google Scholar] [CrossRef]
- Mandal, A. Catheter Uses. Available online: https://www.news-medical.net/health/Catheter-Uses.aspx (accessed on 14 November 2023).
- Low, J.L.; Hsien-Neng Kao, P.; Tambyah, P.A.; Koh, G.L.E.; Ling, H.; Kline, K.A.; Cheow, W.S.; Leong, S.S.J. Development of a polymer-based antimicrobial coating for efficacious urinary catheter protection. Biotechnol. Notes. 2021, 2, 1–10. [Google Scholar] [CrossRef]
- Mulinti, P.; Kalita, D.; Hasan, R.; Quadir, M.; Wang, Y.; Brooks, A. Development and processing of novel heparin binding functionalized modified spider silk coating for catheter providing dual antimicrobial and anticoagulant properties. Materialia 2020, 14, 100937. [Google Scholar] [CrossRef] [PubMed]
- Opálková Šišková, A.; Kozma, E.; Opálek, A.; Kroneková, Z.; Kleinová, A.; Nagy, Š.; Kronek, J.; Rydz, J.; Eckstein Andicsová, A. Diclofenac embedded in silk fibroin fibers as a drug delivery system. Materials 2020, 13, 3580. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Yu, H.; Wang, L.; Zhou, D.; Duan, X.; Zhang, X.; Yin, J.; Luan, S.; Shi, H. Heparin-network-mediated long-lasting coatings on intravascular catheters for adaptive antithrombosis and antibacterial infection. Nat. Commun. 2024, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Voss, B.; Krane, M.; Jung, C.; Brockmann, G.; Braun, S.; Günther, T.; Lange, R.; Bauernschmitt, R. Cardiopulmonary bypass with physiological flow and pressure curves: Pulse is unnecessary! Eur. J. Cardiothorac. Surg. 2010, 37, 223–232. [Google Scholar] [CrossRef]
- Fu, M.; Liu, G.; Wang, W.; Gao, B.; Ji, B.; Chang, Y.; Liu, Y. Hemodynamic evaluation and in vitro hemolysis evaluation of a novel centrifugal pump for extracorporeal membrane oxygen. Ann. Transl. Med. 2021, 9, 679. [Google Scholar] [CrossRef]
- Ahmed, A.; Wang, X.; Yang, M. Biocompatible materials of pulsatile and rotary blood pumps: A brief review. Rev. Adv. Mater. Sci. 2020, 59, 322–339. [Google Scholar] [CrossRef]
- Shen, P.; Wang, Y.; Chen, Y.; Fu, P.; Zhou, L.; Liu, L. Hydrodynamic bearing structural design of blood pump based on axial passive suspension stability analysis of magnetic-hydrodynamic hybrid suspension system. Machines 2021, 9, 255. [Google Scholar] [CrossRef]
- Teo, A.J.T.; Mishra, A.; Park, I.; Kim, Y.J.; Park, W.T.; Yoon, Y.J. Polymeric biomaterials for medical implants and devices. ACS Biomater. Sci. Eng. 2016, 2, 454–472. [Google Scholar] [CrossRef]
- Cleveland Clinic. Available online: https://my.clevelandclinic.org/health/body/17067-heart-valves (accessed on 12 December 2023).
- Singh, S.K.; Kachel, M.; Castillero, E.; Xue, Y.; Kalfa, D.; Ferrari, G.; Isaac, G. Polymeric prosthetic heart valves: A review of current technologies and future directions. Front. Cardiovasc. Med. 2023, 10, 1137827. [Google Scholar] [CrossRef] [PubMed]
- Oveissi, F.; Naficy, S.; Lee, A.; Winlaw, D.S.; Dehghani, F. Materials and manufacturing perspectives in engineering heart valves: A review. Mater. Today Bio 2020, 5, 100038. [Google Scholar] [CrossRef] [PubMed]
- Ovcharenko, E.A.; Seifalian, A.; Rezvova, M.A.; Klyshnikov, K.A. New nanocomposite copolymer based on functionalised graphene oxide for development of heart valves. Sci. Rep. 2020, 10, 5271. [Google Scholar] [CrossRef]
- Motta, S.E.; Peters, M.M.; Chantre, C.O.; Chang, H.; Cera, L.; Liu, Q.; Cordoves, E.M.; Fioretta, E.S.; Zaytseva, P.; Cesarovic, N.; et al. On-demand heart valve manufacturing using focused rotary jet spinning. Matter 2023, 6, 1860–1879. [Google Scholar] [CrossRef]
- Mahmood, A.S. Improvement of the fatigue life of 3D printed nano soft artificial heart and heart valves. Iran. J. Mater. Sci. Eng. 2023, 20, 4. [Google Scholar] [CrossRef]
- Jafari, A.; Vahid Niknezhad, S.; Kaviani, M.; Saleh, W.; Wong, N.; Van Vliet, P.P.; Moraes, C.; Ajji, A.; Kadem, L.; Azarpira, N.; et al. Formulation and evaluation of PVA/gelatin/carrageenan inks for 3D printing and development of tissue-engine heart valves. Adv. Funct. Mater. 2023, 34, 2305188. [Google Scholar] [CrossRef]
- Prawel, D.A.; Dean, H.; Forleo, M.; Lewis, N.; Gangwish, J.; Popat, K.C.; Dasi, L.P.; James, S.P. Hemocompatibility and hemodynamics of novel hyaluronan-polyethylene materials for flexible heart valve leaflets. Cardiovasc. Eng. Technol. 2014, 5, 70–81. [Google Scholar] [CrossRef]
- Park, A.; Song, Y.; Yi, E.; Nguyen, B.T.D.; Han, D.; Sohn, E.H.; Park, Y.; Jung, J.T.; Lee, Y.M.; Cho, Y.H.; et al. Blood oxygenation using fluoropolymer-based artificial lung membranes. ACS Biomater. Sci. Eng. 2020, 6, 6424–6434. [Google Scholar] [CrossRef] [PubMed]
- Geertsma, R.E.; Dekker, R.J.; de Bruijn, A.C.P.; Wassenaar, C.; Hilbers, E.S.M.; Roszek, B. Artificial Organs State-of-the-Art Technology for Device-Based and Cell/Tissue-Based Approaches. RIVM report 360050011/2008. Available online: https://www.rivm.nl/bibliotheek/rapporten/360050011.pdf (accessed on 15 November 2023).
- Alhomsi, Y.; Alsalemi, A.; Noorizadeh, M.; Bensaali, F.; Meskin, N.; Hssain, A.A. A Modular approach for a patient unit for extracorporeal membrane oxygenation simulator. Membranes 2021, 11, 424. [Google Scholar] [CrossRef]
- Olson, S.R.; Murphree, C.R.; Zonies, D.; Meyer, A.D.; Mccarty, O.J.T.; Deloughery, T.G.; Shatzel, J.J. Thrombosis and bleeding in extracorporeal membrane oxygenation (ECMO) without anticoagulation: A systematic review. ASAIO J. 2021, 67, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Rajsic, S.; Breitkopf, R.; Jadzic, D.; Popovic Krneta, M.; Tauber, H.; Treml, B. Anticoagulation strategies during extracorporeal membrane oxygenation: A narrative review. J. Clin. Med. 2022, 31, 5147. [Google Scholar] [CrossRef]
- Große-Berkenbusch, K.; Avci-Adali, M.; Arnold, M.; Cahalan, L.; Cahalan, P.; Velic, A.; Maček, B.; Schlensak, C.; Wendel, H.P.; Stoppelkamp, S. Profiling of time-dependent human plasma protein adsorption on non-coated and heparin-coated oxygenator membranes. Biomater. Adv. 2022, 39, 213014. [Google Scholar] [CrossRef]
- Gerling, K.; Ölschläger, S.; Avci-Adali, M.; Neumann, B.; Schweizer, E.; Schlensak, C.; Wendel, H.P.; Stoppelkamp, S. A Novel C1-esterase inhibitor oxygenator coating prevents FXII activation in human blood. Biomolecules 2020, 10, 1042. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Man, J.; Liu, J.; Li, J.; Song, X.; Wang, J.; Li, J.; Chen, Y. Construction of the mussel-inspired PDAM/lysine/heparin composite coating combining multiple anticoagulant strategies. ACS Appl. Mater. Interfaces 2023, 15, 27719–27731. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Man, J.; Wang, J.; Liu, J.; Song, X.; Yu, X.; Li, J.; Li, R.; Qiu, Y.; Li, J.; et al. Surface modification of polyvinyl chloride with sodium alginate/carboxymethyl chitosan and heparin for realizing the anticoagulation. Int. J. Biol. Macromol. 2023, 254, 127653. [Google Scholar] [CrossRef]
- Abdelrasoul, A.; Kalugin, D.; Shoker, A. Recent developments and current challenges of heparin-grafted hemodialysis membranes. J. Compos. Sci. 2022, 6, 244. [Google Scholar] [CrossRef]
- Radu, E.R.; Voicu, S.I.; Thakur, V.K. Polymeric membranes for biomedical applications. Polymers 2023, 15, 619. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-A.; Ou, S.-M.; Lin, C.-C. Influence of dialysis membranes on clinical outcomes: From history to innovation. Membranes 2022, 12, 152. [Google Scholar] [CrossRef] [PubMed]
- Kalugin, D.; Bahig, J.; Shoker, A.; Abdelrasoul, A. Heparin-immobilized polyethersulfone for hemocompatibility enhancement of dialysis membrane: In situ synchrotron imaging, experimental, and ex vivo studies. Membranes 2023, 13, 718. [Google Scholar] [CrossRef]
- Rose, I.I.; Kather, M.; Roth, H.; Dünkelberg, H.; Rein, L.; Klimosch, S.N.; Schmolz, M.; Wessling, M. Single-step chitosan functionalized membranes for heparinization. J. Membr. Sci. 2022, 655, 120567. [Google Scholar] [CrossRef]
- Lu, Y.T.; Zeng, K.; Fuhrmann, B.; Woelk, C.; Zhang, K.; Groth, T. Engineering of stable cross-linked multilayers based on thermo-responsive PNIPAM-grafted-chitosan/heparin to tailor their physiochemical properties and biocompatibility. ACS Appl. Mater. Interfaces 2022, 14, 29550–29562. [Google Scholar] [CrossRef]
- Jian, R.L.; Mao, L.B.; Xu, Y.; Li, X.F.; Wang, F.P.; Luo, X.G.; Zhou, H.; He, H.P.; Wang, N.; Zhang, T.C. Generation of insulin-producing cells from C3H10T1/2 mesenchymal progenitor cells. Gene 2015, 562, 107–116. [Google Scholar] [CrossRef]
- Smith, B.R.; Edelman, E.R. Nanomedicines for cardiovascular disease. Nat. Cardiovasc. Res. 2023, 2, 351–367. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stent | Drug | Dosage [μg/mm2] | Drug Release [%]/Time [week] | Polymer/Coating | References |
|---|---|---|---|---|---|
| Alex (Balton, Warsaw, Poland) | Sirolimus | 1.0 | 100/8 | poly(D,L-lactide-co-glycolide) | [60,61] |
| Orsiro (Biotronik, Poznań, Poland) | Sirolimus | 1.4 | 50/4 80/12 | PROBIO poly(L-lactide) | [61,62,63] |
| BioMatrix (Biosensors, Irvine, CA, USA) | Biolimus A9™ | 15.6 | 45/4 | polylacticacid | [63,64] |
| Ultimaster™ (Terumo Corporation, Tokyo, Japan) | Sirolimus | 3.9 | 100/12–16 | poly(D,L-lactide-co-caprolactone) | [64,65] |
| Synergy™ (Boston Scientific, Marlborough, MA, USA) | Everolimus | 1.0 | 12 | poly(D,L-lactide-co-glycolide) | [65] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawidlak-Węgrzyńska, B.; Rydz, J.; Musioł, M.; Radziwon-Balicka, A. Polymer-Drug Anti-Thrombogenic and Hemocompatible Coatings as Surface Modifications. Pharmaceutics 2024, 16, 432. https://doi.org/10.3390/pharmaceutics16030432
Zawidlak-Węgrzyńska B, Rydz J, Musioł M, Radziwon-Balicka A. Polymer-Drug Anti-Thrombogenic and Hemocompatible Coatings as Surface Modifications. Pharmaceutics. 2024; 16(3):432. https://doi.org/10.3390/pharmaceutics16030432
Chicago/Turabian StyleZawidlak-Węgrzyńska, Barbara, Joanna Rydz, Marta Musioł, and Aneta Radziwon-Balicka. 2024. "Polymer-Drug Anti-Thrombogenic and Hemocompatible Coatings as Surface Modifications" Pharmaceutics 16, no. 3: 432. https://doi.org/10.3390/pharmaceutics16030432
APA StyleZawidlak-Węgrzyńska, B., Rydz, J., Musioł, M., & Radziwon-Balicka, A. (2024). Polymer-Drug Anti-Thrombogenic and Hemocompatible Coatings as Surface Modifications. Pharmaceutics, 16(3), 432. https://doi.org/10.3390/pharmaceutics16030432