
Remote Monitoring Model for the Preoperative Prehabilitation Program of Patients Requiring Abdominal Surgery



Abstract
:1. Introduction
2. Current Prehabilitation Programs
2.1. Key Outcome Measures Used to Assess the Efficacy of Prehabilitation
2.2. Prehabilitation Program Parameters

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prehabilitation Period | Frequency of Exercise | Activities/Modalities | Intensity |
|---|---|---|---|
| Supervised Prehabilitation | |||
| no record [4] | 45–60 min, 2 times per week | treadmill, rowing, and resistance exercises (leg press, chest press and lateral pull down) | moderate |
| six weeks [5] | 20–30 min, 5 times per week | cross trainer, rowing, cycling | moderate and vigorous |
| four weeks average [18] | 30 min, 3 to 4 times per week | walking, cycling, jogging and resistance exercises | moderate |
| two-four weeks [19] | 60 min, 2 times per week | aerobic training, resistance exercises with inspiratory training | moderate and vigorous |
| Unsupervised Prehabilitation | |||
| four weeks [8] | 50 min, 3 times per week | walking, running, cycling and resistance exercises | light, moderate and vigorous |
| two weeks [9] | 30 min daily | pulmonary exercises- extensive breathing exercise and Walking | no record |
2.3. Incidental Exercise and Inactivity
2.4. Threshold Time and Intensities
3. Development of a Mixed Prehabilitation Program Model
| Prehabilitation Elements | Prehabilitation Boundaries | Remarks |
|---|---|---|
| Time frame of prehabilitation program | Four weeks or six weeks | May be less or more based on the patient status and surgery scheduled. |
| Number of sessions per week | Minimum two sessions | The patient could perform any number of sessions according to the health supervisor guidance. |
| Threshold time of physical activity per week | 150 min moderate intensity or equivalent | 75 min of vigorous intensity is considered equal to 150 min moderate intensity [30,31]. |
| Intensity level | Light, moderate, vigorous | Light >50% of maximal heart rate, moderate 50–70% of maximal heart rate, vigorous 70–80% of maximal heart rate [4]. |
| Minimum time of each session | 10 min or more at a moderate intensity | 5 min of vigorous is equal to 10 min of moderate and approximately 15 min of light intensity [28,29]. |
| Physical exercise types | Walking, running, cross trainer, rowing, treadmill, step up, leg press, cycling, staircase ascending/descending | This could be any pair or more of these nine activities, and is based on the physician’s and physiotherapist’s recommendations. |
| Location of the prehabilitation program | Indoor, GYM, outdoor | According to the availability of physical resources and the patient status. |
| Negative impact | Bed rest | Each day of bed rest will produce negative credit and eliminate the effort of one day of recommended physical activity [14,25]. |
Mathematical Formula of the Mixed Prehabilitation Program
- is the credit gained for the prehabilitation program independent of the total program duration. Common prehabilitation programs have a length of four or six weeks. In this study, we used a six-week prehabilitation program that is represented as . A four-week prehabilitation program is represented by the symbol .
- indicates the exercise intensity level. Here 0.75 is allocated for light intensity, 1 for moderate intensity, and 2 for vigorous intensity. The weighting of the different intensities is based the relative effect of each intensity on improvements in health and fitness [20,22,28,29] described in Section 2.4.
- is the minimum threshold time. This threshold is 10 min of physical activity at a moderate or vigorous intensity [15].
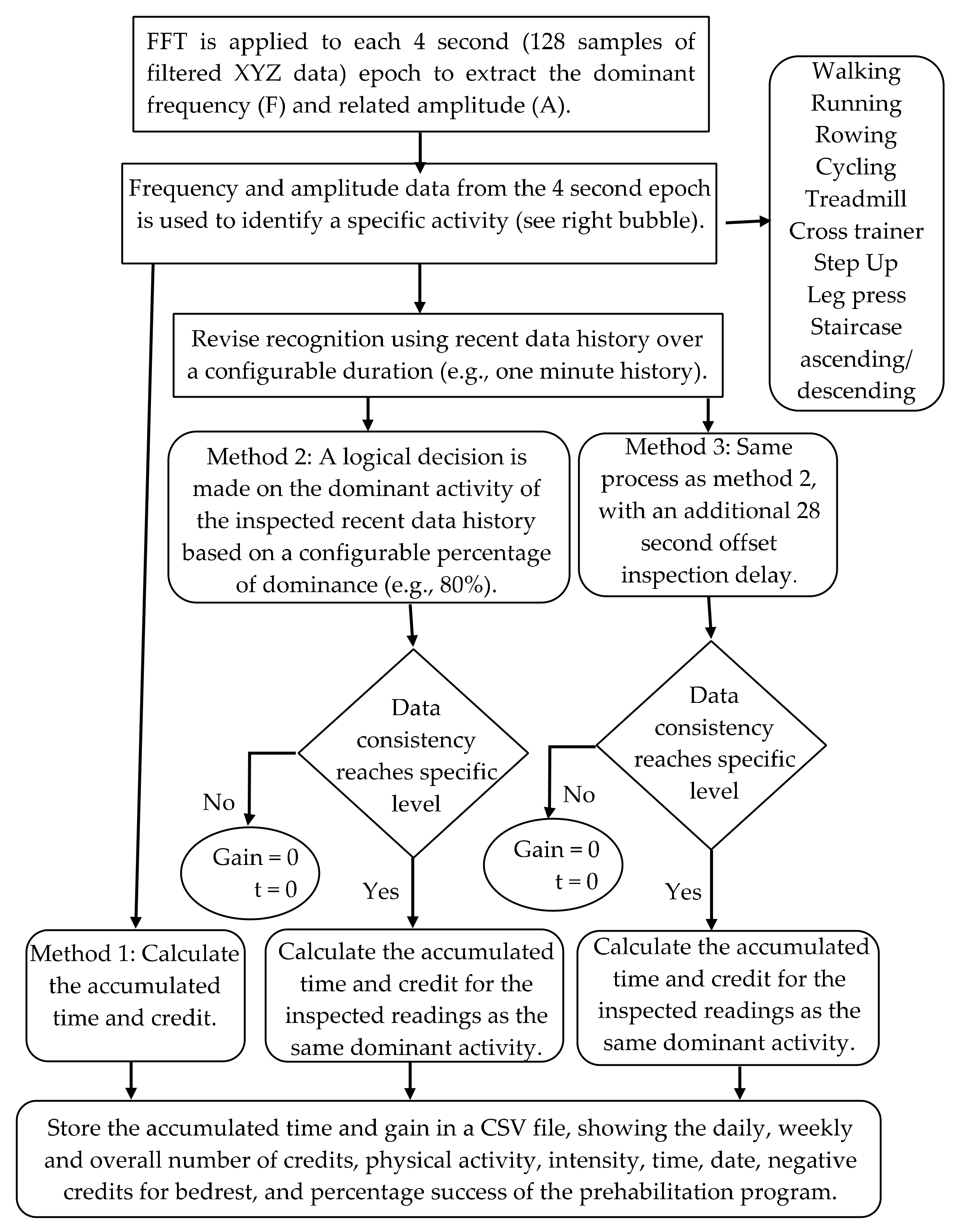
- is the duration of exercise, which is proportional to the standard unit time . Currently, the system considers and calculates each effort done by the patient regardless of meeting threshold time target (10 min at moderate intensity). This is because it is still unclear whether very short bursts exercise (less than 10 min) at a moderate or vigorous intensity should be discarded or not.
- represents the modality or type of prescribed physical exercise. At this stage of the model, all nine types of exercise are initially given the same value. The value for type of exercise is based on previous studies [8,18,30,31] where the patient must perform 150 min of moderate intensity exercise (e.g., 30 min of moderate physical activity five times per week) or equivalent per week, for a period of six weeks. In this example, the total volume of exercise over the six weeks (P) equates to a total of 30 credit points. The exercise intensity (I) would be 1 (moderate intensity), the time per session (De) would be 30 (30 min), and the minimal threshold for time (T) would be 10 min. Given that P, We, De and T are known, Equation (1) can be re-arranged to calculate (see formula below). This would result in being .
- is the total accumulated credits for the six weeks without considering bed rest.
- G is the total accumulated credits with bed rest.
4. Implementation of the Mixed Prehabilitation Model
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lawrence, V.A.; Hazuda, H.P.; Cornell, J.E.; Pederson, T.; Bradshaw, P.T.; Mulrow, C.D.; Page, C.P. Functional independence after major abdominal surgery in the elderly. J. Am. Coll. Surg. 2004, 199, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Teo, J.Y.; Turner, R.; Self, M. Effect of exercise prehabilitation on functional status of patients undergoing bowel resection: A systematic review. Anz J. Surg. 2020, 90, 693–701. [Google Scholar] [CrossRef]
- Nielsen, P.R.; Jørgensen, L.D.; Dahl, B.; Pedersen, T.; Tønnesen, H. Prehabilitation and early rehabilitation after spinal surgery: Randomized clinical trial. Clin. Rehabil. 2010, 24, 137–148. [Google Scholar] [CrossRef]
- Heldens, A.; Bongers, B.; de Vos-Geelen, J.; van Meeteren, N.; Lenssen, A. Feasibility and preliminary effectiveness of a physical exercise training program during neoadjuvant chemoradiotherapy in individual patients with rectal cancer prior to major elective surgery. Eur. J. Surg. Oncol. 2016, 42, 1322–1330. [Google Scholar] [CrossRef]
- Valkenet, K.; Trappenburg, J.C.; Schippers, C.C.; Wanders, L.; Lemmens, L.; Backx, F.J.; van Hillegersberg, R. Feasibility of exercise training in cancer patients scheduled for elective gastrointestinal surgery. Dig. Surg. 2016, 33, 439–447. [Google Scholar] [CrossRef]
- Jones, L.W.; Peddle, C.J.; Eves, N.D.; Haykowsky, M.J.; Courneya, K.S.; Mackey, J.R.; Joy, A.A.; Kumar, V.; Winton, T.W.; Reiman, T. Effects of presurgical exercise training on cardiorespiratory fitness among patients undergoing thoracic surgery for malignant lung lesions. Cancer 2007, 110, 590–598. [Google Scholar] [CrossRef]
- Peddle, C.J.; Jones, L.W.; Eves, N.D.; Reiman, T.; Sellar, C.M.; Winton, T.; Courneya, K.S. Effects of presurgical exercise training on quality of life in patients undergoing lung resection for suspected malignancy: A pilot study. Cancer Nurs. 2009, 32, 158–165. [Google Scholar] [CrossRef]
- Gillis, C.; Li, C.; Lee, L.; Awasthi, R.; Augustin, B.; Gamsa, A.; Liberman, A.S.; Stein, B.; Charlebois, P.; Feldman, L.S. Prehabilitation versus REHABILITATIONA randomized control trial in patients undergoing colorectal resection for cancer. Anesthesiol. J. Am. Soc. Anesthesiol. 2014, 121, 937–947. [Google Scholar]
- Sekine, Y.; Chiyo, M.; Iwata, T.; Yasufuku, K.; Furukawa, S.; Amada, Y.; Iyoda, A.; Shibuya, K.; Iizasa, T.; Fujisawa, T. Perioperative rehabilitation and physiotherapy for lung cancer patients with chronic obstructive pulmonary disease. Jpn. J. Thorac. Cardiovasc. Surg. 2005, 53, 237–243. [Google Scholar] [CrossRef]
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The impact of the COVID-19 pandemic on cancer care. Nat. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef]
- Sell, N.M.; Silver, J.K.; Rando, S.; Draviam, A.C.; Santa Mina, D.; Qadan, M. Prehabilitation Telemedicine in Neoadjuvant Surgical Oncology Patients During the Novel COVID-19 Coronavirus Pandemic. Ann. Surg. 2020, 272, e81. [Google Scholar] [CrossRef]
- Al-Naime, K.; Al-Anbuky, A.; Mawston, G. Human Movement Monitoring and Analysis for Prehabilitation Process Management. J. Sens. Actuator Netw. 2020, 9, 9. [Google Scholar] [CrossRef] [Green Version]
- Coker, R.H.; Hays, N.P.; Williams, R.H.; Wolfe, R.R.; Evans, W.J. Bed rest promotes reductions in walking speed, functional parameters, and aerobic fitness in older, healthy adults. J. Gerontol. Ser. A Biomed. Sci. Med Sci. 2015, 70, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floreani, M.; Rejc, E.; Taboga, P.; Ganzini, A.; Pišot, R.; Šimunič, B.; Biolo, G.; Reggiani, C.; Passaro, A.; Narici, M. Effects of 14 days of bed rest and following physical training on metabolic cost, mechanical work, and efficiency during walking in older and young healthy males. PLoS ONE 2018, 13, e0194291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLellan, A.; Slaght, J.; Craig, C.; Mayo, A.; Sénéchal, M.; Bouchard, D.R. Can older adults improve the identification of moderate intensity using walking cadence? Aging Clin. Exp. Res. 2018, 30, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Moran, J.; Guinan, E.; McCormick, P.; Larkin, J.; Mockler, D.; Hussey, J.; Moriarty, J.; Wilson, F. The ability of prehabilitation to influence postoperative outcome after intra-abdominal operation: A systematic review and meta-analysis. Surgery 2016, 160, 1189–1201. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Silver, J.K.; Feldman, L.S.; McKee, A.; Gilman, S.; Gillis, C.; Scheede-Bergdahl, C.; Gamsa, A.; Stout, N.; Hirsch, B. Surgical prehabilitation in patients with cancer: State-of-the-science and recommendations for future research from a panel of subject matter experts. Phys. Med. Rehabil. Clin. 2017, 28, 49–64. [Google Scholar] [CrossRef]
- Bousquet-Dion, G.; Awasthi, R.; Loiselle, S.-È.; Minnella, E.M.; Agnihotram, R.V.; Bergdahl, A.; Carli, F.; Scheede-Bergdahl, C. Evaluation of supervised multimodal prehabilitation programme in cancer patients undergoing colorectal resection: A randomized control trial. Acta Oncol. 2018, 57, 849–859. [Google Scholar] [CrossRef] [Green Version]
- Dronkers, J.; Lamberts, H.; Reutelingsperger, I.; Naber, R.; Dronkers-Landman, C.; Veldman, A.; van Meeteren, N. Preoperative therapeutic programme for elderly patients scheduled for elective abdominal oncological surgery: A randomized controlled pilot study. Clin. Rehabil. 2010, 24, 614–622. [Google Scholar] [CrossRef]
- Weggemans, R.M.; Backx, F.J.; Borghouts, L.; Chinapaw, M.; Hopman, M.T.; Koster, A.; Kremers, S.; van Loon, L.J.; May, A.; Mosterd, A. The 2017 Dutch physical activity guidelines. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 58. [Google Scholar] [CrossRef]
- Sparling, P.B.; Howard, B.J.; Dunstan, D.W.; Owen, N. Recommendations for physical activity in older adults. BMJ 2015, 350, h100. [Google Scholar] [CrossRef] [Green Version]
- Marshall, S.J.; Levy, S.S.; Tudor-Locke, C.E.; Kolkhorst, F.W.; Wooten, K.M.; Ji, M.; Macera, C.A.; Ainsworth, B.E. Translating physical activity recommendations into a pedometer-based step goal: 3000 steps in 30 minutes. Am. J. Prev. Med. 2009, 36, 410–415. [Google Scholar] [CrossRef]
- Palma, S.; Hasenoehrl, T.; Jordakieva, G.; Ramazanova, D.; Crevenna, R. High-intensity interval training in the prehabilitation of cancer patients—a systematic review and meta-analysis. Supportive Care Cancer 2020, 29, 1781–1794. [Google Scholar] [CrossRef]
- Purswani, J.M.; Ohri, N.; Champ, C. Tracking steps in oncology: The time is now. Cancer Manag. Res. 2018, 10, 2439. [Google Scholar] [CrossRef] [Green Version]
- Reidy, P.T.; McKenzie, A.I.; Brunker, P.; Nelson, D.S.; Barrows, K.M.; Supiano, M.; LaStayo, P.C.; Drummond, M.J. Neuromuscular electrical stimulation combined with protein ingestion preserves thigh muscle mass but not muscle function in healthy older adults during 5 days of bed rest. Rejuvenation Res. 2017, 20, 449–461. [Google Scholar] [CrossRef]
- Kortebein, P.; Symons, T.B.; Ferrando, A.; Paddon-Jones, D.; Ronsen, O.; Protas, E.; Conger, S.; Lombeida, J.; Wolfe, R.; Evans, W.J. Functional impact of 10 days of bed rest in healthy older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 1076–1081. [Google Scholar] [CrossRef] [Green Version]
- Rioux, B.V.; Sénéchal, M.; Kwok, K.; Fox, J.; Gamey, D.; Bharti, N.; Vergis, A.; Hardy, K.; Bouchard, D.R. Association between physical activity intensity and physical capacity among individuals awaiting bariatric surgery. Obes. Surg. 2017, 27, 1277–1283. [Google Scholar] [CrossRef]
- Medicine, A.C.o.S. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Whitfield, G.P.; Carlson, S.A.; Ussery, E.N.; Fulton, J.E.; Galuska, D.A.; Petersen, R. Trends in meeting physical activity guidelines among urban and rural dwelling adults—United States, 2008–2017. Morb. Mortal. Wkly. Rep. 2019, 68, 513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnohr, P.; Scharling, H.; Jensen, J.S. Intensity versus duration of walking, impact on mortality: The Copenhagen City Heart Study. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 72–78. [Google Scholar] [CrossRef]
- Godin, J.; Blodgett, J.M.; Rockwood, K.; Theou, O. Replacing Sedentary Time With Light or Moderate–Vigorous Physical Activity Across Levels of Frailty. J. Aging Phys. Act. 2020, 28, 18–23. [Google Scholar] [CrossRef]





| No. | Mode of Exercise | Intensity | Frequency (Hz) | Amplitude (m/s2) | Estimated Indicator for Measure of Intensity |
|---|---|---|---|---|---|
| 1 | Walking (W) | L | 1.5 | 15–32 | 4 km/h |
| M | 2 | 38–60 | 5 km/h | ||
| V | 2.25–2.5 | 45–75 | 6 km/h | ||
| 2 | Running (RU) | L | 3 | 55–70 | 8 km/h |
| M | 3.25 | 55–75 | 10 km/h | ||
| V | NA | NA | NA | ||
| 3 | Treadmill (TM) | L | 1.75 | 20–25 | 4.5 km/h |
| M | 2 | 45–55 | 5.5 km/h | ||
| V | 2.25 | 50–60 | 6.5 km/h | ||
| 4 | Cycling (C) | L | 0.75–1 | 20–30 | 50 rpm |
| M | 1–1.25 | 30–55 | 70 rpm | ||
| V | 1.25–1.5 | 40–80 | 90 rpm | ||
| 5 | Cross-trainer (CT) | L | 0.75-1 | 8–18 | 50 rpm |
| M | 1–1.25 | 20–28 | 70 rpm | ||
| V | 1.5 | 30–60 | 90 rpm | ||
| 6 | Rowing (RO) | L | 0.25 | 4–6 | 50 Watt |
| M | 0.5 | 11–15 | 70 Watt | ||
| V | 0.75 | 18–26 | 100 Watt | ||
| 7 | Staircase ascension STRM | L | 0.75 and 1.25 | 30–35 and 15–25 | No consistency in both F and A |
| Staircase descension | L | 0.75 and 1.5 | 20–30 and 15–25 | ||
| 8 | Step Ups (STP) | L | 1.5 | 14–18 | 15 cm height |
| M | 1.5 | 20–25 | 20 cm height | ||
| V | 1.75 | 22–26 | 30 cm height | ||
| 9 | Leg Press (LEP) | L | 0.25 | 5–6 | 90 kg, 20 times each session |
| M | 1–2 | 3–5 | 96 kg, 20 times each session | ||
| V | 0.5–3.75 | 0.5–5 | 115 kg, 20 times each session |
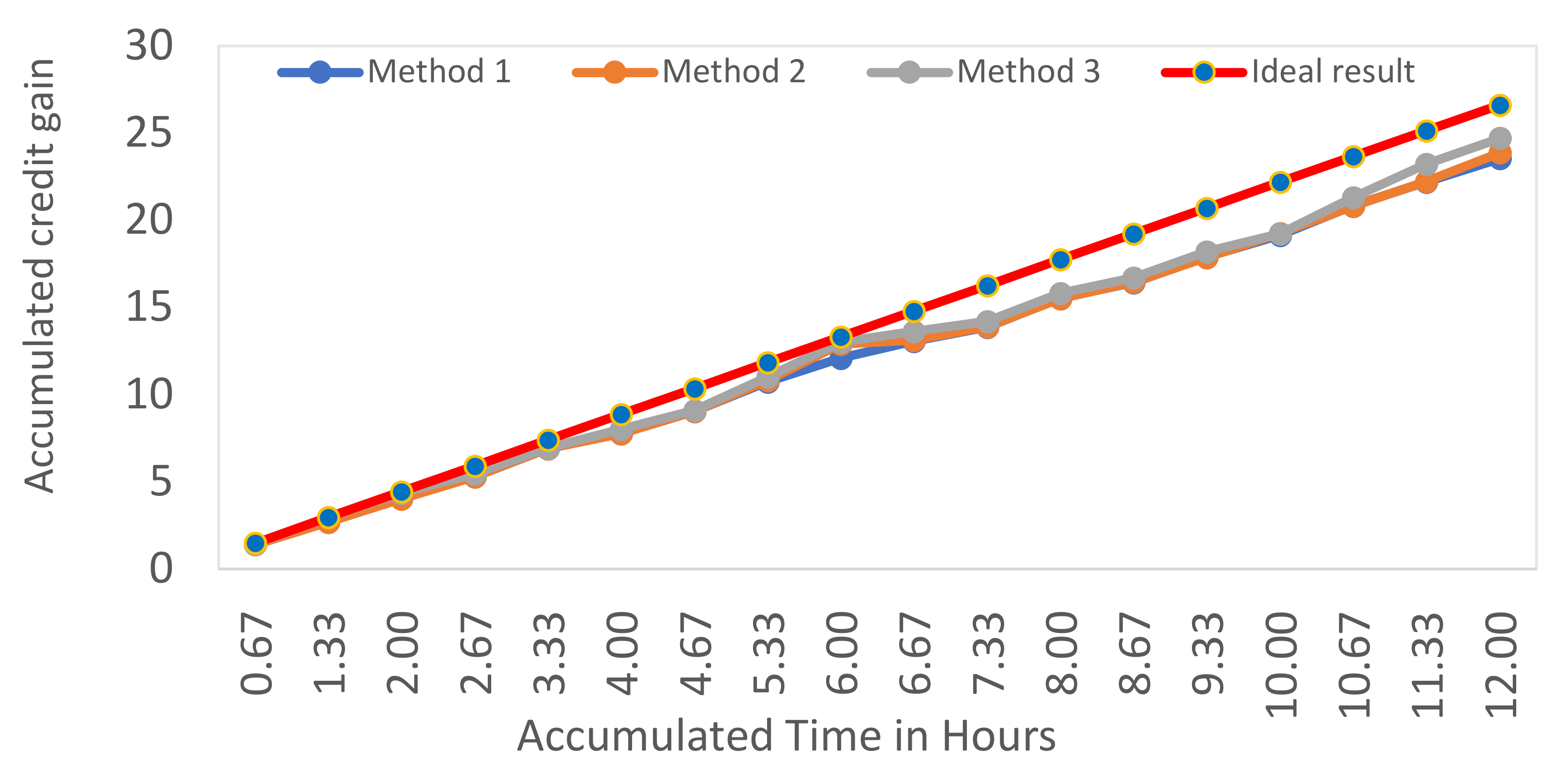
| Method Type | Total Gain Credit | Detected Time (min) | Percentage % |
|---|---|---|---|
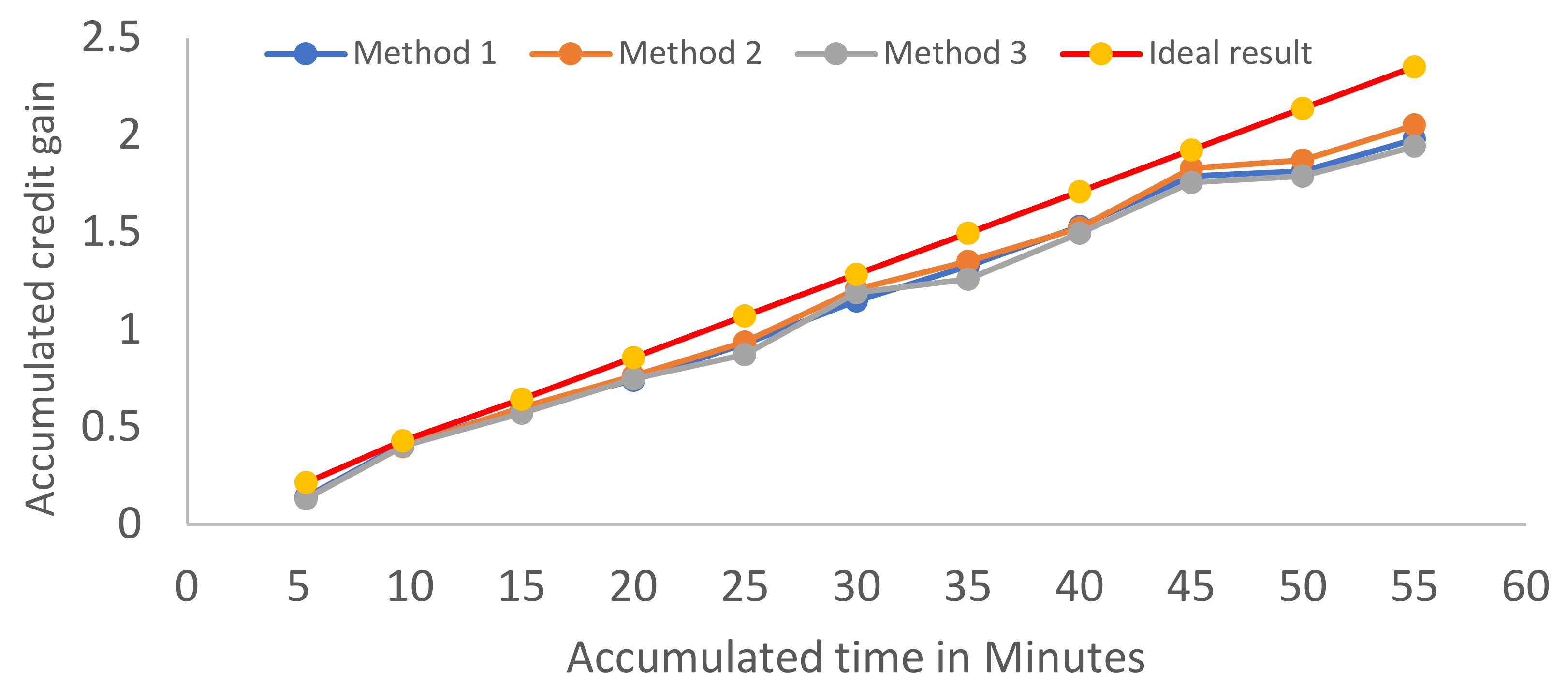
| Ideal | 2.351 | 55 | 100 |
| Method 1 | 1.9422 | 44.26 | 82 |
| Method 2 | 1.98 | 47 | 84 |
| Method 3 | 2.052 | 49 | 87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Naime, K.; Al-Anbuky, A.; Mawston, G. Remote Monitoring Model for the Preoperative Prehabilitation Program of Patients Requiring Abdominal Surgery. Future Internet 2021, 13, 104. https://doi.org/10.3390/fi13050104
Al-Naime K, Al-Anbuky A, Mawston G. Remote Monitoring Model for the Preoperative Prehabilitation Program of Patients Requiring Abdominal Surgery. Future Internet. 2021; 13(5):104. https://doi.org/10.3390/fi13050104
Chicago/Turabian StyleAl-Naime, Khalid, Adnan Al-Anbuky, and Grant Mawston. 2021. "Remote Monitoring Model for the Preoperative Prehabilitation Program of Patients Requiring Abdominal Surgery" Future Internet 13, no. 5: 104. https://doi.org/10.3390/fi13050104
APA StyleAl-Naime, K., Al-Anbuky, A., & Mawston, G. (2021). Remote Monitoring Model for the Preoperative Prehabilitation Program of Patients Requiring Abdominal Surgery. Future Internet, 13(5), 104. https://doi.org/10.3390/fi13050104