

Exploring the Utility of Autonomic Nervous System Evaluation for Stroke Prognosis
 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results
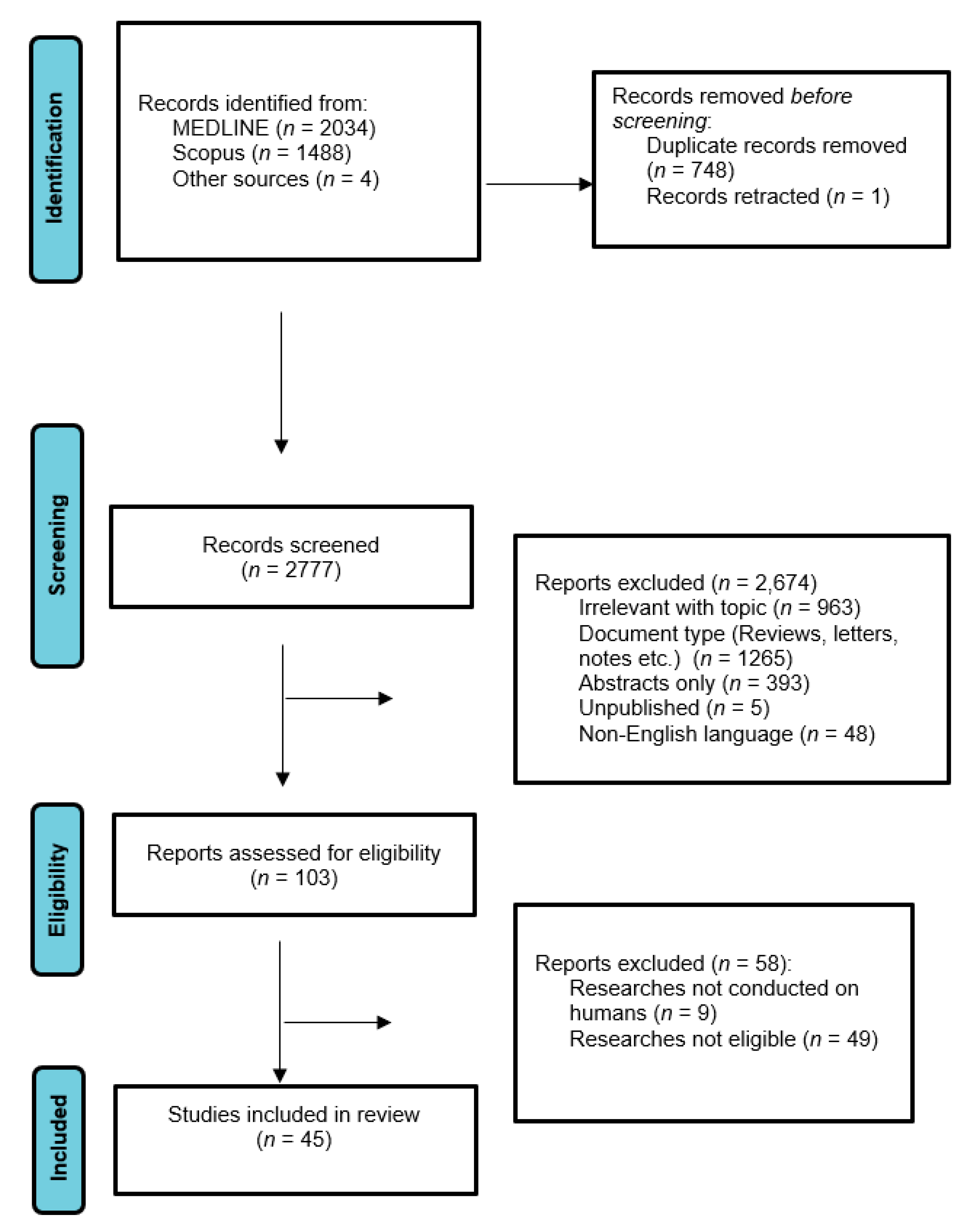
3.1. Database Searches
3.2. Study Characteristics
3.3. Stroke Patient Groups and Demographic Profile
3.4. Reference Groups
3.5. Time of Assessment
3.6. Scales of Stroke Severity and Prognosis/Clinical Outcome
4. Discussion
4.1. Early Neurological Deterioration (within 1st Week)
4.2. Early Stroke Outcome (<1 Month)
4.3. Short-Term Stroke Outcome (<3 Months)
4.4. Long-Term Stroke Outcome (<1 Year)
4.5. Chronic Stroke (>1 Year) Outcome
4.6. Depression Due to AIS
4.7. Immunosuppression Due to AIS
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aho, K.; Harmsen, P.; Hatano, S.; Marquardsen, J.; Smirnov, V.E.; Strasser, T. Cerebrovascular disease in the community: Results of a WHO collaborative study. Bull. World Health Organ. 1980, 58, 113–130. [Google Scholar] [PubMed]
- Al-Qudah, Z.A.; Yacoub, H.A.; Souayah, N. Disorders of the Autonomic Nervous System after Hemispheric Cerebrovascular Disorders: An Update. J. Vasc. Interv. Neurol. 2015, 8, 43–52. [Google Scholar] [PubMed]
- Christidi, F.; Tsiptsios, D.; Fotiadou, A.; Kitmeridou, S.; Karatzetzou, S.; Tsamakis, K.; Sousanidou, A.; Psatha, E.A.; Karavasilis, E.; Seimenis, I.; et al. Diffusion Tensor Imaging as a Prognostic Tool for Recovery in Acute and Hyperacute Stroke. Neurol. Int. 2022, 14, 841–874. [Google Scholar] [CrossRef]
- Christidi, F.; Tsiptsios, D.; Sousanidou, A.; Karamanidis, S.; Kitmeridou, S.; Karatzetzou, S.; Aitsidou, S.; Tsamakis, K.; Psatha, E.A.; Karavasilis, E.; et al. The Clinical Utility of Leukoaraiosis as a Prognostic Indicator in Ischemic Stroke Patients. Neurol. Int. 2022, 14, 952–980. [Google Scholar] [CrossRef] [PubMed]
- Karatzetzou, S.; Tsiptsios, D.; Terzoudi, A.; Aggeloussis, N.; Vadikolias, K. Transcranial magnetic stimulation implementation on stroke prognosis. Neurol. Sci. 2021, 43, 873–888. [Google Scholar] [CrossRef] [PubMed]
- Quinn, T.J.; Singh, S.; Lees, K.R.; Bath, P.M.; Myint, P.K.; VISTA Collaborators. Validating and comparing stroke prognosis scales. Neurology 2017, 89, 997–1002. [Google Scholar] [CrossRef]
- Gordan, R.; Gwathmey, J.K.; Xie, L.-H. Autonomic and endocrine control of cardiovascular function. World J. Cardiol. 2015, 7, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Xhyheri, B.; Manfrini, O.; Mazzolini, M.; Pizzi, C.; Bugiardini, R. Heart Rate Variability Today. Prog. Cardiovasc. Dis. 2012, 55, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Guzik, A.K.; Reeves, M.; Ovbiagele, B.; Johnston, S.C. Stroke Prognostication using Age and NIH Stroke Scale: SPAN-100. Neurology 2012, 80, 21–28. [Google Scholar] [CrossRef]
- Mendelowitz, D. Advances in Parasympathetic Control of Heart Rate and Cardiac Function. Physiology 1999, 14, 155–161. [Google Scholar] [CrossRef]
- Counsell, C.; Dennis, M.; McDowall, M. Predicting functional outcome in acute stroke: Comparison of a simple six variable model with other predictive systems and informal clinical prediction. J. Neurol. Neurosurg. Psychiatry 2004, 75, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Gkantzios, A.; Tsiptsios, D.; Karatzetzou, S.; Kitmeridou, S.; Karapepera, V.; Giannakou, E.; Vlotinou, P.; Aggelousis, N.; Vadikolias, K. Stroke and Emerging Blood Biomarkers: A Clinical Prospective. Neurol. Int. 2022, 14, 784–803. [Google Scholar] [CrossRef] [PubMed]
- Nayani, S.; Sreedharan, S.E.; Namboodiri, N.; Sarma, P.S.; Sylaja, P.N. Autonomic dysfunction in first ever ischemic stroke: Prevalence, predictors and short term neurovascular outcome. Clin. Neurol. Neurosurg. 2016, 150, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Dutsch, M.; Burger, M.; Dorfler, C.; Schwab, S.; Hilz, M.J. Cardiovascular autonomic function in poststroke patients. Neurology 2007, 69, 2249–2255. [Google Scholar] [CrossRef] [PubMed]
- Hilz, M.J.; Moeller, S.; Akhundova, A.; Marthol, H.; Pauli, E.; De Fina, P.; Schwab, S. High NIHSS Values Predict Impairment of Cardiovascular Autonomic Control. Stroke 2011, 42, 1528–1533. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Winstein, C. Can Neurological Biomarkers of Brain Impairment be Used to Predict Poststroke Motor Recovery? A Systematic Review. Neurorehabilit. Neural Repair 2017, 31, 3–24. [Google Scholar] [CrossRef]
- Buitrago-Ricaurte, N.; Cintra, F.; Silva, G.S. Heart rate variability as an autonomic biomarker in ischemic stroke. Arq. Neuropsiquiatr. 2020, 78, 724–732. [Google Scholar] [CrossRef]
- Li, C.; Meng, X.; Pan, Y.; Li, Z.; Wang, M.; Wang, Y. The Association Between Heart Rate Variability and 90-Day Prognosis in Patients with Transient Ischemic Attack and Minor Stroke. Front. Neurol. 2021, 12, 636474. [Google Scholar] [CrossRef]
- Cygankiewicz, I.; Zareba, W. Heart rate variability. Handb. Clin. Neurol. 2013, 117, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Karan, K.R.; Kirsch, R.E.; Hornik, C.P. Cardiovascular Physiology for Intensivists. In Critical Heart Disease in Infants and Children, 3rd ed.; Elsevier: Amsterdam, the Netherlands, 2018; pp. 111–133.e5. [Google Scholar] [CrossRef]
- Bonnemeier, H.; Wiegand, U.K.; Brandes, A.; Kluge, N.; Katus, H.A.; Richardt, G.; Potratz, J. Circadian Profile of Cardiac Autonomic Nervous Modulation in Healthy Subjects: Differing effects of aging and gender on heart rate variability. J. Cardiovasc. Electrophysiol. 2003, 14, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Leung, H.; Chen, X.Y.; Han, J.H.; Leung, T.W.; Soo, Y.; Wong, E.; Chan, A.; Lau, A.; Wong, K.S. Preliminary findings of the effects of autonomic dysfunction on functional outcome after acute ischemic stroke. Clin. Neurol. Neurosurg. 2012, 114, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Sethi, A.; Callaway, C.W.; Sejdić, E.; Terhorst, L.; Skidmore, E.R. Heart Rate Variability Is Associated with Motor Outcome 3-Months after Stroke. J. Stroke Cerebrovasc. Dis. 2016, 25, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Guan, L.; Collet, J.-P.; Wang, Y. Relationship between ischemic stroke locations, etiology subtypes, neurological outcomes, and autonomic cardiac function. Neurol. Res. 2020, 42, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Korpelainen, J.T.; Sotaniemi, K.A.; Huikuri, H.V.; Myllylä, V.V. Abnormal Heart Rate Variability as a Manifestation of Autonomic Dysfunction in Hemispheric Brain Infarction. Stroke 1996, 27, 2059–2063. [Google Scholar] [CrossRef] [PubMed]
- Colivicchi, F.; Bassi, A.; Santini, M.; Caltagirone, C. Cardiac Autonomic Derangement and Arrhythmias in Right-Sided Stroke With Insular Involvement. Stroke 2004, 35, 2094–2098. [Google Scholar] [CrossRef] [PubMed]
- Kerman, I.A. Organization of brain somatomotor-sympathetic circuits. Exp. Brain Res. 2008, 187, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.C.; Lin, H.C.; Lai, Y.R.; Hsu, C.W.; Huang, C.C.; Wang, H.C.; Su, C.M.; Su, Y.J.; Lin, W.C.; Cheng, B.C.; et al. The Effect of Stroke Subtypes on Baroreceptor Sensitivity, a Predict for Acute Stroke Outcome. Biomed. Res. Int. 2019, 2019, 7614828. [Google Scholar] [CrossRef]
- Lees, T.; Shad-Kaneez, F.; Simpson, A.M.; Nassif, N.T.; Lin, Y.; Lal, S. Heart Rate Variability as a Biomarker for Predicting Stroke, Post-stroke Complications and Functionality. Biomark. Insights 2018, 13, 1177271918786931. [Google Scholar] [CrossRef]
- Hung, C.-Y.; Tseng, S.-H.; Chen, S.-C.; Chiu, H.-C.; Lai, C.-H.; Kang, J.-H. Cardiac autonomic status is associated with spasticity in post-stroke patients. Neurorehabilitation 2014, 34, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Shimada, T.; Shindo, A.; Imai, H.; Momosaki, R.; Suzuki, H.; Tomimoto, H. Relationship between Neurological Deterioration and Blood Pressure/Heart Rate Variability in Patients with Acute Cerebral Infarction. J. Stroke Cerebrovasc. Dis. 2022, 31, 106504. [Google Scholar] [CrossRef] [PubMed]
- Mankoo, A.; Roy, S.; Davies, A.; Panerai, R.B.; Robinson, T.G.; Brassard, P.; Beishon, L.C.; Minhas, J.S. The role of the autonomic nervous system in cerebral blood flow regulation in stroke: A review. Auton. Neurosci. 2023, 246, 103082. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-H.; Yen, C.-C.; Hsu, Y.-T.; Chen, H.-H.; Cheng, P.-W.; Tseng, C.-J.; Lo, Y.-K.; Chan, J.Y. Baroreceptor Sensitivity Predicts Functional Outcome and Complications after Acute Ischemic Stroke. J. Clin. Med. 2019, 8, 300. [Google Scholar] [CrossRef]
- Chen, C.-F.; Lin, H.-F.; Lin, R.-T.; Yang, Y.-H.; Lai, C.-L. Relationship between ischemic stroke location and autonomic cardiac function. J. Clin. Neurosci. 2013, 20, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Han, B.; Xia, Y.; Liu, Y.; Wang, C.; Zhang, C. Augmentation of peripheral lymphocyte-derived cholinergic activity in patients with acute ischemic stroke. BMC Neurol. 2019, 19, 236. [Google Scholar] [CrossRef]
- Wang, H.; Yan, F.-L.; Cunningham, M.; Deng, Q.-W.; Zuo, L.; Xing, F.L.; Shi, L.-H.; Hu, S.-S.; Huang, Y. Potential specific immunological indicators for stroke associated infection are partly modulated by sympathetic pathway activation. Oncotarget 2016, 7, 52404–52415. [Google Scholar] [CrossRef] [PubMed]
- Brämer, D.; Hoyer, H.; Günther, A.; Nowack, S.; Brunkhorst, F.M.; Witte, O.W.; Hoyer, D. Study protocol: Prediction of stroke associated infections by markers of autonomic control. BMC Neurol. 2014, 14, 9. [Google Scholar] [CrossRef]
- Scheitz, J.F.; Sposato, L.A.; Schulz-Menger, J.; Nolte, C.H.; Backs, J.; Endres, M. Stroke–Heart Syndrome: Recent Advances and Challenges. J. Am. Hear. Assoc. 2022, 11, e026528. [Google Scholar] [CrossRef]
- Mehra, R.; Tjurmina, O.A.; Ajijola, O.A.; Arora, R.; Bolser, D.C.; Chapleau, M.W.; Chen, P.-S.; Clancy, C.E.; Delisle, B.P.; Gold, M.R.; et al. Research Opportunities in Autonomic Neural Mechanisms of Cardiopulmonary Regulation: A Report From the National Heart, Lung, and Blood Institute and the National Institutes of Health Office of the Director Workshop. JACC Basic Transl. Sci. 2022, 7, 265–293. [Google Scholar] [CrossRef]
- Goldberger, J.J.; Arora, R.; Buckley, U.; Shivkumar, K. Autonomic Nervous System Dysfunction: JACC Focus Seminar. J. Am. Coll. Cardiol. 2019, 73, 1189–1206. [Google Scholar] [CrossRef]
- Mo, J.; Huang, L.; Peng, J.; Ocak, U.; Zhang, J.; Zhang, J.H. Autonomic Disturbances in Acute Cerebrovascular Disease. Neurosci. Bull. 2019, 35, 133–144. [Google Scholar] [CrossRef]
- He, L.; Wang, J.; Zhang, L.; Wang, F.; Dong, W.; Yang, H. Admission Heart Rate Variability Is Associated with Poststroke Depression in Patients With Acute Mild-Moderate Ischemic Stroke. Front. Psychiatry 2020, 11, 696. [Google Scholar] [CrossRef] [PubMed]
- Tessier, A.; Sibon, I.; Poli, M.; Audiffren, M.; Allard, M.; Pfeuty, M. Resting Heart Rate Predicts Depression and Cognition Early after Ischemic Stroke: A Pilot Study. J. Stroke Cerebrovasc. Dis. 2017, 26, 2435–2441. [Google Scholar] [CrossRef] [PubMed]
- Sgoifo, A.; Carnevali, L.; de los Angeles Pico Alfonso, M.; Amore, M. Autonomic dysfunction and heart rate variability in depression. Stress 2015, 18, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Zhang, C.; You, S.; Zheng, D.; Zhong, C.; Dong, H.; Wang, X.; Pei, S.; Cao, Y.; Liu, C.-F. Resting Heart Rate and In-Hospital Mortality in Acute Ischemic Stroke Patients with and Without Atrial Fibrillation. Circ. J. 2020, 84, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Vistisen, S.T.; Hansen, T.K.; Jensen, J.; Nielsen, J.F.; Fleischer, J. Heart rate variability in neurorehabilitation patients with severe acquired brain injury. Brain Inj. 2014, 28, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.-L.; Kuo, T.B.J.; Yang, C.C.H. Parasympathetic activity correlates with early outcome in patients with large artery atherosclerotic stroke. J. Neurol. Sci. 2012, 314, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Bin Wu, B.; Liu, L.; Tang, X.; Yi, Z.; Zeng, L.; Jing, K.; Pan, C. Variability of blood pressure response to orthostatism and reproducibility of orthostatic hypotension in hospitalized patients with acute ischemic stroke. Blood Press. Monit. 2023, 28, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Usui, H.; Nishida, Y. Relationship between Physical Activity and the Very Low-Frequency Component of Heart Rate Variability after Stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 840–843. [Google Scholar] [CrossRef] [PubMed]
- Park, E.J.; Yoo, S.D. Nutritional Biomarkers and Heart Rate Variability in Patients with Subacute Stroke. Nutrients 2022, 14, 5320. [Google Scholar] [CrossRef]
- Heinz, G.; De Angelis, K.; Corso, S.D.; De Sousa, M.H.G.; Viana, A.; Dos Santos, F.; Corrêa, J.C.F.; Corrêa, F.I. Effects of Transcranial Direct Current Stimulation (tDCS) and Exercises Treadmill on Autonomic Modulation of Hemiparetic Patients Due To Stroke—Clinic Test, Controlled, Randomized, Double-Blind. Front. Neurol. 2020, 10, 1402. [Google Scholar] [CrossRef]
- Huang, J.-C.; Chen, C.-F.; Chang, C.-C.; Chen, S.-C.; Hsieh, M.-C.; Hsieh, Y.-P.; Chen, H.-C. Effects of stroke on changes in heart rate variability during hemodialysis. BMC Nephrol. 2017, 18, 90. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Tian, G.; Wang, L.; Lin, W.; Chen, X.; Leung, T.W.H.; Soo, Y.O.Y.; Wong, L.K.S. External Counterpulsation Increases Beat-to-Beat Heart Rate Variability in Patients with Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.-H.; Wang, X.-D.; Yang, J.-J.; Zhou, L.; Pan, Y.-C. Changes of deceleration and acceleration capacity of heart rate in patients with acute hemispheric ischemic stroke. Clin. Interv. Aging 2016, 11, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Chidambaram, H.; Gnanamoorthy, K.; Suthakaran, P.K.; Rajendran, K.; Pavadai, C. Assessment of Autonomic Dysfunction in Acute Stroke Patients at a Tertiary Care Hospital. J. Clin. Diagn. Res. 2017, 11, OC28–OC31. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.-R.; Lin, Y.-J.; Shih, F.-Y.; Wang, H.-C.; Tsai, N.-W.; Kung, C.-T.; Lin, W.-C.; Cheng, B.-C.; Su, Y.-J.; Chang, Y.-T.; et al. Effect of Baroreceptor Sensitivity on Outcomes in Patients with Acute Spontaneous Intracerebral Hemorrhage. World Neurosurg. 2018, 109, e754–e760. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, X.; Liu, H.; Zhang, G.; Xing, C. Can Heart Rate Variability Parameters Be a Biomarker for Predicting Motor Function Prognosis in Patients with Chronic Stroke? In Health Information Science. HIS 2019; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2019; pp. 98–107. [Google Scholar] [CrossRef]
- Graff, B.; Gasecki, D.; Rojek, A.; Boutouyrie, P.; Nyka, W.; Laurent, S.; Narkiewicz, K. Heart rate variability and functional outcome in ischemic stroke: A Multiparameter Approach. J. Hypertens. 2013, 31, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Szabo, J.; Smielewski, P.; Czosnyka, M.; Jakubicek, S.; Krebs, S.; Siarnik, P.; Sykora, M. Heart rate variability is associated with outcome in spontaneous intracerebral hemorrhage. J. Crit. Care 2018, 48, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Tobaldini, E.; Sacco, R.M.; Serafino, S.; Tassi, M.; Gallone, G.; Solbiati, M.; Costantino, G.; Montano, N.; Torgano, G. Cardiac Autonomic Derangement Is Associated with Worse Neurological Outcome in the Very Early Phases of Ischemic Stroke. J. Clin. Med. 2019, 8, 852. [Google Scholar] [CrossRef]
- Miwa, K.; Koga, M.; Fukuda-Doi, M.; Yamamoto, H.; Tanaka, K.; Yoshimura, S.; Ihara, M.; Qureshi, A.I.; Toyoda, K. Effect of Heart Rate Variabilities on Outcome after Acute Intracerebral Hemorrhage: A Post Hoc Analysis of ATACH-2. J. Am. Hear. Assoc. 2021, 10, e020364. [Google Scholar] [CrossRef]
- Jeong, H.-G.; Ko, S.-B.; Kim, C.K.; Kim, Y.; Jung, S.; Kim, T.J.; Yoon, B.-W. Tachycardia burden in stroke unit is associated with functional outcome after ischemic stroke. Int. J. Stroke 2016, 11, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Tian, G.; Leung, H.; Soo, Y.O.; Chen, X.; Ip, V.H.; Mok, V.C.; Chu, W.C.; Wong, K.S.; Leung, T.W. Autonomic Dysfunction Predicts Clinical Outcomes after Acute Ischemic Stroke. Stroke 2018, 49, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.-L.; Lee, J.-T.; Li, C.-R.; Davis, A.H.T.; Yang, C.-C.; Chen, Y.-J. Effects of Heart Rate Variability Biofeedback in Patients with Acute Ischemic Stroke: A Randomized Controlled Trial. Biol. Res. Nurs. 2020, 22, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Xiong, L.; Fan, Y.; Mok, V.C.; Wong, K.S.; Leung, T.W. Stroke Outcome Prediction by Blood Pressure Variability, Heart Rate Variability, and Baroreflex Sensitivity. Stroke 2020, 51, 1317–1320. [Google Scholar] [CrossRef] [PubMed]
- Constantinescu, V.; Matei, D.; Costache, V.; Cuciureanu, D.; Arsenescu-Georgescu, C. Linear and nonlinear parameters of heart rate variability in ischemic stroke patients. Neurol. Neurochir. Polska 2018, 52, 194–206. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Wang, J.; Zhang, L.; Zhang, X.; Dong, W.; Yang, H. Decreased fractal dimension of heart rate variability is associated with early neurological deterioration and recurrent ischemic stroke after acute ischemic stroke. J. Neurol. Sci. 2019, 396, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Tian, G.; Leung, H.W.; Chen, X.Y.; Lin, W.H.; Leung, T.W.; Soo, Y.O.; Siu, D.Y.W.; Wong, L.K.S. Autonomic dysfunction as measured by Ewing battery test to predict poor outcome after acute ischaemic stroke. Hong Kong Med. J. 2019, 25, 9–11. [Google Scholar]
- Wang, Y.; Wang, J.; Meng, P.; Liu, N.; Ji, N.; Zhang, G.; Xu, B.; Zhou, X.; Sun, Y.; Xu, Y.; et al. Mid-Term Blood Pressure Variability Is Associated with Clinical Outcome after Ischemic Stroke. Am. J. Hypertens. 2017, 30, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Sandset, E.C.; Berge, E.; Kjeldsen, S.E.; Julius, S.; Holzhauer, B.; Krarup, L.-H.; Hua, T.A. Heart Rate as a Predictor of Stroke in High-risk, Hypertensive Patients with Previous Stroke or Transient Ischemic Attack. J. Stroke Cerebrovasc. Dis. 2014, 23, 2814–2818. [Google Scholar] [CrossRef] [PubMed]
- Abry, P.; Wendt, H.; Kiyono, K.; Yamamoto, Y.; Watanabe, E.; Hayano, J.; Leonarduzzi, R. Scattering Transform of Heart Rate Variability for the Prediction of Ischemic Stroke in Patients with Atrial Fibrillation. Methods Inf. Med. 2018, 57, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.K.; Aarotale, P.N.; Dehkordi, P.; Lou, J.-S.; Tavakolian, K. Relationship between Ischemic Stroke and Pulse Rate Variability as a Surrogate of Heart Rate Variability. Brain Sci. 2019, 9, 162. [Google Scholar] [CrossRef]
- Webb, A.J.; Mazzucco, S.; Li, L.; Rothwell, P.M. Prognostic Significance of Blood Pressure Variability on Beat-to-Beat Monitoring After Transient Ischemic Attack and Stroke. Stroke 2018, 49, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, K.; Di Tullio, M.R.; Qian, M.; Thompson, J.L.; Labovitz, A.J.; Mann, D.L.; Sacco, R.L.; Pullicino, P.M.; Freudenberger, R.S.; Teerlink, J.R.; et al. Resting Heart Rate and Ischemic Stroke in Patients with Heart Failure. Cerebrovasc. Dis. 2017, 44, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Eng, J.J.; Krassioukov, A. Application of the Sit-Up Test for orthostatic hypotension in individuals with stroke. Auton. Neurosci. 2012, 168, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Bodapati, R.K.; Kizer, J.R.; Kop, W.J.; Kamel, H.; Stein, P.K. Addition of 24-Hour Heart Rate Variability Parameters to the Cardiovascular Health Study Stroke Risk Score and Prediction of Incident Stroke: The Cardiovascular Health Study. J. Am. Heart Assoc. 2017, 6, e004305. [Google Scholar] [CrossRef]
- Idiaquez, J.; Farias, H.; Torres, F.; Vega, J.; Low, D.A. Autonomic symptoms in hypertensive patients with post-acute minor ischemic stroke. Clin. Neurol. Neurosurg. 2015, 139, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Brämer, D.; Günther, A.; Rupprecht, S.; Nowack, S.; Adam, J.; Meyer, F.; Schwab, M.; Surber, R.; Witte, O.W.; Hoyer, H.; et al. Very Low Frequency Heart Rate Variability Predicts the Development of Post-Stroke Infections. Transl. Stroke Res. 2019, 10, 607–619. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors, Year of Publication | Type of Study | Biomarker | Type of Stroke | Number of Participants/Mean Age (y)/Gender (M/F) | Medication (n) | Comorbidities/Risk Factors (n) | Previous Stroke | Follow-Up Time | Time of Assessment | Scale of Stroke Severity and Prognosis/Clinical Outcome | Main Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Early Neurological Deterioration (within 1st week) | |||||||||||
| Shimada et al., 2022 [31] | Longitudinal | BP, HR | IS | 135/72.6 ± 12.5 95M/40F | - | Hypertension (15) Atrial fibrillation (15) Dyslipidemia (32) Diabetes mellitus (32) | NM | Until discharge | On admission | NIHSS (at onset) Barthel index | The fluctuation of the vital index up until the moment of transfer may be used to predict neurological deterioration following transfer to a wheelchair, which may result in a lengthy hospital stay. |
| Han et al., 2020 [45] | Longitudinal | HRV | AIS | 3447/68.6 ± 12.9 1991M/1.456F | Antihypertensive therapy (2014) Antiplatelet therapy (252) Anticoagulation therapy (37) Antiglycemic therapy (649) Statin therapy (104) Thrombolysis treatment (85) | Hypertension (2700) Diabetes mellitus (892) Coronary artery disease (193) Atrial fibrillation (532) | 772 | Until discharge | <7 days from onset | NIHSS (at baseline) | In AIS patients without AF, higher RHR at admission was independently related to in-hospital mortality. |
| Vistisen et al., 2014 [46] | Longitudinal | HRV | ABI | Patients; 49/52.7 ± (15.9 27M/22F Control; 49/52.6 ± 13.7 25M/24F | Calcium antagonists (14) Beta-blockers (6) ACE inhibitors (4) Antihypertensive drug (3) Amiodarone (3) | Type 1 diabetes (2) Type 2 diabetes (1) | - | Until discharge | 6 pm and 10 pm on the admission day, as well as 2 am and 6, am the following day | Functional Independence Measure (FIM) Rancho Los Amigos Scale (RLAS) | In a sample of heterogenic ABI patients admitted for neurorehabilitation, HRV was significantly decreased. |
| Chen et al., 2011 [47] | Longitudinal | HRV | IS (LAA and LAC) | Patients; 50/64.2 ± 11.8 27M/23F Control; 19/66.1 ± 8.5 7M/12F | Calcium channel blockers (P. 7/C. 2) ACEI or ARB (P. 3/C. 3) Other BP-lowering medication (P. 5/C. 0) | Smoking (P. 18/C. 3) Diabetes (P. 16/C. 7) Hypertension (P. 37/C. 15) Hyperlipidemia (P. 38/C. 14) | - | 7 days after admission | Within 48 h after stroke onset | NIHSS (at baseline and on the 7th day) | Patients in the LAA group showed lower parasympathetic activity than those in the LAC group, although they had more sympathetic activity. Depressed parasympathetic activity was linked to a higher probability of poorer early outcomes in the LAA group. |
| Huang et al., 2023 [48] | Cross-sectional | BPRO | AIS | 211/62.8 ± 10.8 136M/75F | CCB (114) ACEI (5) ARB (27) α-blockers (7) Beta-blockers (8) Diuretics (10) | Smoking (73) Alcohol (39) Hypertension (137) Diabetes (55) Coronary artery disease (16) Atrial fibrillation (5) Hyperlipemia (103) Hyperhomocysteinemia (66) | 27 | 5 days | On admission | NIHSS | In hospitalized AIS patients, the repeatability of OH is low, and the simultaneous occurrence of OH and OHTN is frequent. |
| Usui H. and Nishida Y. et al., 2015 [49] | Longitudinal | HRV | IS | 12/67.7 ± 14.8 7M/5F | - | - | NM | Until discharge | 2–4 months after stroke | - | The VLF component of HRV and PA were found to be positively correlated in stroke patients. |
| Park et al., 2022 [50] | Cross-sectional | HRV | IS, HS | 426/67.03 ± 13.03 197M/229F | Beta-blockers (87) Calcium channel blocker (193) ACEI/ARB (199) Diuretics (228) | Hypertension (260) Arrhythmia (74) Diabetes mellitus (158) Dyslipidemia (325) Coronary artery disease (22) Heart failure (70) | - | Until discharge | Within three months of onset | Mini-Mental State Examination | Blood levels of transferrin, prealbumin, and albumin were linked to ANS function as determined by HRV, and their deficit may be a determinant of how severe ANS dysfunction is in stroke patients. |
| Heinz et al., 2020 [51] | Cross-sectional | HRV, VSBP | IS, HS | 12/59 ± 7.00 8M/4F | Beta-blockers (6) Diuretics (2) Calcium channel blockers (3) ECA inhibitors (2) ARB (6) Diabetes T2 medication (3) Medication for cholesterol (3) Medication for arthrosis (1) Medication for spasticity (1) | Diabetes (3) Hypertension (10) Positive HIV (1) High cholesterol levels (3) | NM | Until discharge | First day of treatment | Fugl-Meyer lower limb scale | Except for intragroup comparison, which shows increased engagement in parasympathetic modulation in the group receiving active TtDCS, the treatment has no immediate impact on HRV and VSBP. |
| Huang et al., 2017 [52] | Cross-sectional | HRV | IS, HS | Patients; 30/65.3 ± 8.4 12M/18F Control; 152/60.4 ± 11.7 69M/83F | Beta–blockers (P. 7/C. 25) Calcium channel blockers (P. 6/C. 30) ACEI or ARB (P. 4/C. 26) | Smoking (P. 3/C. 5) Diabetes mellitus (P. 26/C. 58) Hypertension (P. 25/C. 89) Coronary artery disease (P. 22/C. 28) | 30 | Until discharge | Before hemodialysis | - | During hemodialysis, there may be suppressed autonomic nervous reactions against volume unloading, which may worsen outcomes for hemodialysis patients and those who have had a stroke in the past. |
| Xiong et al., 2017 [53] | Longitudinal | HRV | IS | Patients; 48/64.69 ± 11.26 43M/5F Control; 14/59.36 ± 2.24 6M/8F | - | Hypertension (P. 10/C. 0) Diabetes (P. 21/C. 0) Hyperlipidemia (P. 29/C. 0) Smoking (P. 27/C. 0) Alcohol (P. 8/C. 0) Ischemic heart disease (P. 3/C. 0) Large artery disease (P. 39/C. NA) Small vessel disease (P. 9/C. NA) | 13 | Until discharge | Within 14 days of stroke onset | NIHSS (on admission) | Patients displayed an elevated beat-to-beat HRV following ECP, irrespective of the side of the ischemia. Moreover, after ECP in patients with right-sided subacute stroke, sympathetic and parasympathetic cardiac modulations increased. |
| Xu et al., 2016 [54] | Longitudinal | HR | AHIS | Patients: 63/71 ± 12 38M/25F Control: 50/68 ± 11 24M/25F | - | Hyperlipidemia (C.16/P. 18) Diabetes mellitus (C. 12/P. 21) Hypertension (C. 35/P. 50) Smoking (P. 27/C. 20) Alcohol (P. 4/C. 5) | - | Until discharge | Within 72 h after stroke | NIHSS (72 h after stroke) | In individuals with hemispheric infarction, both the DC and AC heart rate reduced, showing a reduction in both vagal and sympathetic regulation. The severity of the stroke was correlated with both DC and AC. |
| Early Stroke Outcome (<1 Month) | |||||||||||
| Chidambaram et al., 2017 [55] | Longitudinal | HRV | IS/HS | 97/60.84 ± 14.12 56M/41F | - | - | - | 30 days | On admission | NIHSS (on admission and on the 30th day) | Patients with autonomic dysfunction also had higher blood pressure readings and increased morbidity and death during the acute phase of stroke. |
| Tsai et al., 2019 [28] | Longitudinal | HRV | AIS | Patients; 34/63.2 ± 8.7 26M/12F Control; 18/59.6 ± 7.8 11M/7F | - | Hypertension (26) Diabetes mellitus (19) Dyslipidemia (23) Coronary artery diseases (2) | NM | 1 month | Upon enrollment | NIHSS (on admission) | Patients who have brainstem or big hemisphere infarction show greater blunting BRS than those who have lacunar infarction, which might help identify patients who may be at risk for poor outcomes. |
| Lai et al., 2015 [56] | Longitudinal | BRS | ICH | Patients; 35/59.60 ± 13.47 25M/10F Control; 30/59.87 ± 6.52 20M/10F | - | Hypertension (26) Diabetes mellitus (7) Coronary artery disease (2) Hyperlipidemia (3) Smoking (6) Alcohol (4) Coagulopathy (1) | - | 30 days | Upon enrollment | mRS (at 30 days) | BRS value at admission is a more accurate indicator of outcome than the admission Glasgow coma score. |
| Short-Term Stroke Outcome (<3 Months) | |||||||||||
| Sethi et al., 2015 [23] | Longitudinal | HRV | IS, HS | 13/61 ± 12 7M/6F | Beta-blockers (3) Calcium channel blocker (4) | Hypertension (6) Kidney stones (1) Pneumonia (1) Stomach ulcers (1) Type 2 diabetes mellitus (3) Hypercholesterolemia (1) Tubal ligation (1) Hyperlipidemia (2) Hyperthyroidism (1) Hypothyroidism (2) Secundum atrial septal defect (1) Four-vessel bypass (1) Appendectomy (1) Hysterectomy (1) Rheumatoid arthritis (1) | - | 3 months | Upon admission | NIHSS (at baseline) | A promising measure to investigate the mechanisms underlying motor recovery after stroke is HRV, which has a good correlation with motor outcome after stroke. |
| Zhang et al., 2019 [57] | Longitudinal | HRV | IS, HS | 64/59.05 ± 10.76 45M/19F | - | Hypertension (51) Diabetes (31) Coronary heart disease (15) Hyperlipidemia (45) Smoking (33) | - | 3 months | 1–3 months after stroke onset | - | There was no association between HRV values and the improvement in activities of daily living for stroke patients during the chronic rehabilitation phase, although there was a strong correlation between HRV parameters and the restoration of motor function. |
| Graff et al., 2013 [58] | Longitudinal | HRV, BP, RR | IS | 63/62 (30–87) 44M/19F | - | - | NM | 90 days | Within first 7 days after the onset of stroke symptoms | NIHSS (at baseline and on the 7th day) mRS (on the 7th and 90th day) | In the acute period of ischemic stroke, HRV measurements, but not blood pressure variability, distinguish groups with varied neurological outcomes. Second, in the immediate phase of ischemic stroke, a quicker respiratory rate is linked to a worse functional prognosis. |
| Szabo et al., 2018 [59] | Longitudinal | HRV | ICH | 47/60.8 ± 16.5 27M/20F | Beta-blockers (7) ACEI or AT (15) Calcium antagonists (6) | Hypertension (35) Amyloid angiopathy (4) Arteriovenous malformation (5) Coagulopathy (3) | - | 3 months | Within 24 h after stroke onset | NIHSS (on admission and at 10 days) mRS (at 3 months) | Autonomic changes appear to be present in acute ICH and are independently linked to poor outcome. |
| Tobaldini et al., 2019 [60] | Longitudinal | HRV | AIS | 41/68.0 ± 12.8 28M/13F | Beta-blockers (12) | Hypercholesterolemia (21) Hypertension (28) Diabetes mellitus (9) Heart failure (3) History of atrial fibrillation or flutter (3) Smoking (12) | 15 | 3 months | At the time of presentation in the emergency department | NIHSS (at the onset) mRS (3 months after stroke onset) | In the very initial stages of AIS, a loss of sympathetic oscillation may be reflected by a decreased 0V% and an elevated 2UV%, which may indicate a worse 3-month outcome. |
| Miwa et al., 2018 [61] | Longitudinal | HRV | ICH | 994/62 615M/379F | Antihypertensives (490) | Hypertension (788) Atrial fibrillation (35) Ischemic heart disease (43) Dyslipidemia (240) | 164 | 3 months | During the initial 24 h post-randomization | NIHSS (at baseline) mRS (at 90 days after randomization) | Throughout the first 24 h, increased mean HR and HR-ARV were independently linked to a poor prognosis in acute ICH. At 24 h, HR-ARV was linked to hematoma growth. |
| Jeong et al., 2016 [62] | Longitudinal | HR | AIS | 246/67.4 ± 12.8 132M/114F | Thrombolytic treatment (21) | Hypertension (179) Diabetes mellitus (74) Atrial fibrillation (57) Hyperlipidemia (78) Smoking (72) | 72 | 3 months | 7 days after onset | NIHSS (on admission) mRS (3 months after stroke) | Individuals who experience more tachycardia throughout their stay in the stroke unit have poorer functional outcomes. |
| Xiong et al., 2018 [63] | Longitudinal | Autonomic function (Ewing Battery) | IS | 150/66.4 ± 9.9 106M/44F | Beta-blockers (26) Calcium-channel blocker (79) Antiplatelet (132) HMG-CoA reductase inhibitor (124) | Hypertension (93) Diabetes mellitus (51) Ischemic heart disease (15) Hyperlipidemia (65) Smoking (64) Alcohol (34) | 34 | 3 months | Within 7 days of stroke symptom onset | NIHSS (on admission) mRS (3 months after stroke onset) Barthel index | Poor functional prognosis following acute ischemic stroke is predicted by autonomic dysfunction as measured by the Ewing battery. |
| Xiong et al., 2011 [22] | Longitudinal | HRV, HA1c | IS | 34/71.7 ± 8.7 23M/11F | - | Hypertension (28) Diabetes (17) Hyperlipidemia (18) Ischemic heart disease (18) Smoking (9) Alcohol (7) | 14 | 2 months | Within 7 days after onset | NIHSS (on admission) mRS (on admission) Barthel index | In individuals with acute ischemic stroke, relatively substantial autonomic dysfunction is associated with a poor functional prognosis. |
| Chang et al., 2019 [64] | Longitudinal | HRVBF | IS | Patients; 19/67.6 ± 11.4 10M/9F Control; 16/67.2 ± 7.6 8M/8F | Beta-blockers (P. 2 /C. 3) Calcium channel blockers (P. 1/C. 1) | Hypertension (P. 13/C. 8) Diabetes (P. 9/C. 8) Heart disease (P. 7/C. 5) | - | 3 months | On admission | NIHSS (on admission) | HRVBF is a potentially effective treatment for AIS patients’ autonomic dysfunction, cognitive decline, and psychological suffering. |
| Tang et al., 2020 [65] | Longitudinal | BPV, HRV, BRS | IS | 142/63.9 ± 10.2 125M/17F | Antihypertensives (93) Antiplatelet (139) ARB (43) ACEI (17) Beta-blockers (20) Calcium channel blockers (36) Diuretics (4) Statin (132) | Hypertension (101) Diabetes mellitus (51) Hyperlipidemia (61) Smoking (79) Alcohol (37) | 38 | 3 months | Within 7 days of an ischemic stroke | NIHSS (on admission) mRS (on admission and at 3 months) | In addition to the well-established predictive variables such as the National Institutes of Health Stroke Scale, a decreased low/high-frequency ratio of systolic BPV and impaired baroreflex sensitivity indicated an unfavorable stroke outcome. |
| Constantinescu et al., 2017 [66] | Longitudinal | HRV | IS | Right MCA IS 15/59.7 ± 10.3 8M/7F Left MCA IS 15/59.4 ± 8.43 7M/8F | - | Hypertension (25) | - | 3 months | Within 6 months post-stroke | mRS (3 months after stroke onset) | In stroke patients, the autonomic nervous system is predisposed to asymmetric, lateralized responses to various stimulation autonomic tests. In right-handed patients, right hemisphere stroke has a more marked sympathetic control on the HR than left hemisphere. |
| Long-term Stroke Outcome (<1 Year) | |||||||||||
| Zhao et al., 2020 [24] | Longitudinal | HRV | AIS | 186/60 (53–66) 150M/36F | Calcium channel blocker (34) ACEI (9) Beta-blockers (3) | Coronary artery disease (29) Hypertension (108) Hyperlipidemia (25) Type 2 diabetes mellitus (55) Smoking (127) Alcohol (121) | 36 | 1 year | Within 1-week post ictus | NIHSS (on admission and at discharge) mRS (on admission, at discharge, and after 3, 6, 12 months) | AIS infarction basin, TOAST subtypes, and neurological outcomes at discharge are related to HRV evaluated after admission, suggesting a potential role for HRV in assessing AIS and identifying high-risk patients. |
| He et al., 2018 [42] | Longitudinal | HRV | AIS | 516/66.14 ± 10.11 253M/263F | Antihypertensives (321) Antiplatelets (126) Lipid-lowering medications (223) | Hypertension (367) Diabetes (154) Hyperlipidemia (274) Smoking (149) Alcohol (153) Family history of stroke (101) | - | 1 year | Within 24 h from onset | NIHSS (at baseline) | Decreased FD and END and 1-year RIS following an acute ischemic stroke are positively correlated. |
| Xiong et al., 2019 [67] | Longitudinal | HR, SBP, DBP | IS | 150/66.4 ± 9.9 106M/44F | - | Hypertension (93) Diabetes mellitus (51) Hyperlipidemia (65) Ischemic heart disease 15) Smoking (64) Alcohol (34) | 34 | Until discharge, 3 months and 1 year | 2–4 weeks post-stroke | NIHSS (on admission) mRS (3 months after stroke onset) | Significant autonomic dysfunction in patients with acute ischemic stroke is associated with a poor functional prognosis. |
| Lin et al., 2018 [68] | Longitudinal | BRS | AIS | 176/62.9 ± 12.3 135M/41F | - | Hypertension (149) Diabetes (74) Family history of stroke (63) Smoking (87) Alcohol (34) Hypercholesterolemia (141) Hypertriglyceridemia (84) | - | 12 months after stroke | Within 1 week after stroke | NIHSS (at 1 and 2 weeks after stroke and at discharge) mRS (1, 3, 6, and 12 months after stroke) | BRS within 1 week of stroke is a reliable indicator of complications during hospitalization for AIS and functional outcome (dependency) at 1 month after stroke. |
| Nayani et al., 2016 [13] | Cross-sectional | HRV | IS | 101/63 73M/28F | - | Systemic hypertension (65) Type 2 DM (31) Dyslipidemia (9) Coronary artery disease (24) Smoking (40) | - | 1 year | Within 2 weeks to 4 weeks post ictus | NIHSS (on admission) mRS (at discharge) | Greater frequency of autonomic dysfunction after stroke is linked to insular involvement and higher impairment at onset. Independent of the severity of the initial stroke, those with AD had a greater risk of infarct expansion, hospitalized cardiovascular complications, and a worse prognosis at 1 year. result |
| Wang et al., 2017 [69] | Longitudinal | BPV | AIS | 873/NM 445M/428F | - | Hypertension (765) Diabetes mellitus (193) Hyperlipidemia (489) SCS (138) Coronary artery disease (116) Congestive heart failure (53) Chronic kidney disease (45) | 186 | 12 months | Within 7 days of onset | NIHSS (at onset and at 3 and 12 months) mRS (at 3 and 12 months) | High systolic or diastolic blood pressure within 7 days of the beginning of acute ischemic stroke was linked to neurological function recovery at 3 months, as well as recurrent stroke and composite cardiovascular events within 12 months. |
| Chronic Stroke (>1 Year) Outcome | |||||||||||
| Sandset et al., 2014 [70] | Longitudinal | HR | IS, TIA | 3014/67.3 ± 8.3 1857M/1157F | Beta-blockers (815) Diuretics (1135) Valsartan (1513) | Diabetes mellitus (657) Smoking (572) Left ventricular hypertrophy with strain (535) History of atrial fibrillation (107) | 3014 | 4.5 years | Within the last 120 days of onset | - | The best predictor of recurrent stroke in high-risk, hypertensive patients with prior stroke or TIA was resting heart rate. |
| Leonarduzzi et al., 2018 [71] | Cross-sectional | HRV | IS | 173 | - | Atrial fibrillation (173) | 47 ± 35 months | On admission | CHA2DS2-VASc | It was discovered that scattering coefficients were highly important in predicting IS, especially for patients not receiving antithrombotic therapy. | |
| Verma et al., 2019 [72] | Longitudinal | PRV, HRV | IS | Patients; 41/64.4 ± 1.3 20M/21F Control; 29/65 ± 2 14M/15F | Antihypertensive medication (5-days prior to the study) | - | NM | - | On admission | NHISS (at the time of recording) mRS (at the time of recording) | Consideration of PRV as a substitute for HRV for assessing autonomic cardiovascular regulation when standing in stroke survivors should be performed with caution. |
| Webb et al., 2017 [73] | Longitudinal | BPV | IS | 472/66.2 ± 13.2 273M/199F | - | Diabetes mellitus (49) Family history (110) Hyperlipidemia (128) Smoking (73) | NM | 2 to 5 years | within 6 weeks of transient ischemic attack or non-disabling stroke | - | Beat-to-beat Independent of mean systolic blood pressure and risk variables, BPV predicted recurrent stroke and cardiovascular events, although short-term BPV on ambulatory blood pressure monitoring did not. |
| Nakanishi et al., 2017 [74] | Longitudinal | RHR, BP | IS | 2060/60 ± 11 1660M/400F | ACEI or ARB (2031) Calcium channel blocker (172) Diuretics (1683) Statins (1265) | Hypertension (1239) Diabetes (657) Smoking (363) Alcohol >2 oz/day (512) History of myocardial infarction (816) History of atrial fibrillation (76) | 252 | Up to 6 years (mean 3.5 ± 1.8 years) | Post-treatment | - | Those who have systolic heart failure in sinus rhythm may be more at risk for ischemic stroke if their RHR is lower. |
| Tang et al., 2012 [75] | Cross-sectional | BP | IS, HS, LS, US | 49/66.1 ± 7.0 29M/20F | - | - | NM | Until discharge | 4.5 ± 3.1 years post-stroke | NIHSS (on admission) Chedoke-McMaster Stroke Assessment | To determine those who have had a stroke with OH, a quick orthostatic tolerance test can be performed at the bedside. |
| Bodapati et al., 2017 [76] | Longitudinal | HRV | IS, HS | 884/75.3 ± 4.6 338M/546F | - | Left ventricular hypertrophy (45) Diabetes mellitus (149) History of heart disease (175) | - | ≤8 years | On admission | CHS-SCORE (on admission) | Information from 24-h Holter monitoring is significantly linked to the occurrence of stroke in older people living in the community who have a normal sinus rhythm. |
| Depression due to AIS | |||||||||||
| Tessier et al., 2017 [43] | Longitudinal | HR, HRV | IS | 56/51.7 ± 13.0 39M/17F | - | Hypertension (23) Dyslipidemia (20) Diabetes (2) | - | 3 months | within the first week after stroke | NIHSS (on admission) Lesion volume mRS (after 3 months) | Patients who are unable to complete questionnaires may still be able to use resting HR measures collected in the early poststroke phase to aid in the early prediction of PSD and PSCI. |
| He et al., 2020 [42] | Longitudinal | HRV | IS | 503/65.93 ± 10.19 246M/257F | Antiplatelets (122) Antihypertensive (272) Lipid-lowering medications (195) | Hypertension (323) Diabetes mellitus (150) Hyperlipidemia (250) Smoking (138) Alcohol (149) Family history of stroke (101) | NM | 3 months | Within 72 h from symptom onset | NIHSS (on admission) | Due to the substantial correlation between decreased HRV and PSD, which is frequent following mild to moderate AIS, FD may be used as a reliable technique to predict PSD rhythms. |
| Idiaquez et al., 2015 [77] | Longitudinal | BP, SCOPA-AUT | IS | Patients: 45/65.8 ± 11.7 28M/17F Control: 55/65.2 ± 15.1 19M/36F | Beta-blockers (C. 7/P. 6) ACEI (C. 17/P. 16) CCB (C. 7/P. 6) Diuretic (C. 6/P. 7) Antidepressant (C. 3/P. 5) | Hyperlipidemia (C.13/P. 9) Diabetes mellitus (C. 8/P. 14) Depression (C. 7/P. 16) Smoking (C. 14/P. 23) | - | Until discharge | Between 3 and 12 months after the first symptomatic stroke | NIHSS (on admission) OCSP | In hypertensive patients with mild ischemic stroke, autonomic symptoms, particularly gastrointestinal, urinary, and cardiovascular function, was much worse. |
| Immunosuppression due to AIS | |||||||||||
| Brämer et al., 2014 [37] | Longitudinal | HRV, WBC, CRP, PCT, copeptin | IS | 240 | - | Infection (240) | - | 3 months | 3–5 days after onset | NIHSS (on admission) mRS (at 3 months) Barthel index | Infections in the later sub-acute period can be predicted using HRV indicators collected during the acute post-stroke period. The role of ANS activity in relation to immunomodulation and the emergence of infections after stroke is represented by HRV indices. |
| Brämer et al., 2019 [78] | Longitudinal | HRV | IS | 250/69 (60–78) 132M/118F | Beta-blockers (107) Antihypertensive drugs (156) | Coronary heart disease (42) Diabetes (58) Arterial hypertension (168) | NM | 3 and 5 days after stroke | 24 h after onset | NIHSS (on admission) | Infectious complications in the immediate post-stroke period are predicted by VLF. |
| Yuan et al., 2019 [36] | Longitudinal | ACh, AChE, ChAT | IS | 994/67.88 572M/422F | - | Hypertension (309) Diabetes mellitus (262) Smoking (233) Alcohol (233) | NM | 1 year | <24 h after onset | NIHSS (at baseline) mRS (at baseline) | In individuals with acute stroke, lymphocytes produced more ACh, and pneumonia was a probable outcome. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orgianelis, I.; Merkouris, E.; Kitmeridou, S.; Tsiptsios, D.; Karatzetzou, S.; Sousanidou, A.; Gkantzios, A.; Christidi, F.; Polatidou, E.; Beliani, A.; et al. Exploring the Utility of Autonomic Nervous System Evaluation for Stroke Prognosis. Neurol. Int. 2023, 15, 661-696. https://doi.org/10.3390/neurolint15020042
Orgianelis I, Merkouris E, Kitmeridou S, Tsiptsios D, Karatzetzou S, Sousanidou A, Gkantzios A, Christidi F, Polatidou E, Beliani A, et al. Exploring the Utility of Autonomic Nervous System Evaluation for Stroke Prognosis. Neurology International. 2023; 15(2):661-696. https://doi.org/10.3390/neurolint15020042
Chicago/Turabian StyleOrgianelis, Ilias, Ermis Merkouris, Sofia Kitmeridou, Dimitrios Tsiptsios, Stella Karatzetzou, Anastasia Sousanidou, Aimilios Gkantzios, Foteini Christidi, Efthymia Polatidou, Anastasia Beliani, and et al. 2023. "Exploring the Utility of Autonomic Nervous System Evaluation for Stroke Prognosis" Neurology International 15, no. 2: 661-696. https://doi.org/10.3390/neurolint15020042
APA StyleOrgianelis, I., Merkouris, E., Kitmeridou, S., Tsiptsios, D., Karatzetzou, S., Sousanidou, A., Gkantzios, A., Christidi, F., Polatidou, E., Beliani, A., Tsiakiri, A., Kokkotis, C., Iliopoulos, S., Anagnostopoulos, K., Aggelousis, N., & Vadikolias, K. (2023). Exploring the Utility of Autonomic Nervous System Evaluation for Stroke Prognosis. Neurology International, 15(2), 661-696. https://doi.org/10.3390/neurolint15020042