
Endoscopic Evaluation and Therapeutic Considerations of Small Bowel Crohn’s Disease


Abstract
:1. Introduction
2. Endoscopic Evaluation of Small Bowel Crohn’s Disease
2.1. Indications of Small Bowel Endoscopy in CD
- (1)
- Suspected isolated small bowel CD [8];
- (2)
- Small bowel evaluation in patients with confirmed CD [9];
- (3)
- Assessment for post-operative CD recurrence in small bowel after ileo-colonic resection [10];
- (4)
- Small bowel evaluation in IBD-unclassified and disease reclassification [8];
- (5)
- Therapeutic interventions in small bowel CD (stricture dilatation, retained capsule or foreign body retrieval, hemostasis for small bowel bleed) [8].
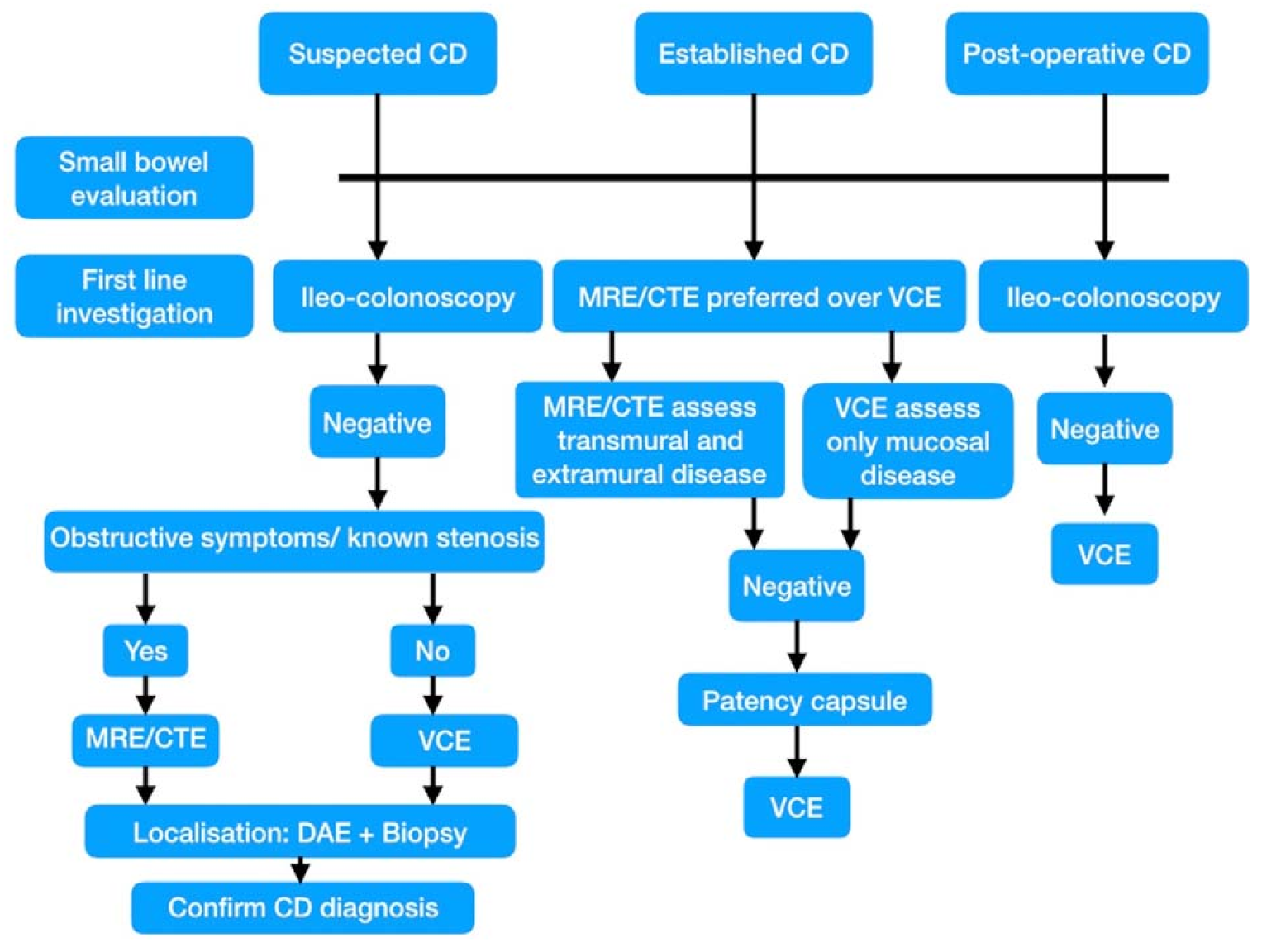
2.2. Role of Small Bowel Endoscopy in Suspected and Established CD
2.3. VCE in Small Bowel CD
2.3.1. Comparison of VCE with Other Diagnostic Modalities
2.3.2. VCE in Suspected Small Bowel CD
2.3.3. VCE in Established Small Bowel CD
Assessing Distribution and Monitoring Disease Activity: The VCE Scores
Mucosal Healing and Treat to Target
Evaluation of Unexplained Anemia or Obscure GI Bleed in CD
Assessment of Postoperative CD Recurrence
Classification of IBD-Unclassified (IBD-U)
Mimics of Crohn Disease on Capsule Endoscopy
Capsule Retention
Patency Capsule
Pan-Enteric Capsules
Application of Deep Learning Technology for VCE in CD
2.4. Enteroscopy in CD
2.4.1. SBE/DBE
2.4.2. BGE
2.4.3. NMSE
2.4.4. DAE in Suspected CD
2.4.5. AE in Established CD
2.4.6. DAE Guided Therapeutic Intervention
Small Bowel Strictures
Endoscopic Balloon Dilatation (EBD)
Outcomes of EBD for Small Bowel Strictures
Factors Predicting Outcomes of EBD
Graded Versus One Step Dilation
Endoscopic Techniques Other Than EBD for Small Bowel Strictures
2.4.7. DAE in Pediatric Patients
2.5. Intra-Operative Enteroscopy (IOE) in CD
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Farmer, R.G.; Hawk, W.A.; Turnbull, R.B., Jr. Clinical patterns in Crohn’s disease: A statistical study of 615 cases. Gastroenterology 1975, 68, 627–635. [Google Scholar] [CrossRef]
- Valle, J.; Alcantara, M.; Perez-Grueso, M.J.; Navajas, J.; Muñoz-Rosas, C.; Legaz, M.L.; Cuena, R.; Carrobles, J.M. Clinical features of patients with negative results from traditional diagnostic work-up and Crohn’s disease findings from capsule endoscopy. J. Clin. Gastroenterol. 2006, 40, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Doherty, G.A.; Moss, A.C.; Cheifetz, A.S. Capsule endoscopy for small-bowel evaluation in Crohn’s disease. Gastrointest. Endosc. 2011, 74, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Broide, E.; Shalem, T.; Richter, V.; Matalon, S.; Shirin, H. The safety and feasibility of a new through-the-scope balloon-assisted enteroscopy in children. J. Pediatr. Gastroenterol. Nutr. 2020, 71, e6–e11. [Google Scholar] [CrossRef] [PubMed]
- Ramchandani, M.; Rughwani, H.; Inavolu, P.; Singh, A.P.; Tevethia, H.V.; Jagtap, N.; Sekaran, A.; Kanakagiri, H.; Darishetty, S.; Reddy, D.N. Diagnostic yield and therapeutic impact of novel motorized spiral enteroscopy in small-bowel disorders: A single-center, real-world experience from a tertiary care hospital (with video). Gastrointest. Endosc. 2021, 93, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.R.; Kim, J.O.; Byeon, J.S.; Yang, D.H.; Ko, B.M.; Goong, H.J.; Jang, H.J.; Park, S.J.; Kim, E.R.; Hong, S.N.; et al. Korean Association for the study of intestinal disease (KASID). Enteroscopy in Crohn’s disease: Are there any changes in role or outcomes over time? A KASID multicenter study. Gut Liver 2020, 6. [Google Scholar] [CrossRef]
- McCain, J.D.; Pasha, S.F.; Leighton, J.A. Role of capsule endoscopy in inflammatory bowel disease. Gastrointest. Endosc. Clin. N. Am. 2021, 31, 345–361. [Google Scholar] [CrossRef]
- Pennazio, M.; Spada, C.; Eliakim, R.; Keuchel, M.; May, A.; Mulder, C.J.; Rondonotti, E.; Adler, S.N.; Albert, J.; Baltes, P.; et al. Small-bowel capsule endoscopy and device-assisted enteroscopy for diagnosis and treatment of small-bowel disorders: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2015, 47, 352–376. [Google Scholar] [CrossRef] [Green Version]
- Bourreille, A.; Ignjatovic, A.; Aabakken, L.; Loftus, E.V., Jr.; Eliakim, R.; Pennazio, M.; Bouhnik, Y.; Seidman, E.; Keuchel, M.; Albert, J.G.; et al. Role of small-bowel endoscopy in the management of patients with inflammatory bowel disease: An international OMED-ECCO consensus. Endoscopy 2009, 41, 618–637. [Google Scholar] [CrossRef] [Green Version]
- Condino, G.; Calabrese, E.; Onali, S. Small bowel capsule endoscopy for assessing early postoperative recurrence of Crohn’s disease: A prospective longitudinal study. Gastroenterology 2013, 144, S425. [Google Scholar] [CrossRef]
- Van Assche, G.; Dignass, A.; Panes, J.; Beaugerie, L.; Karagiannis, J.; Allez, M.; Ochsenkühn, T.; Orchard, T.; Rogler, G.; Louis, E.; et al. European Crohn’s and Colitis Organisation (ECCO). The second European evidence based consensus on the diagnosis and management of Crohn’s disease: Definitions and diagnosis. J. Crohns Colitis 2010, 4, 7–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.D.; Nathan, T.; Rafaelsen, S.R.; Kjeldsen, J. Ileoscopy reduces the need for small bowel imaging in suspected Crohn’s disease. Dan. Med. J. 2012, 59, A4491. [Google Scholar] [PubMed]
- Banerjee, R.; Pal, P.; Mak, J.W.Y.; Ng, S.C. Challenges in the diagnosis and management of inflammatory bowel disease in resource-limited settings in Asia. Lancet Gastroenterol. Hepatol. 2020, 5, 1076–1088. [Google Scholar] [CrossRef]
- Dionisio, P.M.; Gurudu, S.R.; Leighton, J.A.; Leontiadis, G.I.; Fleischer, D.E.; Hara, A.K.; Heigh, R.I.; Shiff, A.D.; Sharma, V.K. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: A meta-analysis. Am. J. Gastroenterol. 2010, 105, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Tukey, M.; Pleskow, D.; Legnani, P.; Cheifet, A.S.; Moss, A.C. The utility of capsule endoscopy in patients with suspected Crohn′s disease. Am. J. Gastroenterol. 2009, 104, 2734–2739. [Google Scholar] [CrossRef]
- Solem, C.A.; Loftus, E.V., Jr.; Fletcher, J.G.; Baron, T.H.; Gostout, C.J.; Petersen, B.T.; Tremaine, W.J.; Egan, L.J.; Faubion, W.A.; Schroeder, K.W.; et al. Small-bowel imaging in Crohn’s disease: A prospective, blinded, 4-way comparison trial. Gastrointest. Endosc. 2008, 68, 255–266. [Google Scholar] [CrossRef] [PubMed]
- González-Suárez, B.; Rodriguez, S.; Ricart, E.; Ordás, I.; Rimola, J.; Díaz-González, Á.; Romero, C.; de Miguel, C.R.; Jáuregui, A.; Araujo, I.K.; et al. Comparison of capsule endoscopy and magnetic resonance enterography for the assessment of small bowel lesions in Crohn’s disease. Inflamm. Bowel Dis. 2018, 24, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Kopylov, U.; Yung, D.E.; Engel, T.; Vijayan, S.; Har-Noy, O.; Katz, L.; Oliva, S.; Avni, T.; Battat, R.; Eliakim, R.; et al. Diagnostic yield of capsule endoscopy versus magnetic resonance enterography and small bowel contrast ultrasound in the evaluation of small bowel Crohn’s disease: Systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 854–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.D.; Nathan, T.; Rafaelsen, S.R.; Kjeldsen, J. Diagnostic accuracy of capsule endoscopy for small bowel Crohn’s disease is superior to that of MR enterography or CT enterography. Clin. Gastroenterol. Hepatol. 2011, 9, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Girelli, C.M.; Porta, P.; Malacrida, V.; Barzaghi, F.; Rocca, F. Clinical outcome of patients examined by capsule endoscopy for suspected small bowel Crohn’s disease. Dig. Liver Dis. 2007, 39, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.; Holleran, G.; Costigan, D.; McNamara, D. Capsule endoscopy: High negative predictive value in the long term despite a low diagnostic yield in patients with suspected Crohn’s disease. United Eur. Gastroenterol. J. 2013, 1, 461–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dilauro, S.; Crum-Cianflone, N.F. Ileitis: When it is not Crohn’s disease. Curr. Gastro. Enterol. Rep. 2010, 12, 249–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, J.L.; Eisen, G.M.; Lewis, B.; Gralnek, I.M.; Zlotnick, S.; Fort, J.G. Investigators. Video capsule endoscopy to prospectively assess small bowel injury with celecoxib, naproxen plus omeprazole, and placebo. Clin. Gastroenterol. Hepatol. 2005, 3, 133–141. [Google Scholar] [CrossRef]
- Jung, E.S.; Lee, S.P.; Kae, S.H.; Kim, J.H.; Kim, H.S.; Jang, H.J. Diagnostic accuracy of fecal calprotectin for the detection of small bowel Crohn’s disease through capsule endoscopy: An updated meta-analysis and systematic review. Gut Liver 2020, 24. [Google Scholar] [CrossRef]
- Pal, P.; Reddy, D.N.; Nabi, Z. Role of Small Bowel Endoscopy in Diagnosis and Management of Inflammatory Bowel Disease: Current Perspective, Endoscopy in Small Bowel Diseases; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Bouguen, G.; Levesque, B.G.; Feagan, B.G.; Kavanaugh, A.; Peyrin-Biroulet, L.; Colombel, J.F.; Hanauer, S.B.; Sandborn, W.J. Treat to target: A proposed new paradigm for the management of Crohn’s disease. Clin. Gastroenterol. Hepatol. 2015, 13, 1042–1050.e2. [Google Scholar] [CrossRef] [Green Version]
- Mow, W.S.; Lo, S.K.; Targan, S.R.; Dubinsky, M.C.; Treyzon, L.; Abreu-Martin, M.T.; Papadakis, K.A.; Vasiliauskas, E.A. Initial experience with wireless capsule enteroscopy in the diagnosis and management of inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2004, 2, 31–40. [Google Scholar] [CrossRef]
- Gralnek, I.M.; Defranchis, R.; Seidman, E.; Leighton, J.A.; Legnani, P.; Lewis, B.S. Development of a capsule endoscopy scoring index for small bowel mucosal inflammatory change. Aliment. Pharmacol. Ther. 2008, 27, 146–154. [Google Scholar] [CrossRef]
- Gal, E.; Geller, A.; Fraser, G.; Levi, Z.; Niv, Y. Assessment and validation of the new capsule endoscopy Crohn’s disease activity index (CECDAI). Dig. Dis. Sci. 2008, 53, 1933–1937. [Google Scholar] [CrossRef]
- Omori, T.; Kambayashi, H.; Murasugi, S.; Ito, A.; Yonezawa, M.; Nakamura, S.; Tokushige, K. Comparison of lewis score and capsule endoscopy Crohn’s disease activity index in patients with Crohn’s disease. Dig. Dis. Sci. 2020, 65, 1180–1188. [Google Scholar] [CrossRef]
- Yablecovitch, D.; Lahat, A.; Neuman, S.; Levhar, N.; Avidan, B.; Ben-Horin, S.; Eliakim, R.; Kopylov, U. The Lewis score or the capsule endoscopy Crohn’s disease activity index: Which one is better for the assessment of small bowel inflammation in established Crohn’s disease? Ther. Adv. Gastroenterol. 2018, 11, 1756283X17747780. [Google Scholar] [CrossRef] [Green Version]
- Fairbrass, K.M.; Costantino, S.J.; Gracie, D.J.; Ford, A.C. Prevalence of irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease in remission: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1053–1062. [Google Scholar] [CrossRef]
- Niv, Y. Diagnostic value of capsule endoscopy during relapse in co-morbid irritable bowel syndrome and Crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2004, 16, 1073–1074. [Google Scholar] [CrossRef] [PubMed]
- Sipponen, T.; Haapamäki, J.; Savilahti, E.; Alfthan, H.; Hämäläinen, E.; Rautiainen, H.; Koskenpato, J.; Nuutinen, H.; Färkkilä, M. Fecal calprotectin and S100A12 have low utility in prediction of small bowel Crohn’s disease detected by wireless capsule endoscopy. Scand. J. Gastroenterol. 2012, 47, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Flamant, M.; Trang, C.; Maillard, O.; Sacher-Huvelin, S.; Rhun, M.L.; Galmiche, J.P.; Bourreille, A. The prevalence and outcome of jejunal lesions visualized by small bowel capsule endoscopy in Crohn’s disease. Inflamm. Bowel Dis. 2013, 19, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Annese, V.; Manetti, N. Capsule endoscopy in Crohn’s disease: Is there enough light in the tunnel? J. Crohns Colitis 2014, 8, 1598–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niv, E.; Fishman, S.; Kachman, H.; Arnon, R.; Dotan, I. Sequential capsule endoscopy of the small bowel for follow-up of patients with known Crohn’s disease. J. Crohns Colitis Mar. 2014, 22, 1616–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, B.; Holleran, G.; Chin, J.L.; Smith, S.; Ryan, B.; Mahmud, N.; Smith, S.; Ryan, B.; Mahmud, N.; McNamara, D. A prospective 52 week mucosal healing assessment of small bowel Crohn’s disease as detected by capsule endoscopy. J. Crohns Colitis Sep. 2014, 22, 1601–1609. [Google Scholar] [CrossRef] [Green Version]
- Leighton, J.A.; Triester, S.L.; Sharma, V.K. Capsule endoscopy: A meta-analysis for use with obscure gastrointestinal bleeding and Crohn’s disease. Gastrointest. Endosc. Clin. N. Am. 2006, 16, 229–250. [Google Scholar] [CrossRef]
- Bourreille, A.; Jarry, M.; D’Halluin, P.N.; Ben-Soussan, E.; Maunoury, V.; Bulois, P.; Sacher-Huvelin, S.; Vahedy, K.; Lerebours, E.; Heresbach, D. Wireless capsule endoscopy versus ileocolonoscopy for the diagnosis of postoperative recurrence of Crohn’s disease: A prospective study. Gut 2006, 55, 978–983. [Google Scholar] [CrossRef] [Green Version]
- Beltrán, V.P.; Nos, P.; Bastida, G.; Bastida, G.; Beltrán, B.; Argüello, L.; Aguas, M.; Rubín, A.; Pertejo, V.; Sala, T. Evaluation of postsurgical recurrence in Crohn’s disease: A new indication for capsule endoscopy? Gastrointest. Endosc. 2007, 66, 533–540. [Google Scholar] [CrossRef]
- Hammoudi, N.; Auzolle, C.; Minh, M.L.T.; Boschetti, G.; Bezault, M.; Buisson, A.; Pariente, B.; Treton, X.; Seksik, P.; Fumery, M.; et al. Postoperative endoscopic recurrence on the neoterminal ileum but not on the anastomosis is mainly driving long-term outcomes in Crohn’s disease. Am. J. Gastroenterol. 2020, 115, 1084–1093. [Google Scholar] [CrossRef]
- Lo, S.; Zaidel, O.; Tabibzadeh, S.; Papadakis, K.A.; Leo, T.; Kimble, J.; Vasiliauskas, E. Utility of wireless capsule enteroscopy (WCE) and IBD serology in reclassifying indeterminate colitis (IC). Gastroenterology 2003, 124, A192. [Google Scholar] [CrossRef]
- Kalla, R.; McAlindon, M.E.; Drew, K.; Sidhu, R. Clinical utility of capsule endoscopy in patients with Crohn’s disease and inflammatory bowel disease unclassified. Eur. J. Gastroenterol. Hepatol. 2013, 25, 706–713. [Google Scholar] [CrossRef]
- Min, S.B.; Le-Carlson, M.; Singh, N.; Nylund, C.M.; Gebbia, J.; Haas, K.; Lo, S.; Mann, N.; Melmed, G.Y.; Rabizadeh, S.; et al. Video capsule endoscopy impacts decision making in pediatric IBD: A single tertiary care center experience. Inflamm. Bowel Dis. 2013, 19, 2139–2145. [Google Scholar] [CrossRef]
- Maunoury, V.; Sovoye, G.; Bourreille, A.; Bouhnik, Y.; Jarry, M.; Sacher-Huvelin, S.; Ben Soussan, E.; Lerebours, E.; Galmiche, J.P.; Colombel, J.F. Value of wireless capsule endoscopy in patients with indeterminate colitis (inflammatory bowel disease type unclassified). Inflamm. Bowel Dis. 2007, 13, 152–155. [Google Scholar] [CrossRef]
- Lim, Y.J.; Yang, C.-H. Non-steroidal anti-inflammatory drug-induced enteropathy. Clin. Endosc. 2012, 45, 138–144. [Google Scholar] [CrossRef]
- Rana, S.S.; Sharma, V.; Sharma, R.; Nada, R.; Gupta, R.; Bhasin, D.K. Capsule endoscopy in small bowel Crohn’s disease and tuberculosis. Trop. Doct. 2017, 47, 113–118. [Google Scholar] [CrossRef]
- Singh, A. Cryptogenic multifocal ulcerating stenosing enteropathy(CMUSE) and/or chronic non-specific multiple ulcers of the small intestine(CNSU) and non-granulomatous ulcerating jejunoileitis (NGUJI). Curr. Gastroenterol. Rep. 2019, 10, 53. [Google Scholar] [CrossRef]
- Kim, H.M.; Kim, Y.J.; Kim, H.J.; Park, S.W.; Bang, S.; Song, S.Y. A pilot study of capsule endoscopy for the diagnosis of radiation enteritis. Hepatogastroenterology 2011, 58, 459–464. [Google Scholar]
- Okuda, K.; Daimon, Y.; Iwase, T.; Mitsufuji, S. Novel findings of capsule endoscopy and double-balloon enteroscopy in a case of eosinophilic gastroenteritis. Clin. J. Gastroenterol. 2013, 6, 16–19. [Google Scholar] [CrossRef]
- Akram, S.; Murray, J.A.; Pardi, D.S.; Alexander, G.L.; Schaffner, J.A.; Russo, P.A.; Abraham, S.C. Adult autoimmune enteropathy: Mayo Clinic Rochester experience. Clin. Gastroenterol. Hepatol. 2007, 5, 1282–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durmush, D.; Kaffes, A.J. Small bowel strictures. Curr. Opin. Gastroenterol. 2019, 35, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Cheifetz, A.S.; Kornbluth, A.A.; Legnani, P.; Schmelkin, I.; Brown, A.; Lichtiger, S.; Lewis, B.S. The risk of retention of the capsule endoscope in patients with known or suspected Crohn’s disease. Am. J. Gastroenterol. 2006, 101, 2218–2222. [Google Scholar] [CrossRef] [PubMed]
- Pasha, S.F.; Pennazio, M.; Rondonotti, E.; Wolf, D.; Buras, M.R.; Albert, J.G.; Cohen, S.A.; Cotter, J.; D’Haens, G.; Eliakim, R.; et al. Capsule retention in Crohn’s disease: A meta-analysis. Inflamm. Bowel Dis. 2020, 26, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Rondonotti, E. Capsule retention: Prevention, diagnosis and management. Ann. Transl. Med. 2017, 5, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, A.; Heigh, R.I.; Hara, A.K.; Decker, G.A.; Crowell, M.D.; Gurudu, S.R.; Pasha, S.F.; Fleischer, D.E.; Harris, L.A.; Post, J.; et al. Performance of the patency capsule compared with nonenteroclysis radiologic examinations in patients with known or suspected intestinal strictures. Gastrointest. Endosc. 2011, 74, 834–839. [Google Scholar] [CrossRef]
- Caunedo-Alvarez, A.; Romero-Vazquez, J.; Herrerias-Gutierrez, J.M. Patency and agile capsules. World J. Gastroenterol. 2008, 14, 5269–5273. [Google Scholar] [CrossRef]
- Rasmussen, B.; Nathan, T.; Jensen, M.D. Symptomatic patency capsule retention in suspected Crohn’s disease. J. Crohns Colitis 2016, 10, 1445–1447. [Google Scholar] [CrossRef] [Green Version]
- Silva, M.; Cardoso, H.; Cunha, R.; Peixoto, A.; Gaspar, R.; Gomes, S.; Santos, A.L.; Lopes, S.; Macedo, G. Evaluation of small-bowel patency in Crohn’s disease: Prospective study with a patency capsule and computed tomography. GE Port. J. Gastroenterol. 2019, 26, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Leighton, J.A.; Helper, D.J.; Gralnek, I.M.; Dotan, I.; Fernandez-Urien, I.; Lahat, A.; Malik, P.; Mullin, G.E.; Rosa, B. Comparing diagnostic yield of a novel pan-enteric video capsule endoscope with ileocolonoscopy in patients with active Crohn’s disease: A feasibility study. Gastrointest. Endosc. 2017, 85, 196–205. [Google Scholar] [CrossRef]
- Oliva, S.; Aloi, M.; Viola, F.; Mallardo, S.; Civitelli, F.; Maccioni, F.; Hassan, C.; Papoff, P.; Cucchiara, S.; Cohen, S.A. A Treat to Target Strategy Using Panenteric Capsule Endoscopy in Pediatric Patients With Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 2060–2067. [Google Scholar] [CrossRef]
- Klang, E.; Barash, Y.; Margalit, R.Y.; Soffer, S.; Shimon, O.; Albshesh, A.; Ben-Horin, S.; Amitai, M.M.; Eliakim, R.; Kopylov, U. Deep learning algorithms for automated detection of Crohn’s disease ulcers by video capsule endoscopy. Gastrointest. Endosc. 2020, 91, 606–613.e2. [Google Scholar] [CrossRef]
- Klang, E.; Grinman, A.; Soffer, S.; Margalit Yehuda, R.; Barzilay, O.; Amitai, M.M.; Konen, E.; Ben-Horin, S.; Eliakim, R.; Barash, Y.; et al. Automated detection of Crohn’s disease intestinal strictures on capsule endoscopy images using deep neural networks. J. Crohns Colitis 2020, 20, 749–756. [Google Scholar]
- Barash, Y.; Azaria, L.; Soffer, S.; Yehuda, R.M.; Shlomi, O.; Ben-Horin, S.; Eliakim, R.; Klang, E.; Kopylov, U. Ulcer severity grading in video capsule images of patients with Crohn’s disease: An ordinal neural network solution. Gastrointest. Endosc. 2021, 93, 187–192. [Google Scholar] [CrossRef]
- Nardo, G.D.; Esposito, G.; Ziparo, C.; Micheli, F.; Masoni, L.; Villa, M.P.; Parisi, P.; Manca, M.B.; Baccini, F.; Corleto, V.D. Enteroscopy in children and adults with inflammatory bowel disease. World J. Gastroenterol. 2020, 21, 5944–5958. [Google Scholar] [CrossRef]
- Ali, R.; Wild, D.; Shieh, F.; Diehl, D.L.; Fischer, M.; Tamura, W.; Rubin, D.T.; Kumbhari, V.; Okolo, P.; Storm, A. Deep enteroscopy with a conventional colonoscope: Initial multicenter study by using a through-the-scope balloon catheter system. Gastrointest. Endosc. 2015, 82, 855–860. [Google Scholar] [CrossRef]
- Inavolu, P.; Singh, A.P.; Kanakagiri, H.; Reddy, D.N.; Ramchandani, M. Motorized spiral enteroscope-assisted retrieval of video capsule in a patient with Crohn’s disease. VideoGIE 2020, 22, 488–491. [Google Scholar] [CrossRef]
- Rahman, A.; Ross, A.; Leighton, J.A.; Schembre, D.; Gerson, L.; Lo, S.K.; Waxman, I.; Dye, C.; Semrad, C. Double-balloon enteroscopy in Crohn’s disease: Findings and impact on management in a multicenter retrospective study. Gastrointest. Endosc. 2015, 82, 102–107. [Google Scholar] [CrossRef]
- Holleran, G.; Valerii, G.; Tortora, A.; Scaldaferri, F.; Conti, S.; Amato, A.; Gasbarrini, A.; Costamagna, G.; Riccioni, M.E. The use of single balloon enteroscopy in Crohn’s disease and its impact on clinical outcome. Scand. J. Gastroenterol. 2018, 53, 925–929. [Google Scholar] [CrossRef]
- Tun, G.S.; Rattehalli, D.; Sanders, D.S.; McAlindon, M.E.; Drew, K.; Sidhu, R. Clinical utility of double-balloon enteroscopy in suspected Crohn’s disease: A single-centre experience. Eur. J. Gastroenterol. Hepatol. 2016, 28, 820–825. [Google Scholar] [CrossRef]
- Christian, K.E.; Kapoor, K.; Goldberg, E.M. Performance characteristics of retrograde single-balloon endoscopy: A single center experience. World J. Gastrointest. Endosc. 2016, 8, 501–507. [Google Scholar] [CrossRef]
- Navaneethan, U.; Vargo, J.J.; Menon, K.V.; Sanaka, M.R.; Tsai, C.J. Impact of balloon-assisted enteroscopy on the diagnosis and management of suspected and established small-bowel Crohn’s disease. Endosc. Int. Open 2014, 2, E201–E206. [Google Scholar] [CrossRef] [Green Version]
- Schulz, C.; Mönkemüller, K.; Salheiser, M.; Bellutti, M.; Schütte, K.; Malfertheiner, P. Double-balloon enteroscopy in the diagnosis of suspected isolated Crohn’s disease of the small bowel. Dig. Endosc. 2014, 26, 236–242. [Google Scholar] [CrossRef]
- Urs, A.N.; Martinelli, M.; Rao, P.; Thomson, M.A. Diagnostic and therapeutic utility of double-balloon enteroscopy in children. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 204–212. [Google Scholar] [CrossRef]
- Uchida, K.; Yoshiyama, S.; Inoue, M.; Koike, Y.; Yasuda, H.; Fujikawa, H.; Okita, Y.; Araki, T.; Tanaka, K.; Kusunoki, M. Double balloon enteroscopy for pediatric inflammatory bowel disease. Pediatr. Int. 2012, 54, 806–809. [Google Scholar] [CrossRef]
- Ridder, L.D.; Mensink, P.B.; Lequin, M.H.; Aktas, H.; de Krijger, R.R.; van der Woude, C.J.; Escher, J.C. Single- balloon enteroscopy, magnetic resonance enterography, and abdominal US useful for evaluation of small-bowel disease in children with (suspected) Crohn’s disease. Gastrointest. Endosc. 2012, 75, 87–94. [Google Scholar] [CrossRef]
- Nardo, G.D.; Oliva, S.; Aloi, M.; Rossi, P.; Casciani, E.; Masselli, G.; Ferrari, F.; Mallardo, S.; Stronati, L.; Cucchiara, S. Usefulness of single-balloon enteroscopy in pediatric Crohn’s disease. Gastrointest. Endosc. 2012, 75, 80–86. [Google Scholar] [CrossRef]
- Seiderer, J.; Herrmann, K.; Diepolder, H.; Schoenberg, S.O.; Wagner, A.C.; Göke, B.; Ochsenkühn, T.; Schäfer, C. Double-balloon enteroscopy versus magnetic resonance enteroclysis in diagnosing suspected small-bowel Crohn’s disease: Results of a pilot study. Scand. J. Gastroenterol. 2007, 42, 1376–1385. [Google Scholar] [CrossRef]
- Mensink, P.B.; Groenen, M.J.; Van Buuren, H.R.; Kuipers, E.J.; Van der Woude, C.J. Double-balloon enteroscopy in Crohn’s disease patients suspected of small bowel activity: Findings and clinical impact. J. Gastroenterol. 2009, 44, 271–276. [Google Scholar] [CrossRef]
- Kondo, J.; Iijima, H.; Abe, T.; Komori, M.; Hiyama, S.; Ito, T.; Nakama, A.; Tominaga, K.; Kubo, M.; Suzuki, K.; et al. Roles of double-balloon endoscopy in the diagnosis and treatment of Crohn’s disease: A multicenter experience. J. Gastroenterol. 2010, 45, 713–720. [Google Scholar] [CrossRef]
- Möschler, O.; May, A.; Müller, M.K.; Ell, C. German DBE Study group. Complications in and performance of double-balloon enteroscopy (DBE): Results from a large prospective DBE database in Germany. Endoscopy 2011, 43, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, K.; Fujii, T.; Suzuki, K.; Shimizu, H.; Motobayashi, M.; Hibiya, S.; Saito, E.; Nagahori, M.; Watanabe, M.; Ohtsuka, K. Small bowel healing detected by endoscopy in patients with Crohn’s disease After treatment with antibodies against tumor necrosis factor. Clin. Gastroenterol. Hepatol. 2020, 18, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Takabayashi, K.; Hosoe, N.; Kato, M.; Hayashi, Y.; Nanki, K.; Fukuhara, K.; Mikami, Y.; Mizuno, S.; Sujino, T.; Mutaguchi, M.; et al. Significance of endoscopic deep small bowel evaluation using balloon-assisted enteroscopy for Crohn’s disease in clinical remission. J. Gastroenterol. 2021, 56, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Bouhnik, Y.; Carbonnel, F.; Laharie, D.; Stefanescu, C.; Hébuterne, X.; Abitbol, V.; Nachury, M.; Brixi, H.; Bourreille, A.; Picon, L.; et al. Efficacy of adalimumab in patients with Crohn’s disease and symptomatic small bowel stricture: A multicentre, prospective, observational cohort (CREOLE) study. Gut 2018, 67, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Bettenworth, D.; Lopez, R.; Hindryckx, P.; Levesque, B.G. Heterogeneity in endoscopic treatment of Crohn’s disease-associated strictures: An international inflammatory bowel disease specialist survey. J. Gastroenterol. 2016, 51, 939–948. [Google Scholar] [CrossRef]
- Bruining, D.H.; Zimmermann, E.M.; Loftus, E.V., Jr.; Sandborn, W.J.; Sauer, C.G.; Strong, S.A.; Society of Abdominal Radiology Crohn’s Disease-Focused Panel. Consensus recommendations for evaluation, interpretation, and utilisation of computed tomography and magnetic resonance enterography in patients with small bowel Crohn’s disease. Gastroenterology 2018, 154, 1172–1194. [Google Scholar] [CrossRef]
- Bettenworth, D.; Bokemeyer, A.; Kou, L.; Lopez, R.; Bena, J.F.; El Ouali, S.; Mao, R.; Kurada, S.; Bhatt, A.; Beyna, T.; et al. Systematic review with meta-analysis: Efficacy of balloon-assisted enteroscopy for dilation of small bowel Crohn’s disease strictures. Aliment Pharmacol. Ther. 2020, 52, 1104–1116. [Google Scholar] [CrossRef]
- Bettenworth, D.; Mucke, M.M.; Lopez, R.; Singh, A.; Zhu, W.; Guo, F.; Matsui, T.; James, T.W.; Herfarth, H.; Goetz, M.; et al. Efficacy of endoscopic dilation of gastroduodenal Crohn’s disease strictures: A systematic review and meta-analysis of individual patient data. Clin. Gastroenterol. Hepatol. 2019, 17, 2514–2522.e8. [Google Scholar] [CrossRef] [Green Version]
- Bettenworth, D.; Gustavsson, A.; Atreja, A.; Lopez, R.; Tysk, C.; van Assche, G.; Rieder, F. A pooled analysis of efficacy, safety, and long-term outcome of endoscopic balloon dilation therapy for patients with stricturing Crohn’s disease. Inflamm. Bowel Dis. 2017, 23, 133–142. [Google Scholar] [CrossRef]
- Shen, B.; Kochhar, G.; Navaneethan, U.; Farraye, F.A.; Schwartz, D.A.; Iacucci, M.; Bernstein, C.N.; Dryden, G.; Cross, R.; Bruining, D.H.; et al. Practical guidelines on endoscopic treatment for Crohn’s disease strictures: A consensus statement from the Global Interventional Inflammatory Bowel Disease Group. Lancet Gastroenterol. Hepatol. 2020, 5, 393–405. [Google Scholar] [CrossRef]
- Hirai, F.; Andoh, A.; Ueno, F.; Watanabe, K.; Ohmiya, N.; Nakase, H.; Kato, S.; Esaki, M.; Endo, Y.; Yamamoto, H.; et al. Efficacy of Endoscopic Balloon Dilation for Small Bowel Strictures in Patients With Crohn’s Disease: A Nationwide, Multi-centre, Open-label, Prospective Cohort Study. J Crohns Colitis. 2018, 12, 394–401. [Google Scholar] [CrossRef]
- Nishida, Y.; Hosomi, S.; Yamagami, H.; Yukawa, T.; Nagami, Y.; Tanaka, F.; Kamata, N.; Tanigawa, T.; Shiba, M.; Watanabe, T.; et al. Analysis of the Risk Factors of Surgery after Endoscopic Balloon Dilation for Small Intestinal Strictures in Crohn’s Disease Using Double-balloon Endoscopy. Intern. Med. 2017, 56, 2245–2252. [Google Scholar] [CrossRef] [Green Version]
- Sunada, K.; Shinozaki, S.; Nagayama, M.; Yano, T.; Takezawa, T.; Ino, Y.; Sakamoto, H.; Miura, Y.; Hayashi, Y.; Sato, H.; et al. Long-term Outcomes in Patients with Small Intestinal Strictures Secondary to Crohn’s Disease After Double-balloon Endoscopy-assisted Balloon Dilation. Inflamm. Bowel Dis. 22, 380–386. [CrossRef] [Green Version]
- Hirai, F.; Beppu, T.; Takatsu, N.; Yano, Y.; Ninomiya, K.; Ono, Y.; Hisabe, T.; Matsui, T. Long-term outcome of endoscopic balloon dilation for small bowel strictures in patients with Crohn’s disease. Dig. Endosc. 2014, 26, 545–551. [Google Scholar] [CrossRef]
- Gill, R.S.; Kaffes, A.J. Small bowel stricture characterization and outcomes of dilatation by double-balloon enteroscopy: A single-centre experience. Therap. Adv. Gastroenterol. 2014, 7, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Hirai, F.; Beppu, T.; Sou, S.; Seki, T.; Yao, K.; Matsui, T. Endoscopic balloon dilatation using double-balloon endoscopy is a useful and safe treatment for small intestinal strictures in Crohn’s disease. Dig. Endosc. 2010, 22, 200–204. [Google Scholar] [CrossRef]
- Despott, E.J.; Gupta, A.; Burling, D.; Tripoli, E.; Konieczko, K.; Hart, A.; Fraser, C. Effective dilation of small-bowel strictures by double-balloon enteroscopy in patients with symptomatic Crohn’s disease (with video). Gastrointest. Endosc. 2009, 70, 1030–1036. [Google Scholar] [CrossRef]
- Ohmiya, N.; Arakawa, D.; Nakamura, M.; Honda, W.; Shirai, O.; Taguchi, A.; Itoh, A.; Hirooka, Y.; Niwa, Y.; Maeda, O.; et al. Small-bowel obstruction: Diagnostic comparison between double-balloon endoscopy and fluoroscopic enteroclysis, and the outcome of enteroscopic treatment. Gastrointest. Endosc. 2009, 69, 84–93. [Google Scholar] [CrossRef]
- Pohl, J.; May, A.; Nachbar, L.; Ell, C. Diagnostic and therapeutic yield of push-and-pull enteroscopy for symptomatic small bowel Crohn’s disease strictures. Eur. J. Gastroenterol. Hepatol. 2007, 19, 529–534. [Google Scholar] [CrossRef]
- Fukumoto, A.; Tanaka, S.; Yamamoto, H.; Yao, T.; Matsui, T.; Iida, M.; Goto, H.; Sakamoto, C.; Chiba, T.; Sugano, K. Diagnosis and treatment of small-bowel stricture by double balloon endoscopy. Gastrointest. Endosc. 2007, 66, S108–S112. [Google Scholar] [CrossRef]
- Karstensen, J.G. Biodegradable stents for the treatment of bowel strictures in Crohn’s disease: Technical results and challenges. Endosc. Int. Open 2016, 4, E296–E300. [Google Scholar] [CrossRef] [Green Version]
- Das, R.; Singh, R.; Din, S.; Lund, J.; Krishnamoorthy, R.; Hearing, S.; Norton, B.; Williams, J.; Fraser, C.; Goddard, A.; et al. Therapeutic resolution of focal, predominantly anastomotic Crohn’s disease strictures using removable stents: Outcomes from a single-center case series in the United Kingdom. Gastrointest. Endosc. 2020, 92, 344–352. [Google Scholar] [CrossRef]
- Yokoyama, K.; Yano, T.; Kumagai, H.; Mizuta, K.; Ono, S.; Imagawa, T.; Yamamoto, H.; Yamagata, T. Double-balloon enteroscopy for pediatric patients: Evaluation of safety and efficacy in 257 cases. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 34–40. [Google Scholar] [CrossRef]
- Reddy, P.M.; Kulkarni, S.; Nabi, Z.; Kasle, S.; Chavan, R.; Pal, P.; Shrimal, P.; Choudhary, H.; Sayyed, M.; Reddy, D.N. Single balloon enteroscopy in children for evaluation of small bowel diseases in children: A large, tertiary center study. J. Pediatr. Surg. 2020. [Google Scholar] [CrossRef]
- Hotokezaka, M.; Jimi, S.I.; Hidaka, H.; Maehara, N.; Eto, T.A.; Chijiiwa, K. Role of intraoperative enteroscopy for surgical decision making with Crohn’s disease. Surg. Endosc. 2007, 21, 1238–1242. [Google Scholar] [CrossRef]
- Esaki, M.; Matsumoto, T.; Hizawa, K.; Aoyagi, K.; Mibu, R.; Iida, M.; Fujishima, M. Intraoperative enteroscopy detects more lesions but is not predictive of postoperative recurrence in Crohn’s disease. Surg. Endosc. 2001, 15, 455–459. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Number | Longitudinal Extent | Descriptors |
|---|---|---|---|
| First tertile | |||
| Villous appearance | Normal—0 Edematous—1 | Short segment—8 Long segment—12 Whole tertile—20 | Single—1 Patchy—14 Diffuse—17 |
| Ulcer | None—0 Single—3 Few—5 Multiple—10 | Short segment—5 Long segment—10 Whole tertile—15 | <1/4—9 1/4–1/2—12 >1/2—18 |
| Second tertile | |||
| Villous appearance | Normal—0 | Short segment—8 | Single—1 |
| Edematous—1 | Long segment—12 | Patchy—14 | |
| Whole tertile—20 | Diffuse—17 | ||
| Ulcer | None—0 | Short segment—5 | <1/4—9 |
| Single—3 | Long segment—10 | 1/4–1/2—12 | |
| Few—5 | Whole tertile—15 | > 1/2—18 | |
| Multiple—10 | |||
| Third tertile | |||
| Villous appearance | Normal—0 Edematous—1 | Short segment—8 Long segment—12 Whole tertile—20 | Single—1 Patchy—14 Diffuse—17 |
| Ulcer | None—0 Single—3 Few—5 Multiple—10 | Short segment—5 Long segment—10 Whole tertile—15 | <1/4—9 1/4–1/2—12 > 1/2—18 |
| Stenosis (rated for the whole study) | |||
| Stenosis | None—0 | Ulcerated—24 | Traversed—7 |
| Single—14 | Non-ulcerated—2 | Not traversed—10 | |
| Multiple—20 |
| CECDAI Scoring System | ||
|---|---|---|
| CECDAI | Proximal | Distal |
| A. Inflammation score | ||
| 0 = None | ||
| 1 = Mild to moderate edema/hyperemia/denudation | ||
| 2 = Severe edema/hyperemia/denudation | ||
| 3 = Bleeding, exudate, aphthae, erosion, small ulcer (≤0.5 cm) | ||
| 4 = Moderate ulcer (0.5–2 cm), pseudopolyp | ||
| 5 = Large ulcer (2 cm) | ||
| B. Extent of disease score | ||
| 0 = None | ||
| 1 = Focal disease (single segment) | ||
| 2 = Patchy disease (multiple segments) | ||
| 3 = Diffuse disease | ||
| C. Narrowing (stricture) | ||
| 0 = None | ||
| 1 = Single-passed | ||
| 2 = Multiple-passed | ||
| Segmental score = (A × B) + C | ||
| Total score = ((A1 × B1 + C1) + (A2 × B2 + C2)) | ||
| Author | DAE System | Patient Subgroup | Study Design | Suspected CD (n) | Proportion with CD (%) | Diagnostic Yield (%) | Impact on Management: Suspected CD (%) | Histology Suggestive or Confirmatory of CD |
|---|---|---|---|---|---|---|---|---|
| Broide et al., 2020, [4] | BGE | Pediatric IBD | Prospective | 15 (IBD) | 3/15 (20%) | 15/15 (100%) | ||
| Holleran et al., 2018, [70] | SBE | Adult CD | Retrospective | 13 | 4/13 (31%) | 8/13 (61.5%) | ||
| Tun et al., 2016. [71] | DBE | Adult CD | Retrospective | 100 | 38/100 (38%) | 71/100 (71%) | 71/100 (71%) | 23/100 (23%, 8% diagnostic, 15% supportive) |
| Christian et al., 2016, [72] | Retrograde SBE | Adult CD | Retrospective | 29 | 12/29 (38%) | |||
| Rahman et al., 2015. [69] | DBE | Adult CD | Retrospective | 43 | 17/43 (39.5%) | 34/43 (79%) | 33/43 (77%) | |
| Navaneethan et al., 2014, [73] | SBE or DBE | Adult CD | Retrospective | 22 | 6/22 (27%) | 22/22 (100%) | ||
| Schulz et al., 2014, [74] | DBE | Adult CD | Retrospective | 16 | 7/16 (44%) | 3/16 (19%) | ||
| Urs et al., 2014, [75] | DBE | Pediatric CD | Prospective | 3 | 2/3 (66%) | 3/3 (100%) | 2/3 (66%) | |
| Uchida et al.,2012, [76] | DBE | Pediatric CD | Prospective | 8 | 2/8 (25%) | 7/8 (87.5%) | 2/8 (25%) | |
| De Riddler et al., 2012, [77] | SBE | Pediatric CD | Prospective | 14 | 8/14 (57%) | 14/14 (100%) | ||
| Di Nardo, 2012, [78] | SBE | Pediatric CD | Prospective | 16 | 12/16 (75%) | 16/16 (100%) |
| Author | DAE System | Patient Subgroup | Study Design | Known CD (n) | Diagnostic Yield Confirmed CD (%) | Impact on Management: Confirmed CD (%) | Therapeutic Intervention (Endoscopic) |
|---|---|---|---|---|---|---|---|
| Broide et al., 2020, [4] | BGE | Pediatric IBD | Prospective | 9 | 9/9 (100%) | ||
| Holleran et al., 2018, [70] | SBE | Adult CD | Retrospective | 39 | 30/39 (77%) | 33/39 (85%) | 13/39 (33.3%) |
| Rahman et al., 2015, [69] | DBE | Adult CD | Retrospective | 38 | 33/38 (87%) | 31/38 (82%) | 3/38 (8%) |
| Navaneethan et al., 2014, [73] | SBE or DBE | Adult CD | Retrospective | 43 | 41/43 (95.3%) | 23/43 (53%) | |
| Urs et al., 2014, [75] | DBE | Pediatric CD | Prospective | 5 | 5/5 (100%) | 5/5 (100%) | |
| Uchida et al., 2012, [76] | DBE | Pediatric CD | Prospective | 4 | 4/4 (100%) | 3/4 (75%) | 1/4 (25%) |
| De Riddler et al., 2012, [77] | SBE | Pediatric CD | Prospective | 6 | 5/6 (83%) | 5/6 (83%) | |
| Di Nardo, 2012, [78] | SBE | Pediatric CD | Prospective | 14 | 14/14 (100%) | 14/14 (100%) | 3/14 (21%) |
| Kondo et al., 2010, [81] | DBE | Adult CD | Retrospective | 50 | 48% (percentage of active lesions among all enteroscopy sessions) | 53% (overall impact including new cases of CD) | |
| Mensink et al., 2009, [80] | DBE | Adult CD | Retrospective | 40 | 24/60 (40%) | 18/40 (45%) | 2/40 (5%) |
| Author | DAE System | Study Design | CD/no of Strictures (n) | Total Number of Dilations (Per Patient Mean) | Dilation Diameter: Mean (Range) (mm) | Technical Success (%) | Short Term Clinical Efficacy (%) | Major Complications (%) | Follow up (Months) | Recurrence of Symptoms | Re-Dilatation on Follow up | Surgery on Follow up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hirai et al., 2018, [92] | SBE or DBE | Prospective | 95 | 15 (8–20) | 94% | 69.5 | 5% | 24 | ||||
| Holleran et al., 2018, [70] | SBE | Retrospective | 13 | 14 (1) | 13 (12–15) | 100 | 80 | 0 | 8 | 24 | 7.7 | 0 |
| Nishida et al. 2017, [93] | DBE | Retrospective | 37 | 72 | 8.1 | 27.1 | 48.6 | |||||
| Sunada et al., 2016, [94] | DBE | Retrospective | 85 | 473 | 12.4 (8–20) | 87 | 5.9 | 41.9 | 75.3 | 24.7 (5 years) | ||
| Navaneethan et al., 2014, [73] | SBE or DBE | Retrospective | 8 | 10 | 75 | 16 | 66.6 | |||||
| Hirai et al., 2014, [95] | DBE | Retrospective | 65 | 105 | NA | 80 | 80 | 4.6 | 40.3 | 36.5 | 50 | 26.2 |
| Gill et al., 2014, [96] | DBE | Retrospective | 10 | 18 | 13.3 | 100 | 80 | 20 | 16 | 40 | 40 | 30 |
| Hirai et al.,2010, [97] | DBE | Retrospective | 25 | 55 | NA | 72 | 72 | 8 | 11.4 | 22.2 | 22.2 | 28 |
| Kondo et al., 2010, [81] | DBE | Retrospective | 8 | 18 (1.5) | 100 | 87.5 | 0 | |||||
| Despott et al., 2009, [98] | DBE | Prospective | 11 | 18 (2) | 15.4 (12–20) | 81.8 | 72.7 | 9.1 | 20.5 | 22.2 | 22.2 | 9.1 |
| Ohmiya et al., 2009, [99] | DBE | Retrospective | 16 | 18 | NA (8–20) | 96 | 100 | 0 | 16 | 31 | 12.5 | 18.8 |
| Pohl et al., 2007, [100] | Push enteroscopy | NA | 10 | 15 (1.5) | 17 (12–20) | 80 | 60 | 0 | 10 | 50 | 40 | |
| Fukumoto et al., 2007, [101] | DBE | Prospective | 23 | 35 (1.52) | NA | 100 | 74 | 0 | 12 | 26.1 | 17.1 | 8.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banerjee, R.; Pal, P. Endoscopic Evaluation and Therapeutic Considerations of Small Bowel Crohn’s Disease. Gastroenterol. Insights 2021, 12, 238-258. https://doi.org/10.3390/gastroent12020021
Banerjee R, Pal P. Endoscopic Evaluation and Therapeutic Considerations of Small Bowel Crohn’s Disease. Gastroenterology Insights. 2021; 12(2):238-258. https://doi.org/10.3390/gastroent12020021
Chicago/Turabian StyleBanerjee, Rupa, and Partha Pal. 2021. "Endoscopic Evaluation and Therapeutic Considerations of Small Bowel Crohn’s Disease" Gastroenterology Insights 12, no. 2: 238-258. https://doi.org/10.3390/gastroent12020021
APA StyleBanerjee, R., & Pal, P. (2021). Endoscopic Evaluation and Therapeutic Considerations of Small Bowel Crohn’s Disease. Gastroenterology Insights, 12(2), 238-258. https://doi.org/10.3390/gastroent12020021