
Neurite Damage in Patients with Migraine


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Imaging Protocols
2.3. Statistical Analysis
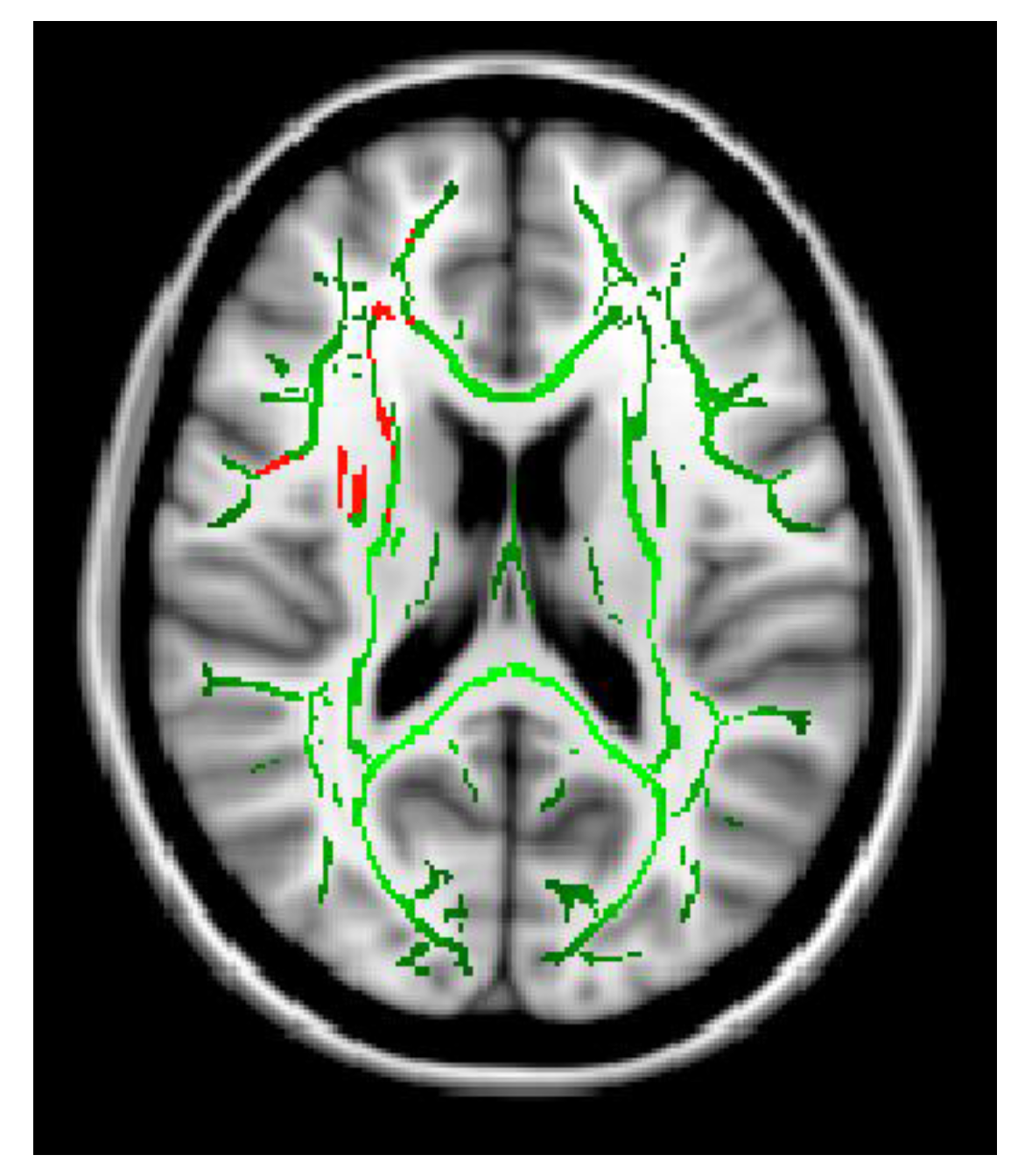
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Lassen, L.H.; Haderslev, P.A.; Jacobsen, V.B.; Iversen, H.K.; Sperling, B.; Olesen, J. Cgrp May Play a Causative Role in Migraine. Cephalalgia 2002, 22, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Tepper, S.; Ashina, M.; Reuter, U.; Brandes, J.L.; Doležil, D.; Silberstein, S.; Winner, P.; Leonardi, D.; Mikol, D.; Lenz, R. Safety and efficacy of erenumab for preventive treatment of chronic migraine: A randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2017, 16, 425–434. [Google Scholar] [CrossRef]
- Silberstein, S.; Dodick, D.; Bigal, M.; Yeung, P.; Goadsby, P.; Blankenbiller, T.; Grozinski-Wolff, M.; Yang, R.; Ma, Y.; Aycardi, E. Fremanezumab for the Preventive Treatment of Chronic Migraine. N. Engl. J. Med. 2017, 377, 2113–2122. [Google Scholar] [CrossRef]
- Förderreuther, S.; Zhang, Q.; Stauffer, V.L.; Aurora, S.K.; Láinez, M.J.A. Preventive effects of galcanezumab in adult patients with episodic or chronic migraine are persistent: Data from the phase 3, randomized, double-blind, placebo-controlled EVOLVE-1, EVOLVE-2, and REGAIN studies. J. Headache Pain 2018, 19, 121. [Google Scholar] [CrossRef]
- Croop, R.; Lipton, R.B.; Kudrow, D.; Stock, D.A.; Kamen, L.; Conway, C.M.; Stock, E.G.; Coric, V.; Goadsby, P.J. Oral rimegepant for preventive treatment of migraine: A phase 2/3, randomised, double-blind, placebo-controlled trial. Lancet 2021, 397, 51–60. [Google Scholar] [CrossRef]
- Ailani, J.; Lipton, R.B.; Goadsby, P.J.; Guo, H.; Miceli, R.; Severt, L.; Finnegan, M.; Trugman, J.M. Atogepant for the Preventive Treatment of Migraine. N. Engl. J. Med. 2021, 385, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Lipton, R.B.; Ailani, J.; Halker Singh, R.B.; Shewale, A.R.; Zhao, S.; Trugman, J.M.; Yu, S.Y.; Viswanathan, H.N. Ubrogepant, an Acute Treatment for Migraine, Improved Patient-Reported Functional Disability and Satisfaction in 2 Single-Attack Phase 3 Randomized Trials, ACHIEVE I and II. Headache J. Head Face Pain 2020, 60, 686–700. [Google Scholar] [CrossRef]
- Ailani, J.; Lipton, R.B.; Hutchinson, S.; Knievel, K.; Lu, K.; Butler, M.; Yu, S.Y.; Finnegan, M.; Severt, L.; Trugman, J.M. Long-Term Safety Evaluation of Ubrogepant for the Acute Treatment of Migraine: Phase 3, Randomized, 52-Week Extension Trial. Headache J. Head Face Pain 2020, 60, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Alpuente, A.; Gallardo, V.J.; Asskour, L.; Caronna, E.; Torres-Ferrus, M.; Pozo-Rosich, P. Salivary CGRP can monitor the different migraine phases: CGRP (in)dependent attacks. Cephalalgia 2021, 42, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Alpuente, A.; Gallardo, V.J.; Asskour, L.; Caronna, E.; Torres-Ferrus, M.; Pozo-Rosich, P. Salivary CGRP and Erenumab Treatment Response: Towards Precision Medicine in Migraine. Ann. Neurol. 2022, 92, 846–859. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, L.R. Imaging Evaluation of Acute Ischemic Stroke. Stroke 2011, 42, S12–S15. [Google Scholar] [CrossRef] [PubMed]
- Robert, J.; Young, E.A.K. Brain MRI: Tumor evaluation. J. Magn. Reson. Imaging 2006, 24, 709–724. [Google Scholar]
- Wintermark, M.; Sanelli, P.C.; Anzai, Y.; Tsiouris, A.J.; Whitlow, C.T. Imaging Evidence and Recommendations for Traumatic Brain Injury: Advanced Neuro- and Neurovascular Imaging Techniques. Am. J. Neuroradiol. 2015, 36, E1–E11. [Google Scholar] [CrossRef] [PubMed]
- Glenn, O.A.; Barkovich, A.J. Magnetic Resonance Imaging of the Fetal Brain and Spine: An Increasingly Important Tool in Prenatal Diagnosis, Part 1. AJNR Am. J. Neuroradiol. 2006, 27, 1604–1611. [Google Scholar] [PubMed]
- Greitz, D.; Hannerz, J.; Rähn, T.; Bolander, H.; Ericsson, A. MR imaging of cerebrospinal fluid dynamics in health and disease. Acta Radiol. 1994, 35, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Kakeda, S.; Korogi, Y. The efficacy of a voxel-based morphometry on the analysis of imaging in schizophrenia, temporal lobe epilepsy, and Alzheimer’s disease/mild cognitive impairment: A review. Neuroradiology 2010, 52, 711–721. [Google Scholar] [CrossRef]
- Kruit, M.C.; van Buchem, M.A.; Hofman, P.A.M.; Bakkers, J.T.N.; Terwindt, G.M.; Ferrari, M.D.; Launer, L.J. Migraine as a Risk Factor for Subclinical Brain Lesions. JAMA 2004, 291, 427–434. [Google Scholar] [CrossRef]
- Kruit, M.C.; Launer, L.J.; Ferrari, M.D.; van Buchem, M.A. Brain stem and cerebellar hyperintense lesions in migraine. Stroke 2006, 37, 1109–1112. [Google Scholar] [CrossRef]
- MacClellan, L.R.; Giles, W.; Cole, J.; Wozniak, M.; Stern, B.; Mitchell, B.D.; Kittner, S.J. Probable Migraine with Visual Aura and Risk of Ischemic Stroke: The Stroke Prevention in Young Women Study. Stroke 2007, 38, 2438–2445. [Google Scholar] [CrossRef]
- Hamedani, A.G.; Rose, K.M.; Peterlin, B.L.; Mosley, T.H.; Coker, L.H.; Jack, C.R.; Knopman, D.S.; Alonso, A.; Gottesman, R.F. Migraine and white matter hyperintensities: The ARIC MRI study. Neurology 2013, 81, 1308–1313. [Google Scholar] [CrossRef]
- Monteith, T.; Gardener, H.; Rundek, T.; Dong, C.; Yoshita, M.; Elkind, M.S.V.; DeCarli, C.; Sacco, R.L.; Wright, C.B. Migraine, White Matter Hyperintensities, and Subclinical Brain Infarction in a Diverse Community: The Northern Manhattan Study. Stroke 2014, 45, 1830–1832. [Google Scholar] [CrossRef]
- Øie, L.R.; Kurth, T.; Gulati, S.; Dodick, D.W. Migraine and risk of stroke. J. Neurol. Neurosurg. Psychiatry 2020, 91, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Sakai, F.; Igarashi, H. Prevalence of migraine in Japan: A nationwide survey. Cephalalgia 1997, 17, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.; Kim, D.-W.; Kim, B.-K.; Kim, J.-M.; Jang, T.-W.; Park, J.; Lee, K.; Cho, S.-J. Gender-specific influence of socioeconomic status on the prevalence of migraine and tension-type headache: The results from the Korean headache survey. J. Headache Pain 2013, 14, 82. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, F.; Koch, M.; Schmidt, R.; Offenbacher, H.; Payer, F.; Freidl, W.; Lechner, H. The prevalence of cerebral damage varies with migraine type: A MRI study. Headache 1992, 32, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Boudreau, G.; Leroux, E. The complications of migraine classified under the international classification of headache disorders: A review. Headache Care 2006, 3, 85–90. [Google Scholar] [CrossRef]
- Kurth, T.; Winter, A.C.; Eliassen, A.H.; Dushkes, R.; Mukamal, K.J.; Rimm, E.B.; Willett, W.C.; Manson, J.E.; Rexrode, K.M. Migraine and risk of cardiovascular disease in women: Prospective cohort study. BMJ 2016, 353, i2610. [Google Scholar] [CrossRef]
- West, B.H.; Noureddin, N.; Mamzhi, Y.; Low, C.G.; Coluzzi, A.C.; Shih, E.J.; Gevorgyan Fleming, R.; Saver, J.L.; Liebeskind, D.S.; Charles, A.; et al. Frequency of Patent Foramen Ovale and Migraine in Patients with Cryptogenic Stroke. Stroke 2018, 49, 1123–1128. [Google Scholar] [CrossRef]
- Takagi, H.; Umemoto, T. A meta-analysis of case-control studies of the association of migraine and patent foramen ovale. J. Cardiol. 2016, 67, 493–503. [Google Scholar] [CrossRef]
- Pezzini, A.; Grassi, M.; Lodigiani, C.; Patella, R.; Gandolfo, C.; Casoni, F.; Musolino, R.; Calabro, R.S.; Bovi, P.; Adami, A.; et al. Predictors of Migraine Subtypes in Young Adults with Ischemic Stroke: The Italian Project on Stroke in Young Adults. Stroke 2011, 42, 17–21. [Google Scholar] [CrossRef]
- Lance, J.W. The pathophysiology of migraine. Ann. Acad. Med. Singap. 1985, 14, 4–11. [Google Scholar] [PubMed]
- Hadjikhani, N.; Sanchez del Rio, M.; Wu, O.; Schwartz, D.; Bakker, D.; Fischl, B.; Kwong, K.K.; Cutrer, F.M.; Rosen, B.R.; Tootell, R.B.H.; et al. Mechanisms of migraine aura revealed by functional MRI in human visual cortex. Proc. Natl. Acad. Sci. USA 2001, 98, 4687–4692. [Google Scholar] [CrossRef] [PubMed]
- Tfelt-Hansen, P.C. History of migraine with aura and cortical spreading depression from 1941 and onwards. Cephalalgia 2009, 30, 780–792. [Google Scholar] [CrossRef]
- Burstein, R.; Noseda, R.; Borsook, D. Migraine: Multiple Processes, Complex Pathophysiology. J. Neurosci. Off. J. Soc. Neurosci. 2015, 35, 6619–6629. [Google Scholar] [CrossRef] [PubMed]
- Schulte, L.H.; Mehnert, J.; May, A. Longitudinal Neuroimaging over 30 Days: Temporal Characteristics of Migraine. Ann. Neurol. 2020, 87, 646–651. [Google Scholar] [CrossRef]
- Arkink, E.B.; Terwindt, G.M.; de Craen, A.J.M.; Konishi, J.; van der Grond, J.; van Buchem, M.; Ferrari, M.D.; Kruit, M.C. Infratentorial Microbleeds. Stroke 2015, 46, 1987–1989. [Google Scholar] [CrossRef]
- Dai, Z.; Zhong, J.; Xiao, P.; Zhu, Y.; Chen, F.; Pan, P.; Shi, H. Gray matter correlates of migraine and gender effect: A meta-analysis of voxel-based morphometry studies. Neuroscience 2015, 299, 88–96. [Google Scholar] [CrossRef]
- Liu, J.; Lan, L.; Li, G.; Yan, X.; Nan, J.; Xiong, S.; Yin, Q.; von Deneen, K.M.; Gong, Q.; Liang, F.; et al. Migraine-Related Gray Matter and White Matter Changes at a 1-Year Follow-Up Evaluation. J. Pain 2013, 14, 1703–1708. [Google Scholar] [CrossRef]
- Shibata, Y.; Goto, M.; Ishiyama, S. Analysis of Migraine Pathophysiology by Magnetic Resonance Imaging. OBM Neurobiol. 2022, 6, 115. [Google Scholar] [CrossRef]
- DaSilva, A.F.M.; Granziera, C.; Nouchine Hadjikhani, J.S. Thickening in the somatosensory cortex of patients with migraine. Neurology 2007, 69, 1990–1995. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, J.B.; Suh, S.I.; Seo, W.K.; Oh, K.; Koh, S.B. Thickening of the somatosensory cortex in migraine without aura. Cephalalgia 2014, 34, 1125–1133. [Google Scholar] [CrossRef]
- Chong, C.D.; Dodick, D.W.; Schlaggar, B.L.; Schwedt, T.J. Atypical age-related cortical thinning in episodic migraine. Cephalalgia 2014, 34, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Maleki, N.; Becerra, L.; Brawn, J.; Bigal, M.; Burstein, R.; Borsook, D. Concurrent functional and structural cortical alterations in migraine. Cephalalgia 2012, 32, 607–620. [Google Scholar] [CrossRef] [PubMed]
- Messina, R.; Rocca, M.A.; Colombo, B.; Valsasina, P.; Horsfield, M.A.; Copetti, M.; Falini, A.; Comi, G.; Filippi, M. Cortical Abnormalities in Patients with Migraine: A Surface-based Analysis. Radiology 2013, 268, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Ishiyama, S.; Matsushita, A. White matter diffusion abnormalities in migraine and medication overuse headache: A 1.5-Tesla tract-based spatial statistics study. Clin. Neurol. Neurosurg. 2018, 174, 167–173. [Google Scholar] [CrossRef]
- Schwedt, T.J.; Si, B.; Li, J.; Wu, T.; Chong, C.D. Migraine Subclassification via a Data-Driven Automated Approach Using Multimodality Factor Mixture Modeling of Brain Structure Measurements. Headache J. Head Face Pain 2017, 57, 1051–1064. [Google Scholar] [CrossRef] [PubMed]
- Planchuelo-Gómez, Á.; García-Azorín, D.; Guerrero, Á.L.; de Luis-García, R.; Rodríguez, M.; Aja-Fernández, S. Alternative Microstructural Measures to Complement Diffusion Tensor Imaging in Migraine Studies with Standard MRI Acquisition. Brain Sci. 2020, 10, 711. [Google Scholar] [CrossRef]
- Schramm, S.; Börner, C.; Reichert, M.; Baum, T.; Zimmer, C.; Heinen, F.; Bonfert, M.V.; Sollmann, N. Functional magnetic resonance imaging in migraine: A systematic review. Cephalalgia 2023, 43, 03331024221128278. [Google Scholar] [CrossRef]
- Ishiyama, S.; Shibata, Y.; Ayuzawa, S.; Matsushita, A.; Matsumura, A.; Ishikawa, E. The Modifying of Functional Connectivity Induced by Peripheral Nerve Field Stimulation using Electroacupuncture for Migraine: A Prospective Clinical Study. Pain Med. 2022, 23, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Planchuelo-Gómez, Á.; García-Azorín, D.; Guerrero, Á.L.; Aja-Fernández, S.; Rodríguez, M.; de Luis-García, R. White matter changes in chronic and episodic migraine: A diffusion tensor imaging study. J. Headache Pain 2020, 21, 1. [Google Scholar] [CrossRef]
- Zhang, H.; Schneider, T.; Wheeler-Kingshott, C.A.; Alexander, D.C. NODDI: Practical in vivo neurite orientation dispersion and density imaging of the human brain. NeuroImage 2012, 61, 1000–1016. [Google Scholar] [CrossRef] [PubMed]
- Seyedmirzaei, H.; Nabizadeh, F.; Aarabi, M.H.; Pini, L. Neurite Orientation Dispersion and Density Imaging in Multiple Sclerosis: A Systematic Review. J. Magn. Reson. Imaging 2023, 58, 1011–1029. [Google Scholar] [CrossRef]
- Andica, C.; Kamagata, K.; Hatano, T.; Saito, A.; Uchida, W.; Ogawa, T.; Takeshige-Amano, H.; Zalesky, A.; Wada, A.; Suzuki, M.; et al. Free-Water Imaging in White and Gray Matter in Parkinson’s Disease. Cells 2019, 8, 839. [Google Scholar] [CrossRef] [PubMed]
- Nakaya, M.; Sato, N.; Matsuda, H.; Maikusa, N.; Shigemoto, Y.; Sone, D.; Yamao, T.; Ogawa, M.; Kimura, Y.; Chiba, E.; et al. Free water derived by multi-shell diffusion MRI reflects tau/neuroinflammatory pathology in Alzheimer’s disease. Alzheimer Dement. 2022, 8, e12356. [Google Scholar] [CrossRef]
- Kraguljac, N.V.; Guerreri, M.; Strickland, M.J.; Zhang, H. Neurite Orientation Dispersion and Density Imaging in Psychiatric Disorders: A Systematic Literature Review and a Technical Note. Biol. Psychiatry Glob. Open Sci. 2023, 3, 10–21. [Google Scholar] [CrossRef]
- Timmers, I.; Roebroeck, A.; Bastiani, M.; Jansma, B.; Rubio-Gozalbo, E.; Zhang, H. Assessing Microstructural Substrates of White Matter Abnormalities: A Comparative Study Using DTI and NODDI. PLoS ONE 2016, 11, e0167884. [Google Scholar] [CrossRef]
- Penzes, P.; Cahill, M.E.; Jones, K.A.; VanLeeuwen, J.-E.; Woolfrey, K.M. Dendritic spine pathology in neuropsychiatric disorders. Nat. Neurosci. 2011, 14, 285–293. [Google Scholar] [CrossRef]
- Nazeri, A.; Mulsant, B.H.; Rajji, T.K.; Levesque, M.L.; Pipitone, J.; Stefanik, L.; Shahab, S.; Roostaei, T.; Wheeler, A.L.; Chavez, S.; et al. Gray Matter Neuritic Microstructure Deficits in Schizophrenia and Bipolar Disorder. Biol. Psychiatry 2017, 82, 726–736. [Google Scholar] [CrossRef]
- Zhao, J.; Li, J.-B.; Wang, J.-Y.; Wang, Y.-L.; Liu, D.-W.; Li, X.-B.; Song, Y.-K.; Tian, Y.-S.; Yan, X.; Li, Z.-H.; et al. Quantitative analysis of neurite orientation dispersion and density imaging in grading gliomas and detecting IDH-1 gene mutation status. NeuroImage Clin. 2018, 19, 174–181. [Google Scholar] [CrossRef]
- Parker, T.D.; Slattery, C.F.; Zhang, J.; Nicholas, J.M.; Paterson, R.W.; Foulkes, A.J.M.; Malone, I.B.; Thomas, D.L.; Modat, M.; Cash, D.M.; et al. Cortical microstructure in young onset Alzheimer’s disease using neurite orientation dispersion and density imaging. Hum. Brain Mapp. 2018, 39, 3005–3017. [Google Scholar] [CrossRef]
- Wu, Y.-C.; Mustafi, S.M.; Harezlak, J.; Kodiweera, C.; Flashman, L.A.; McAllister, T.W. Hybrid Diffusion Imaging in Mild Traumatic Brain Injury. J. Neurotrauma 2018, 35, 2377–2390. [Google Scholar] [CrossRef] [PubMed]
- Hara, S.; Hori, M.; Ueda, R.; Hayashi, S.; Inaji, M.; Tanaka, Y.; Maehara, T.; Ishii, K.; Aoki, S.; Nariai, T. Unraveling Specific Brain Microstructural Damage in Moyamoya Disease Using Diffusion Magnetic Resonance Imaging and Positron Emission Tomography. J. Stroke Cerebrovasc. Dis. 2019, 28, 1113–1125. [Google Scholar] [CrossRef]
- Sacco, S.; Caverzasi, E.; Papinutto, N.; Cordano, C.; Bischof, A.; Gundel, T.; Cheng, S.; Asteggiano, C.; Kirkish, G.; Mallott, J.; et al. Neurite Orientation Dispersion and Density Imaging for Assessing Acute Inflammation and Lesion Evolution in MS. Am. J. Neuroradiol. 2020, 41, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Winston, G.P. The potential role of novel diffusion imaging techniques in the understanding and treatment of epilepsy. Quant. Imaging Med. Surg. 2015, 5, 279–287. [Google Scholar]
- Sone, D.; Sato, N.; Ota, M.; Maikusa, N.; Kimura, Y.; Matsuda, H. Abnormal neurite density and orientation dispersion in unilateral temporal lobe epilepsy detected by advanced diffusion imaging. NeuroImage Clin. 2018, 20, 772–782. [Google Scholar] [CrossRef]
- Schwedt, T.J.; Chong, C.D. Medication Overuse Headache: Pathophysiological Insights from Structural and Functional Brain MRI Research. Headache J. Head Face Pain 2017, 57, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, N.; Admiraal-Behloul, F.; Arkink, E.B.; Kruit, M.C.; Schoonman, G.G.; Ferrari, M.D.; Van Buchem, M.A. Attack Frequency and Disease Duration as Indicators for Brain Damage in Migraine. Headache J. Head Face Pain 2008, 48, 1044–1055. [Google Scholar] [CrossRef]
- Gomez-Pilar, J.; Martínez-Cagigal, V.; García-Azorín, D.; Gómez, C.; Guerrero, Á.; Hornero, R. Headache-related circuits and high frequencies evaluated by EEG, MRI, PET as potential biomarkers to differentiate chronic and episodic migraine: Evidence from a systematic review. J. Headache Pain 2022, 23, 95. [Google Scholar] [CrossRef]
- Smith, S.M. Tract-based spatial statistics. NeuroImage 2006, 31, 1487–1505. [Google Scholar] [CrossRef]
- Szabó, N.; Kincses, Z.T.; Párdutz, Á.; Tajti, J.; Szok, D.; Tuka, B.; Király, A.; Babos, M.; Vörös, E.; Bomboi, G.; et al. White matter microstructural alterations in migraine: A diffusion-weighted MRI study. Pain 2012, 153, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Yuan, K.; Qin, W.; Zhao, L.; Dong, M.; Liu, P.; Yang, X.; Liu, J.; Sun, J.; Zhou, G.; et al. Axonal loss of white matter in migraine without aura: A tract-based spatial statistics study. Cephalalgia 2013, 33, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Li, X.L.; Fang, Y.N.; Gao, Q.C.; Lin, E.J.; Hu, S.H.; Ren, L.; Ding, M.H.; Luo, B.N. A Diffusion Tensor Magnetic Resonance Imaging Study of Corpus Callosum from Adult Patients with Migraine Complicated with Depressive/Anxious Disorder. Headache J. Head Face Pain 2011, 51, 237–245. [Google Scholar] [CrossRef]
- Rocca, M.A.; Pagani, E.; Colombo, B.; Tortorella, P.; Falini, A.; Comi, G.; Filippi, M. Selective diffusion changes of the visual pathways in patients with migraine: A 3-T tractography study. Cephalalgia 2008, 28, 1061–1068. [Google Scholar] [CrossRef]
- Coppola, G.; Tinelli, E.; Lepre, C.; Iacovelli, E.; Di Lorenzo, C.; Di Lorenzo, G.; Serrao, M.; Pauri, F.; Fiermonte, G.; Bianco, F.; et al. Dynamic changes in thalamic microstructure of migraine without aura patients: A diffusion tensor magnetic resonance imaging study. Eur. J. Neurol. 2014, 21, 287-e13. [Google Scholar] [CrossRef]
- Coppola, G.; Di Renzo, A.; Tinelli, E.; Iacovelli, E.; Lepre, C.; Di Lorenzo, C.; Di Lorenzo, G.; Di Lenola, D.; Parisi, V.; Serrao, M.; et al. Evidence for brain morphometric changes during the migraine cycle: A magnetic resonance-based morphometry study. Cephalalgia 2015, 35, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Qin, W.; Liu, P.; Zhao, L.; Yu, D.; Dong, M.; Liu, J.; Yang, X.; von Deneen, K.M.; Liang, F.; et al. Reduced fractional anisotropy of corpus callosum modulates inter-hemispheric resting state functional connectivity in migraine patients without aura. PLoS ONE 2012, 7, e45476. [Google Scholar] [CrossRef]
- Karsan, N.; Goadsby, P.J. Neuroimaging in the pre-ictal or premonitory phase of migraine: A narrative review. J. Headache Pain 2023, 24, 106. [Google Scholar] [CrossRef]
- Kasia, K.M.; Noemi, M.; Flavia Di, P.; Vaughan, G.M.; Paul, M.M.; Luke, A.H. Fluctuating Regional Brainstem Diffusion Imaging Measures of Microstructure across the Migraine Cycle. Eneuro 2019, 6, 5–19. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Migraine | Healthy Volunteer | p | |
|---|---|---|---|
| n | 29 | 23 | - |
| Male/female | 2/27 | 6/17 | ns |
| Mean age ±SD | 44.5 ± 13.5 | 44.9 ± 12.7 | ns |
| Duration ± SD | 21.4 ± 15.7 | - | - |
| MOH(Yes/No) | 4/25 | - | - |
| EM/CM | 17/12 | - | - |
| EM | CM | p | |
|---|---|---|---|
| n | 17 | 12 | |
| Male/female | 0/17 | 1/11 | |
| Mean age +SD | 46.6 ± 14.6 | 41.4 ± 11.0 | 0.3 |
| Duration +SD | 23.9 ± 15.4 | 17.6 ± 15.3 | 0.32 |
| MOH | Non-MOH | p | |
|---|---|---|---|
| n | 4 | 25 | |
| Male/female | 0/4 | 1/24 | |
| Mean age + SD | 37.8 ± 7.1 | 45.6 ± 13.9 | 0.155 |
| Duration + SD | 7.5 ± 4.6 | 23.6 ± 15.7 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shibata, Y.; Ishiyama, S. Neurite Damage in Patients with Migraine. Neurol. Int. 2024, 16, 299-311. https://doi.org/10.3390/neurolint16020021
Shibata Y, Ishiyama S. Neurite Damage in Patients with Migraine. Neurology International. 2024; 16(2):299-311. https://doi.org/10.3390/neurolint16020021
Chicago/Turabian StyleShibata, Yasushi, and Sumire Ishiyama. 2024. "Neurite Damage in Patients with Migraine" Neurology International 16, no. 2: 299-311. https://doi.org/10.3390/neurolint16020021
APA StyleShibata, Y., & Ishiyama, S. (2024). Neurite Damage in Patients with Migraine. Neurology International, 16(2), 299-311. https://doi.org/10.3390/neurolint16020021